

Abstract
External auditory canal (EAC) osteomas are rare, benign bony neoplasms that occur in wide range of patients. While chronic irritation and inflammation have been suggested as causal factors in several cases, significant data is lacking to support these suspicions. Symptoms are rare and can include hearing loss, vertigo, pain and tinnitus. Diagnosis is made based on a combination of clinical history and examination, radiographic imaging, and histopathology. Osteomas of the EAC are usually found incidentally and are unilateral and solitary. Computed tomography reveals a hyperdense, pedunculated mass arising from the tympanosquamous suture and lateral of the isthmus. Histopathologically, EAC osteomas are covered with periosteum and squamous epithelium, and consist of lamalleted bone surrounding fibrovascular channels with minimal osteocysts. Osteomas have historically been compared and contrasted with exostoses of the EAC. While they share similarities, more often than not it is possible to distinguish the two bony neoplasms based on clinical history and radiographic studies. Debate remains in the medical literature as to whether basic histopathology can distinguish osteomas of the EAC from exostoses. Surgical excision is the standard treatment for EAC osteomas, however close observation is considered acceptable in asymptomatic patients.
Keywords: Osteoma, External auditory canal, Exostosis, Radiology, Pathology
History
A 28-year-old male was referred to the Otorhinolaryngology clinic for a left ear mass that was incidentally found during a routine audiology evaluation. The patient related that his primary care physician had first noticed the lesion 2 years prior. He denied a history of trauma to the ear or hearing loss, but stated recurrent left-sided otitis media as well as frequent cerumen impactions. Clinical examination revealed a hard, irregularly shaped mass of the left anterior auditory canal measuring approximately 2.0 mm. The mass and surrounding skin were normal in color and no surface ulcerations were noted. The right ear showed no abnormalities. The patient’s health history was otherwise unremarkable and he denied participating, more than occasionally, in water sports.
Radiographic Features
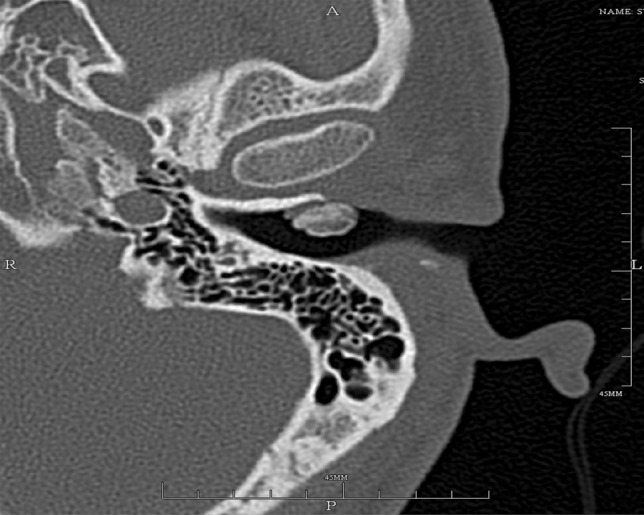
A non-contrast computerized tomographic (CT) scan of the skull base and temporal bones was obtained using 1 mm axial and coronal slices. The CT scan was remarkable for a non-obstructing, partially pedunuclated, hyperdense mass of the left anterior external auditory canal (Fig. 1). Review of the sections demonstrated the mass originated at the tympanosquamous suture (Fig. 2). The mass measured 1.0 cm by 0.6 cm, which was best appreciated on the axial images. The remainder of the structures of the middle and external ear were unremarkable, and the right ear showed no pathologic changes.
Fig. 1.
Computer tomographic (CT) images of the skull base and temporal bones show a left nonobstructing external auditory canal osteoma measuring 1 × 0.6 cm
Fig. 2.
Computer tomographic (CT) shows the lesion originating from the tympanosquamous or tympanomastoid suture line (arrow)
Diagnosis
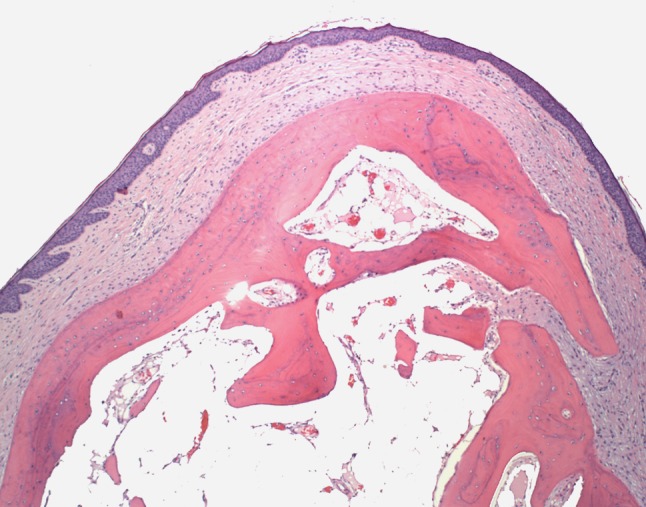
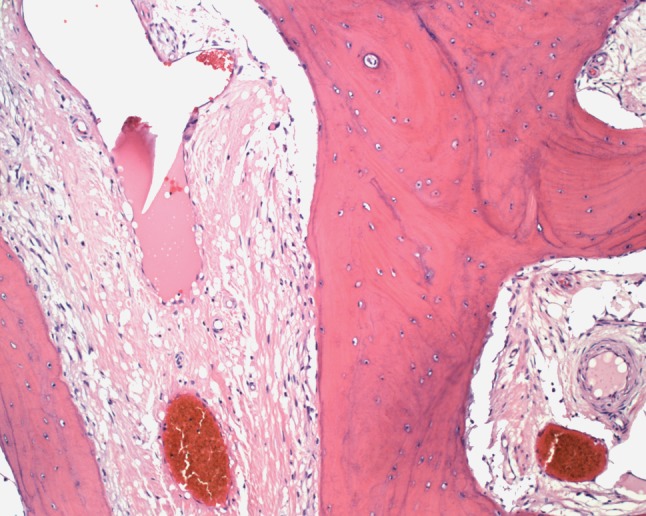
Histologic examination of hematoxylin and eosin stained slides revealed a mass of cancellous bone composed of trabeculae of bone and fibrofatty marrow surfaced by unremarkable epithelium (Fig. 3). Fibrovascular channels were seen with small vessels (Fig. 4).
Fig. 3.
Epithelium overlying a nodule of well-developed bone with fatty marrow
Fig. 4.

The fibrovascular channels with small vessels are readily identified
Discussion
Osteomas are considered bony neoplasms that show a predilection for the external auditory canal (EAC), mastoid cortex, facial bones, and mandible [1]. Osteomas of the EAC are considered benign tumors as they are non-invasive; however, they can cause significant symptoms due to mass effect and auditory canal obstruction [2–4].
Over the last several decades, there has been an ongoing debate over distinguishing osteoma from exostosis of the external auditory canal. Indolent by nature, both osteomata and exostoses of the EAC are often found incidentally. Of the two entities, exostosis is much more common with a reported incidence of 0.6% and occurring more frequently in middle aged men. While chronic irritation such as cold water exposure and repeated otitis externa are directly correlated with the development of exostosis, a clear etiology of osteoma of the EAC has yet to be discerned [5, 6]. While there are a few reported cases of osteamata of the EAC developing in surfers and cold water swimmers, the majority of medical literature provides only anecdotal evidence that suggests injury, inflammation, hormones, infection, developmental disorders, and genetic defects may play roles in the development of external auditory canal osteomata [1, 3, 6, 7]. Similarly, epidemiologic data is lacking for osteoma of the EAC, in part due to its low incidence. Medical literature suggests the neoplasm effects a wide range of age groups starting in the second decade of life and there is inconclusive, as well as conflicting, data regarding gender partiality [2, 4, 8].
Symptoms are similar between osteomas and exostoses and can include vertigo, paroxysmal tinnitus, sensorineural hearing loss, trigeminal neuralgia, and pain [3, 4]. There is a reported case of a cholesteatoma developing in conjunction with an osteoma of the external auditory canal, possibly secondary to impaired epithelial migration [2].
Radiographically, an osteoma appears as a single, unilateral, pedunculated hyperdense mass on computed topography (CT) scan originating from the tympanosquamous or tympanomastoid suture line and extending into the internal auditory canal (IAC) space with otherwise preserved canal dimensions [6, 7]. T1-weighted MRI may show a high-intensity signal representative of bone marrow within the neoplasm [3]. Similarly, exostoses are seen on CT scan as hyperdense lesions protruding into the IAC; however, they traditionally appear as multiple, bilateral, smooth-bordered, broad-based lesions without deep extension [5, 7].
Histologically, an osteama of the external auditory canal is generally covered with periosteum and squamous epithelium, and consists of lamellated bone with minimal osteocytes surrounding fibrovascular channels. The fibrovascular channels are often irregular and contain abundant fibrous tissue and sinusoidal blood vessels [6, 7, 9]. Furthermore, an osteoma can be compact, spongy, or mixed, with the compact type containing haversion systems and the spongy type containing trabecular bone with marrow [5]. In contrast, exostoses consist of parallel, concentric layers of subperiosteal bone with abundant osteocytes [3, 7]. Graham sought out to distinguish the two entities in his study that was published in 1979, where he concluded that the presence or absence of fibrovascular channels is a distinguishing histologic difference between an osteoma of the EAC and exostosis, respectively. However, findings reported in a more recent study by Fenton et al. [5, 6] which had a larger specimen number, concluded that basic histology alone cannot necessarily distinguish the two bony neoplasms as several cases of exostosis in their study had fibrovascular channels present on histology.
Due largely to the indolent nature of osteomata of the external auditory canal, patients are often asymptomatic and the lesions are found incidentally during unrelated evaluations. As such, periodic observation is a reasonable approach, saving surgical excision for symptomatic lesions or those where complications are anticipated. Surgical excision can usually be accomplished via an external approach through the external auditory meatus without complications [2, 8]. Prognosis is excellent.
Footnotes
Disclaimer: The opinions and assertions expressed herein are those of the author and are not to be construed as official or representing the views of the Department of the Navy or the Department of Defense.
References
- 1.Liétin B, et al. Osteoma of the internal auditory canal. European annals or otorhinolaryngology. Head Neck Dis. 2010;127:15–19. doi: 10.1016/j.anorl.2010.02.004. [DOI] [PubMed] [Google Scholar]
- 2.Orita Y, et al. Osteoma with cholesteatoma in the external auditory canal: case report. Int J Pediatr Otorhinolaryngol. 1998;43:289–293. doi: 10.1016/S0165-5876(98)00022-6. [DOI] [PubMed] [Google Scholar]
- 3.Venelin G, et al. Bilateral osteomas arising from the internal auditory canal: case report. Neurosurgery. 2008;62:E528–E529. doi: 10.1227/01.neu.0000316023.81786.b6. [DOI] [PubMed] [Google Scholar]
- 4.Denia A, et al. Extracanalicular Osteomas of the Temporal Bone. Arch Otolaryngol. 1979;105:706–709. doi: 10.1001/archotol.1979.00790240020005. [DOI] [PubMed] [Google Scholar]
- 5.Fenton JE, Turner J, Fagan PA. A histopathologic review of temporal bone exostosis and osteomata. Laryngoscope. 1996;106(5):624–628. doi: 10.1097/00005537-199605000-00020. [DOI] [PubMed] [Google Scholar]
- 6.Graham MD. Osteomas and exostosis of the external auditory canal. A clinical, histopathologic and scanning electron microscope study. Laryngoscope. 1979;88:566–572. doi: 10.1177/000348947908800422. [DOI] [PubMed] [Google Scholar]
- 7.Baik FM, et al. Comparative case series of exostosis and osteomas of the internal auditory canal. Ann Otol Rhinol Laryngol. 2011;120(4):255–260. doi: 10.1177/000348941112000407. [DOI] [PubMed] [Google Scholar]
- 8.Sheehy JL. Diffuse exostosis and osteomata of the external auditory canal: a report of 100 operations. Otolaryngol Head Neck Surg. 1982;90:337–342. [PubMed] [Google Scholar]
- 9.Kemink JL, Graham MD. Osteomas and exostosis of the external auditory canal–medical and surgical management. J Otolaryngol. 1982;11(2):101–106. [PubMed] [Google Scholar]