

Abstract
Objective
The purpose of this case report is to describe management and outcomes of a patient with scoliosis.
Clinical Features
A 9-year-old female patient with a double curve pattern with Cobb angles of 18° and 24° (thoracic/thoracolumbar) compatible with scoliosis presented for physical therapy treatment.
Intervention and Outcome
Physiotherapy treatment with a combination of manipulative and rehabilitation techniques was used. After finishing the treatment, the patient had Cobb angles of 7° and 11°, an improvement of 55% and 54%, respectively. After 6 months, these effects were maintained, as the patient had Cobb angles of 11° and 11°. The clinical appearance of the patient improved after the course of care. The patient was evaluated for psychological outcomes by applying the following tests: Scoliosis Research Society 22, Bad Sobernheim Stress, and the Brace Questionnaire The patient had the maximum score in all tests at the conclusion of therapy.
Conclusion
The patient responded favorably to manipulative and rehabilitation techniques. At the end of care, the patient did not show psychological sequelae with selected outcome measures.
Key indexing terms: Scoliosis, Posture, Physical therapy, Spinal curvatures
Introduction
Adolescent idiopathic scoliosis, the most common form of scoliosis, is a structural 3-dimensional deformity of the spine and trunk that occurs in otherwise healthy children during puberty.1 Curvatures less than 10° are viewed as a variation of normal, as those curves have little potential for progression.2,3 Idiopathic scoliosis is estimated to affect about 2% to 3% of young females.1,4-6
The conventional treatment of a child or an adolescent with idiopathic scoliosis often lasts months or years.7 Not only does the disease produce a visible deformity of the body, but also the treatment itself may cause psychological stress and induce stress reactions.7 Wearing a corrective brace at school or outside home is the reason for both physical and psychological discomfort because there is still an insufficient level of acceptance of such a treatment at school society.7 Outcomes from psychosocial and health-related quality of life (QoL) studies indicate that body image is a complex and significant issue for patients with scoliosis and their clinicians.8 In patients with adolescent idiopathic scoliosis, the prevalence of associated psychological disorders may be as high as 19%.9,10
Therefore, scoliosis is currently recognized as an important risk factor for psychological discomfort and poor QoL, especially in brace-treated patients.3,9,11-13 However, conservative treatment may also significantly impact patients’ psychological well-being and negatively affect their QoL.3,9 To evaluate the QoL of the patients, Weiss et al constructed 2 questionnaires designated to assess the stress induced by the deformity (Bad Sobernheim Stress Questionnaire [BSSQ]-Deformity) as well as by the treatment with a brace (BSSQ-Brace).7 Similarly, other questionnaires have been proposed, specifically targeted to scoliotic populations, including the Scoliosis Research Society 22 (SRS-22)14 and the Brace Questionnaire (BrQ).15 By using these tools, we evaluated the patient's psychological outcome after the treatment.
Previous authors have investigated the effectiveness of various physiotherapeutic modalities in the treatment of scoliosis, such as Pilates,16 stretching and massage,17 therapeutic exercises,18 orthotics,19 and ultrasonography or electric stimulation.20 However, manipulative in combination with rehabilitative techniques have not been reported extensively. Preliminary evidence suggests that these procedures may be beneficial for reducing the curvatures associated with scoliosis.20,21 The purpose of this case study is to report the psychological and clinical responses of combining manipulative and rehabilitative techniques in adolescent idiopathic scoliosis.
Case report
A 9-year-old female patient, height of 115 cm and weight of 25 kg, from Italy presented a double curve pattern with a Cobb angle of 18° thoracic and 24° thoracolumbar and a high and anterior left shoulder. These characteristics were compatible with diagnose of scoliosis1 and not within the usual range that indicates surgical intervention. To prevent possible future psychological negative impacts upon her health, the patient and the patient's family were advised to undergo physiotherapy treatment. All rights of the patient were protected, and they gave consent for publication of this case. Psychological monitoring was present in the patient's visits. Attention was paid to the availability of the patient to carry out the study and verbal acceptance of the treatment.
The treatment consisted of 15 minutes of deep tissue massage applied to the postural muscles and stretching. Spinal manipulation22,23 was added that consisted of derotation technique know as the Divesified Technique in a sitting position, dorsal and lateral recumbency (Fig 1), and active exercises through stimulation of the vestibuloocular system, the somatosensory system, and reflexes.6,20 This procedure was performed for 20 minutes at each visit. Considering the patient's age, we used this treatment as an alternative to the brace to reduce the risks of noncompliance and distress. The same rationale was used to select the frequency and schedule of the treatment.
Fig 1.

Derotation technique. A, Lumbar derotation technique, in the lateral decubitus, in the lumbar scoliosis convex to left. B, Technical standardization in dorsal recumbency in the lumbar spine in rotation with restricted mobility. C, Thoracic derotation technique, in the lateral decubitus, in the thoracic scoliosis convex to right. D, Thoracic derotation technique, in the sitting position of a thoracic scoliosis, convex to the right.
Manipulative therapy was performed during 36 visits that aimed to restore sagittal thoracic and thoracolumbar curves to normal without affecting the normal psychological development of the patient. Six months after the treatment, psychological evaluation was performed. To do that, 3 parameters were used: the SRS-22,9,24 the BrQ,15 and the BSSQ in its “brace version.” The summary score is obtained by summing the score of the single items and ranges from 0 (maximum stress) to 24 (minimum stress).7,9
After 36 weeks of treatment, patient's Cobb angles measured by radiographs were 7°/11° (thoracic/thoracolumbar) compared with 18°/24° at the beginning of the treatment, an improvement of 55%/54%. After 6 months of follow-up, the Cobb angles were 11°/11° (Fig 2). In addition, the thoracic curve was corrected and fused to less than 10°. The clinical appearance of the patient was improved by the procedure performed compared with her initial double curve pattern. According to the psychological evaluation, the patient's compliance with the treatment was 100%, with full tolerance of the treatment. In addition, no signs of social isolation or anxiety were observed in the patient before, during, or after the treatment. According to the psychological tests, after 6 months of follow-up, the patient presented a high QoL (SRS-22 = 105, BrQ = 141, BSSQ = 27; summarized in Table 1), in contrast to those patients of the same age who wear braces.7,9 In addition, at the end of the treatment, the patient demonstrated cognitive development comparable to a patient of the same age without treatment.
Fig 2.
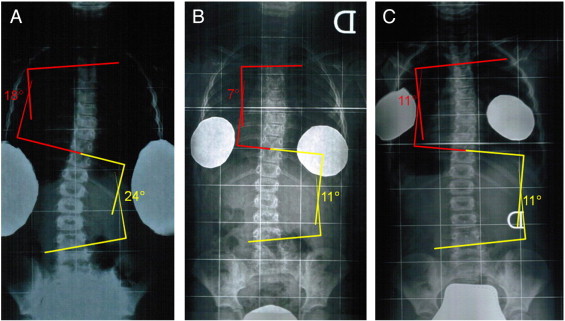
Radiographs taken (A) before treatment, (B) after 9 months of treatment, and (C) at 6-month follow-up after the end of treatment.
Table 1.
Distribution of scores for SRS-22, BrQ and BSSQ
| Variables | Value | Mean |
|---|---|---|
| SRS-22 | ||
| Function/activity | 14 | 4.66 |
| Pain | 24 | 4.8 |
| Mental health | 30 | 5.0 |
| Self-image/appearance | 21 | 3.5 |
| Satisfaction with management | 10 | 5.0 |
| Total | 105 | 4.91 |
| BrQ | ||
| General health perception | 10 | 5.0 |
| Physical functioning | 35 | 5.0 |
| Emotional functioning | 8 | 1.6 |
| Self-esteem and aesthetics | 2 | 1.0 |
| Vitality | 10 | 5.0 |
| School activity | 15 | 5.0 |
| Bodily pain | 30 | 5.0 |
| Social functioning | 35 | 5.0 |
| Total | 141 | 4.15 |
| BSSQ | ||
| Total = little stress | 27 | 3.37 |
Discussion
Scoliosis is a structural 3-dimensional deformity of the spine and trunk that occurs during puberty because of several factors.2,3 In general, the larger the scoliotic curve, the higher is the risk of progression. Similarly, thoracic and thoracolumbar double curves have greater chances of progression than single curves. Moreover, patients with less skeletal maturity have a worse prognosis than adults.2,3 Small variations in curvatures are sometimes viewed as normal, as they have little potential for progression2,3 and, in some cases, will correct by themselves over time.
This case demonstrated the effects of 9 months of physiotherapy and 6 months of follow-up on double curve in a patient with idiopathic scoliosis. These results suggest that the intervention had an immediate effect on mechanical standardization of double curve. Moreover, physiotherapy treatment did not affect quality of living with idiopathic scoliosis.
The effectiveness of the brace treatment in adolescent idiopathic scoliosis is widely acknowledged.7,9,11,12,25 However, brace treatments have some disadvantages. Patients, usually young, have to wear the brace for 18 to 23 hours a day for several years; the brace is often visible and can be uncomfortable to wear.26 This type of treatment can be rather bothersome26 and may significantly impact patients’ psychological well-being and negatively affect their QoL.9,21 Bracing may have psychological impacts at the beginning of treatment, including reduced self-esteem.3,9,13,27 Because of psychological issues alone, a 9% rate of brace-treatment distress and discontinuation among girls has been reported.9,12 Poor compliance with a brace protocol is associated with even poorer QoL. In addition, noncompliant patients have decreased vitality, combined with physical-emotional and social deterioration.12 Moreover, noncompliance with brace wear is often an issue and varies from refusal to wear the orthosis to premature discontinuation of the use of that brace and to less than full-time use of the brace.26
Others have found that spinal manipulation alone does not appear to alter spinal structure when administered as a sole treatment modality.20 Therefore, we hypothesized that treatment of adolescent idiopathic scoliosis should include the use of both manipulative and rehabilitative procedures so that structural changes can be accomplished. Consequently, a careful choice of specific and personalized exercises and therapies may be more effective than conventional care; and such treatment may avoid brace prescription in countering scoliosis.28 However, more research needs to be done in a controlled setting to test these hypotheses.
A retrospective analysis of 24 months, 28 patients with scoliosis receiving chiropractic rehabilitation was reported. The authors demonstrated sustained radiographic, self-rated, and psychological benefits after treatment ceased.29 Chiropractic treatment was also associated with a reduction in a severe case of adolescent idiopathic scoliosis (46° Cobb angle) in a young female after she had previously received conservative medical treatment that failed to stop curve progression.30
Currently, nonsurgically treated patients are encouraged to participate in sports and physical activity; and scoliosis is not a contraindication to participation in most sports31; therefore, this could also increase the QoL of the patients. In addition, manipulation of the spine under anesthesia is an outpatient procedure performed to restore normal joint kinematics and musculoskeletal function.32 Pain, functional, and radiographic outcomes demonstrated improvements immediately following treatment for this patient.32 Taken together, these therapeutic alternatives should also be considered depending on the patient's case.
Body image and health-related QoL are significant issues for patients with scoliosis because of cosmetic deformity and physical and psychological symptoms.8 Increased severity of structural spine deformation correlates with a greater likelihood of social and psychological complications.33
Although the treatment was successful, the fundamental explanations of our results are unknown. The mechanisms underlying our outcomes might be related to increased spine movement and ligamentous lengthening of the concavities of the scoliotic curvatures. Therefore, it is possible that the addition of manipulative and rehabilitative techniques allowed us to mobilize regions of the spine that were not successfully mobilized by other means. In addition, the present case introduces a possible alternative conservative therapy and does not appear to induce a detrimental effect in the patient's psychological development. It is suggested that the decision to perform a given treatment of adolescent idiopathic scoliosis should not be based solely on a health practitioner's opinion; it should also include the opinions and guidance of the psychology staff.
Limitations
There are limitations to this case report. This report demonstrates only a single case; and therefore, the management protocol cannot be generalized to all cases of adolescent idiopathic scoliosis. A single case report does not prove cause and effect. Because of the nature of the case and the lack of a placebo, it is possible that there were other influences and that this patient may have improved without treatment.
Conclusion
The management protocol used in this case seemed to produce clinical improvements for this patient. In addition, the patient did not show psychological sequel after the treatment. These results confirm the urgent need of large, high-quality, randomized controlled studies of such techniques to demonstrate their validity. We recommend that outcome measures of these studies should include psychological and social effects.
Funding sources and potential conflicts of interest
This work was supported by personal funds of J.H.V. and in part by a grant from the J. Robert Cade Foundation to G.B.S. G.B.S. is also a member of the Consejo Nacional de Investigaciones Científicas y Técnicas (CONICET) Argentina. No conflicts of interest were reported for this study.
References
- 1.Morningstar M.W., Strauchman M.N., Gilmour G. Adolescent idiopathic scoliosis treatment using Pettibon corrective procedures: a case report. J Chiropr Med. 2004;3(3):96–103. doi: 10.1016/S0899-3467(07)60093-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Weiss H.R. Adolescent idiopathic scoliosis—case report of a patient with clinical deterioration after surgery. Patient Saf Surg. 2007;1:7. doi: 10.1186/1754-9493-1-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Negrini S., Aulisa L., Ferraro C., Fraschini P., Masiero S., Simonazzi P. Italian guidelines on rehabilitation treatment of adolescents with scoliosis or other spinal deformities. Eura Medicophys. 2005;41(2):183–201. [PubMed] [Google Scholar]
- 4.Negrini A., Parzini S., Negrini M.G., Romano M., Atanasio S., Zaina F. Adult scoliosis can be reduced through specific SEAS exercises: a case report. Scoliosis. 2008;3:20. doi: 10.1186/1748-7161-3-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lange J.E., Steen H., Brox J.I. Long-term results after Boston brace treatment in adolescent idiopathic scoliosis. Scoliosis. 2009;4:17. doi: 10.1186/1748-7161-4-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rowe D.E., Feise R.J., Crowther E.R., Grod J.P., Menke J.M., Goldsmith C.H. Chiropractic manipulation in adolescent idiopathic scoliosis: a pilot study. Chiropr Osteopat. 2006;14:15. doi: 10.1186/1746-1340-14-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kotwicki T., Kinel E., Stryla W., Szulc A. Estimation of the stress related to conservative scoliosis therapy: an analysis based on BSSQ questionnaires. Scoliosis. 2007;2:1. doi: 10.1186/1748-7161-2-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tones M.J., Moss N.D. The impact of patient self assessment of deformity on HRQL in adults with scoliosis. Scoliosis. 2007;2:14. doi: 10.1186/1748-7161-2-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Aulisa A.G., Guzzanti V., Perisano C., Marzetti E., Specchia A., Galli M. Determination of quality of life in adolescents with idiopathic scoliosis subjected to conservative treatment. Scoliosis. 2010;5:21. doi: 10.1186/1748-7161-5-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bunge E.M., Juttmann R.E., de Kleuver M., van Biezen F.C., de Koning H.J. Health-related quality of life in patients with adolescent idiopathic scoliosis after treatment: short-term effects after brace or surgical treatment. Eur Spine J. 2007;16(1):83–89. doi: 10.1007/s00586-006-0097-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Richards B.S., Bernstein R.M., D'Amato C.R., Thompson G.H. Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management. Spine (Phila Pa 1976) 2005;30(18):2068–2075. doi: 10.1097/01.brs.0000178819.90239.d0. discussion 76-7. [DOI] [PubMed] [Google Scholar]
- 12.Rivett L., Rothberg A., Stewart A., Berkowitz R. The relationship between quality of life and compliance to a brace protocol in adolescents with idiopathic scoliosis: a comparative study. BMC Musculoskelet Disord. 2009;10:5. doi: 10.1186/1471-2474-10-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Weiss H.R., Bess S., Wong M.S., Patel V., Goodall D., Burger E. Adolescent idiopathic scoliosis—to operate or not? A debate article. Patient Saf Surg. 2008;2(1):25. doi: 10.1186/1754-9493-2-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Benli I.T., Ates B., Akalin S., Citak M., Kaya A., Alanay A. Minimum 10 years follow-up surgical results of adolescent idiopathic scoliosis patients treated with TSRH instrumentation. Eur Spine J. 2007;16(3):381–391. doi: 10.1007/s00586-006-0147-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vasiliadis E., Grivas T.B., Gkoltsiou K. Development and preliminary validation of Brace Questionnaire (BrQ): a new instrument for measuring quality of life of brace treated scoliotics. Scoliosis. 2006;1:7. doi: 10.1186/1748-7161-1-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Blum C.L. Chiropractic and Pilates therapy for the treatment of adult scoliosis. J Manipulative Physiol Ther. 2002;25(4):E3. doi: 10.1067/mmt.2002.123336. [DOI] [PubMed] [Google Scholar]
- 17.Tarola G.A. Manipulation for the control of back pain and curve progression in patients with skeletally mature idiopathic scoliosis: two cases. J Manipulative Physiol Ther. 1994;17(4):253–257. [PubMed] [Google Scholar]
- 18.Romano M., Negrini S. Manual therapy as a conservative treatment for adolescent idiopathic scoliosis: a systematic review. Scoliosis. 2008;3:2. doi: 10.1186/1748-7161-3-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lantz C.A., Chen J. Effect of chiropractic intervention on small scoliotic curves in younger subjects: a time-series cohort design. J Manipulative Physiol Ther. 2001;24(6):385–393. doi: 10.1067/mmt.2001.116419. [DOI] [PubMed] [Google Scholar]
- 20.Morningstar M.W., Woggon D., Lawrence G. Scoliosis treatment using a combination of manipulative and rehabilitative therapy: a retrospective case series. BMC Musculoskelet Disord. 2004;5:32. doi: 10.1186/1471-2474-5-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Morningstar M.W., Joy T. Scoliosis treatment using spinal manipulation and the Pettibon Weighting System: a summary of 3 atypical presentations. Chiropr Osteopat. 2006;14:1. doi: 10.1186/1746-1340-14-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lee R.Y. Kinematics of rotational mobilisation of the lumbar spine. Clin Biomech (Bristol, Avon) 2001;16(6):481–488. doi: 10.1016/s0268-0033(01)00036-5. [DOI] [PubMed] [Google Scholar]
- 23.Maitland G., Hengeveld E., Banks K., English K. 6th ed. Butterworth-Heinemann; Oxford: 2000. Maitland' s vertebral manipulation. [Google Scholar]
- 24.D'Agata E., Testor C.P., Rigo M. Spanish validation of Bad Sobernheim Stress Questionnaire (BSSQ (brace).es) for adolescents with braces. Scoliosis. 2010;5:15. doi: 10.1186/1748-7161-5-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Aulisa A.G., Guzzanti V., Galli M., Perisano C., Falciglia F., Aulisa L. Treatment of thoraco-lumbar curves in adolescent females affected by idiopathic scoliosis with a progressive action short brace (PASB): assessment of results according to the SRS committee on bracing and nonoperative management standardization criteria. Scoliosis. 2009;4:21. doi: 10.1186/1748-7161-4-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Canavese F., Kaelin A. Adolescent idiopathic scoliosis: indications and efficacy of nonoperative treatment. Indian J Orthop. 2011;45(1):7–14. doi: 10.4103/0019-5413.73655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lenssinck M.L., Frijlink A.C., Berger M.Y., Bierman-Zeinstra S.M., Verkerk K., Verhagen A.P. Effect of bracing and other conservative interventions in the treatment of idiopathic scoliosis in adolescents: a systematic review of clinical trials. Phys Ther. 2005;85(12):1329–1339. [PubMed] [Google Scholar]
- 28.Negrini S., Zaina F., Romano M., Negrini A., Parzini S. Specific exercises reduce brace prescription in adolescent idiopathic scoliosis: a prospective controlled cohort study with worst-case analysis. J Rehabil Med. 2008;40(6):451–455. doi: 10.2340/16501977-0195. [DOI] [PubMed] [Google Scholar]
- 29.Morningstar M.W. Outcomes for adult scoliosis patients receiving chiropractic rehabilitation: a 24-month retrospective analysis. J Chiropr Med. 2011;10(3):179–184. doi: 10.1016/j.jcm.2011.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Chen K.C., Chiu E.H. Adolescent idiopathic scoliosis treated by spinal manipulation: a case study. J Altern Complement Med. 2008;14(6):749–751. doi: 10.1089/acm.2008.0054. [DOI] [PubMed] [Google Scholar]
- 31.Green B.N., Johnson C., Moreau W. Is physical activity contraindicated for individuals with scoliosis? A systematic literature review. J Chiropr Med. 2009;8(1):25–37. doi: 10.1016/j.jcm.2008.11.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Morningstar M.W., Strauchman M.N. Management of a 59-year-old female patient with adult degenerative scoliosis using manipulation under anesthesia. J Chiropr Med. 2010;9(2):77–83. doi: 10.1016/j.jcm.2010.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Dickson R.A. Conservative treatment for idiopathic scoliosis. J Bone Joint Surg Br. 1985;67(2):176–181. doi: 10.1302/0301-620X.67B2.3872301. [DOI] [PubMed] [Google Scholar]