

Introduction
Although the relationship between personality and depressive illness is complex (Shea, 2005), there is empirical evidence that some personality features such as neuroticism, harm avoidance, introversion, dependency, self-criticism or perfectionism are related to depressive illness risk (Gunderson et al. 1999). Moreover, personality traits, especially neuroticism, may explain the increased prevalence of depression among females (Goodwin & Gotlib, 2004).
Few studies have explored neuroticism, extraversion and psychoticism as risk factors for depression after an event as stressful as childbirth. Pitt (1968) was the first author to report high scores on neuroticism and low scores on extraversion among postpartum depressed women. Similar results were found in a comparison of mothers with and without postpartum depressive symptoms (Dudley et al. 2001; Podolska et al. 2010). A case-control study comparing women with recurrent major depression with and without a history of postpartum depression found no personality trait differences between them; however, those with a history of postpartum depression showed higher neuroticism and psychoticism and lower extraversion than controls. These results suggested that these traits did not confer a specific risk for the postnatal onset episodes (Jones et al. 2010). Prospective studies have also studied the link between personality and postpartum depression; however, these data are not conclusive due to methodological limitations, such as sample size (Kumar & Robson, 1984; Watson et al. 1984; Areias et al. 1991; Boyce et al. 1991; Matthey et al. 2000), selection bias (Kumar & Robson, 1984; Areias et al. 1991; Boyce et al. 1991; Matthey et al. 2000), or depression assessment (self-report measures versus clinical diagnosis: Boyce et al. 1991; Matthey et al. 2000; Dudley et al. 2001; Saisto et al. 2001; Van Bussel et al. 2009) or because the authors did not take into account confounding factors such as stressful life events or social support (Watson et al. 1984; Kumar & Robson, 1984; Boyce et al. 1991; Matthey et al. 2000; Saisto et al. 2001; Verkerk et al. 2005; Van Bussel et al. 2009). (See Supplementary material, Table S1.)
The aim of this paper was to extend the previous knowledge of the role of neuroticism, extroversion and psychoticism as risk factors for postpartum depression (depression symptomatology and clinical diagnosis) considering psychosocial variables in a large cohort of women from the general population.
Method
Between December 2003 and October 2004, women (second to third days postpartum) were recruited from seven acute-care teaching hospitals in Spain and invited to participate in a 32-week follow-up study (Sanjuán et al. 2008). All participants were Spanish, Caucasian and able to understand and answer clinical questionnaires. None of the participants had a current depression or other psychiatric illness during pregnancy. Moreover, those women whose children died after birth were excluded. The institutional review boards of the participating hospitals approved the study. All women gave written informed consent.
At baseline (second to third days postpartum) all participants completed a semi-structured interview that included sociodemographic data (i.e. age, marital status, job and economic situation), obstetric variables (parity and type of delivery) and personal and family history of psychiatric illness (any psychiatry conditions with pharmacological or psychological treatment were considered). Furthermore, all women were assessed, as follows.
(1) Validated Spanish version of the Eysenck Personality Questionnaire Revised Short Scale (EPQ-RS; Eysenck & Eysenck, 2001)
The EPQ-RS consists of 48 items from the 100-item EPQ-R and measures three dimensions of personality: extraversion (E), neuroticism (N) and psychoticism (P). We obtained gender T-scores for the Spanish population. In the present study, we also used a categorical personality classification. T-scores greater than 55 defined high extraversion, high neuroticism and high psychoticism, whereas T-scores less than or equal to 45 defined low-extraversion, low-neuroticism and low-psychoticism groups.
(2) Spanish version of the St Paul Ramsey Life Experience Scale (Baca-Garcia et al. 2007)
The St Paul Ramsey Life Experience Scale rated the impact of participants' stressful life events using a seven-point scale of severity over the pregnancy period. Six different categories of events were considered: primary support, social environment, housing, work, health and economy. The outcome variable was dichotomous: absence or presence (with at least a severity score of 2 in one or more categories) of stressful life events during pregnancy.
(3) Spanish validated version of the Duke-UNC Functional Social Support Questionnaire (Bellón et al. 1996)
The Duke-UNC Functional Social Support Questionnaire is an 11-item, self-administered questionnaire designed to evaluate perceived functional social support. The item response options are on a five-point scale ranging from 1 (‘much less than I would like’) to 5 (‘as much as I would like’). Higher scores reflect higher perceived social support.
(4) Spanish validated version of the Edinburgh Postnatal Depression Scale (EPDS; Garcia-Esteve et al. 2003)
The EPDS was used to assess depressive symptoms at early postpartum. The EPDS is a 10-item self-report scale with four possible responses and a total score ranging from 0 to 30 and has been used as a screening tool for non-psychotic psychiatric disorders in the postpartum period (Navarro et al. 2007).
At 8 and 32 weeks postpartum, the presence of depressive symptoms was evaluated with the EPDS. All women who scored EPDS >9 at 8 and 32 weeks postpartum were defined as probable postpartum depression cases (Garcia-Esteve et al. 2003; Navarro et al. 2007). The Spanish version of the Diagnostic Interview for Genetics Studies (DIGS) for DSM-IV (Roca et al. 2007) adapted for postpartum depression evaluated all probable cases of major postpartum depression during the 32 weeks after delivery.
For the univariate analysis, we used the χ2 test and Student's t test for qualitative and quantitative variables, respectively. Outcomes variables were: (1) depressive symptoms (EPDS >9) at 8 weeks postpartum; (2) depressive symptoms (EPDS >9) at 32 weeks in the case of EPDS ⩽9 at 8 weeks; and (3) the presence of a major depressive episode during the 32 weeks after delivery using DIGS for DSM-IV criteria. The independent variables were neuroticism, extraversion and psychoticism, although we also considered other variables related to personality and depression, as well as sociodemographic variables.
To find an adequate logistic regression model for each of the three outcomes as a function of the independent variables of interest, we used the procedure proposed by Hosmer & Lemeshow (2000). First, univariate logistic models for all variables of interest were fit and models with a significance level less than 0.25 were included in the multivariate model. Then, backward selection removed variables from the model if they were not significant at the 0.05 level, as long as the parameter estimates of the remaining variables did not change substantially; in this way we ruled out potential confounders from the model. Once the model included only significant variables, we checked whether previously excluded variables were now significant. We also considered possible interactions of the remaining variables. Finally, we checked the model's global goodness of fit. Model parameters were interpreted in terms of adjusted odds ratios (aORs) and 95% confidence intervals (CIs). The data analyses were carried out using SPSS 11.5 (SPSS. Inc., USA) and the R statistical software package (http://www.r-project.org).
Results
This study included 1974 women, 94 (5%) of whom chose not to participate and 76 (3.8%) of whom were excluded because of incomplete EPDS questionnaires; thus, the final sample comprised 1804 women. At the 8-week follow-up, 1407 (78%) women remained in the study. At 32 weeks, 1337 (74.1%) women were evaluated. Women who dropped out during the follow-up period were more likely to have a lower education level (p<0.001), economic problems (p=0.002), no long-term relationship (p=0.001) and no psychiatric history (p=0.002) than the final sample; there were no significant differences among personality variables, social support and number of stressful life events suffered during pregnancy.
The total sample (n=1804) had a mean age of 31.7 (s.d.=4.6), and a range of 18–46 years; 32% of participants had only attended primary school, 41% finished secondary school and 27% had a college degree. Almost all were married or had a stable partner (97%) and lived with their own family (95%). Most participants (68%) were employed. Of the participants, 9% reported some economic problems, 46% were primiparous, 80% had a vaginal delivery, 31% had a family psychiatric history and 16% had a personal psychiatric history. The mean T-score for personality dimensions at baseline was 51.1 (s.d.=9.6) for extraversion, 43.6 (s.d.=8.5) for neuroticism and 48.0 (s.d.=8.9) for psychoticism. The mean EPDS score was 6.1 (s.d.=4.5). In regard to social support, the Duke-UNC score mean was 52.0 (s.d.=8.6). Of the women, 37% reported having suffered at least one stressful life event during pregnancy.
The mean EPDS score was 5.3 (s.d.=4.6) at 8 weeks postpartum and 4.4 (s.d.=4.7) at 32 weeks postpartum. At 8 weeks, we identified 214 women (11.9%) with depressive symptoms (i.e. EPDS >9). At 32 weeks postpartum, 24% women had EPDS >9, but only 102 (7.6%) women had depressive symptomatology after 8 weeks. Overall, 173 women (12.7%) had a major depressive episode confirmed by DIGS during the first 32 weeks postpartum; 53.8% were recurrences and 46.2% were new onsets.
The results of the univariate analysis showed significant differences in personality dimensions and other potential predictors between women with or without postpartum depressive symptoms (i.e. EPDS >9) and major postpartum depression (DSM-IV) (Table 1). With respect to personality traits, women with depressive symptoms at 8 weeks as well as women with a major postpartum depression episode during the 32 weeks postpartum obtained lower scores on extraversion and higher scores on neuroticism and psychoticism than women from healthy groups. However, when the appearance of depressive symptoms at 32 weeks postpartum was considered, differences were only found on neuroticism.
Table 1.
Differences in personality dimensions and other risk factors between women with and without postpartum depression
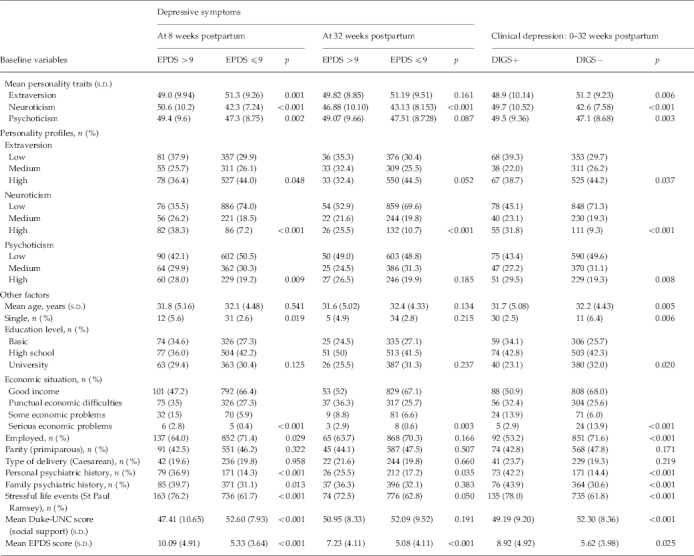
EPDS, Edinburgh Postnatal Depression Scale; DIGS, Diagnostic Interview for Genetics Studies; s.d., standard deviation.
Logistic regression analyses were used to explore personality features, taking into account other risk factors that could help to predict depressive symptoms (i.e. EPDS >9) at 8 and 32 weeks postpartum, as well as a major depressive episode using the DSM-IV criteria during 32 weeks postpartum. Neuroticism was the only personality trait which increased the risk of EPDS scores >9 at 8 and 32 weeks postpartum as well as a major depressive episode during the 32 weeks after childbearing (aOR 1.05, 95% CI 1.02–1.07; aOR 1.04, 95% CI 1.01–1.08 and aOR 1.05, 95% CI 1.02–1.08, respectively). Other risk factors such as EPDS scores at baseline, history of depression, social support, economic situation and stressful life events during pregnancy were also identified as risk factors for postpartum depression (Table 2).
Table 2.
Final logistic regression models for postpartum depression
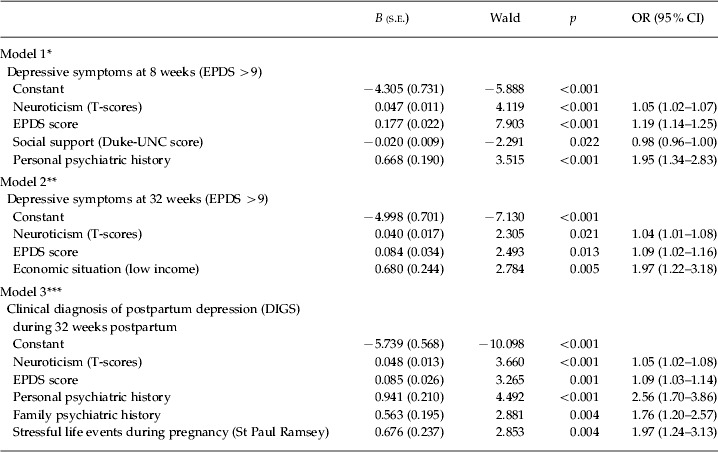
s.e., Standard error; OR, odds ratio; CI, confidence interval; EPDS, Edinburgh Postnatal Depression Scale; DIGS, Diagnostic Interview for Genetics Studies.
Goodness of fit:
p=0.66, ** p=0.55, *** p=0.4.
Discussion
This study confirmed in a large and representative sample of postpartum women that neuroticism is an independent predictor of major postpartum depression and depressive symptomatology at 8 and 32 weeks postpartum. Supporting research on stress vulnerability in women, our study found that high neuroticism raises the probability that a major depressive episode presents after a major biological, psychological and social life event such as giving birth. However, it is worth noting that high neuroticism showed a slightly moderate effect size, and that personal and family psychiatric histories are also important risk factors in the first weeks after delivery, at 6 months and beyond. Moreover, this study highlights the role of environmental factors such as social support, economical problems and other stressful life events during pregnancy. Together, all these variables contribute to depression after delivery.
The role of other personality traits was less clear. Neither extraversion nor psychoticism was confirmed as a risk factor after controlling for EPDS scores at baseline as well as other confounding factors. Consistent with our results, extraversion has failed to predict EPDS scores (Boyce et al. 1991; van Bussel et al. 2009) and clinical major depression (Areias et al. 1996). In our study, low extraversion was associated with EPDS scores greater than 9 at 8 weeks and with major postpartum depression (DSM-IV), which might be explained by state effects on extraversion scores (Enns & Cox, 1997; Griens et al. 2002). Thus, the association between extraversion and depression would disappear after controlling for EPDS scores and other factors at baseline. In agreement with other findings in postpartum populations (Kumar & Robson, 1984; Watson et al. 1984), psychoticism did not predict postpartum depression; however, the results of the univariate analysis showed that psychoticism was associated with EPDS scores at 8 weeks postpartum and with major postpartum depression (DSM-IV). These results are also consistent with a recent case-control study on women with recurrent major depression and a history of postpartum depression (Jones et al. 2010). Psychoticism has also been related to an excess of severe and threatening life events, depressive symptoms and suicide ideation in cross-sectional studies in non-postpartum populations (Farmer et al. 2001; Kumar & Pradhan, 2003; Pickering et al. 2003).
The results of the study cannot be generalized to the general population because we excluded women with psychiatric disorders during pregnancy, which is a risk factor for postpartum depression (Dennis & Ross, 2006). We chose this strategy to ensure that we were dealing with vulnerability to the onset of a new major postpartum depressive episode. Nevertheless, we assessed personality 2 days after delivery, and some women experience a transient affective syndrome called postpartum blues (Henshaw, 2003). For this reason, we decided to include EPDS scores at baseline in regression models. We did not exclude women with a history of major depression before pregnancy, so we cannot determine if personality traits were a residual symptomatology of previous depressive episodes; however, our analysis controlled for personal psychiatry history. Moreover, we did not study all personality traits; so future postpartum cohort studies should include other personality traits such as perfectionism (Mazzeo et al. 2006; Gelabert et al. 2011) and coping styles (de Tychey et al. 2005). Recent preliminary data showed that self-criticism traits might also be an important factor in the persistence of depressive symptoms in postpartum depression (Vliegen et al. 2010). However, we were interested in studied personality traits and other risk factors in the postpartum period. The strengths of this study compared with previous reports in this field are: the large sample of the general population, the longitudinal design, the method of depression assessment, and the advantage of taking into account confounding factors such as stressful life events or social support during pregnancy. It would have been interesting to study stressful life events and social support also during the postpartum period.
Overall, these findings have clinical implications for women at risk of postpartum depression before leaving the obstetric ward. Understanding the effect of neuroticism, along with other biological and social variables, allows clinicians to detect subgroups of women with an increased vulnerability to postpartum depression who might receive early psychological and psychiatric care.
Acknowledgements
This work was supported by the Instituto Carlos III (Spanish Ministry of Health; grant numbers P1041635, PI041783, PI041779, PI0411761, PI041791, PI041766 and PI041782), as well as the Spanish Psychiatric Genetics and Genotyping network G03/184, RTA (RD06/001/1009), and Generalitat de Catalunya, SGR2009/1435).
Supplementary material
For supplementary material accompanying this paper, visit http://dx.doi.org/10.1017/S0033291712000712.
Declaration of Interest
None.
References
- Areias MEG, Kumar R, Barros H, Figueiredo E. Correlates of postnatal depression in mothers and fathers. British Journal of Psychiatry. 1996;169:36–41. doi: 10.1192/bjp.169.1.36. [DOI] [PubMed] [Google Scholar]
- Baca-Garcia E, Parra CP, Perez-Rodriguez MM, Diaz-Sastre C, Reyes-Torres R, Saiz-Ruiz J, de Leon J. Psychosocial stressors may be strongly associated with suicide attempts. Stress and Health. 2007;23:191–198. [Google Scholar]
- Bellón JA, Delgado A, de Dios J, Lardelli P. Validez y fiabilidad del cuestionario de apoyo social funcional Duke-UK-11 [Validity and reliability of the Duke-UK-11 functional social support questionnaire] Atención Primaria. 1996;18:153–163. [PubMed] [Google Scholar]
- Boyce P, Parker G, Barnett B, Cooney M, Smith F. Personality as a vulnerability factor to depression. British Journal of Psychiatry. 1991;159:106–114. doi: 10.1192/bjp.159.1.106. [DOI] [PubMed] [Google Scholar]
- Dennis CL, Ross LE. Depressive symptomatology in the immediate postnatal period: identifying maternal characteristics related to true- and false-positive screening scores. Canadian Journal of Psychiatry. 2006;51:265–273. doi: 10.1177/070674370605100501. [DOI] [PubMed] [Google Scholar]
- de Tychey C, Spitz E, Briançon S, Lighezzolo J, Girvan F, Rosati A, Thockler A, Vincent S. Pre- and postnatal depression and coping: a comparative approach. Journal of Affective Disorders. 2005;85:323–326. doi: 10.1016/j.jad.2004.11.004. [DOI] [PubMed] [Google Scholar]
- Dudley M, Roy K, Kelk N, Bernard D. Psychological correlates of depression in fathers and mothers in the first postnatal year. Journal of Reproductive and Infant Psychology. 2001;19:187–202. [Google Scholar]
- Enns MW, Cox BJ. Personality dimensions and depression: review and commentary. Canadian Journal of Psychiatry. 1997;42:274–284. doi: 10.1177/070674379704200305. [DOI] [PubMed] [Google Scholar]
- Eysenck HJ, Eysenck SBG. Cuestionario revisado de personalidad de Eysenck: versiones completa (EPQ-R) y abreviada (EPQ-RS) [Eysenck Personality Questionnaire Revised: Full Version (EPQ-R) and Short (EPQ-RS)] TEA; Madrid: 2001. [Google Scholar]
- Farmer A, Redman K, Harris T, Webb R, Mahmood A, Sadler S, McGuffin P. The Cardiff sib-pair study: suicidal ideation in depressed and healthy subjects and their siblings. Crisis. 2001;22:71–73. doi: 10.1027//0227-5910.22.2.71. [DOI] [PubMed] [Google Scholar]
- Garcia-Esteve L, Ascaso C, Ojuel J, Navarro P. Validation of the Edinburgh Postnatal Depression Scale (EPDS) in Spanish mothers. Journal of Affective Disorders. 2003;75:71–76. doi: 10.1016/s0165-0327(02)00020-4. [DOI] [PubMed] [Google Scholar]
- Gelabert E, Garcia-Esteve L, Martín-Santos R, Gutiérrez F, Torres A, Subirà S. Psychometric properties of the Spanish version of the Frost Multidimensional Perfectionism Scale in women. Psicothema. 2011;23:140–145. [PubMed] [Google Scholar]
- Goodwin RD, Gotlib IH. Gender differences in depression: the role of personality factors. Psychiatry Research. 2004;126:135–142. doi: 10.1016/j.psychres.2003.12.024. [DOI] [PubMed] [Google Scholar]
- Griens AMGF, Jonker K, Spinhoven P, Blom MBJ. The influence of depressive state features on trait measurement. Journal of Affective Disorders. 2002;70:95–99. doi: 10.1016/s0165-0327(00)00371-2. [DOI] [PubMed] [Google Scholar]
- Gunderson JG, Triebwasser J, Phillips KA, Sullivan CN. Cloninger C. R. Personality and Psychopathology. American Psychiatric Press; Washington, DC: 1999. Personality and vulnerability to affective disorders; pp. 3–32. ), pp. [Google Scholar]
- Henshaw C. Mood disturbance in the early puerperium: a review. Archives of Women's Mental Health. 2003;6:33–42. doi: 10.1007/s00737-003-0004-x. [DOI] [PubMed] [Google Scholar]
- Hosmer DW, Lemeshow S. Applied Logistic Regression. John Wiley and Sons; New York: 2000. [Google Scholar]
- Jones L, Scott J, Cooper C, Forty L, Smith KG, Sham P, Farmer A, McGuffin P, Craddock N, Jones I. Cognitive style, personality and vulnerability to postnatal depression. British Journal of Psychiatry. 2010;196:200–205. doi: 10.1192/bjp.bp.109.064683. [DOI] [PubMed] [Google Scholar]
- Kumar R, Robson KM. A prospective study of emotional disorders in childbearing women. British Journal of Psychiatry. 1984;144:35–47. doi: 10.1192/bjp.144.1.35. [DOI] [PubMed] [Google Scholar]
- Kumar U, Pradhan RK. Correlates of suicide ideation: a factor analytic study. Social Science International. 2003;19:36–43. [Google Scholar]
- Matthey S, Barnett B, Ungerer J, Waters B. Paternal and maternal depressed mood during the transition to parenthood. Journal of Affective Disorders. 2000;60:75–85. doi: 10.1016/s0165-0327(99)00159-7. [DOI] [PubMed] [Google Scholar]
- Mazzeo SE, Landt MCTS, Jones I, Mitchell K, Kendler KS, Neale MC, Aggen SH, Bulik CM. Associations among postpartum depression, eating disorders, and perfectionism in a population-based sample of adult women. International Journal of Eating Disorders. 2006;39:202–211. doi: 10.1002/eat.20243. [DOI] [PubMed] [Google Scholar]
- Navarro P, Ascaso C, Garcia-Esteve L, Aguado J, Torres A, Martin-Santos R. Postnatal psychiatric morbidity: a validation study of the GHQ-12 and the EPDS as screening tools. General Hospital Psychiatry. 2007;29:1–7. doi: 10.1016/j.genhosppsych.2006.10.004. [DOI] [PubMed] [Google Scholar]
- Pickering A, Farmer A, Harris T, Redman K, Mahmood A, Sadler S, McGuffin P. A sib-pair study of psychoticism, life events and depression. Personality and Individual Differences. 2003;34:613–623. [Google Scholar]
- Pitt B. ‘Atypical’ depression following childbirth. British Journal of Psychiatry. 1968;114:1325–1335. doi: 10.1192/bjp.114.516.1325. [DOI] [PubMed] [Google Scholar]
- Podolska MZ, Bidzan M, Majkowicz M, Podolski J, Sipak-Szmigiel O, Ronin-Walknowska E. Personality traits assessed by the NEO Five-Factor Inventory (NEO-FFI) as part of the perinatal depression screening program. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research. 2010;16:77–81. [PubMed] [Google Scholar]
- Roca M, Martin-Santos R, Saiz J, Obiols J, Serrano MJ, Torrens M, Subira S, Gili M, Navines R, Ibanez A, Nadal M, Barrantes N, Canellas F. Diagnostic Interview for Genetic Studies (DIGS): inter-rater and test–retest reliability and validity in a Spanish population. European Psychiatry. 2007;22:44–48. doi: 10.1016/j.eurpsy.2006.10.004. [DOI] [PubMed] [Google Scholar]
- Saisto T, Salmela-Aro K, Nurmi JE, Halmesmaki E. Psychosocial predictors of disappointment with delivery and puerperal depression. A longitudinal study. Acta Obstetricia et Gynecologica Scandinavica. 2001;80:39–45. doi: 10.1034/j.1600-0412.2001.800108.x. [DOI] [PubMed] [Google Scholar]
- Sanjuán J, Martín-Santos R, Garcia-Esteve L, Carot JM, Guillamat R, Gutierrez-Zotes A, Gornemann I, Canellas F, Baca-Garcia E, Jover M, Navinés R, Valles V, Vilella E, de Diego Y, Castro JA, Ivorra JL, Gelabert E, Guitart M, Labad A, Mayoral F, Roca M, Gratacòs M, Costas J, van Os J, de Frutos R. Mood changes after delivery role of the serotonin transporter gene. British Journal of Psychiatry. 2008;193:383–388. doi: 10.1192/bjp.bp.107.045427. [DOI] [PubMed] [Google Scholar]
- Shea MTY. Rosenbluth M., Kennedy S. H., Bagby R. M. Depression and Personality: Conceptual and Clinical Challenges. American Psychiatric Publishing; Arlington: 2005. Personality traits/disorders and depression: a summary of conceptual and empirical findings; pp. 43–64. ), pp. [Google Scholar]
- Van Bussel JCH, Spitz B, Demyttenaere K. Depressive symptomatology in pregnant and postpartum women. An exploratory study of the role of maternal antenatal orientations. Archives of Women's Mental Health. 2009;12:155–166. doi: 10.1007/s00737-009-0061-x. [DOI] [PubMed] [Google Scholar]
- Verkerk G, Denollet J, Van Heck G, Van Son M, Pop V. Personality factors as determinants of depression in postpartum women: a prospective 1-year follow-up study. Psychosomatic Medicine. 2005;67:632–637. doi: 10.1097/01.psy.0000170832.14718.98. [DOI] [PubMed] [Google Scholar]
- Vliegen N, Luyten P, Besser A, Casalin S, Kempke S, Tang E. Stability and change in levels of depression and personality: a follow-up study of postpartum depressed mothers that were hospitalized in a mother–infant unit. Journal of Nervous and Mental Disease. 2010;198:45–51. doi: 10.1097/NMD.0b013e3181c8aa57. [DOI] [PubMed] [Google Scholar]
- Watson JP, Elliott SA, Rugg AJ, Brough DI. Psychiatric disorder in pregnancy and the first postnatal year. British Journal of Psychiatry. 1984;144:453–462. doi: 10.1192/bjp.144.5.453. [DOI] [PubMed] [Google Scholar]