

Abstract
Myopia is a major public health problem pertaining to eye that entails substantial societal, personal, educational, and economical impact. Various surveys in India have found the prevalence of myopia ranging from 6.9% to 19.7%. Myopia progression is irreversible and methods for the correction of myopia are not without complications. Myopia closely resembles Timira involving first and second Patala in terms of symptoms, anatomical structures involved, and the pathogenesis of the disease. The study is aimed at evaluating the efficacy of the Akshi-Tarpana procedure with Jeevantyadi Ghrita in fresh and old myopes. A total of 54 patients (108 eyes) having myopia ≥-6 D were registered for the study and divided into two groups (Group A, Akshi-Tarpana with Jeevantyadi Ghrita, and Group B, Akshi-Tarpana with plain Go Ghrita), by stratified sampling. The procedure was done in 5 sittings of 5 days each with an equal interval of 5 days between each sitting. A total of 22 patients in Group A and 18 in Group B completed the treatment. Obtained data were statistically analyzed using a t-test and the study reveals that objectively, 09.30% and 05.55% eyes were cured, 16.28% and 02.78% markedly improved, and 34.88% and 11.11% moderately improved in Group A and B, respectively.
Keywords: Akshi-Tarpana, Jeevantyadi Ghrita, Patala, Timira
Introduction
Myopia is a major public health problem pertaining to eye that entails substantial societal, personal, educational, and economical impacts. Myopia is the state of refraction in which parallel rays of light are brought to focus in front of the retina of a resting eye.[1] Myopia is measured by the spherical power in diopters of the diverging lens needed to focus light onto the retina, which can be expressed as the spherical equivalent or refraction in the least myopic meridian.[2,3] The clinical correlates of myopia include blurred distance of vision, eye rubbing, and squinting.
Myopia is highly prevalent in our society, affecting at least 25% of the adult population in the United States[4] and is even more common in Asian countries, affecting up to 84% of adolescents.[5] Various surveys in India have found the myopia prevalence ranging from 6.9% to 19.7%.[6,7] Furthermore, its prevalence may be increasing over time as suggested by some studies in various countries including Singapore, Australia, and the United States.[8–11] Due to the significance of myopia as a global public health concern, it was chosen as a priority for Vision 2020, World Health Organization's global initiative for the elimination of avoidable blindness by year 2020.[12]
Though the modern counterpart has made tremendous and remarkable progress in the field of ophthalmology but no satisfactory and universally accepted treatment for myopia is available. Myopia progression is irreversible and there is no cure. Methods for the correction of myopia are not without complications, including corneal infections due to contact lens wear and corneal scarring and persistent corneal haze from refractive surgery.[13] Refractive surgeries for treatment of myopia are both costly and unsuitable for children's eyes and do not change axial elongation, which is the commonest source of myopia.[14] Hence, the Ayurvedic science can be explored to find a better alternative to manage this condition.
Myopia closely resembles with Timira involving first and second Patala in terms of symptoms, anatomical structures involved, and the pathogenesis of the disease. Though various drugs and local therapeutic procedures like Nasya, Anjana, Akshi Tarpana, etc., have been mentioned in Ayurvedic texts for the management of Timira, but Akshi-Tarpana is the foremost on account of its sound literary and practical evidences. Previously, many works have been carried out on the efficacy of Akshi-Tarpana in Timira (myopia) – with encouraging results but no one has conducted the study with Shodhana Nasya (as Poorva-Karma) prior to Akshi-Tarpana as indicated in all the Ayurvedic texts. In Timira (myopia), Chakshushya, Rasayana, and Tridosha mitigating action might be helpful. Ghrita is one among the best Rasayana drugs and Jivanti is one among the best Chakshushya drugs, and most of the contents of Jeevantyadi Ghrita have Tridosha pacifying action. So Jivantyadi Ghrita having all the properties was selected for the study. Also, previous study[15] reported almost equal efficacy of Akshi-Tarpana with plain Go Ghrita and medicated Ghrita in Timira (myopia). Keeping these points in view, the present clinical study was planned with following aims and objectives:
to evaluate the efficacy of Akshi-Tarpana with Jeevantyadi Ghrita and plain Go Ghrita in Timira (myopia) in fresh and old myopia and
to compare the efficacy of Akshi-Tarpana with Jeevantyadi Ghrita and plain Go Ghrita in Timira (myopia).
Materials and Methods
Patient selection
Patients attending the OPD and IPD of Department of Shalakya, IPGT and RA Hospital, with signs and symptoms of Timira (myopia) were registered irrespective of their sex, religion, occupation, education, etc. A total of 54 patients (108 eyes) were recruited for the study. Myopia was defined as a mean spherical equivalent of ≤–0.50 D, as described by Quinn et al.[16] An elaborative case-taking proforma was specially designed for the purpose of incorporating all aspects of the disease on Ayurvedic and modern parlance.
Informed consent was taken from all the registered patients for the trial.
Sampling technique
A total of 54 registered patients were divided into two groups (Group A, 28 patients; Group B, 26 patients) by a stratified sampling method in order to maintain the uniformity in both the groups in terms of dioptric power. The study was kept single blind so as to avoid any psychological effect from patient's side.
In Group A, Akshi-Tarpana was done with Jeevantyadi Ghrita[17] and in Group B, Akshi-Tarpana was done with plain Go Ghrita.[18]
Inclusion criteria
The study patients included those within the age group of 08–30 years having signs and symptoms of Timira (myopia) up to −6.0 D.
Exclusion criteria
Patients having any other known ocular pathology, e.g., cataract, corneal opacity, etc., with a history of iridocyclitis, retinal disease, etc., were excluded. Patients aged below 07 years and above 30 years and having a dioptric power more than –6 D were also excluded.
Investigations
Following investigations were carried out in order to rule out any systemic disease:
Routine hematological tests: Hb, TC, DC, ESR
Biochemical tests: Blood sugar (F), serum cholesterol
Urine test: Routine and microscopic
Stool test: Routine and microscopic
Drug selection and dosage
For the Poorva-Karma of the procedure, following drugs were used in both the groups:
Eranda Bhrishta Haritaki: 05 g with lukewarm water for 3 days.
Nasya with Krishnadya Taila: 4–8 drops per nostril for next 3 days.
For the main procedure (Akshi-Tarpana), following drugs were used:
Jeevantyadi Ghrita in Group A: Quantity sufficient
Plain Go Ghrita in Group B: Quantity sufficient
Akshi-Tarpana was carried out in 5 sittings of 5 days each, with an equal interval (noninterventional period) of 5 days between each sitting in both the groups.
The duration of the procedure was 51 days.
Follow-up was done for 1 month after completion of the course of the procedure.
Assessment criteria
Subjective
The patients were subjectively assessed based on the symptoms – Durastha Avyakta Darshana (indistinct distant vision) , Vihwala Darshana (blurred vision), Shirobhitapa (headache), Netrasrava (watering), Netrayasa (eye strain), and Netradaha (burning sensation) – by adopting the following scoring pattern:
Cured: 100% relief in signs and symptoms and no recurrence during the follow-up study.
Marked improvement: 76–99% improvement in signs and symptoms.
Moderate improvement: 51–75% improvement in signs and symptoms.
Mild improvement: 26–50% improvement in signs and symptoms.
Unchanged: Up to 25% reduction in signs and symptoms.
Objective
Unaided visual acuity (UAVA) was measured using Snellen's chart and was recorded as numerical convention and later converted into percentage as per the method of Lyle.[19] Refraction was done by using Snellen's chart:
Cured: 1 D reduction in the spherical dioptric power or complete remission.
Marked improvement: 0.75 D reduction in the spherical dioptric power.
Moderate improvement: 0.50 D reduction in the spherical dioptric power.
Mild improvement: 0.25 D reduction in the spherical dioptric power.
Unchanged: No reduction in the spherical dioptric power.
Statistical analysis
The effect of therapy in both the groups is assessed by applying t-test. The results obtained are considered highly significant for P<0.001, significant for P<0.01, and insignificant for P<0.05 or P>0.05.
Observations
Out of a total of 54 patients (108 eyes) recruited for the study, maximum patients were from the age group of 14–19 years followed by the age group of 20–25 years. A total of 81.48% patients were students. As the disease manifests in school-going children, and also, it is a proven fact that simple myopia usually begins in childhood since the eyes continue to grow during childhood, myopia almost always occurs before the age of 20 and then gets stable in adulthood.
A total of 51.85% of patients were males followed by 48.15% females. Although there is no theoretical description regarding any gender predominance in myopia, Jenson[20] in 1985 reported the female-to-male ratio as 4.4:3.6. A higher rate in females is also confirmed by results obtained from a study on Greek students having 46% females and 29.7% male students as myopic.[21] But in the present study, a slight male predominance was observed which could be a matter of chance.
A total of 94.44% patients belonged to the urban area, and according to a previous study, it was observed that in urban areas, myopia rates were higher than those in rural areas [Table 1].[22]
Table 1.
General observation-wise distribution of 54 patients of Timira – myopia
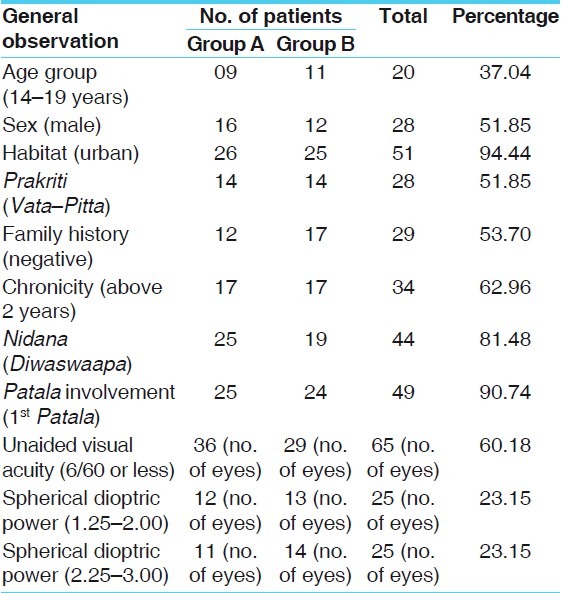
A total of 51.85% patients had Vata–Pitta Prakriti. Though, Timira (myopia) occurs due to the aggravation of Vata as depicted in Ayurvedic texts, as this sample is very small, no definite correlation between Sharira Prakriti and Timira occurrence could be established [Table 1].
It was found that 53.70% patients were having a negative family history. A total of 62.96% patients had chronicity above 2 years, 18.52% patients had chronicity between 1 and 2 years, followed by 1.85% patients having up to 1-year chronicity. Also, 16.67% patients were newly detected myopes [Table 1].
Maximum number, i.e. 81.48%, of patients were having Diwaswapa as Nidana, followed by 62.96% having Ratrijagarana; 59.26% patients had Mootravegadharana, 46.30% had Sookshmanireekshana, and 42.59% patients had Malavegadharana as their Nidana. Shoka was found in 29.63% patients, Krodha in 24.07% patients, and Klesha in 22.22% patients [Table 1].
A total of 90.74% were having the involvement of first Patala and 09.25% of the patients were having the involvement of second Patala [Table 1].
It was found that 60.18% of eyes of patients had an unaided visual acuity of 6/60 or less, 23.15% eyes had a visual acuity of 6/24–6/36, while 12.03% eyes had a visual acuity of 6/12–6/18 and only 04.63% had a visual acuity of 6/6–6/9 [Table 1].
A total of 23.15% eyes were having a myopic spherical dioptric power of 1.25–2.00 D and 2.25–3.00 D each, followed by 21.30% eyes having a dioptric power of 0.25–1.00 D, while 14.81% eyes had a dioptric power of 3.25–4.0 D and 09.26% eyes had a dioptric power of 4.25–5.00 D, and only 07.41% had a dioptric power of 05.25–6.00 D [Table 1].
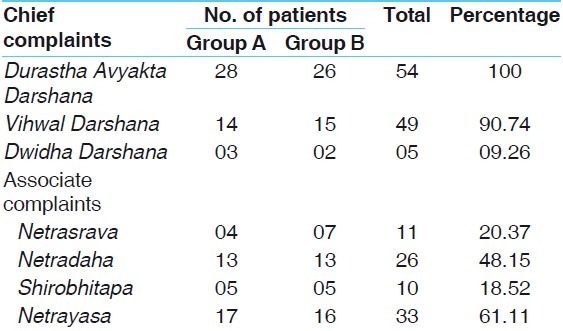
Hundred percent patients were having Durastha Avyakta Darshana (indistinct distant vision), while 90.74% patients had Vihwala Darshana (blurred vision) and only 09.26% of patients had Dwidha Darshana (diplopia) as chief complaints. A total of 61.11% patients had Netrayasa (eye strain), 48.15% patients were having Shirobhitapa (headache), 20.37% were having Netrasrava (watering), and 18.52% patients had Netradaha (burning sensation) as associated complaints [Table 2].
Table 2.
Chief complaints and associated complaintwise distribution of 54 patients of Timira – myopia
Results and Discussion
Effect of therapies on subjective symptoms
Durastha Avyakta Darshana or indistinct distant vision was relieved by 43.33% (P<0.001) in 22 patients of Group A and by 40.48% (P<0.001) in Group B. Vihwala Darshana (blurred vision) was relieved by 44.19% in Group A (P<0.001) and by 34.48% (P<0.001) in Group B [Table 3].
Table 3.
Effect of Akshi-Tarpana on chief complaints of Timira of Groups A and B
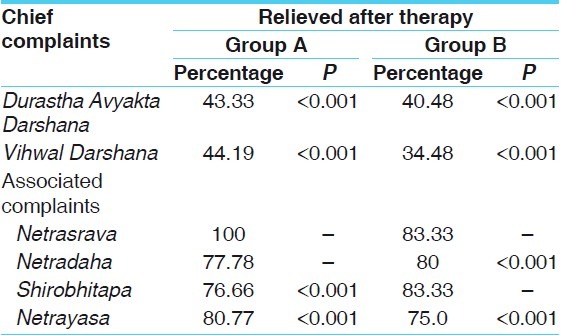
The present clinical study shows that Akshi–Tarpana with both Jeevantyadi Ghrita and Go Ghrita is statistically equally effective in treating symptoms like Avyakta Darshana and Vihwala Darshana but percentage-wise, Group A has shown better results.
In associated symptoms, Netrasrava was relieved by 100%, Netradaha by 77.78%, Netrayasa by 80.77%, and Shirobhitapa by 76.66% which are statistically significant (P<0.001) in Group A while in Group B, Netrasrava and Netradaha were relieved by 83.33%, Shirobhitapa by 80.00% and Netrayasa by 75.0% which are statistically significant (P<0.001) [Table 3].
Group A is more effective in associated symptoms of Netrasrava and Netrayasa while Group B is more effective in managing Netradaha.
Effect of therapies on clinical refraction
The dioptric power of the spherical lens was reduced by 19.13% in the right eye and 13.48% in the left eye in Group A, both the results being statistically significant (P<0.001) [Table 4].
Table 4.
Effect of Akshi-Tarpana on clinical refraction in patients of Timira of Groups A and B

The dioptric power of the spherical lens was reduced by 09.80% in the right eye and 10.27% in the left in Group B, both the results being statistically significant (P<0.001) [Table 4].
The above result shows that Akshi-Tarpana with Jeevantyadi Ghrita is more effective in the improvement of dioptric power (spherical glasses) as compared to plain Go Ghrita.
The dioptric power of the cylindrical lens was reduced by 20.45% in the right eye and 29.54% in the left in Group A, both the results being statistically insignificant (P<0.05) [Table 4].
The dioptric power of the cylindrical lens was reduced by 07.14% in the right eye and 0.00% in the left eye in Group B, both the results being statistically insignificant (P>0.05) [Table 4].
The above-mentioned results show that Akshi-Tarpana with Jeevantyadi Ghrita is more effective in the improvement of dioptric power (cylindrical glasses) as compared to plain Go Ghrita.
Effect of therapies on fresh and old myopes
The dioptric power of the spherical lens in fresh myopes showed 46.15% improvement in the right eye and 30.0% improvement in the left eye in Group A.
The dioptric power of the spherical lens in fresh myopes showed 25.0% improvement in both eyes in Group B.
The results cannot be statistically evaluated as the sample size was small (n<6) but it shows that Akshi-Tarpana with Jeevantyadi Ghrita is more effective in the improvement of dioptric power (spherical glasses) in fresh myopes as compared to plain Go Ghrita.
The dioptric power of spherical lens in old myopes was reduced by 15.69% in the right eye and 11.9% in the left eye of 18 patients of Group A, both the results being statistically significant (P<0.001).
The dioptric power of the spherical lens in old myopes was reduced by 07.87% in the right eye and 08.46% in the left eye of 15 patients of Group B, both the results being statistically significant (P<0.01). The above-mentioned results show that Akshi-Tarpana with Jeevantyadi Ghrita is more effective in the improvement of dioptric power (spherical glasses) in old myopes also as compared to plain Go Ghrita.
Subjective
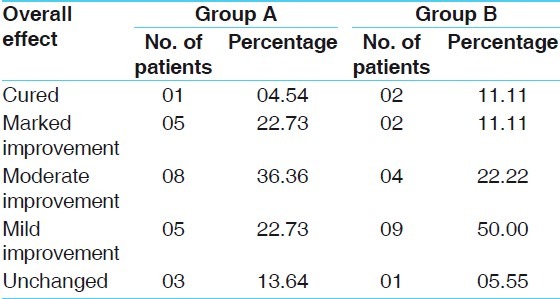
Overall effect of therapies on subjective symptoms in 40 patients of myopia (80 eyes) is as follows:
Total of 04.54% patients were cured in Group A and 11.11% in Group B. Marked improvement was seen in 22.73% patients in Group A and 11.11% in Group B. Moderate improvement was observed in 36.36% patients in Group A and 22.22% in Group B. A mild improvement was observed in 22.73% patients in Group A and 50% in Group B. No change was observed in 13.64% patients in Group A and 05.55% in Group B [Table 5].
Table 5.
Total effect of Akshi-Tarpana in subjective symptoms of patients of Timira of Groups A and B
Objective
Overall effect of therapies on objective symptoms (spherical dioptric power) in 40 patients (80 eyes) of myopia is as follows:
On assessing the results objectively on the basis of the reduction in spherical power, it was found that 09.30% patients were cured in Group A and 05.55% in Group B. A total of 16.28% patients in Group A and 02.78% patients in Group B got a marked improvement. A total of 34.88% and 11.11% patients, respectively, in Groups A and B got a moderate improvement. A mild improvement was seen in 23.25% and 44.44% patients in Groups A and B, respectively. It was found that 16.28% patients in Group A and 36.11% patients in Group B were having unchanged refractive status even after treatment [Table 6].
Table 6.
Objective assessment of the therapies in both groups of patients of Timira
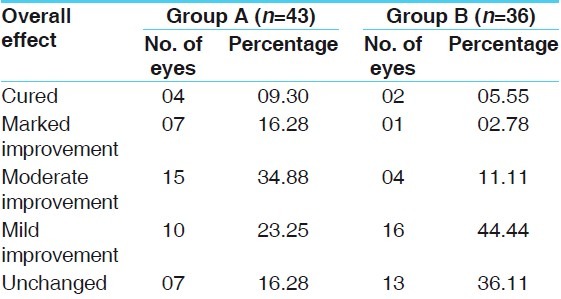
Overall effect of therapy shows that Jeevantyadi Ghrita is more effective in objective symptoms also as compared to plain Go Ghrita.
Probable mode of action of Poorva-Karma before Akshi-Tarpana
As Koshtha is the site for Pachaka Pitta and it nourishes all other Pittas (including Alochaka Pitta) at their respective sites, Kaya Shuddhi/Koshtha Shuddhi definitely breaks the Samprapti of Timira. Therefore, at least Kostha Shuddhi for 3 days is highly recommended.
Shiro Shuddhi by Nasya removes the Srotorodha and opens the channels to receive the Sneha. Eye is an organ which should be protected from vitiated Kapha. The Shiro-Shodhana definitely helps to protect the excessive vitiation of Kapha. Also, Nasya Karma is a specific treatment methodology mainly indicated for Urdhvajatrugata Vikaras in Ayurveda.
Before Nasya, Abhyanga is specifically done in Murdha Pradesha which causes vasodilatation in the skin and muscles by stimulating receptors of the sympathetic nervous system. Vasodilatation increases blood flow and helps to remove the toxic products.
Acharya Charaka has described the mechanism of Swedana Karma as it helps to dissolve Shleshma, makes the channels soft, by which Vatadi Doshas and other contents can flow through in their normal directions, and increases the secretion of vitiated Shleshma through the channel. So, due to Ushna Guna of Swedana, Kapha Dosha gets liquefied:[23]
When the lukewarm oil enters the nasal cavity, the network of Srotamsi carries the Taila towards the desired sites and cleanses the channel.
By Shodhana property of its (Krishnadya Taila) ingredients, probably removes the Ama at the cellular level and pacifies the vitiated Vata and Kapha Dosha. Due to Stroto Shodhana and Vata–Kapha Shamana, Avarana and Sanga of Vata–Kapha Dosha is removed and nutrition is brought to the respective sites.
Kapha should be controlled first; for this, Nasya is the best method and after that Akshi-Tarpana can be done for Vatashamaka properties.[24]
Probable mode of action of Akshi-Tarpana
Considering the Doshakarma, the trial drug appears to be predominantely Vatashamaka followed by Pittashamaka and Kaphashamaka (by virtue of its Rasa, Guna, Veerya, and Vipaka). Thus, the overall effect of the compound drug is Vata Pradhana Tridosha Shamaka and hence it disintegrates the pathology of Timira, which is also Vata Pradhana Tridoshaja in its manifestation.
The Ghrita has the quality of trespassing into minute channels of the body. Hence, when applied in the eye, it enters deeper layers of Dhatus and cleanses every minute part of them.
The lipophilic action of Ghrita facilitates the transportation of the drug to the target organ and finally reaching the cell, because the cell membrane also contains lipid. This liphophilic nature of Ghrita facilitates the entry of drug into the eyeball through the corneal surface since the corneal epithelium is permeable to lipid-soluble substances and lipid-soluble substances cross the corneal epithelium irrespective of their molecular size.
Moreover, Ghrita preparation used in Akshi-Tarpana is in the form of suspension containing different particles of the drugs and the particles do not leave the eye as quick as a solution. Tissue contact time and bioavailability is more and hence therapeutic concentration can be achieved by Akshi-Tarpana.
This facilitates the action of drug by two ways – first by allowing more absorption of the drug by the corneal surface and secondly by exerting direct pressure upon the cornea. There may be changes in the refractive index of the cornea causing less convergence of light rays.
Conclusion
Maximum patients were from the school-going age group and having a habit of working on computers and studying for long time, supporting the theory which states that excessive use of accommodation will lead to the development of myopia.
In few patients, even if no change in clinical refraction was observed, still the overall clarity of vision was found to be improved and asthenopic symptoms like Netrayasa, Netrasrava, Netradaha, etc., were remarkably reduced.
In the reduction of the dioptric power, Jeevantyadi Ghrita has shown better results than plain Go Ghrita. Newly detected cases and patients having a dioptric power less than –3.0 D were found to have better results.
The duration of the treatment is short; hence, for reaching at any definite conclusion, further long-duration studies are needed. Since the study has shown interesting results, it is recommended that the study should be carried out on a large number of patients with longer duration to evaluate and analyze the results.
References
- 1.Curtin BJ. The myopias: Basic science and clinical management. Philadelphia, PA: Harper and Row; 1985. [Google Scholar]
- 2.Curtin B. Topics to be considered when establishing standards for clinical myopia studies. Acta Ophthalmol Suppl. 1988;185:61–2. doi: 10.1111/j.1755-3768.1988.tb02665.x. [DOI] [PubMed] [Google Scholar]
- 3.Angle J, Wissmann DA. The epidemiology of myopia. Am J Epidemiol. 1980;111:220–8. doi: 10.1093/oxfordjournals.aje.a112889. [DOI] [PubMed] [Google Scholar]
- 4.Sperduto RD, Seigel D, Roberts J, Rowland M. Prevalence of myopia in the United States. Arch Ophthalmol. 1983;101:405–7. doi: 10.1001/archopht.1983.01040010405011. [DOI] [PubMed] [Google Scholar]
- 5.Lin LL, Shih YF, Tsai CB, Chen CJ, Lee LA, Hung PT, et al. Epidemiologic study of ocular refraction among schoolchildren in Taiwan in 1995. Optom Vis Sci. 1999;76:275–81. doi: 10.1097/00006324-199905000-00013. [DOI] [PubMed] [Google Scholar]
- 6.Jain IS, Jain S, Mohan K. The epidemiology of high myopia—changing trends. Indian J Ophthalmol. 1983;31:723–8. [PubMed] [Google Scholar]
- 7.Mohan M, Pakrasi S, Zutshi R. Myopia in India. ActaOphthalmolSuppl. 1988;185:19–23. doi: 10.1111/j.1755-3768.1988.tb02655.x. [DOI] [PubMed] [Google Scholar]
- 8.Rajan U, Tan FT, Chan TK. Increasing prevalence of myopia in Singapore school children. In: Chew SJ, Weintraub J, editors. Proceedings of the Fifth International Conferenceon Myopia, Toronto, Ontario, Canada, June 22-24, 1994. New York: Myopia International Research Foundation; 1995. pp. 41–6. [Google Scholar]
- 9.Wensor M, McCarty CA, Taylor HR. Prevalence and risk factors of myopia in Victoria, Australia. Arch Ophthalmol. 1999;117:658–63. doi: 10.1001/archopht.117.5.658. [DOI] [PubMed] [Google Scholar]
- 10.Wang Q, Klein BE, Klein R, Moss SE. Refractive status in the Beaver Dam Eye Study. Invest Opthalmol Vis Sci. 1994;35:4344–7. [PubMed] [Google Scholar]
- 11.Mutti DO, Zadnik K. Age-related decreases in the prevalence of myopia: Longitudinal change or cohort effect? Invest Ophthalmol Vis Sci. 2000;41:2103–7. [PubMed] [Google Scholar]
- 12.McCarty CA, Taylor HR. Myopia and vision 2020. Am J Ophthalmol. 2000;129:525–7. doi: 10.1016/s0002-9394(99)00444-4. [DOI] [PubMed] [Google Scholar]
- 13.Ruben M, Khoo CY. Contact lenses: Medical aspects. Singapore: PG Publishers; 1989. [Google Scholar]
- 14.Norton TT. Animal models of myopia: Learning how vision controls the size of the eye. ILAR J. 1999;40:59–77. doi: 10.1093/ilar.40.2.59. [DOI] [PubMed] [Google Scholar]
- 15.Ashu Vinayaka, Manjusha R. A clinical study on the efficacy of Tarpana and ShatavaryadiChurna in the management of Timirawsr to Myopia. I. P. G. T. and R. A. 2004 [Google Scholar]
- 16.Walline JJ, Zadnik K, Mutti DO. Validity of surveys reporting myopia, astigmatism and presbyopia. Optom Vis Sci. 1996;73:376–81. doi: 10.1097/00006324-199606000-00004. [DOI] [PubMed] [Google Scholar]
- 17.Vagbhata, Ashtanga Hridaya – Sarvanga Sundari Comm. 02-03. Vol. 13. Varanasi: Chaukhambha Surbharti Prakashana; 2002. pp. 818–9. [Google Scholar]
- 18.Sushruta, Sushruta Samhita Dalhana Comm. -Nibandhasangraha. 07. Vol. 18. Varanasi: Chaukhambha Surbharati Prakashan; 2003. p. 633. [Google Scholar]
- 19.Keith LT, Cross AG, Cook CAG, editors. May and Worth's manual of diseases of eye. New Delhi: CBS Publication; 1985. [Google Scholar]
- 20.Jenson HE. Vision and refraction of school children.Acta. Opthalmalogy. 1985;63(Suppl):173–83. [Google Scholar]
- 21.Mavracanas TA, Mandalos A, Peios D, Golias V, Megalou K, Gregoriadou A, et al. Prevalence of myopia in a sample of Greek students. Act Ophthalmol Scand. 2000;78:656–9. doi: 10.1034/j.1600-0420.2000.078006656.x. [DOI] [PubMed] [Google Scholar]
- 22.Saw SM, Hong RZ, Zang MZ, Fu ZF, Ye M, Tan D, et al. “Near work activity and Myopia in rural and urban school children in China”. J Paediatr Ophthalmol Strabismus. 2001;38:149–55. doi: 10.3928/0191-3913-20010501-08. [DOI] [PubMed] [Google Scholar]
- 23.Chikitsasthana. 71-76. Vol. 17. New Delhi: Rashtriya Sanskrit Sansthan; 2006. Agnivesha, Charak Samhita. [Google Scholar]
- 24.Shanthakumari PK. A textbook of ophthalmology in Ayurveda. 1st ed. Thiruvananthapuram: Matha Ayurveda Eye Hospital, Jayaprakash Lane, Kudappanakunnu; 2002. [Google Scholar]