

Abstract
Background. Increasing levels of obesity over recent decades have been expected to lead to an epidemic of diabetes and a subsequent reduction in life expectancy, but instead all-cause and cardiovascular-specific mortality rates have decreased steadily in most developed countries and life expectancy has increased. Methods. This paper suggests several factors that may be masking the effects of obesity on life expectancy. Results. It is possible that health and life expectancy gains could be even greater if it was not for the increasing prevalence of extreme obesity. It is also possible that the principal impact of obesity is on disability-free life expectancy rather than on life expectancy itself. Conclusion. If the principal impact of obesity were through disability-free life expectancy rather than on life expectancy itself, this would have substantial implications for the health of individuals and the future burden on the health care system.
1. Introduction
Obesity has reached unprecedented levels globally and its rise is projected to continue. This has caused widespread concern, considering the associations between obesity and a range of adverse health conditions. There is a widely held view that the increasing rates of obesity will lead to an epidemic of diabetes, other chronic conditions, and a subsequent reduction in life expectancy. However the picture is complicated. Since the 1960s all-cause and cardiovascular-specific mortality rates have decreased steadily in most developed countries, and life expectancy has consistently increased [1]. The aim of this paper is to suggest several reasons for the discrepancy between increasing levels of obesity and gains in life expectancy, and those factors may be masking the effects of obesity on life expectancy.
A better understanding of the way in which obesity affects health and longevity will help determine the most appropriate response to increasing levels of excess body weight and assist our understanding of the likely impact of obesity on the health of individuals and the future burden on the health care system.
2. Population Trends
An increasing prevalence of obesity has been observed in most countries worldwide. This is considered to have led to an “epidemic” of type II diabetes. The progression of this epidemic, in tandem with cardiovascular disease and several other morbidities associated with obesity, is predicted to slow or reverse the decline in mortality that has been noted in most Western countries over the past 30–40 years [1].
The data accumulated to date have provided relatively little evidence in support of this view. Levels of obesity have been increasing since the 1950s (albeit slowly, initially) in the USA and other developed countries [2]. Over the same period, life expectancy has continued to increase at an undiminished rate [3], and cardiovascular-specific mortality rates have also decreased continually [4].
Why the Contradiction? —
A number of factors may explain the apparent discrepancy.
(1) Improvement in Other Risk Factors —
It is possible that the deleterious impact of obesity is outweighed by other factors favourably influencing life expectancy. Capewell et al. (2010) have reported that in the United States three of the six major risk factors for CHD—total cholesterol, prevalence of smoking, and physical activity levels—improved between 1988 and 2003 [5]. There was also a lowering of blood pressure in men [5]. Under this scenario, the rate of decline of all-cause and CVD mortality might be faster still if it was not for the increasing prevalence of diabetes [5, 6], for which there is a clear association with heart disease [7]. Examples of factors driving mortality down include population-wide changes such as reductions in the prevalence and intensity of smoking [7]. However, Stewart et al. (2009) have predicted that over the next decade the negative effects of increasing levels of obesity will outweigh the benefits from reductions in the prevalence of smoking [7]. However, Peto et al. (2010) critiqued this finding, suggesting that Stewart et al. (2009) have overestimated the hazards of obesity and underestimated the hazards of smoking [8].
(2) Pharmacological Treatment —
There is the possibility of improved medical interventions in some of the pathways linking obesity to CVD and all-cause mortality. For example, improved control of hypertension and better management of dyslipidaemia may blunt the impact of obesity on adverse health outcomes [3, 9]. Hypertension has been fairly well controlled in recent years, and there has been increased use of statins, angiotensin pathway inhibitors, and aspirin, all of which may be contributing to the limited effect of rising obesity levels.
(3) Prevalence of More Extreme Obesity —
The impact of obesity may have been overestimated because its principal adverse effects are experienced by a minority of the population. The most robust estimates of the association between BMI and mortality, from the Prospective Studies Collaboration of 900,000 adults in 57 prospective studies, suggests that the mortality risk from excess body weight increases from a BMI of 25 but is not substantial until BMI exceeds 32–35 [10]. Between 15 and 25 percent of the US population have BMIs in this range. It is a significant proportion but nevertheless a clear minority of the population, at least currently. Although significant increases in the prevalence of severe obesity (BMI > 40) have been reported in a number of countries [11, 12], the risk for this group is outweighed by the considerably less significant risks associated with body weight in the majority of the population (Figure 1).
Figure 1.
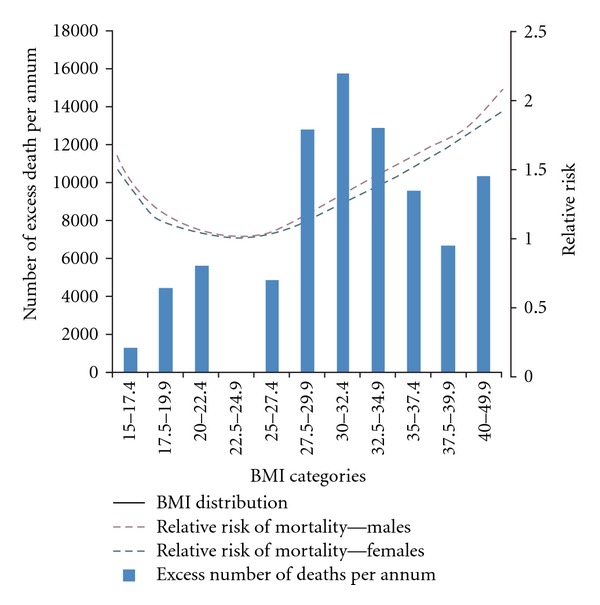
Risk relationships between body weight and mortality.
(4) Reversal of Relationship in Old Age —
In old age those of low body weight are at higher risk of disability (limitations to activities of daily living) and mortality [13]. The relationship between obesity and health appears to reverse in old age. For example, Diehr et al. (1988) found little relationship between BMI and mortality in older adults, except for those of very low body weight, who had a higher mortality than others [13]. It is likely, however, that this reversal of the obesity and health relationship in older people is due to weight loss in old age due to health problems or disease.
(5) Body Weight Per Se Not Associated with Mortality —
It is possible that body weight is not a significant risk factor for mortality. Body weight may act simply as a surrogate for a constellation of attributes of lifestyle, in particular diet, physical activity level, and genetic factors [14]. If this were the case, obese individuals would represent a heterogeneous group of high body weight due to a variety of reasons, some of which may not be so strongly related as others to morbidity or mortality.
(6) Latency Period and Cohort Effect —
It is possible that the deleterious impact of recent obesity trends has not yet affected life expectancy due to a considerable latency period between onset of obesity and disease. Recent cohorts of the US population are experiencing a greater magnitude and duration of obesity over their lifetime [15]. The duration of exposure to obesity has been reported to have an important impact on disease and mortality [16]. Thus, it is possible that the adverse impact of obesity is a function of both severity and duration, and that with more recent cohorts the deleterious impact of obesity on life expectancy will be observed [15]. Indeed, recent mortality statistics (2008) in the US demonstrate, for the first time in over 25 years, a slight decline in US life expectancy [17]. Nevertheless, in this same report diabetes and cardiovascular mortality rates maintain a continual decline. Furthermore, in an assessment of overweight and obesity on the risk of cardiovascular disease and mortality in middle-aged men, Arnlov et al. (2010) [18] observed a lag time of only 10 years. Additionally, the positive effects of weight loss after bariatric surgery on conditions such as diabetes, hypertension, and dyslipidemia have occurred in a much shorter period (less than two years) [19].
(7) The Obesity Paradox —
There is the “obesity paradox” in which survival from acute events such as myocardial infarction, heart failure, and dialysis for renal failure is improved in patients with overweight and obesity [20–22]. The mechanism for this observation is not known but is unlikely to be simply that more severely ill patients have lost weight on account of the severity of their illness. It is also possible that diseases such as hypertension and diabetes may be more aggressive and of a different origin in lean individuals than when they are associated with obesity. For example, among patients with a history of hypertension and coronary artery disease, Uretsky et al. (2007) found that overweight and obesity (classes I to III) were associated with a lower risk of morbidity and mortality compared with normal-weight patients, despite poorer blood pressure control [20].
—
Thus, considerations such as lag time, duration of exposure to obesity, and increasing proportions of the population with severe obesity suggest that obesity may in the future have a considerable impact on life expectancy. However there are also important reasons—improved control of hypertension, shape of BMI-mortality relationship, and body weight as a surrogate marker of lifestyle—why obesity may not be strongly linked to life expectancy, except at the extremes of the weight distribution. Rather, the principle impact of obesity may be on disability-free life expectancy. Several studies suggest an association between body weight and a higher risk of becoming disabled [23–25], although others dispute this [3, 26].
3. Conclusion
Several reasons explain why the impact of obesity on life expectancy may be more complex than is commonly recognised. It is possible that the principal impact of obesity is on disability-free life expectancy rather than on life expectancy itself. It is also possible that health and life expectancy gains could be even greater if it was not for the increasing prevalence of extreme obesity.
It is important to understand why life expectancy is generally continuing to improve despite a high and increasing prevalence of obesity. Further research in this area and careful monitoring of recent cohorts and future trends will assist policy makers with determining the most appropriate response to increasing levels of obesity. If only those with more extreme obesity are facing substantial health and mortality risks, this will help inform as to the appropriate mix of population and high-risk (targeting people already obese, or at risk of significant weight gain, e.g.) approaches to obesity reduction. If the principle impact of obesity is on disability-free life expectancy rather than on life expectancy itself, this has substantial implications for the heath of individuals and the future burden on the health care system.
References
- 1.Olshansky SJ, Passaro DJ, Hershow RC, et al. A potential decline in life expectancy in the United States in the 21st century. New England Journal of Medicine. 2005;352(11):1138–1145. doi: 10.1056/NEJMsr043743. [DOI] [PubMed] [Google Scholar]
- 2.Parikh NI, Pencina MJ, Wang TJ, et al. Increasing Trends in Incidence of Overweight and Obesity over 5 Decades. American Journal of Medicine. 2007;120(3):242–250. doi: 10.1016/j.amjmed.2006.06.004. [DOI] [PubMed] [Google Scholar]
- 3.Christensen K, Doblhammer G, Rau R, Vaupel JW. Ageing populations: the challenges ahead. The Lancet. 2009;374(9696):1196–1208. doi: 10.1016/S0140-6736(09)61460-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Stamler J. The marked decline in coronary heart disease mortality rates in the United States, 1968-1981; summary of findings and possible explanations. Cardiology. 1985;72(1-2):11–22. doi: 10.1159/000173836. [DOI] [PubMed] [Google Scholar]
- 5.Capewell S, Ford ES, Croft JB, Critchley JA, Greenlund KJ, Labarthe DR. Cardiovascular risk factor trends and potential for reducing coronary heart disease mortality in the United States of America. Bulletin of the World Health Organization. 2010;88(2):120–130. doi: 10.2471/BLT.08.057885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fox CS, Pencina MJ, Meigs JB, Vasan RS, Levitzky YS, D’Agostino RB. Trends in the incidence of type 2 diabetes mellitus from the 1970s to the 1990s: the Framingham Heart Study. Circulation. 2006;113(25):2914–2918. doi: 10.1161/CIRCULATIONAHA.106.613828. [DOI] [PubMed] [Google Scholar]
- 7.Stewart ST, Cutler DM, Rosen AB. Forecasting the effects of obesity and smoking on U.S. life expectancy. New England Journal of Medicine. 2009;361(23):2252–2260. doi: 10.1056/NEJMsa0900459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Peto R, Whitlock G, Jha P. Effects of obesity and smoking on U.S. life expectancy. New England Journal of Medicine. 2010;362(9):855–856. doi: 10.1056/NEJMc1000079. [DOI] [PubMed] [Google Scholar]
- 9.Chobanian AV. Improved hypertension control: cause for some celebration. Journal of the American Medical Association. 2010;303(20):2082–2083. doi: 10.1001/jama.2010.692. [DOI] [PubMed] [Google Scholar]
- 10.Prospective Studies Collaboration. Body-mass index and cause-specific mortality in 900,000 adults: collaborative analyses of 57 prospective studies. The Lancet. 2009;373(9669):1083–1096. doi: 10.1016/S0140-6736(09)60318-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Walls HL, Wolfe R, Haby MM, et al. Trends in BMI of urban Australian adults, 1980–2000. Public Health Nutrition. 2010;13(5):631–638. doi: 10.1017/S1368980009991455. [DOI] [PubMed] [Google Scholar]
- 12.Sturm R. Increases in morbid obesity in the USA: 2000–2005. Public Health. 2007;121(7):492–496. doi: 10.1016/j.puhe.2007.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Diehr P, Bild DE, Harris TB, Duxbury A, Siscovick D, Rossi M. Body mass index and mortality in nonsmoking older adults: the cardiovascular health study. American Journal of Public Health. 1998;88(4):623–629. doi: 10.2105/ajph.88.4.623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hernán MA, Taubman SL. Does obesity shorten life? The importance of well-defined interventions to answer causal questions. International Journal of Obesity. 2008;32(3):S8–S14. doi: 10.1038/ijo.2008.82. [DOI] [PubMed] [Google Scholar]
- 15.Lee JM, Pilli S, Gebremariam A, et al. Getting heavier, younger: trajectories of obesity over the life course. International Journal of Obesity. 2010;34(4):614–623. doi: 10.1038/ijo.2009.235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Abdullah A, Wolfe R, Stoelwinder JU, et al. The number of years lived with obesity and the risk of all-cause and cause-specific mortality. doi: 10.1093/ije/dyr018. International Journal of Epidemiology. In press. [DOI] [PubMed] [Google Scholar]
- 17.Minino A, Yu J, Kochanek K. Division of vital statistics. deaths: preliminary data for 2008. National Vital Statistics Reports. 2010 [PubMed]
- 18.Arnlov J, Ingelsson E, Sundström J, Lind L. Response to letters regarding article, "the impact of body mass index and the metabolic syndrome on the risk of cardiovascular disease and death in middle-aged men". Circulation. 2010;122(11):230–236. doi: 10.1161/CIRCULATIONAHA.109.887521. [DOI] [PubMed] [Google Scholar]
- 19.Vogel JA, Franklin BA, Zalesin KC, et al. Reduction in predicted coronary heart disease risk after substantial weight reduction after bariatric surgery. American Journal of Cardiology. 2007;99(2):222–226. doi: 10.1016/j.amjcard.2006.08.017. [DOI] [PubMed] [Google Scholar]
- 20.Uretsky S, Messerli FH, Bangalore S, et al. Obesity Paradox in Patients with Hypertension and Coronary Artery Disease. American Journal of Medicine. 2007;120(10):863–870. doi: 10.1016/j.amjmed.2007.05.011. [DOI] [PubMed] [Google Scholar]
- 21.Schmidt D, Salahudeen A. The obesity-survival paradox in hemodialysis patients: why do overweight hemodialysis patients live longer? Nutrition in Clinical Practice. 2007;22(1):11–15. doi: 10.1177/011542650702200111. [DOI] [PubMed] [Google Scholar]
- 22.Lancefield T, Clark DJ, Andrianopoulos N, et al. Is there an obesity paradox after percutaneous coronary intervention in the contemporary era? An analysis from a multicenter Australian registry. JACC. Cardiovascular Interventions. 2010;3(6):660–668. doi: 10.1016/j.jcin.2010.03.018. [DOI] [PubMed] [Google Scholar]
- 23.Walter S, Kunst A, MacKenbach J, Hofman A, Tiemeier H. Mortality and disability: the effect of overweight and obesity. International Journal of Obesity. 2009;33(12):1410–1418. doi: 10.1038/ijo.2009.176. [DOI] [PubMed] [Google Scholar]
- 24.Reynolds SL, Saito Y, Crimmins EM. The impact of obesity on active life expectancy in older American men and women. Gerontologist. 2005;45(4):438–444. doi: 10.1093/geront/45.4.438. [DOI] [PubMed] [Google Scholar]
- 25.Backholer K, Wong E, Freak-Poli R, Walls HL, Peeters A. Increasing body weight and risk of limitations in activities of daily living: a systematic review and meta-analysis. Obesity Reviews. 2012;13(5):456–468. doi: 10.1111/j.1467-789X.2011.00970.x. [DOI] [PubMed] [Google Scholar]
- 26.Vaupel JW. Biodemography of human ageing. Nature. 2010;464(7288):536–542. doi: 10.1038/nature08984. [DOI] [PMC free article] [PubMed] [Google Scholar]