

Abstract
Studies of retrograde amnesia are reviewed. First, the issues of temporal gradients of retrograde amnesia are discussed. Second, the question of the anatomical substrates of this syndrome are considered. Finally, some evidence for fractionation of different classes of memoranda within the retrograde time period are presented.
My interest in retrograde memory loss has been rekindled recently by the evidence of different patterns of preserved and impaired knowledge of events, people, and words acquired before the onset of the amnesic syndrome. It now appears that retrograde impairments like anterograde impairments are not global but fractionate. It is the evidence of such fractionations that have far-reaching theoretical implications. But first, a brief account of some “remote” experiments will provide a framework for discussing these developments.
The normal individual is able to maintain a constantly changing and updated record of salient personal and public events. It is this record that is impaired in the amnesic patient. Some degree of retrograde amnesia, the loss of memory for events antedating the onset of illness, has been a constant feature though even this “fact” has recently been challenged (1). Estimates of the duration of retrograde defects have been very variable. Very long periods of retrograde amnesia encompassing in some instances entire lifespans have been reported. These long periods of retrograde amnesia have presented both the psychologist and neurologist alike with a conundrum that was formulated in Ribot’s law (2): “The dissolution of memory is inversely related to the recency of the event.” Thus, recent memories are held to be more vulnerable than remote memories. Indeed in our culture it is a generally held belief that remote memories are better recalled than more recent memories in older people. Despite the formality of Ribot’s law and despite the theoretical importance of the existence of retrograde defects, the evidence for many years was based on mere anecdote.
We therefore decided to attempt to devise objective and quantitative measures that compared memory for recent and remote events. Everyone is exposed through the media of newspapers, radio, and television to a continuing series of ephemeral happenings that provide a source of common experience. In our original experiment, we assessed memory for events spanning a 30-year period using a verbal format and also memory for famous faces. We tested both recall and recognition in a very large group of normal subjects from each decade of adult life (3).
Briefly, we found clear-cut forgetting curves over time for both events and faces for all the age groups sampled. The time- and age-related functions on both the recall and recognition versions of the famous faces test were particularly striking. Contrary to received wisdom, there was no suggestion whatever of relative sparing of old memories in the older age groups as compared with younger subjects. The performance of a small group of amnesic patients tested on these original questionnaire type tests was gravely impaired at all time periods sampled and, as was observed with the older subjects, there was no hint of sparing of remote memories (4). Paradoxically, the introduction of quantitative methods succeeded in initiating controversy rather than solving a problem. Two debates ensued: (i) there was the issue of temporal gradients and (ii) there was the issue of whether there was more than one type of amnesic.
Our original demonstration (3) that the duration of a retrograde memory deficit might be lifelong without any sparing of the most remote events was criticized on the grounds that our patients were so impaired that we had merely recorded “floor” effects. It was suggested that if we had used easier tasks evidence of a temporal gradient would be obtained. However, in my view, good levels of performance for old memories can only be achieved by abandoning any attempt to match for salience. Some studies have deliberately chosen test items that normal subjects can perform at an 80% level at all time periods sampled. This results in memory for ephemeral contemporary events being contrasted with, say, household names such as Marilyn Monroe. On such tests, there is indeed evidence of temporal gradients in amnesic patients. This, I would argue, is an artifact of item selection. I would attribute evidence of a temporal gradient to a shift from accessing episodic memory to accessing factual knowledge. Here I make the assumption without reviewing the supporting evidence that there is a double dissociation between deficits in factual knowledge in patients with neocortical lesions and episodic memory in patients with an amnesic syndrome (5). Some support for the validity of this contention derives from testing teenagers who could be expected to know items that probed factual knowledge of the culture but fail on items that probed episodic events. In our original studies, a group of 50 teenagers were tested on our remote memory tests. As predicted, their performance was very poor for all time periods sampled other than the contemporary events (3). Indeed, I would suggest that the relative contribution of episodic memory and factual knowledge can be estimated by recording the performance of teenagers of these types of test.
I turn now to anatomical considerations. It has been suggested that global amnesia following bilateral lesions of the medial surface of the temporal lobe differs from lesions in the diencephalon. More specifically, it has been suggested that long periods of retrograde amnesia are characteristic of amnesics with diencephalic lesions. In contrast, the medial temporal lobe cases have a disproportionately severe anterograde amnesia, sparing to some extent retrograde memories (6, 7). I do not agree; in my experience, both types of amnesic can have a dense retrograde amnesia, one that appears to be lifelong.
I shall review briefly two densely amnesic patients, both of whom came to autopsy, to illustrate this point.
Patient 1.
E.A. (born 1907) was a right-handed bricklayer who developed an acute Korsakoff psychosis due to alcohol in 1962.
He died in 1976. At autopsy, marked gliosis, shrinkage, and discoloration bilaterally in the medial nuclei of the mammillary bodies were demonstrated. In addition, there was a thin band of gliosis bilaterally between the subependymal zone and the medial dorsal nucleous of the thalamus. No other abnormalities of note were observed. [For a more detailed report, see Mair et al. (8).] E.A. was intellectually intact apart from his dense amnesic syndrome. His verbal and performance IQs were within the average range and he scored at a chance level on a recognition memory test for words and faces (Table 1). He was tested on our original retrograde memory questionnaires. His recall of both events and faces was virtually obliterated for all time periods sampled. On the recognition versions of the tasks, his performance was close to chance again for all time periods sampled. His scores, together with a contemporary-aged matched control group, on the famous faces test are given in Fig. 1.
Table 1.
Intelligence and memory test scores
| Patient 1 (E.A.) | Patient 2 (N.T.) | Patient 3 (R.F.R.) | Patient 4 (P.S.) | |
|---|---|---|---|---|
| WAIS/WAIS-R | ||||
| Verbal IQ | 107 | 103 | 128 | 96 |
| Performance IQ | 101 | 99 | 110 | 90 |
| Recognition Memory Test (ref. 9) | ||||
| Words (n = 50) | 29 (<1%) | 35 (<5%) | 31 (<1%) | 23 (<1%) |
| Faces (n = 50) | 27 (<1%) | 25 (<1%) | 32 (<1%) | 27 (<1%) |
Figure 1.
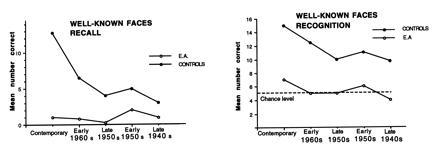
Performance of patient 1 on test of memory for faces as a function of time period sampled.
Patient 2.
N.T. (born 1907) was a right-handed housewife. She underwent a right temporal lobectomy in 1961 for the treatment of intractable epilepsy.
She died in 1986 at the age of 79. At autopsy a sclerotic lesion of the unoperated left hippocampus was found. At all levels, CA2 was almost totally depleted of neurons. Cells of CA1 were relatively preserved and in CA3 and CA4 were much reduced in number. Some atrophy of the right mammillary body was considered to be secondary to the lobectomy. [For a more detailed report see Warrington and Duchen (10).]
Although cognitively still intact postoperatively, she became densely amnesic. Her verbal and performance IQ scores were within the average range and she scored below 5% on both the verbal and visual versions of the recognition memory test (see Table 1). On the original retrograde memory questionnaire, her performance was very similar to that of E.A. the patient with mammillary body atrophy. On both of the recall versions of the test she scored at “floor” level. On the recognition versions, her scores were close to chance on all time periods sampled. Her scores, together with a contemporary-aged matched control group, are given in Fig. 2.
Figure 2.
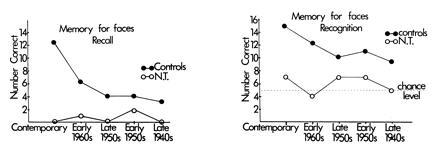
Performance of patient 2 on test of memory for faces as a function of time period sampled. [Reprinted from ref. 10. Copyright (1992), with kind permission from Elsevier Science Ltd, The Boulevard, Langford Lane, Kidlington OX5 16B, United Kingdom.]
These two patients, E.A. and N.T., were very similar in their pattern of cognitive performance. Both were intellectually intact and had a dense amnesic syndrome with the retrograde component appearing to be global and lifelong. Yet they were dissimilar anatomically; E.A. was a “good” example of amnesia arising from a diencephalic lesion and N.T.’s amnesia resulted from a very circumscribed lesion in the hippocampus. It is my contention that these two patients provide good evidence that temporal lobe amnesics and diencephalic amnesics do not necessarily differ.
It is now well-established that anterograde memory deficits are complex both in terms of what type of memories are preserved and lost and also in terms of the precise method of testing retention. It now appears that this is also the case for retrograde memory deficits. I shall describe two case reports in which unexpected dissociations were observed.
Patient 3.
R.F.R. (born 1932) was a 54-year-old police officer in whom a herpes simplex encephalitis was diagnosed in 1985. A computed tomography scan demonstrated bilateral medial temporal lobe lesions and more extensive damage in the right temporal lobe. When he recovered from the acute phase of the illness, he had a dense anterograde and retrograde amnesia. His performance on cognitive tasks that did not have a memory component was reasonably competent (see Table 1). In contrast, his performance on standard memory tests was totally defective. [For more detailed accounts of this case, see Warrington and McCarthy (11) and McCarthy and Warrington (12).]
His autobiographical knowledge was extremely sparse. He was asked to write his own life history given four headings as prompts on seven consecutive occasions. These accounts were skeletal and repetitive. For example, at his first attempt to describe his service career, he wrote “I was a regular, short-service airman with the Royal Air Force, attached to the Royal Air Force Photographic Intelligence Section. I spent most of my service time in the Middle East. I served a total of just under 4 years”. Each successive attempt was almost identical and at his fifth attempt he wrote “I was a short-term regular serviceman with the Royal Air Force serving as an ‘intelligence photographer,’ mainly in the Middle East.”
We used the Crovitz technique to elicit evidence of episodic memory (13). I think it is fair to say that at most three of his responses could be judged a true memory of an episode from his past. His memory for public events was as bad; on a 20-item questionnaire, he gave only one adequate response, whereas a small matched control group obtained a mean score of 15 correct.
R.F.R. was also tested on a subset of our original famous faces stimuli. The recognition version of this test required him to match one of three equally famous names to the face. His performance was very defective when compared with that of the contemporary controls. His total recall score across the three time periods sampled (maximum score of 45) was 3, whereas a matched control group achieved a mean score of 24.5. However, strikingly different results were obtained when his memory for famous names was tested using cuing techniques. R.F.R. was first asked to name 45 personalities famous from the 1960s through the 1980s; when unable to do so, he was given the individual’s forename and the initial letter of the surname. Subsequently, he was asked to generate or guess the individual name from the verbal cue alone. The remarkable finding was that despite his grave failure on the naming task, his scores on the photograph and cue condition was within the normal range and actually better than the controls with the verbal cue alone (Table 2). Further evidence of an intact vocabulary for famous names and famous faces was obtained from a familiarity judgement test. A famous face was paired with two similar nonentities and the famous individual’s name was paired with two similar but nonfamous names (e.g., Ian Paisley, Frank Smith, Stan Hughes). R.F.R.’s performance was at the lower limits of normal on the visual version of this task and he made only one error on the verbal version. This result stands in striking contrast to his inability to even match a face to one of three names (Table 3).
Table 2.
Naming and name completion (R.F.R.)
| Contemporary
|
Mid
1970s
|
Late 1960s
|
||||
|---|---|---|---|---|---|---|
| R.F.R. | Controls | R.F.R. | Controls | R.F.R. | Controls | |
| Naming photograph with photograph | 0 | 9 | 1 | 7 | 1 | 6 |
| Name completion with photograph | 11 | 14 | 9 | 11.3 | 7 | 11.4 |
| Name completion without photograph | 12 | 8.7 | 13 | 6.8 | 11 | 5.5 |
Maximum = 15. Number correct (R.F.R.) and mean number correct (Controls).
Table 3.
Familiarity judgements: Visual version
| Time period
|
||
|---|---|---|
| 1908–1985 | 1970–1980 | |
| Controls | 13 | 14 |
| R.F.R. | 13 | 12 |
Maximum = 15. Number correct (R.F.R.) and mean number correct (Controls).
Two other aspects of R.F.R.’s retrograde memory are of interest. First, R.F.R. had a good vocabulary for “new” words. He was able to provide very adequate definitions of words that have come into the British vocabulary within the last 20 years—the period for which he was densely amnesic—for example, IRA, AIDS, and Thatcherism. He made only one error in defining 50 new words.
Despite good evidence of a well-preserved name and face vocabulary that could be elicited with cued recall and familiarity judgement procedures, there was no evidence that he had any knowledge of the events in which the names were embedded. This was observed even when the event must have been the sole opportunity for acquiring the name in the first place (e.g., Who was Yvonne Fletcher? What happened to Yvonne Fletcher?). We contrasted his ability to recognize the defining attributes of people with the defining attributes of the events that made them notable. There were 18 “Who was?” questions and 18 matched “What happened?” questions. He obtained a creditable score of 14 of 18 on the “Who was?” questions and 7 of 18, a chance score, on the “What happened?” question. It should be emphasized that these were not intrinsically famous proper names but had merely become known for their role in an ephemeral event.
Patient 4.
The last patient I want to discuss was reported recently by Hodges and McCarthy (14). Their patient, P.S. (born 1922), was a 67-year-old garage proprietor. In 1989, he suffered a bilateral thalamic stroke. Although densely amnesic, he was intellectually intact (see Table 1). His belief or contention that he was on shore leave from active service in the navy during World War II was especially striking. His autobiographical account of events was sparse and somewhat inaccurate. The Crovitz technique in which autobiographical events were probed with 15 key words did not produce a single specific episode. He made numerous and major errors in identifying photographs of friends and relations. He was probed about 12 major family events from three decades (1960s–1980s) and his responses were all either incorrect or frankly confabulatory.
His memory for public events and famous people was by comparison well-preserved. Although he had difficulty in producing the names of a set of 72 famous faces, his ability to identify them and recognize them from three choices was reasonably good and well within the control range. He was subsequently asked to give a verbal description of these individuals’ names (e.g., describe Michael Heseltine) and for 60 of these 72 names he was able to provide accurate and detailed responses. He also performed at a very high level on a face and name familiarity task. Although his ability to date the period of their fame was poor, his performance was remarkably good when required to rank sets of three personalities from the most contemporary to the least contemporary. This evidence of good memory for personalities did not generalize other domains of public knowledge. His recognition of true and false events that were not directly related to an individual (e.g., Berlin airlift) was only just above chance.
Hodges and McCarthy (14) summarize their findings as follows: “Our patient P.S. shows material specificity in his retrograde amnesia, that is, his amnesia is more pronounced for some types of information than others. Personally relevant information and autobiographical knowledge appear to be more severely affected than the knowledge of famous people and public events.”
I have tried to present a chronological account, albeit from a personal perspective of the developments in our understanding of retrograde amnesia, from the time that it attracted clinical observation, until now, that has become the subject of sophisticated experimentation. The first simple recall and recognition tasks have led to more complex manipulations of the memoranda being probed. Thus, amnesia for people depends not only on how it is tested but also on who is being remembered. Retrograde amnesia can no longer be viewed as a global, all-encompassing deficit. Apart from the major dissociation between episodic memory and semantic memory, we now have evidence of two further dissociations within the domain of episodic memory. The dissociation between people and events has been documented in patient 3 (R.F.R.) and the dissociation of personal and public events in patient 4 (P.S.). The architecture of past memories is being revealed by patients with retrograde amnesic impairments.
Footnotes
The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. §1734 solely to indicate this fact.
References
- 1.Siegert R J, Warrington E K. Cortex. 1996;32:177–185. doi: 10.1016/s0010-9452(96)80026-8. [DOI] [PubMed] [Google Scholar]
- 2.Ribot T A. The Diseases of Memory. New York: Appleby; 1882. [Google Scholar]
- 3.Warrington E K, Sanders H I. Q J Exp Psychol. 1971;23:423–431. doi: 10.1080/14640747108400254. [DOI] [PubMed] [Google Scholar]
- 4.Sanders H I, Warrington E K. Brain. 1971;94:661–668. doi: 10.1093/brain/94.4.661. [DOI] [PubMed] [Google Scholar]
- 5.Warrington E K. Br J Clin Psychol. 1986;25:1–12. [Google Scholar]
- 6.Squire L R. In: Neuropsychological Assessments of Neuropsychiatric Disorders. Grant I, Adams K M, editors. New York: Oxford Univ. Press; 1986. pp. 268–299. [Google Scholar]
- 7.Parkin A J. Cortex. 1984;20:479–508. doi: 10.1016/s0010-9452(84)80053-2. [DOI] [PubMed] [Google Scholar]
- 8.Mair W G P, Warrington E K, Weiskrantz L. Brain. 1978;102:749–783. doi: 10.1093/brain/102.4.749. [DOI] [PubMed] [Google Scholar]
- 9.Warrington E K. Recognition Memory Test. Windsor, England: NFER-Nelson; 1984. [Google Scholar]
- 10.Warrington E K, Duchen L W. Neuropsychologia. 1992;30:437–450. doi: 10.1016/0028-3932(92)90091-y. [DOI] [PubMed] [Google Scholar]
- 11.Warrington E K, McCarthy R A. In: Diseases of the Nervous System. 2nd Ed. Asbury A K, McKhann G M, McDonald W I, editors. Philadelphia: Saunders; 1992. pp. 718–728. [Google Scholar]
- 12.McCarthy R A, Warrington E K. Neuropsychologia. 1992;30:633–644. doi: 10.1016/0028-3932(92)90068-w. [DOI] [PubMed] [Google Scholar]
- 13.Crovitz H F, Schiffman H. Bull Psychonom Soc. 1974;4:517–518. [Google Scholar]
- 14.Hodges J R, McCarthy R A. Brain. 1993;116:921–940. doi: 10.1093/brain/116.4.921. [DOI] [PubMed] [Google Scholar]