

Abstract
WEBSITE FEATURE
A 53-year-old woman who had undergone bioprosthetic aortic valve replacement 1 year earlier presented with altered mental status. Cardiovascular auscultation revealed holosystolic and holodiastolic murmurs at the left parasternal border. Transthoracic echocardiography revealed normal chamber sizes, a left ventricular (LV) ejection fraction of 0.75, and a turbulent jet from the LV outflow tract to the right atrium (RA) through a Gerbode-type defect just below the aortic valve (Fig. 1). Color-flow Doppler echocardiography revealed a jet velocity of 6 m/s with a peak gradient of 144 mmHg, consistent with a restrictive defect (Figs. 2 and 3). Moderate paravalvular insufficiency was detected, and an eccentric regurgitant jet, directed toward the Gerbode defect, entered the RA during diastole (Fig. 4A). Because aortic diastolic pressure is higher than RA pressure, left-to-right shunting across the defect was seen during both systole and diastole (Fig. 4B). The small defect required no surgical intervention.

Fig. 1 Two-dimensional transthoracic echocardiograms show a Gerbode defect (arrows) in A) apical 4-chamber and B) subcostal views.
LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle

Fig. 2 Two-dimensional color-flow Doppler echocardiograms show blood flow during systole from the left ventricle to the right atrium through the Gerbode defect (arrows) in A) apical 4-chamber and B) subcostal views.
LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle
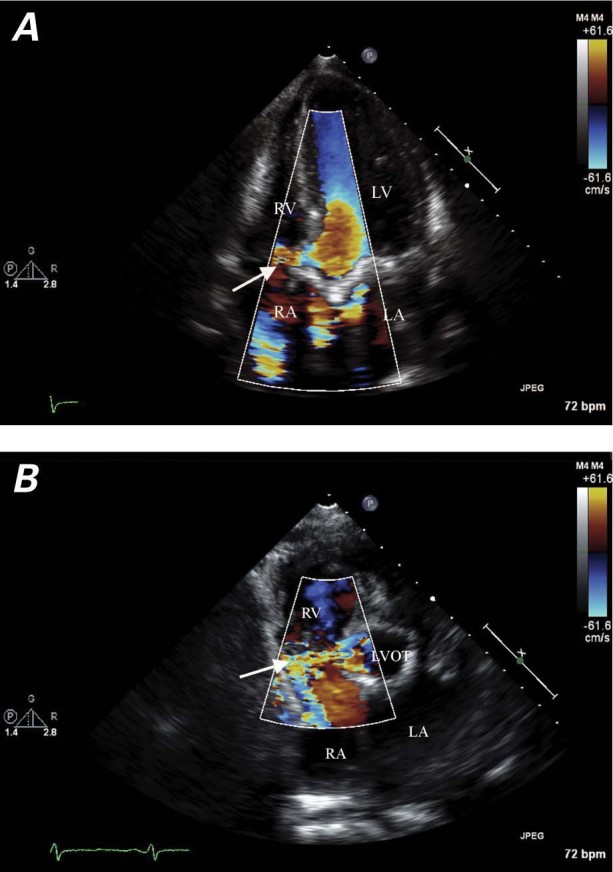
Fig. 3 Color-flow Doppler echocardiograms show blood flow through the Gerbode defect (arrows) A) from the left ventricle to the right atrium (2-dimensional apical 5-chamber view) and B) from the left ventricular outflow tract to the right atrium (parasternal short-axis view).
LA = left atrium; LVOT = left ventricular outflow tract; RA = right atrium; RV = right ventricle
Real-time motion images are available at www.texasheart.org/journal.
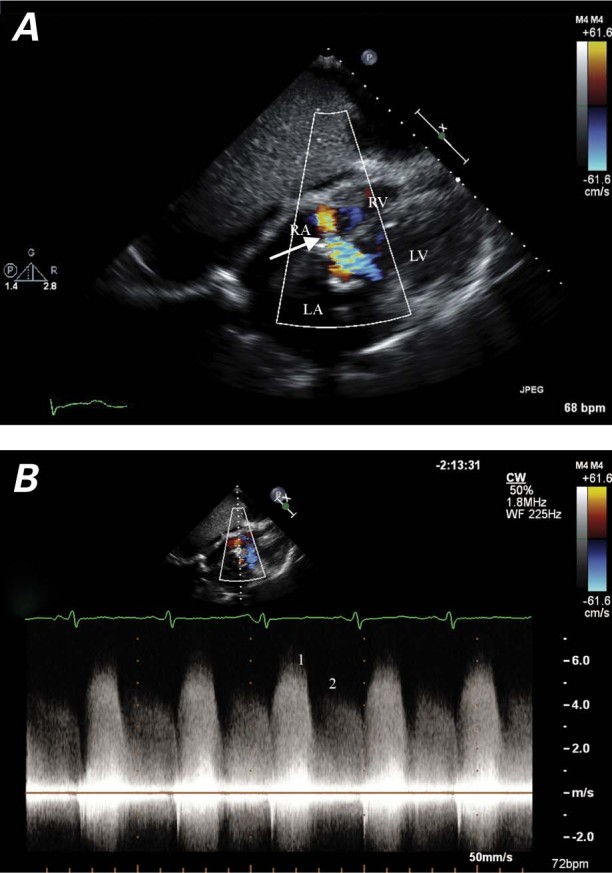
Fig. 4 A) Color-flow Doppler echocardiogram (subcostal view) shows an aortic-insufficiency jet entering the right atrium through the Gerbode defect (arrow) during diastole. B) Continuous-wave Doppler echocardiogram through the Gerbode defect shows a higher velocity of flow entering the right atrium during systole (1), and a lower velocity of aortic-insufficiency flow entering during diastole (2).
LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle
Comment
A Gerbode defect (LV–RA communication) is possible because the tricuspid valve is apical in relation to the mitral valve.1 Acquired causes of Gerbode defect include valve replacement, blunt trauma, infective endocarditis, myocardial infarction, and postsurgical repair of ventricular septal defects.2,3 Shunting across a Gerbode defect occurs mainly in systole, because LV systolic pressure is much higher than RA pressure; in diastole, LV pressure is only slightly higher.3 The unusual finding in our patient was the eccentric aortic-insufficiency jet directed toward the Gerbode defect. The left-to-right shunt was physiologically similar to a sinus of Valsalva aneurysm rupture that results in aortic–RA shunting throughout systole and diastole.
Supplementary Material
Footnotes
Address for reprints: Ajay Vallakati, MD, 1016 – 50th St., Apt. E, Brooklyn, NY 11219, E-mail: ajayvhs@yahoo.com
References
- 1.Pursnani AK, Tabaksblat M, Saric M, Perk G, Loulmet D, Kronzon I. Acquired Gerbode defect after aortic valve replacement. J Am Coll Cardiol 2010;55(25):e145. [DOI] [PubMed]
- 2.Moaref AR, Aslani A, Zamirian M, Sharifkazemi MB. Left ventricular to right atrial communication (Gerbode-type defect) after mitral valve replacement. J Am Soc Echocardiogr 2008;21(4):408.e1–2. [DOI] [PubMed]
- 3.Silbiger JJ, Kamran M, Handwerker S, Kumar N, Marcali M. The Gerbode defect: left ventricular to right atrial communication-anatomic, hemodynamic, and echocardiographic features. Echocardiography 2009;26(8):993–8. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.