

Abstract
Qnexa (VI-0521) is an investigational fixed-dose combination drug of phentermine and topiramate currently in Phase III clinical trials for the treatment of obesity. Vivus, Inc. has demonstrated efficacy of their product and are currently addressing FDA safety concerns with the possibility of a New Drug Application (NDA) resubmission.
Keywords: Qnexa, phentermine, topiramate, weight-loss, obesity
Qnexa (VI-0521) is a novel fixed-dose combination of phentermine and topiramate (PHEN/TPM) in late-stage development by Vivus, Inc. as a potential treatment for obesity, including weight loss and maintenance of weight loss when used in conjunction with diet and exercise. PHEN/TPM is recommended for obese patients (BMI > 30 kg/m2) or overweight patients (BMI > 27 kg/m2) with weight-related comorbidities such as hypertension, type 2 diabetes, dyslipidemia, or central adiposity (abdominal obesity). The NIH reported in 2007 that approximately 68% of adults in the U.S. are obese or overweight and estimated the U.S. medical burden of obesity to be approximately $147 billion in 2008.1 Obesity is associated with numerous comorbidities, including diabetes, heart disease, dyslipidemia, hypertension, stroke, cancer, and depression. According to the NIH, the initial goal of weight loss therapy is to reduce body weight by approximately 10% from baseline.2 Unfortunately, currently approved pharmacotherapies are associated with <5% weight loss and are often poorly tolerated, leaving bariatric surgery as the only effective, yet invasive, treatment for obesity. These findings have spurred investigation into combination pharmacotherapies, such as Qnexa, to potentially fill this treatment gap to safely deliver sufficient and durable weight loss of >10%.
Phentermine and topiramate are both currently approved and marketed drugs with over six million and nine million prescriptions in 2009, respectively. Phentermine monotherapy was approved for the short-term treatment of obesity in 1959. Topiramate monotherapy was approved in 1996 for the treatment of seizures and in 2004 for migraine prophylaxis. The Qnexa NDA was filed with PHEN/TPM available in three dosage strengths: low (3.75 mg PHEN/23 mg TPM), mid (7.5 mg PHEN/46 mg TPM), and high (15 mg PHEN/92 mg TPM) with phentermine as immediate release and topiramate as controlled release. Mid-dose PHEN/TPM once daily is the proposed recommended maintenance dose.
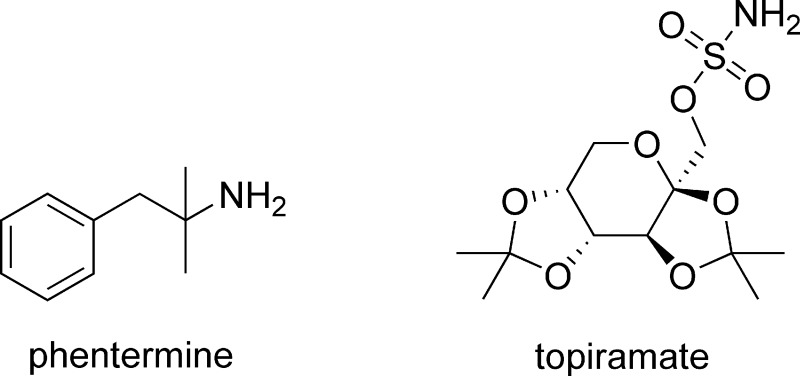
Phentermine, an amphetamine analogue, is an appetite suppressant interacting at biogenic amine transporters in the CNS including the norepinephrine transporter (NET), dopamine transporter (DAT), and the serotonin transporter (SERT), causing a release of the respective neurotransmitter. Phentermine acts as a potent substrate at NET and has weaker activity at DAT and SERT with EC50 values of 39, 262, and 3511 nM, respectively.3 As such, phentermine-induced central norepinephrine release is its primary mechanism of action for inducing weight loss by reducing food intake.3 Topiramate, a monosaccharide d-fructose derivative, exhibits a combination of properties including modulatory effects on sodium channels, enhancement of GABA-activated chloride channels, inhibition of excitatory neurotransmission through actions on kainate and AMPA receptors, and inhibition of carbonic anhydrase (CA) isoenzymes in particular CA II and IV.4 The precise mechanism of topiramate’s effect on weight is unclear; however, it is known to increase satiety (satisfaction) and alter taste.
The efficacy of Qnexa was assessed through two randomized (OB-302 and OB-303), double-blind, placebo-controlled 56 week phase III clinical trials. OB-302 enrolled 1300 subjects with BMI values > 35 kg/m2, no comorbidities on a 2:1:2 placebo−low-dose PHEN/TPM−high-dose PHEN/TPM regimen, whereas OB-303 enrolled 2500 subjects with lower BMI values with weight-related comorbidities on a 2:1:2 placebo−mid-dose PHEN/TPM−high-dose PHEN/TPM regimen.5 Both trials involved a 4 week titration phase plus lifestyle modifications. The majority of subjects were middle-aged Caucasian women with approximately one-third being extremely obese (BMI > 40 kg/m2). Subject completion of the 56 week treatment was 53%, 57%, 69%, and 62% for the placebo, low-dose, mid-dose, and high-dose PHEN/TPM groups, respectively.5 Adverse effects (AEs) were the major reason for failure to complete the study. Statistically significant dose-related reduction in percent body weight (baseline to week 56) was observed for all PHEN/TPM-treated groups relative to placebo. The highest mean weight loss was 10.6% for the high-dose PHEN/TPM treatment groups followed by 8.4%, 5.1%, and 1.7% for the mid-dose, low-dose, and placebo treatment groups, respectively.5 Results indicate all three PHEN/TPM doses were efficacious for weight loss and showed expected improvement in blood pressure, lipids, and glycemia.
In terms of safety, five areas were of focus: teratogenicity, psychiatric-related AEs, cognitive-related AEs, metabolic acidosis, and cardiovascular AEs. Topiramate at doses 2−34 times the proposed maximum dose in PHEN/TPM is a known teratogen in mice, rats, and rabbits causing craniofacial defects and limb abnormalities. During the trial, 34 pregnancies were reported and all trial participants discontinued drug treatment around 5.4 weeks gestation. Nineteen pregnancies were carried to term; of these, 13 infants were born to mothers on the PHEN/TPM treatment and no congenital anomalies were found.5 Although low, approximately 4−7% as many subjects randomized to high-dose PHEN/TPM versus placebo discontinued the study due to anxiety-, sleep-, and depression-related AEs; no concerns with suicide were determined.5 Topiramate used at doses of 100−400 mg/day for migraine prophylaxis and treatment of seizures is associated with dose-dependent increased incidence of cognitive-associated events including confusion, psychomotor slowing, difficulty with concentration, attention, memory, and speech or language problems. More cognitive events occurred with the PHEN/TPM treatment groups (low-dose, 2.0%; mid-dose, 5.6%; high-dose, 7.8%) relative to placebo (1.7%); however, the clinical significance is unknown.5 Metabolic acidosis is a concern due to topiramate’s ability to inhibit CA leading to increased renal excretion of bicarbonate. No reports of severe metabolic acidosis occurred during the trial; however, 22 cases of mild, sustained metabolic acidosis which adversely affects bone structure and function occurred in the PHEN/TPM groups relative to 5 placebo cases.5 Lastly, cardiovascular AEs were evaluated. Results showed small mean increases in heart rate and arrhythmias for the PHEN/TPM groups.5 If approved, the FDA requests Vivus, Inc. to complete long-term trials to further evaluate these cardiovascular AEs.
In an October 2010 press release, Vivus, Inc. announced that it received a Complete Response Letter (CRL) from the FDA regarding its NDA for Qnexa stating that the NDA would not be approved in its present form.6 The FDA requested a comprehensive assessment of topiramate’s and phentermine/topiramate’s teratogenic potential, including a detailed plan and strategy to evaluate and mitigate the potential teratogenic risks in women of childbearing potential taking the drug for the treatment of obesity.6 Additionally, the FDA asked Vivus, Inc. to provide evidence that the elevation in heart rate associated with Qnexa does not increase the risk for major adverse cardiovascular events.6 No new clinical studies were requested in the CRL; however, the FDA requested that Vivus, Inc. formally submit results from recently completed clinical studies. At this writing, Vivus, Inc. is continuing efforts to secure regulatory approval for Qnexa in the U.S. They have submitted a briefing document to the FDA addressing items in the CRL7 and have attended an End-of-Review meeting where the FDA requested that Vivus, Inc. assess the feasibility of analyzing existing healthcare databases to determine the historical incidence of oral cleft in offspring of women treated with topiramate for migraine prophylaxis (100 mg).8 Vivus, Inc. anticipates continued dialogue with the FDA on planned resubmission of the Qnexa NDA.8
References
- Flegal K. M.; Carroll M. D.; Ogden C. L.; Curtin L. R. (2010) Prevalence and trends in obesity among US adults, 1999−2008. J. Am. Med. Assoc. 303, 235–241. [DOI] [PubMed] [Google Scholar]
- NIH/NHLBI, NAASO . (2000) The Practical guide: Identification, Evaluation, and Treatment of Overweight and Obesity in Adults, NIH, Bethesda, MD. [Google Scholar]
- Rothman R. B.; Baumann M. H. (2009) Appetite suppressants, cardiac valve disease and combination pharmacotherapy. Am. J. Ther. 16, 354–364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shank R. P.; Gardocki J. F.; Streeter A. J.; Maryanoff B. E. (2000) An overview of the preclinical aspects of topiramate: pharmacology, pharmacokinetics, and mechanism of action. Epilepsia 41, S3–S9. [PubMed] [Google Scholar]
- http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDrugsAdvisoryCommittee/UCM218824.pdf.
- Vivus, Inc. press release, October 28, 2010. http://ir.vivus.com/releasedetail.cfm?ReleaseID=524576.
- Vivus, Inc. press release, December 4, 2010. http://ir.vivus.com/releasedetail.cfm?ReleaseID=536626.
- Vivus, Inc. press release, January 21, 2011. http://ir.vivus.com/releasedetail.cfm?ReleaseID=544917.