

Abstract
Dengue is the most important mosquito-borne, arboviral infection found in tropical and sub-tropical climates. Clinical presentation varies from a severe flu-like illness to a potentially lethal dengue hemorrhagic fever. Dengue has been regarded as a nonneurotropic virus. However, there are reports describing neurological involvements in dengue virus infection. The neurological involvement in dengue virus infection includes encephalitis, acute disseminated encephalomyelitis, transverse myelitis, and Guillain-Barre syndrome. The neurological spectrum of dengue patients has been limited because of small number of case reports, paucity of imaging, and neurophysiologic studies. There are only a few isolated case reports and case series documenting acute pure motor quadriparesis in dengue fever. We report acute pure motor reversible quadriparesis due to hypokalemia. Clinicians in the endemic area should be aware of such association of acute pure motor reversible quadriparesis with dengue fever
Keywords: Dengue fever, flaccid paralysis, hypokalemia, quadriparesis
INTRODUCTION
Acute hypokalemic quadriparesis is an uncommon presentation of dengue fever, not yet widely recognised. Only few cases are reported from various institutes worldwide. Awareness of this condition will enable physicians to keep a possibility of hypokalemia in patients of dengue fever presenting with paresis and to manage specifically and effectively.
CASE REPORT
A 20-year-old young male was admitted to our hospital with a chief complaint of progressively increasing weakness of all the four limbs for 1 day. He had the history of high-grade fever for 5 days which responded to antipyretic with generalised body ache. The patient reported that his weakness started first from lower limbs, and within hours it progressed to involve upper limbs also. There was no history of neck pain, sensory symptoms in limbs, recent vaccination, diarrheal illness, recent vigorous exercise or heavy carbohydrate meal. On general examination, he was afebrile and rest of his vitals were normal. On neurological examination, only finding was grade 1–2/5 power in both upper and lower limb with diminished reflexes. There was no cranial nerve involvement, sensory deficit or any evidence of bladder, bowel, or bulbar dysfunction. His single breath count was 35. There was no past or family history of similar weakness or any episodic weakness. Blood investigations on admission were as follows: hemoglobin was 13.8 g/dl, total leucocyte count was 8.8 × 103/μl with 44% polymorphs, 54% lymphocytes and 2% monocytes. The platelet count was 1,00,000/mm.[1] His blood biochemistry revealed serum potassium 1.82 mmol/l, sodium 139 mmol/l, and a normal creatinine kinase value, the arterial blood gas analysis showed a pH of 7.34, bicarbonate 16.7 mmol/l and anion gap 5.1 mmol/l. His renal and thyroid function tests were completely normal, and the liver function test showed a normal serum bilirubin with SGOT and SGPT of 90 and 100 IU/l, respectively. Urine analysis showed a pH of 6 with normal specific gravity and no proteinuria or glycosuria, and spot urinary sodium potassium and calcium were within normal limits, the hospital stay was uneventful. After 7 days, a challenge test performed with heavy carbohydrates diet and strenuous exercise, followed by rest, failed to produce any weakness. For the challenge test, the patient was hospitalized, and the procedure was explained to him. An informed consent was obtained. It was undertaken in an intensive care setting. His nerve conduction velocity (NCV)/electromyography (EMG) was completely normal, ECG showed prominent U waves [Figure 1], his dengue NS1 antigen ELISA[2] as well as dengue IgM antibody test were positive. A diagnosis of dengue fever with thrombocytopenia with hypokalemic motor paralysis was made and the patient was given intravenous potassium chloride infusion. His motor power improved rapidly and at 10 h of starting treatment his power was completely normal. On the second day of treatment, his repeat serum potassium was 3.9 meq/l. The patient was not given any treatment for thrombocytopenia and was kept under observation as no signs of bleeding diathesis were present. At the end of first week, his platelet count became completely normal. The patient was discharged on 5th day of admission with advice for follow-up.
Figure 1.
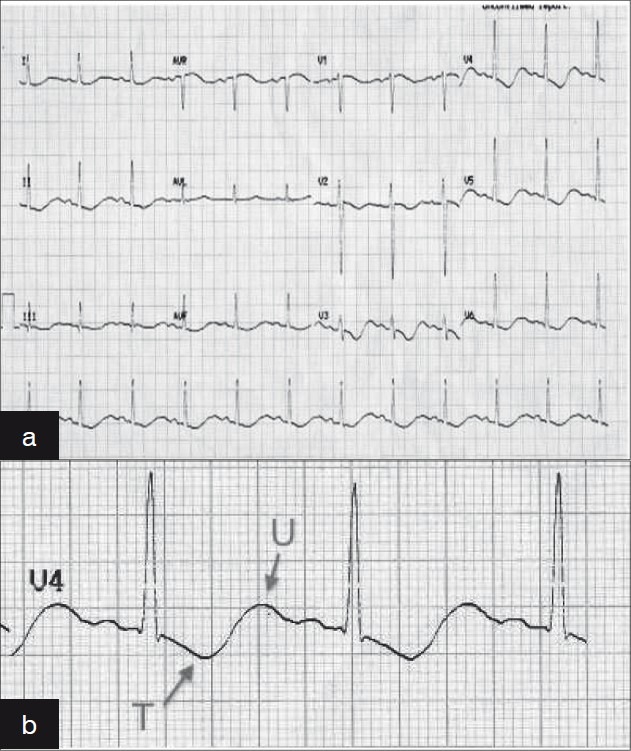
(a) ECG at the time of presentation, At the time of presentation when serum potassium is 1.82 mmol.l, Electrocardiogram revealed heart rate of 75/min with prolongation of PR interval, ST segment depression, T wave inversion and prominent U wave typical feature of Hypokalemic (b) ECG shows prominent U wave and T wave inversion, MID precordiallead of patient shows T wave inversion and prominent U waves
DISCUSSION
Dengue was regarded as a nonneurotropic virus. There are however recent reports on neurotropism or neuroinvasion of dengue virus infection.[2,3] The syndrome of acute pure motor weakness in dengue was quite characteristic and has not been comprehensively evaluated in earlier reports. The clinical picture simulated Guillain–Barre (GB) syndrome. The presence of fever at the time of weakness, normal nerve conduction studies and the absence of albumin cytological dissociation and response with potassium supplement excluded the possibility of GB syndrome.[2] Familial periodic paralysis was unlikely because there was no family history of episodic motor weakness and this being their first episode. The pathology of neurological manifestation is multiple and includes neurotropic effect of dengue virus, systemic effect of dengue infection, and immune-mediated injury.[4] Jha and Ansari[5] reported three confirmed cases of dengue infection causing acute reversible-hypokalemic pure motor quadriparesis. Gupta et al.[1] reported two confirmed cases of hypokalemic periodic paralysis precipitated by upper respiratory tract infection of viral etiology. They also observed that potassium supplementation resulted in rapid improvement of symptoms. Santos et al.[6] reported GB syndrome in the course of dengue. The clinical profile of dengue is changing, and the neurological manifestations are reported more frequently. Widodo et al.[2] observed prevalence of hypokalemia in 23% (n = 105) of the hospitalised patients with infectious disease and Kalita et al. studied 16 patients with dengue fever with quadriparesis, in seven, the pure motor quadriparesis was due to myositis.[6] Hypokalemia in association with infectious diseases, particularly in dengue fever, has been reported. Hypokalemic paralysis secondary to chikungunya fever has also been documented.[7] The putative mechanism of the hypokalemia in our patients could be either due to redistribution of potassium in cells or transient renal tubular abnormalities leading to increased urinary potassium wasting. Preliminary investigations were not suggestive of renal tubular abnormalities. However, transient self-limiting renal tubular defects secondary to infections cannot be ruled out. Increased catecholamine levels in response to stress of the infection and secondary insulin release may result in an intracellular shift of potassium and hypokalemia. Anabolic states following rapid cell re-growth in patients of pernicious anemia treated with vitamin B12 and in patients with neutropenia after treatment with a granulocyte-macrophage colony stimulating factor can result in hypokalemia due to a potassium shift into cells.[8]
ACKNOWLEDGMENT
We owe thanks to the patient and her relatives for having patience and their contribution to this undertaking.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Gupta M, Lehl SS, Singh R, Sachdev A. Hypokalemic periodic paralysis;2 novel causes. Internet J Neurol. 2009;12:1. [Google Scholar]
- 2.Widodo D, Setiawan B, Chen K, Nainggolan L, Santoso WD. The prevalence of hypokalemia in hospitalized patients with infectious diseases problem at Cipto Mangunkusumo Hospital, Jakarta. Acta Med Indones. 2006;38:202–5. [PubMed] [Google Scholar]
- 3.Kalita J, Misra UK, Mahadevan A, Shankar SK. Acute pure motor quadriplegia: Is it dengue myositis? Electromyogr Clin Neurophysiol. 2005;45:357–61. [PubMed] [Google Scholar]
- 4.Pancharoen C, Thisyakorn U. Neurological manifestations in dengue patients. Southeast Asian J Trop Med Public Health. 2001;32:341–5. [PubMed] [Google Scholar]
- 5.Jha S, Ansari MK. Dengue infection causing acute hypokalemic quadriparesis. Neurol India. 2010;58:592–4. doi: 10.4103/0028-3886.68657. [DOI] [PubMed] [Google Scholar]
- 6.Santos NQ, Azoubel AC, Lopes AA, Costa G, Bacellar A. Guillain-Barré syndrome in the course of dengue: Case report. Arq Neuropsiquiatr. 2004;62:144–6. doi: 10.1590/s0004-282x2004000100025. [DOI] [PubMed] [Google Scholar]
- 7.Rampal , Sharda M, Meena H. Hypokalemic paralysis following Chikungunya fever. J Assoc Physicians India. 2007;55:598. [PubMed] [Google Scholar]
- 8.Singer GG, Brenner BM, et al. Harrison's principles of internal medicine. 17th ed. New York: Mcgraw-Hill Companies; 2008. Fluid and electrolyte disturbances; pp. 274–85. [Google Scholar]