

Abstract
Introduction
Spinal stab wound injuries are quite rare and only few patients have been reported on the basis of MRI scan.
Methods
A 25-year-old man was stabbed at C1/2 and had an incomplete Brown-Sequard syndrome. He underwent surgical exploration because of CSF leakage on the fourth day.
Results
After a follow-up period of 32 months, he was left with a remaining loss of the proprioception of the right foot. We show detailed CT and MR images with the focus on the lesions of the dura and myelon and compared them with intraoperative images. In addition, we contrast our findings with a review of literature published over the last three decades.
Conclusion
MRI gives the most detailed view of soft tissue lesions in SSWs and is in accordance with our intraoperative findings.
Keywords: Stab wound, Spine, Myelon, MRI, Brown-Sequard syndrome
Introduction
In parts of the world (e.g. in South Africa) spinal stab wounds (SSWs) occur quite frequently, but not so in Europe. However, according to a UK study [1], these injuries are increasing in number. Thus, they deserve closer attention. In the US, spinal cord injuries (SCIs) make up only 2.6% [2] of all the trauma cases, of which fewer than 1.5% [3–5] can be attributed to stab wounds. The most reported site is the thoracic spine, followed by the cervical and the lumbar spine [3, 6, 7]. The craniocervical junction is rarely affected due to the anatomy of this region [8–10].
Severe SSWs with neurologic deficit and CSF leakage are very rare entities at our department. Explicit treatment guidelines are therefore missing. Corresponding to the published data with an increasing incidence, more injured patients are expected. Thus, the enrolled case does not only give a detailed overview of the pathomechanism related to the anatomy but also figures out an investigation and therapeutic plan. Above all, we prove that the preoperative performed CT/MRI images are in accordance with the intraoperative photos and are essential for planning the approach.
Case report
In the course of a fight, a 25-year-old man was stabbed with a knife in the neck and in the back. He was taken to the next local hospital and then transferred to our institution because of a right-sided hemiplegia. At his admission, he was somnolent but cooperative and showed stable vital signs despite a blood alcohol level of 1.8%. There were multiple clean-cut skin wounds (3 cm in length) from the neck to the thoracic spine level, including a lesion of the spleen. Neurologic examination revealed a slightly impaired motor function of the arm (grade 4/5) and a higher-grade paresis of the right lower limb (grade 3/5). The sensory examination indicated a hypaesthesia of the right side with spared sacral sensation and a normal anal sphincter tone. The deep tendon reflexes were present bilaterally. Repeated neurologic investigations did not show any deterioration.
A persisting cerebrospinal fluid (CSF) leakage from the upper wound was given a conservative treatment. A splenectomy was necessary to stop the continuous blood loss on the third day. The patient was kept analgosedated, because an increased discharge of CSF with a total amount of 400 ml per day made further treatment with an entire duraplasty mandatory [11, 12] on the fifth day. On the following day, the patient woke up. The neurologic assessment showed a deterioration of the best motor function to grade 3/5. Hypaesthesia had improved in general, but the right lower leg was still impaired. The impaired proprioception of the leg persisted until the patient’s discharge from the rehabilitation ward 5 weeks later.
After a follow-up period of 32 months, the extremities had regained full and equal strength. In contrast to a diminished proprioception of the right foot, the ipsilateral hyposensitivity had fully recovered. Pain and temperature sensation of the contralateral side was normal (Figs. 1, 2, 3, 4).
Fig. 1.
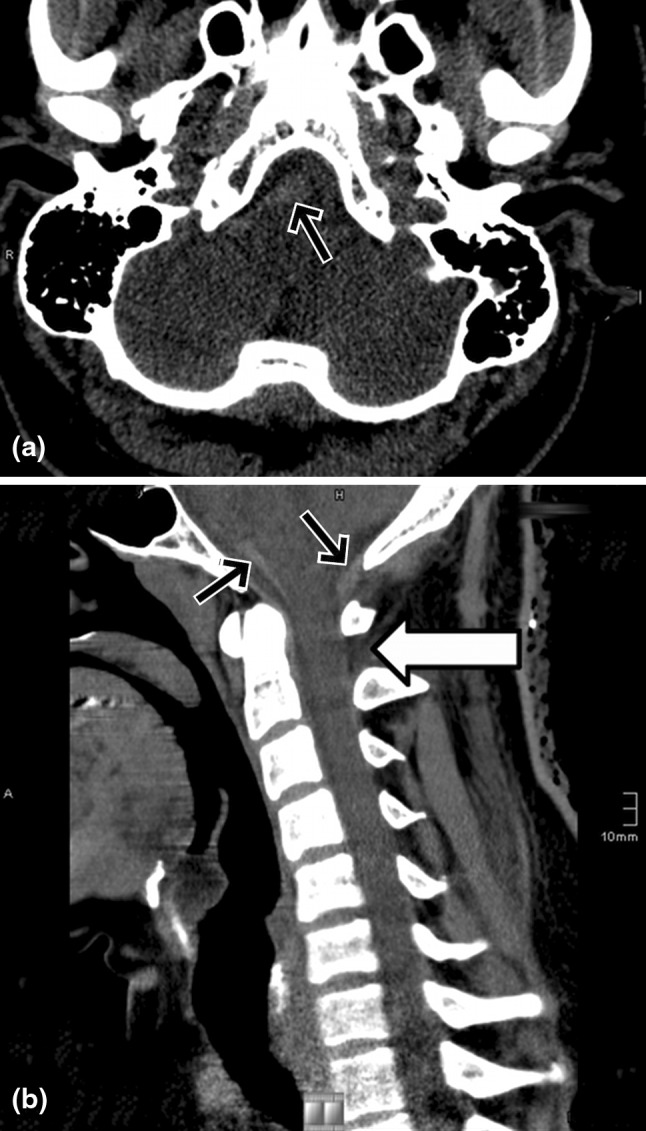
a, b Axial CT and reconstructed sagittal MPR showing acute perimedullar hemorrhage (black arrows); a dural defect can hardly be seen (white arrow)
Fig. 2.
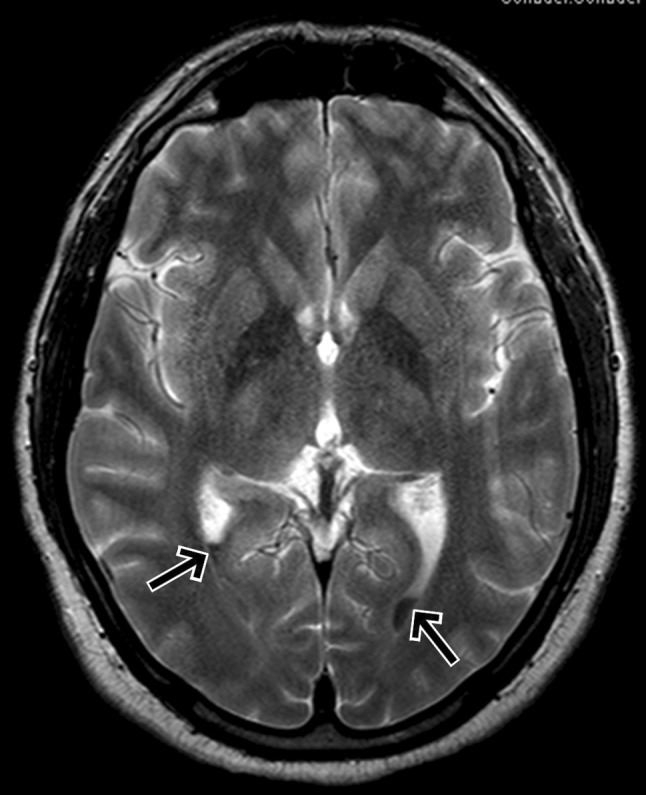
MRI axial T2-weighted sequence demonstrating a fluid level in the posterior horn of the ventricles due to hemorrhage
Fig. 3.

MRI T2-weighted sagittal image hypointense structures indicate acute hemorrhage in perimedullar and prepontine location (black arrows) and a laceration of the dorsomedian dura mater between C1/2 (white arrow); a faint hyperintense signal in the posterior parts of the medulla also can be seen
Fig. 4.

MRI T1-weighted sagittal image demonstrating subarachnoid hemorrhage (black arrows) but in this case the dural defect cannot be seen as clearly as in the T2-weighted image
Discussion
Stab wounds of the spine are significantly more common in South Africa, where 25% of all the patients with SCIs are affected thereby. The three largest series reporting over 900 cases of SSWs are from this region [3, 6, 13]. By comparison, most North American series describe the epidemiology of SSWs between 8 and 11% of all penetrating spinal injuries [14–17].
Spinal stab wounds usually present themselves in an acute form and show typical skin lesions.
However, there are patients who do not seek immediate medical attention. There are four reported cases of delayed SSWs, dating back between 4 weeks and 30 years after the stabbing [18–21].
There are several mechanisms of causing an acute neurologic deficit following spinal stabbing. The blade either damages neural elements of the spinal cord directly, causes infarction due to a lesion of the artery of Adamkiewicz [22, 23], or, less frequent, a spinal epidural hematoma. In the case of a direct penetration, the patient is usually left with an incomplete spinal cord injury based on the anatomic bony singularity.
The spinous processes in the sagittal plane and the transverse processes in the coronal plane form a gutter into the interlaminar space, so that the blade hits only one side of the spinal cord, always resulting in a Brown-Sequard variant [3]. At the cervicomedullary junction, the obliquity and thickness of the occipital squama deflect the stabbing instrument in order that it usually slides along the undersurface into the atlanto-occipital or atlanto-axial interspace [9]. Vertebral vessels may be damaged, if the blade is deflected towards the spinal canal. Possibly, it penetrates the dura, causing subsequent CSF leakage, pneumocephalus [12] and a lesion of the myelon. An association with Horner’s syndrome [8] or a traumatic pseudomeningocele after cervical SSWs has been reported [24]. Vascular complications are embolisms, the development of aneurysms or arteriovenous fistulas [9]. The metal fragments of the weapon remaining in the myleon can transfix the spinal cord and induce myelopathy [19–21].
Cerebrospinal fluid leakage towards the skin is scarcely found, only in 4% of the cases [3]. CSF leakage lasting for more than 3–4 days may become life threatening on account of potential pneumocephalus [12].
The diagnostic work-up should start with analyzing plain radiographs to exclude any metal fragment. Osseous lesions and free air can be best detected using a CT. If there is no metal fragment in the wound, magnetic resonance imaging (MRI) provides a superior view of the extent of injury [25–28]. MRI traces the path the blade has taken through the soft tissue and shows foreign bodies. Moreover, it detects intraspinal hemorrhage, acute cord edema as well as contusions of the spinal cord. T2-weighted fat saturated and STIR (short tau inversion recovery) sequences are recommended; they are very useful in identifying ligamentous disruption and dural lesions (Figs. 5, 6, 7).
Fig. 5.

MR axial T2-weighted images, showing the absence of the dorsomedian aspect of the hypointense dura (white arrow)
Fig. 6.

MR axial T1-weighted images, showing the absence of the dorsomedian aspect of the hypointense dura (white arrow)
Fig. 7.
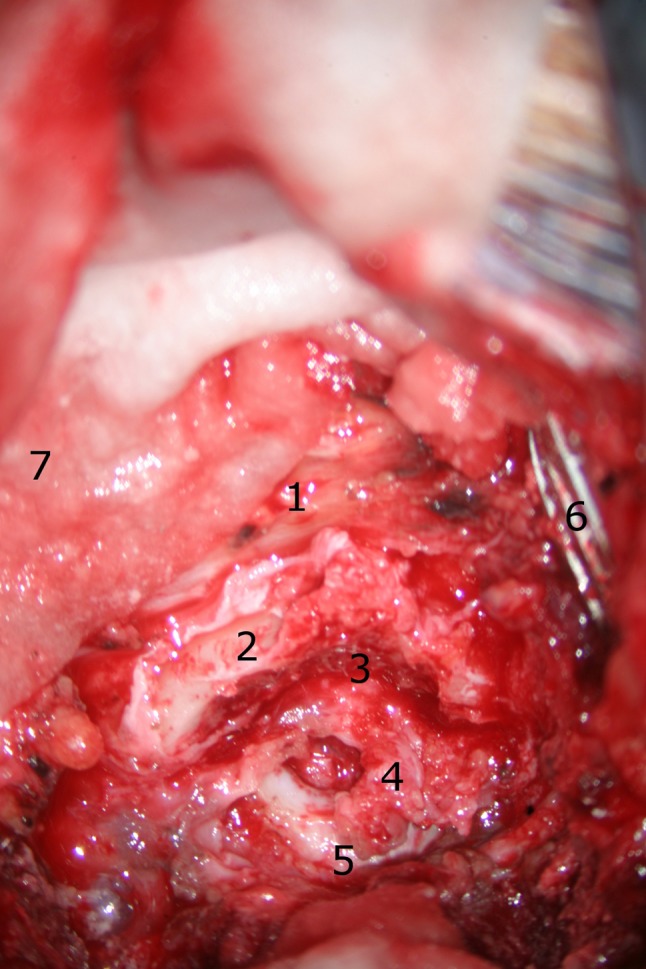
The patient is in a prone position and the head fixed with a pinion headholder. The surgeon is at the head of the table, so the caudal direction is at 12 o’clock. The skin is cutted median above the spinous processes and the paravertebral muscles are moved laterally. Overview of the situs: 1 spinous process of C3, 2 right lamina of the axis, 3 area of partial laminectomy, 4 dura lesion, 5 posterior arch of the atlas, 6 retractor, 7 cotton pad
Nevertheless, MRI findings do not have a great influence on the acute decision of whether to operate or not [29]. The majority of SSWs are treated conservatively, including a primary closure after local debridement, intravenous antibiotics and tetanus prophylaxis. Spinal infections are rare [6].
Surgical exploration of a stab injury remains controversial [3–7, 18, 30, 31] but it is suggested for progressive neurologic deficit, an incomplete lesion or persistent CSF leaks for more than 4 days. A secondary deterioration is most often caused by an infection and usually makes drainage necessary [29].
Besides, initial MR images help the radiologist to distinguish between an intradural or intraspinal hematoma with radiologic signs of cord compression and a complete cord injury. In the first case, an urgent evacuation is mandatory [3], whereas a completely transected cord is managed conservatively. In the event of neurologic worsening, MR helps to detect a hematoma, an edema or an early infection on contrast scans. Moreover, retained metal fragments may entail a delayed neurologic deterioration because they have transfixed the cord or developed myelopathy [19–21, 26]. There are no current data available that could supply reliable information on the prognostic value of MRI scans in terms of the SSWs.
Our patient’s plain radiographs of the cervical and thoracic spine do not demonstrate any fracture or retained foreign body. The CT scans exclude an osseous lesion and indicate a deep stabbing on the left side between C1 and C2. The MRI scans render perfect images of the extension of the wound. Penetrating the body from the left lateral, the blade drove horizontally into the interlaminar space. The dura was cut median and, along this direction, the myelon was injured right paramedian. In consequence of persistent liquorrhea, we performed a duraplasty through a partial laminectomy of the caudal aspect of the atlas. The intraoperative photos show a clean-cut myelon correlating with the MR images and the clinical findings of an incomplete Brown-Sequard syndrome. Due to a 4 days’ delay in surgery and the circulation of the cerebrospinal fluid, the intradural hemorrhage could not be verified anymore (Figs. 8, 9, 10).
Fig. 8.

Magnification of the dura lesion. On the ground the incision of the myelon is visible. 1 spinous process of C3, 2 right lamina of the axis, 3 area of partial laminectomy, 4 dura lesion, 6 retractor, 8 myelon
Fig. 9.

The myelon lesion is focused for the best view: the cut ends in the myelon. There is no bleeding whether of the myelon nor epi-/subdural anymore. The suction tube is held in the left hand. 4 dura lesion, 8 myelon, 10 cut into the myelon, 11 suction tube
Fig. 10.

Overview of the entire duraplasty before the wound is closed. A partial laminectomy of C1 was necessary to get enough intact dura for tight sutures. 2 right lamina of the axis, 3 area of partial laminectomy, 7 cotton pad, 12 duraplasty, 13 epidural fat, 14 suture
The prognosis of SSWs is better than that of blunt SCIs or gunshot wounds. Presented with incomplete SCIs, 66% of the patients have a good recovery [6, 13, 18]. The outcome of our patient concurs with the reviewed literature.
Conclusion
On account of the anatomy, the majority of SSWs induce a partial hemisection of the spinal cord and appear clinically most often as a Brown-Sequard variant.
MRI gives the most detailed view of soft tissue lesions in SSWs and is in accordance with our intraoperative findings. The prognostic value of MRI in regard to SSWs remains uncertain. In the case of persistent liquorrhea, however, MRI is likely to be of great help to the surgeon in finding the dural defect.
Conflict of interest
None of the authors has any potential conflict of interest.
References
- 1.Offiah C, Twigg S. Imaging assessment of penetrating craniocerebral and spinal trauma. Clin Radiol. 2009;64:1146–1157. doi: 10.1016/j.crad.2009.06.004. [DOI] [PubMed] [Google Scholar]
- 2.Burney RE, Maio RF, Maynard F, et al. Incidence, characteristics, and outcome of spinal cord injury at trauma centers in North America. Arch Surg. 1993;128:596–599. doi: 10.1001/archsurg.1993.01420170132021. [DOI] [PubMed] [Google Scholar]
- 3.Peacock WJ, Shrosbree RD, Key AD. A review of 450 stabwounds of the spinal cord. S Afr Med J. 1977;51:961–964. [PubMed] [Google Scholar]
- 4.Waters RL, Sie I, Adkins RH, et al. Motor recovery following spinal cord injury caused by stab wounds: a multicenter study. Paraplegia. 1995;33:98–101. doi: 10.1038/sc.1995.23. [DOI] [PubMed] [Google Scholar]
- 5.Rubin G, Tallman D, Sagan L, et al. An unusual stab wound of the cervical spinal cord: a case report. Spine. 2001;26:444–447. doi: 10.1097/00007632-200102150-00023. [DOI] [PubMed] [Google Scholar]
- 6.Velmahos GC, Degiannis E, Hart K, et al. Changing profiles in spinal cord injuries and risk factors influencing recovery after penetrating injuries. J Trauma. 1995;38:334–337. doi: 10.1097/00005373-199503000-00004. [DOI] [PubMed] [Google Scholar]
- 7.Takemura S, Sasai K, Ohnari H, et al. Brown-Sequard-plus syndrome due to stab injury: a case report. Spinal Cord. 2006;44:518–521. doi: 10.1038/sj.sc.3101871. [DOI] [PubMed] [Google Scholar]
- 8.Garcia-Manzanares MD, Belda-Sanchis JI, Giner-Pascual M, et al. Brown-Sequard syndrome associated with Horner’s syndrome after a penetrating trauma at the cervicomedullary junction. Spinal Cord. 2000;38:705–707. doi: 10.1038/sj.sc.3101062. [DOI] [PubMed] [Google Scholar]
- 9.Villiers JC, Grant AR. Stab wounds at the craniocervical junction. Neurosurgery. 1985;17:930–936. doi: 10.1227/00006123-198512000-00010. [DOI] [PubMed] [Google Scholar]
- 10.Pal HK, Bhatty GB, Deb S, et al. Traumatic pseudomeningocele at craniovertebral junction following stab injury. Injury. 1998;29:142–143. doi: 10.1016/S0020-1383(97)00149-6. [DOI] [PubMed] [Google Scholar]
- 11.Page RD, Lye RH. Stab wound of the neck: potential pitfalls in management. Arch Emerg Med. 1989;6:225–229. doi: 10.1136/emj.6.3.225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rahaminov N, Mulla H, Freiman S. Cerebrospinal fluid leakage and pneumocephalus secondary to spine stab wounds. J Orthopaed Traumatol. 2010;11:57–59. doi: 10.1007/s10195-009-0070-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lipschitz R. Stab wounds of the spinal cord. In: Vinken PJ, Bruyn GW, editors. Handbook of clinical neurology. New York: Elsevier; 1976. pp. 197–207. [Google Scholar]
- 14.Heary RF, Vacaro AR, Mesa JJ, Balderston RA. Thoracolumbar infections in penetrating injuries to the spine. Ortho Clin N Am. 1996;27:69–81. [PubMed] [Google Scholar]
- 15.Robertson DP, Simpson RK. Penetrating injuries restricted to the cauda equina: a retrospective review. Neurosurgery. 1992;31:265–269. doi: 10.1227/00006123-199208000-00011. [DOI] [PubMed] [Google Scholar]
- 16.Simpson RK, Venger BH, Narayan RK. Treatment of acute penetrating injuries of the spine: a retrospective analysis. J Trauma. 1989;29:42–46. [PubMed] [Google Scholar]
- 17.Venger BH, Simpson RK, Narayan RK. Neurosurgical intervention in penetrating spinal trauma with associated visceral injury. J Neurosurg. 1989;70:514–518. doi: 10.3171/jns.1989.70.4.0514. [DOI] [PubMed] [Google Scholar]
- 18.Kulkarni AV, Bhandari M, Stiver S, et al. Delayed presentation of spinal stab wound: case report and review of the literature. J Emerg Med. 2000;18:209–213. doi: 10.1016/S0736-4679(99)00196-1. [DOI] [PubMed] [Google Scholar]
- 19.Jones FD, Woosley RE. Delayed myelopathy secondary to retained intraspinal metallic fragment. Case report. J Neurosurg. 1981;55:979–982. doi: 10.3171/jns.1981.55.6.0979. [DOI] [PubMed] [Google Scholar]
- 20.Wolf SM. Delayed traumatic myelopathy following transfixion of the spinal cord by a knife blade. Case report. J Neurosurg. 1973;38:221–225. doi: 10.3171/jns.1973.38.2.0221. [DOI] [PubMed] [Google Scholar]
- 21.Fung CF, Ng TH. Delayed myelopathy after a stab wound with a retained intraspinal foreign body: case report. J Trauma. 1992;32:539–541. doi: 10.1097/00005373-199204000-00020. [DOI] [PubMed] [Google Scholar]
- 22.Keane JR, Gama LR. Isolated paraplegia from a remote stab wound. Neurosurgery. 1993;33:274–276. doi: 10.1227/00006123-199308000-00014. [DOI] [PubMed] [Google Scholar]
- 23.Rogers FB, Osler TM, Shackford SR, Wald SL. Isolated stab wound to the artery of Adamkiewicz: case report and review of the literature. J Trauma. 1997;43:549–551. doi: 10.1097/00005373-199709000-00031. [DOI] [PubMed] [Google Scholar]
- 24.Seo BR, Lee JK, Lee JH, Kim SH. An unusual stab wound causing a traumatic pseudomeningocele at the craniocervical junction. J Clin Neurosci. 2009;16:1365–1367. doi: 10.1016/j.jocn.2008.10.020. [DOI] [PubMed] [Google Scholar]
- 25.Alkan A, Baysal T, Saras K, et al. Early MRI findings in stab wounds of the cervical spine: two case reports. Neuroradiology. 2002;44:64–66. doi: 10.1007/s002340100646. [DOI] [PubMed] [Google Scholar]
- 26.Flanders AE, Schaefer DM, Doan HT, Mishkin MM, Gonzalez CF, Northrup BE. Acute cervical spine trauma: correlation of MR imaging findings with degree of neurologic deficit. Radiology. 1990;177:25–33. doi: 10.1148/radiology.177.1.2399326. [DOI] [PubMed] [Google Scholar]
- 27.Uppot RN, Gheyi VK, Gould SW, Ito H. Pneumocephalus and Brown-Sèquard’s neurologic injury caused by a stab wound to the neck. Am J Roentgenol. 1999;173:1504. doi: 10.2214/ajr.173.6.10584791. [DOI] [PubMed] [Google Scholar]
- 28.Seo B-R, Lee J-K, Jeong I-H, Moon S-J, et al. An unusual stab wound causing a traumatic pseudomeningocele at the craniocervial junction. Case reports. J Clin Neurosci. 2009;16:1365–1367. doi: 10.1016/j.jocn.2008.10.020. [DOI] [PubMed] [Google Scholar]
- 29.Jacobsohn M, Semple P, Dunn R, Candy S. Stab injuries to the spinal cord: a retrospective study on clinical findings and magnetic resonance imaging changes. Neurosurgery. 2007;61:1262–1267. doi: 10.1227/01.neu.0000306105.76259.63. [DOI] [PubMed] [Google Scholar]
- 30.Larsen LB, Tollesson G, Solgaard T. Spinal cord injury following knife stab wound [in Norwegian] Tidsskr Nor Laegeforen. 2001;121:434–435. [PubMed] [Google Scholar]
- 31.Lee KH, Lin JS, Pallatroni HF, Ball PA. An unusual case of penetrating injury to the spine resulting in cauda equina syndrome. Spine. 2007;32:E290–E293. doi: 10.1097/01.brs.0000260986.70179.8e. [DOI] [PubMed] [Google Scholar]