

Abstract
Warfarin is a commonly used oral anticoagulant with a narrow therapeutic range and large interindividual variability in daily dose. Compared with Caucasians, Chinese are known to require lower doses of warfarin. Differences between Caucasians and Chinese in the allelic frequencies of two genes, CYP2C9 and VKORC1, largely explain the difference in dose requirement. There are other genetic polymorphisms that may further explain the response to warfarin. The VKORC1 genotype is an important determinant of response to warfarin in Chinese, but some genetic variants found in other ethnic groups that have a large effect on warfarin response and dosing are not commonly found in Chinese. Therefore, it is important to recognize and beware of ethnic differences in the pharmacogenetics of the response to warfarin, especially in the design of algorithms to aid dosing in clinical practice.
Keywords: algorithm, Chinese, CYP2C9 gene, VKORC1 gene, warfarin
Introduction
Warfarin, a commonly used oral anticoagulant, is indicated for the prevention and treatment of thromboembolic events in patients with deep vein thrombosis, pulmonary embolism, atrial fibrillation and prosthetic heart valves. It is a racemic mixture of S-warfarin and R-warfarin, with S-warfarin being the more active isomer and having a greater therapeutic effect. As shown in Figure 1, these enantiomers are extensively metabolized by various cytochrome P450 enzymes. R-Warfarin is mainly metabolized by cytochrome P450 1A2 (CYP1A2), CYP2C19 and CYP3A4, while S-warfarin is predominantly metabolized by CYP2C9. Both enantiomers affect the coagulation cascade by inhibiting the activity of vitamin K epoxide reductase complex 1 (VKORC1) and thus interfering with the activation of clotting factors II, VII, IX and X (Figure 1). Warfarin has a narrow therapeutic window, with potentially life-threatening consequences for under- or overdosing; therefore, frequent monitoring of its effect, as measured by the international normalized ratio (INR), is warranted. Moreover, the large interindividual variations in dose response make warfarin dosing a challenging task. In general, the initial phase of warfarin dosing requires 4–6 weeks of frequent clinic visits, blood tests and fine adjustment of dosage. Besides patients' clinical characteristics, such as age, gender, bodyweight, concurrent medications, diet, comorbidities and patient compliance level [1], genetic variations have also been shown to have a large influence in warfarin dosing.
Figure 1.
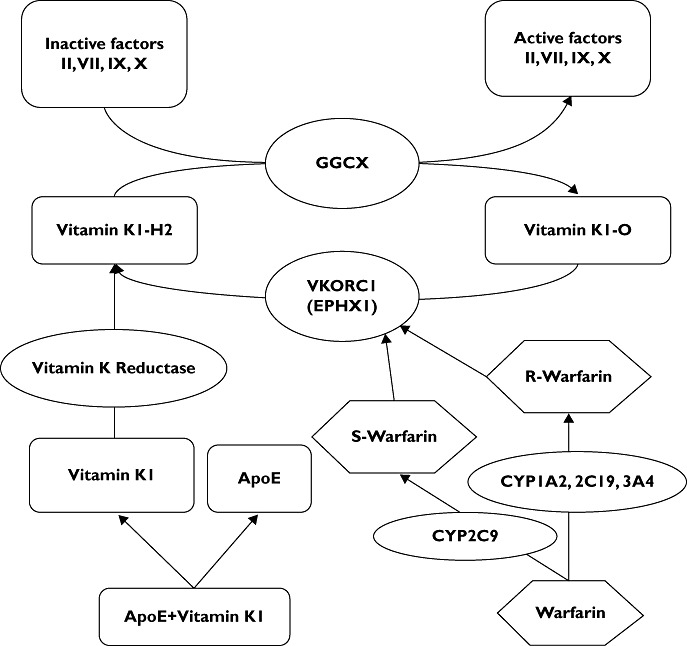
Mechanism of action for warfarin. Circulatory vitamin K1, being carried by apolipoprotein E (ApoE), is taken up by receptors. It is then reduced to vitamin K1H2 by vitamin K reductase. The reduced vitamin K1H2, as a cofactor for γ-glutamyl carboxylase (GGCX), converts the inactive Factors II, VII, IX and X to the active forms that are required for coagulation. Vitamin K epoxide reductase complex 1 (VKORC1) and possibly epoxide hydrolase 1 (EPHX1) catalyse the reduction of vitamin K1O. Warfarin, after being metabolized by cytochrome P450 isoforms to R-warfarin and S-warfarin, inhibits VKORC1, decreases the amount of vitamin K1H2 and thus interferes with the activation of clotting factors
Two genes, CYP2C9 and VKORC1, have been identified as important genetic determinants of warfarin dosing and have been studied intensively over the last decade. The most common CYP2C9 genotype among all ethnic groups is CYP2C9*1, found in around 80% of Caucasians and 95% of Chinese [2]; however, a major difference is observed between the Caucasians and Chinese in the allelic frequency of CYP2C9*2 (Table 1). About 10–15% of Caucasians harbour this allele, but is absent in most Chinese. Gene variants of CYP2C9 are associated with a lower warfarin dose requirement. In a meta-analysis by Lindh et al. [3], carriers of CYP2C9*2 and CYP2C9*3 alleles required lower warfarin doses than carriers of the wild-type CYP2C9*1 genotype (19.6% lower warfarin dose for those with *1/*2 genotype than those with *1/*1 genotype; 33.7% lower for *1/*3 genotype; 36.0% lower for *2/*2 genotype; 56.7% lower for *2/*3 genotype and 78.1% lower for *3/*3 genotype).
Table 1.
Allelic frequencies of selected polymorphisms in CYP2C9 in different countries/regions
| 2C9*1 (wild-type) (%) | 2C9*2 (rs 1799853) (%) | 2C9*3 (rs1057910) (%) | Country/region | Reference |
|---|---|---|---|---|
| 76 | 13 | 11 | Israel | [20] |
| 83 | 12 | 5 | USA | [35] |
| 82 | 11 | 7 | Sweden | [36] |
| 77.2 | 14.9 | 7.9 | Italy | [37] |
| 98 | 0 | 2 | Singapore* | [29] |
| 95.3 | 0 | 4.7 | Malaysia† | [38] |
| 97 | 0 | 3 | Taiwan | [30] |
| 96 | 0 | 4 | China | [39] |
Subjects comprised Chinese, Malays and Indians, with Chinese being the predominant group.
Subjects were all Malaysian Chinese.
Different allelic frequencies are also observed with the two most common single nucleotide polymorphisms (SNPs) in the VKORC1 gene, −1639G>A (rs9923231) and 1173C>T (rs9934438) (Table 2). Around 35% Caucasians carry the CC genotype of the 1173C>T variant, but only about 15% carry the TT genotype; however, the majority of Chinese (69–85%) carry the TT genotype, while only a handful of them (1–6%) carry the CC genotype. Similar findings are seen with the −1639G>A variant. Allelic frequency is the highest in the GG genotype (36%) and lowest in the AA genotype (15%) with the Caucasian population. The opposite trend is observed with the Chinese population; only 1% has the GG genotype and 83% the AA genotype. Yang et al. [4] reported that carriers with genotypes −1639GG and −1639GA required warfarin doses 102 and 52% higher, respectively, than those with −1639AA. When compared with the carriers with genotype 1173TT, carriers with genotypes 1173CC and 1173 CT required a dose of warfarin 97 and 44% higher, respectively.
Table 2.
Allelic frequencies of selected polymorphisms in VKORC1 in different countries/regions
| Reference SNP | Genotypes | Country/region | Reference | ||
|---|---|---|---|---|---|
| rs9934438 (1173C>T) | CC (%) | CT (%) | TT (%) | ||
| 36.8 | 46.9 | 16.3 | Italy | [40] | |
| 36.1 | 50.7 | 12.7 | USA | [13] | |
| 34 | 49 | 17 | France | [41] | |
| 1 | 14 | 85 | China | [41] | |
| 1.11 | 14.76 | 84.13 | China | [19] | |
| 6 | 25 | 69 | Hong Kong | [42] | |
| rs9923231 (–1639G>A) | AA | AG | GG | ||
| 14.9 | 48.9 | 36.2 | Sweden | [36] | |
| 16.5 | 48.2 | 35.3 | Sweden | [43] | |
| 79.8 | 18.3 | 1.9 | Taiwan | [44] | |
| 83.7 | 15.7 | 0.6 | China | [39] | |
| 85.76 | 13.29 | 0.95 | China | [19] | |
Warfarin dosing algorithm
Several warfarin dosing algorithms that incorporate clinical characteristics and genetic information have been developed for better estimation of warfarin dosing. None of these algorithms was intended to replace the requirement of INR monitoring, but to increase the accuracy and reduce the trial-and-error approach of warfarin dosing, especially during the initial phase. As shown by the International Warfarin Pharmacogenetics Consortium study [5], the addition of genetic information to clinical information increased the accuracy of dose estimation when compared with the clinical algorithm or fixed-dose approach and was especially beneficial to patients with higher risk of overdosing or underdosing.
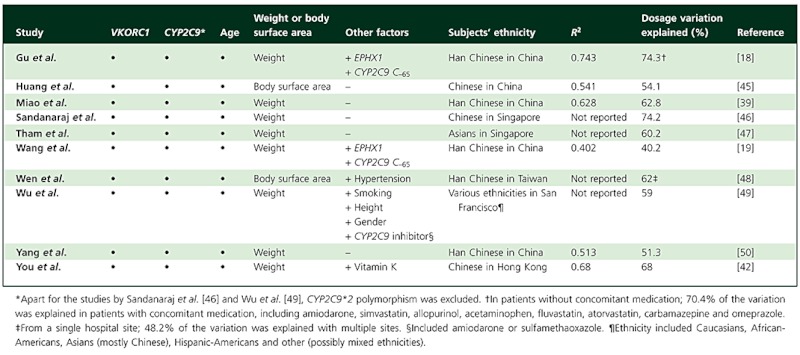
As mentioned earlier, ethnicity is one of the important factors that influence warfarin dose requirement, and variations in allelic frequencies among different ethnic groups have been observed. It comes as no surprise that ethnic-specific dosing algorithms have been developed, and some of them were for the Chinese. Chinese patients are known to be more sensitive to warfarin; they require lower doses of warfarin than Caucasians. In the study by Yu et al. [6], the mean dose of warfarin in Hong Kong Chinese was 3.3 mg daily, while the usual warfarin daily dose for Caucasians was 4–6 mg. Moreover, as shown in a study by You et al. [7], the Chinese had a high incidence of major bleeding, such as gastrointestinal bleeding, gross haematuria or haemoptysis, even when the INR was slightly increased but still within the therapeutic range. Studies that have included genotype information in the dosing algorithms for the Chinese population are summarized in Table 3. The use of clinical factors (for example, age, weight/body surface area, gender and concurrent medications) alone can account for approximately 20% of warfarin dose variability [8]. With the introduction of genetic factors into the algorithm, a higher percentage of dosage variation can be explained. As shown in Table 3, between 48 and 74% of the dose variation can now be explained with the incorporation of VKORC1 and CYP2C9 genotypes. One notable difference in most of the algorithms listed in Table 3, when compared with other algorithms for Caucasians, is the inclusion of the CYP2C9*3 variant but not the CYP2C9*2 variant. The main reason for the exclusion of the CYP2C9*2 variant in the algorithms is mostly due to its rarity in the Chinese population, as shown in Table 1[2, 9].
Table 3.
Summary of algorithms for warfarin dosage in Chinese populations
 |
Other genetic polymorphisms
Although the incorporation of CYP2C9 and VKORC1 can explain more warfarin dosage variation than clinical factors alone, there is at least 26% of the dose variability that remains unaccounted for. Other genes, such as CYP4F2, epoxide hydrolase 1 (EPHX1), γ-glutamyl carboxylase (GGCX), apolipoprotein E (ApoE) and CYP2C9 C−65, have been investigated recently. A summary of the effects of these genetic polymorphisms on warfarin dosage is listed in Table 4.
Table 4.
Summary of the effects of other genetic polymorphisms that might influence warfarin dosage
| Gene | Reference SNP | Country/region | Minor Variant | Frequency (%) | Contribution to dose variance (%) | Reference |
|---|---|---|---|---|---|---|
| CYP4F2 | rs2108622 | USA | T | 30 | 2 | [11] |
| USA | T | 25 | 4 | [12] | ||
| USA | T | 31.15 | 5 | [13] | ||
| China | T | 28 | 4 | [14] | ||
| Singapore** | T | 17 | 3 | [15] | ||
| Taiwan | T | 23.6 | Not significant | [16] | ||
| Singapore** | A† | 24.4 | 3 | [51] | ||
| EPHX1 | rs4653436 | USA | A | 31.8 | Not significant | [13] |
| China | A | 24.85 | Not reported‡ | [18] | ||
| China | A | 25.31 | Not reported‡ | [19] | ||
| rs1877724 | Taiwan | T | 31.95 | 1.84 | [16] | |
| Singapore** | T | 34.8 | 0.8 | [51] | ||
| rs1051740 | Israel | C | 25 | Not significant | [20] | |
| rs2234922 | Israel | G | 24.2 | Not significant | [20] | |
| GGCX | rs12714145 | Sweden | A | 40.8 | Not significant | [23] |
| USA | A | 29.7 | Not significant | [25] | ||
| China | A | 34.3 | 2.3 | [26] | ||
| China | T | 41.19 | Not significant | [19] | ||
| Taiwan | A | 32.3 | Not significant | [16] | ||
| rs11676382 | USA | G | 7.55 | 0.3 | [25] | |
| Taiwan | G | 0 | Not significant | [16] | ||
| ApoE | Sweden | ε4 | 19.1 | 6§ | [28] | |
| Singapore¶ | ε4 | 7 | Not significant | [29] | ||
| CYP2C9 C–65 | rs9332127 | USA | C | 0 | Not significant | [30] |
| Taiwan | C | 5.8 | Not reported** | [30] | ||
| China | C | 4.25 | Not reported** | [19] | ||
| China | C | 4.35 | Not reported** | [18] |
Subjects comprised of Chinese, Malays and Indians, with Chinese being the predominant group.
Genotypes were reported in reverse orientation.
Although the contribution to dose variance was not reported, it was reported that subjects with the A allele required a higher dose of warfarin.
Within the CYP2C9*1/*1 group, with age as a covariate.
Subjects comprised Chinese, Malays and Indians, with Chinese being the predominant group.
Although the contribution to dose variance was not reported, it was reported that subjects with the C allele required a lower dose of warfarin.
CYP4F2 is another cytochrome P450 enzyme that is involved in the metabolism of vitamin K, and its polymorphism could result in altered vitamin K levels as well as warfarin dose requirements [10]. About 30% of the Caucasian population carries the minor allele of SNP rs2108622, which explains 2–5% of the variance in dose [11–13]. A study by Cen et al. [14] showed that 28% Han Chinese carried a variant copy of CYP4F2 and reported that this polymorphism contributed to about 4% of the variance in warfarin dose of the Chinese population. Likewise, Singh et al. [15] reported that 17% of Asians (predominant with Chinese) carried the minor allele of CYP4F2. It was estimated that approximately 3% of the variation in warfarin dosage variance can be explained by CYP4F2. However, a study by Lee et al. [16] did not find that this polymorphism significantly influenced warfarin dosage in Chinese. Nonetheless, similar contributions of this SNP (2–5%) to warfarin dose variance were observed in both Caucasian and Chinese populations.
Epoxide hydrolase 1 is another subunit of VKORC1 (Figure 1), which is located in the endoplasmic reticulum [17]. A study by Carlquist et al. [13] in the USA showed that the frequencies of the genotypes GG, GA and AA for SNP rs4653436 were 44, 48.2 and 7.7%, respectively. However, no difference was found in warfarin dosage requirement among the different alleles. Gu et al. [18] and Wang et al. [19] reported that approximately 55% of the Chinese population carried the GG genotype, 41% the GA genotype and 4% the AA genotype. Both studies showed that there was a small but significant correlation between polymorphism of EPHX1 and warfarin dosing requirement. Gu et al. [18] demonstrated that patients with GG or GA genotypes required lower warfarin dosage than those with AA genotype, while Wang et al. [19] showed that EPHX1 was one of the significant variables to the warfarin dosing algorithm. A study by Loebstein et al. [20] has shown that two other SNPs (rs1051740 and rs2234922) were not significant in contributing to the warfarin dose variance. However, another SNP (rs1877724), reported by both Lee et al. [16] and Chan et al. [21], was shown to have an additional contribution to dose variance by 0.8–1.8%. Although more studies are needed before firm conclusions can be drawn, it appears that EPHX1 variants have different impacts in Caucasian and Chinese populations. Similar frequencies of minor alleles of EPHX1 variants were reported, around 25–35%, in the two populations, but EPHX1 variants added relatively small but significant contributions to warfarin dosage variance in the Chinese but not in the Caucasians.
As shown in Figure 1, GGCX is another enzyme essential for the vitamin K-dependent clotting factors and coagulation pathway [22]. Wadelius et al. [23] reported that the frequency of the A allele (minor allele) of SNP rs12714145 was 40.8% and that carriers of this allele would have a higher warfarin dosage requirement (3.3% more than those with the G allele) [24]. However, the allele did not contribute significantly to additional warfarin dosage variance. King et al. [25] also found that this SNP did not have any impact on warfarin dose prediction. The minor allelic frequency of this SNP in the Chinese population, as reported by Lee et al. [16], Wang et al. [19] and Huang et al. [26], is around 32–40%. Huang et al. [26] demonstrated that this variant could account for 2.3% of the variance of individual warfarin dose requirement, whereas Lee et al. [16] and Wang et al. [19] could not detect such a significant association. Lee et al. [16] also pointed out that a significant association of the GGCX polymorphism with warfarin dosing was observed in the Caucasian and Japanese populations, but this association could not be replicated in the Han Chinese population. Another SNP of GGCX, rs11676382, was reported by Lee et al. [16] and King et al. [25]. While King et al. [25] reported that 7.55% of Caucasians carried the minor allele (G allele) and contributed 0.3% to warfarin dosage variance, neither study could detect the G allele in the Chinese population. Unlike EPHX1, which has similar allelic frequency but different impact in different ethnicities, the impact from GGCX variants, if any, was small and similar across different ethnic groups.
Apolipoprotein E is a glycoprotein that plays a central role in the uptake of vitamin K [27]. Allelic frequencies of ε2, ε3 (wild-type) and ε4, as reported by Kohnke et al. [28], were 6.0, 74.9 and 19.1%, respectively, in a Swedish population. They demonstrated that ε4 homozygous patients required a significantly higher warfarin dose (56.9 mg week−1) than those with one or no ε4 alleles (34.3 and 34.6 mg week−1, respectively). Lal et al. [29] studied the influence of ApoE genotype on warfarin dose requirement in Asian patients (predominantly Chinese); 78% of the subjects carried the wild-type genotype, but no significant influence on warfarin dosing requirement was found among different ApoE genotypes.
Besides the most common CYP2C9*2 and CYP2C9*3 alleles, other CYP2C9 polymorphisms have also been studied and identified. A novel genotypic polymorphism, CYP2C9 C−65 (rs933127), was reported in Taiwan Han Chinese by Chern et al. [30]. The frequency of C–65 variant allele (GC or CC genotype) was 5.8% for the Taiwan Han Chinese, but not detectable in Caucasians. Carriers of this variant allele were found to require significantly lower daily warfarin doses than those with the GG genotype. Gu et al. [18] reported that Han Chinese with GC or CC genotypes required lower warfarin dosages (0.9 ± 0.2 mg day−1) than those with the GG genotype (3.3 ± 1.2 mg day−1). Similar findings were shown by Wang et al. [19]. Both Wang et al. [19] and Gu et al. [18] found that this variant allele was one of the strong predictors of warfarin dosage and was incorporated into their dosage algorithms.
The studies on polymorphisms of CYP4F2, EPHX1, GGCX, ApoE and CYP2C9 C−65 showed that these have minimal and often undetectable effects on warfarin requirement, yet they have demonstrated that their impacts are subject to the prevalence of genetic variants in the ethnic population. One good example of how this difference can affect the capability of warfarin dosing algorithms to explain dose variability is the prevalence of CYP2C9*8 among African-Americans. CYP2C9*8, another CYP2C9 polymoprhism, was reported by Scott et al. [31] as the most prevalent variant allele among African-Americans, instead of CYP2C9*2 or *3. Approximately one in 11 (0.047) African-Americans were carriers of this variant allele, while only one in 50 (0.010) Asians were carriers of this allele. As a result of lower frequencies of the more common alleles (e.g. CYP2C9*2 or *3), the warfarin dosing algorithm explains dose variability less well in African-Americans than in Caucasians. Thus, identification and incorporation of ethnic-specific genetic factors may facilitate better prediction of warfarin dosage in algorithms.
Possible pitfalls when evaluating results in Chinese/Asian populations
When Asians from China, Hong Kong, Taiwan, Singapore, Malaysia, Vietnam and other Southeast Asian or Asian countries are combined as a single group for investigation, information pertinent to the study (patient demographics and results) should be broken down into each ethnic group, because differences exist among ethnic groups. For example, Lee et al. [32] demonstrated that out of the five East Asian populations (Han Chinese from Taiwan, India, Indonesia, Philippines, Thailand and Vietnam) that they have studied, the VKORC1 haplotype structure in the Indian population was significantly different from the other four Asian populations. The H7 haplotype was the major haplotype in the Indian population (76%), whereas H1 haplotype was the predominant one in the rest of the populations studied. A similar finding was shown in a study by Gan et al. [33]; the allelic frequency distribution of VKORC1 genotypes was similar in the Chinese and Malay populations but different in the Indian population. The genotype frequencies for VKORC1−1639AA and −1639GG for all the study participants were 50 and 21%, respectively. When broken down by patients' ethnicity, however, the genotype frequencies for −1639AA and −1639GG were 67 and 6%, respectively, for Chinese and 7 and 80%, respectively, for Indians [33]. This study demonstrated that extra care should be taken when results are pooled from different populations, even from the same geographical area.
Another possible pitfall happens when pooling results of the Han Chinese population of different regions. Although Han Chinese is the largest subethnic group in China, numerous subethnic groups are found in China. Different allelic frequencies have been found among different Chinese subethnic groups, as shown by Ross et al. [34]. The C allele of CYP2C9*3 is absent in the Han population; however, it was present in more than 10% of the Tu, Tujia and Xibo subethnic groups. All Han and Oroqen populations were found to be carriers of the T allele of VKORC1 SNP rs9923231, while only 75% of the She population were carriers of this allele. With the growth in China's urbanization and globalization, more ethnic minorities who used to live in rural communities are moving to the big cities. With interethnic marriages, the ethnic minorities will be less genetically and culturally distinct. This means that ethnic minorities will be less easily identified by their names, their place of abode and their cultural habits.
Conclusions
There is no doubt that different genotype compositions exist between different ethnic groups; the concept of ‘one size fits all’ might not be applicable to warfarin dosing algorithms. Although there may still be pharmacogenetic factors influencing warfarin response that have eluded us, what we already know serves to heighten our awareness of the important contribution of genetic polymorphism to dosage variability. Warfarin, a medication with a narrow therapeutic window that is commonly used, is a good starting point for personalized medicine and demonstrates its potential and importance. A better understanding of the genetic polymorphisms in individuals can facilitate the dosing of warfarin in a more accurate and timely manner that could lead to better clinical outcomes.
Competing Interests
There are no competing interests to declare.
REFERENCES
- 1.Loebstein R, Yonath H, Peleg D, Almog S, Rotenberg M, Lubetsky A, Roitelman J, Harats D, Halkin H, Ezra D. Interindividual variability in sensitivity to warfarin-nature or nurture? Clin Pharmacol Ther. 2001;70:159–64. doi: 10.1067/mcp.2001.117444. [DOI] [PubMed] [Google Scholar]
- 2.Lal S, Rao Jada S, Xiang X, Lim W-T, Lee EJD, Chowbay B. Pharmacogenetics of target genes across the warfarin pharmacological pathway. Clin Pharmacokinet. 2006;45:1189–200. doi: 10.2165/00003088-200645120-00004. [DOI] [PubMed] [Google Scholar]
- 3.Lindh J, Holm L, Andersson M, Rane A. Influence of CYP2C9 genotype on warfarin dose requirements – a systematic review and meta-analysis. Eur J Clin Pharmacol. 2009;65:365–75. doi: 10.1007/s00228-008-0584-5. [DOI] [PubMed] [Google Scholar]
- 4.Yang L, Ge W, Yu F, Zhu H. Impact of VKORC1 gene polymorphism on interindividual and interethnic warfarin dosage requirement – a systematic review and meta analysis. Thromb Res. 2010;125:e159–e66. doi: 10.1016/j.thromres.2009.10.017. [DOI] [PubMed] [Google Scholar]
- 5.International Warfarin Pharmacogenetics Consortium. Estimation of the warfarin dose with clinical and pharmacogenetic data. N Engl J Med. 2009;360:753–64. doi: 10.1056/NEJMoa0809329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yu HCM, Chan TYK, Critchley JAJH, Woo KS. Factors determining the maintenance dose of warfarin in Chinese patients. QJM. 1996;89:127–36. doi: 10.1093/qjmed/89.2.127. [DOI] [PubMed] [Google Scholar]
- 7.You JHS, Chan FWH, Wong RSM, Cheng G. Is INR between 2.0 and 3.0 the optimal level for Chinese patients on warfarin therapy for moderate-intensity anticoagulation? Br J Clin Pharmacol. 2005;59:582–7. doi: 10.1111/j.1365-2125.2005.02361.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gladding P, Mackay J, Zeng I, Stewart R, Prabkahar R, Webster M, White H. A simulation of warfarin maintenance dose requirement using a pharmacogenetic algorithm in an ethnically diverse cohort. Personalized Medicine. 2010;7:319–25. doi: 10.2217/pme.10.24. [DOI] [PubMed] [Google Scholar]
- 9.Gage BF. Pharmacogenetics-based coumarin therapy. Hematology Am Soc Hematol Educ Program. 2006:467–73. doi: 10.1182/asheducation-2006.1.467. [DOI] [PubMed] [Google Scholar]
- 10.McDonald MG, Rieder MJ, Nakano M, Hsia CK, Rettie AE. CYP4F2 Is a vitamin K1 oxidase: an explanation for altered warfarin dose in carriers of the V433M variant. Mol Pharmacol. 2009;75:1337–46. doi: 10.1124/mol.109.054833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Caldwell MD, Awad T, Johnson JA, Gage BF, Falkowski M, Gardina P, Hubbard J, Turpaz Y, Langaee TY, Eby C, King CR, Brower A, Schmelzer JR, Glurich I, Vidaillet HJ, Yale SH, Qi Zhang K, Berg RL, Burmester JK. CYP4F2 genetic variant alters required warfarin dose. Blood. 2008;111:4106–12. doi: 10.1182/blood-2007-11-122010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sagreiya H, Berube C, Wen A, Ramakrishnan R, Mir A, Hamilton A, Altman RB. Extending and evaluating a warfarin dosing algorithm that includes CYP4F2 and pooled rare variants of CYP2C9. Pharmacogenet Genomics. 2010;20:407–13. doi: 10.1097/FPC.0b013e328338bac2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Carlquist J, Horne B, Mower C, Park J, Huntinghouse J, McKinney J, Muhlestein J, Anderson J. An evaluation of nine genetic variants related to metabolism and mechanism of action of warfarin as applied to stable dose prediction. J Thromb Thrombolysis. 2010;30:358–64. doi: 10.1007/s11239-010-0467-3. [DOI] [PubMed] [Google Scholar]
- 14.Cen HJ, Zeng WT, Leng XY, Huang M, Chen X, Li JL, Huang ZY, Bi HC, Wang XD, He YL, He F, Zhou RN, Zheng QS, Zhao LZ. CYP4F2 rs2108622: a minor significant genetic factor of warfarin dose in Han Chinese patients with mechanical heart valve replacement. Br J Clin Pharmacol. 2010;70:234–40. doi: 10.1111/j.1365-2125.2010.03698.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Singh O, Sandanaraj E, Subramanian K, Lee LH, Chowbay B. Influence of CYP4F2 rs2108622 (V433M) on warfarin dose requirement in Asian patients. Drug Metab Pharmacokinet. 2011;26:130–6. doi: 10.2133/dmpk.dmpk-10-rg-080. [DOI] [PubMed] [Google Scholar]
- 16.Lee MM, Chen CH, Chou CH, Lu LS, Chuang HP, Chen YT, Saleem AN, Wen MS, Chen JJ, Wu JY, Chen YT. Genetic determinants of warfarin dosing in the Han-Chinese population. Pharmacogenomics. 2009;10:1905–13. doi: 10.2217/pgs.09.106. [DOI] [PubMed] [Google Scholar]
- 17.Wadelius M, Pirmohamed M. Pharmacogenetics of warfarin: current status and future challenges. Pharmacogenomics J. 2007;7:99–111. doi: 10.1038/sj.tpj.6500417. [DOI] [PubMed] [Google Scholar]
- 18.Gu Q, Kong Y, Schneede J, Xiao YB, Chen L, Zhong QJ, Wang XF, Hao J, Chen BC, Chen JJ. VKORC1-1639G>A, CYP2C9, EPHX1691A>G genotype, body weight, and age are important predictors for warfarin maintenance doses in patients with mechanical heart valve prostheses in southwest China. Eur J Clin Pharmacol. 2010;66:1217–27. doi: 10.1007/s00228-010-0863-9. [DOI] [PubMed] [Google Scholar]
- 19.Wang TL, Li HL, Tjong WY, Chen QS, Wu GS, Zhu HT, Hou ZS, Xu S, Ma SJ, Wu M, Tai S. Genetic factors contribute to patient-specific warfarin dose for Han Chinese. Clin Chim Acta. 2008;396:76–9. doi: 10.1016/j.cca.2008.07.005. [DOI] [PubMed] [Google Scholar]
- 20.Loebstein R, Vecsler M, Kurnik D, Austerweil N, Gak E, Halkin H, Almog S. Common genetic variants of microsomal epoxide hydrolase affect warfarin dose requirements beyond the effect of cytochrome P450 2C9. Clin Pharmacol Ther. 2005;77:365–72. doi: 10.1016/j.clpt.2005.01.010. [DOI] [PubMed] [Google Scholar]
- 21.Chan SL, Thalamuthu A, Goh BC, Chia KS, Chuah B, Wong A, Lee SC. Exon sequencing and association analysis of EPHX1 genetic variants with maintenance warfarin dose in a multiethnic Asian population. Pharmacogenet Genomics. 2011;21:35–41. doi: 10.1097/fpc.0b013e328341b68f. [DOI] [PubMed] [Google Scholar]
- 22.Presnell S, Stafford D. The vitamin K-dependent carboxylase. Thromb Haemost. 2002;87:937–46. [PubMed] [Google Scholar]
- 23.Wadelius M, Chen LY, Downes K, Ghori J, Hunt S, Eriksson N, Wallerman O, Melhus H, Wadelius C, Bentley D, Deloukas P. Common VKORC1 and GGCX polymorphisms associated with warfarin dose. Pharmacogenomics J. 2005;5:262–70. doi: 10.1038/sj.tpj.6500313. [DOI] [PubMed] [Google Scholar]
- 24.Chen LY, Eriksson N, Gwilliam R, Bentley D, Deloukas P, Wadelius M. Gamma-glutamyl carboxylase (GGCX) microsatellite and warfarin dosing. Blood. 2005;106:3673–4. doi: 10.1182/blood-2005-04-1711. [DOI] [PubMed] [Google Scholar]
- 25.King C, Deych E, Milligan P, Eby C, Lenzini P, Grice G, Porche-Sorbet R, Ridker P, Gage B. Gamma-glutamyl carboxylase and its influence on warfarin dose. Thromb Haemost. 2010;104:750–4. doi: 10.1160/TH09-11-0763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Huang S-W, Xiang XD-K, Huang L, Chen B-L, An B-Q, Li G-F, Luo Z-Y. Influence of GGCX genotype on warfarin dose requirements in Chinese patients. Thromb Res. 2011;127:131–4. doi: 10.1016/j.thromres.2010.10.027. [DOI] [PubMed] [Google Scholar]
- 27.Stehle S, Kirchheiner J, Lazar A, Fuhr U. Pharmacogenetics of oral anticoagulants: a basis for dose individualization. Clin Pharmacokinet. 2008;47:565–94. doi: 10.2165/00003088-200847090-00002. [DOI] [PubMed] [Google Scholar]
- 28.Kohnke H, Sörlin K, Granath G, Wadelius M. Warfarin dose related to apolipoprotein E (APOE) genotype. Eur J Clin Pharmacol. 2005;61:381–8. doi: 10.1007/s00228-005-0936-3. [DOI] [PubMed] [Google Scholar]
- 29.Lal S, Sandanaraj E, Jada SR, Kong M-C, Lee L-H, Goh B-C, Lee S-C, Chowbay B. Influence of APOE genotypes and VKORC1 haplotypes on warfarin dose requirements in Asian patients. Br J Clin Pharmacol. 2008;65:260–4. doi: 10.1111/j.1365-2125.2007.03053.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Chern HD, Ueng TH, Fu YP, Cheng CW. CYP2C9 polymorphism and warfarin sensitivity in Taiwan Chinese. Clin Chim Acta. 2006;367:108–13. doi: 10.1016/j.cca.2005.11.026. [DOI] [PubMed] [Google Scholar]
- 31.Scott SA, Jaremko M, Lubitz SA, Kornreich R, Halperin JL, Desnick RJ. CYP2C9*8 is prevalent among African–Americans: implications for pharmacogenetic dosing. Pharmacogenomics. 2009;10:1243–55. doi: 10.2217/pgs.09.71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lee MTM, Chen CH, Chuang HP, Lu LS, Chou CH, Chen YT, Liu CY, Wen MS, Lu JJ, Chang CF, Wu JY, Chen YT. VKORC1 haplotypes in five East-Asian populations and Indians. Pharmacogenomics. 2009;10:1609–16. doi: 10.2217/pgs.09.80. [DOI] [PubMed] [Google Scholar]
- 33.Gan G, Phipps M, Lee M, Lu L, Subramaniam R, Bee P, Chang S. Contribution of VKORC1 and CYP2C9 polymorphisms in the interethnic variability of warfarin dose in Malaysian populations. Ann Hematol. 2011;90:635–41. doi: 10.1007/s00277-010-1119-6. [DOI] [PubMed] [Google Scholar]
- 34.Ross KA, Bigham AW, Edwards M, Gozdzik A, Suarez-Kurtz G, Parra EJ. Worldwide allele frequency distribution of four polymorphisms associated with warfarin dose requirements. J Hum Genet. 2010;55:582–89. doi: 10.1038/jhg.2010.73. [DOI] [PubMed] [Google Scholar]
- 35.Aquilante CL, Langaee TY, Lopez LM, Yarandi HN, Tromberg JS, Mohuczy D, Gaston KL, Waddell CD, Chirico MJ, Johnson JA. Influence of coagulation factor, vitamin K epoxide reductase complex subunit 1, and cytochrome P450 2C9 gene polymorphisms on warfarin dose requirements. Clin Pharmacol Ther. 2006;79:291–302. doi: 10.1016/j.clpt.2005.11.011. [DOI] [PubMed] [Google Scholar]
- 36.Wadelius M, Chen LY, Lindh JD, Eriksson N, Ghori MJR, Bumpstead S, Holm L, McGinnis R, Rane A, Deloukas P. The largest prospective warfarin-treated cohort supports genetic forecasting. Blood. 2009;113:784–92. doi: 10.1182/blood-2008-04-149070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hamberg AK, Wadelius M, Lindh JD, Dahl ML, Padrini R, Deloukas P, Rane A, Jonsson EN. A pharmacometric model describing the relationship between warfarin dose and INR response With respect to variations in CYP2C9, VKORC1, and age. Clin Pharmacol Ther. 2010;87:727–34. doi: 10.1038/clpt.2010.37. [DOI] [PubMed] [Google Scholar]
- 38.Ngow H, Wan Khairina W, Teh L, Lee W, Harun R, Ismail R, Salleh M. CYP2C9 polymorphism: prevalence in healthy and warfarin-treated Malay and Chinese in Malaysia. Singapore Med J. 2009;50:490–3. [PubMed] [Google Scholar]
- 39.Miao L, Yang J, Huang C, Shen Z. Contribution of age, body weight, and CYP2C9 and VKORC1 genotype to the anticoagulant response to warfarin: proposal for a new dosing regimen in Chinese patients. Eur J Clin Pharmacol. 2007;63:1135–41. doi: 10.1007/s00228-007-0381-6. [DOI] [PubMed] [Google Scholar]
- 40.D'Andrea G, D'Ambrosio RL, Di Perna P, Chetta M, Santacroce R, Brancaccio V, Grandone E, Margaglione M. A polymorphism in the VKORC1 gene is associated with an interindividual variability in the dose-anticoagulant effect of warfarin. Blood. 2005;105:645–9. doi: 10.1182/blood-2004-06-2111. [DOI] [PubMed] [Google Scholar]
- 41.Larramendy-Gozalo C, Yang J, Verstuyft C, Bodin L, Dubert L, Zhang Y, Xu C, Fan L, Jaillon P, Becquemont L. Genetic polymorphism of vitamin K epoxide reductase (VKORC1) 1173C>T in a Chinese and a Caucasian population. Basic Clin Pharmacol Toxicol. 2006;98:611–3. doi: 10.1111/j.1742-7843.2006.pto_440.x. [DOI] [PubMed] [Google Scholar]
- 42.You J, Wong R, Waye M, Mu Y, Lim C, Choi K-c CG. Warfarin dosing algorithm using clinical, demographic and pharmacogenetic data from Chinese patients. J Thromb Thrombolysis. 2011;31:113–8. doi: 10.1007/s11239-010-0497-x. [DOI] [PubMed] [Google Scholar]
- 43.Scott SA, Khasawneh R, Peter I, Kornreich R, Desnick RJ. Combined CYP2C9, VKORC1 and CYP4F2 frequencies among racial and ethnic groups. Pharmacogenomics. 2010;11:781–91. doi: 10.2217/pgs.10.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Yuan HY, Chen JJ, Lee MTM, Wung JC, Chen YF, Charng MJ, Lu MJ, Hung CR, Wei CY, Chen CH, Wu JY, Chen YT. A novel functional VKORC1 promoter polymorphism is associated with inter-individual and inter-ethnic differences in warfarin sensitivity. Hum Mol Genet. 2005;14:1745–51. doi: 10.1093/hmg/ddi180. [DOI] [PubMed] [Google Scholar]
- 45.Huang SW, Chen HS, Wang XQ, Huang L, Xu DL, Hu XJ, Huang ZH, He Y, Chen KM, Xiang DK, Zou XM, Li Q, Ma LQ, Wang HF, Chen BL, Li L, Jia YK, Xu XM. Validation of VKORC1 and CYP2C9 genotypes on interindividual warfarin maintenance dose: a prospective study in Chinese patients. Pharmacogenet Genomics. 2009;19:226–34. doi: 10.1097/FPC.0b013e328326e0c7. [DOI] [PubMed] [Google Scholar]
- 46.Sandanaraj E, Lai S, Cheung Y, Xiang X, Kong M, Lee L, Ooi L, Chowbay B. VKORC1 diplotype-derived dosing model to explain variability in warfarin dose requirements in Asian patients. Drug Metab Pharmacokinet. 2009;24:365–75. doi: 10.2133/dmpk.24.365. [DOI] [PubMed] [Google Scholar]
- 47.Tham LS, Goh BC, Nafziger A, Guo JY, Wang LZ, Soong R, Lee SC. A warfarin-dosing model in Asians that uses single-nucleotide polymorphisms in vitamin K epoxide reductase complex and cytochrome P450 2C9. Clin Pharmacol Ther. 2006;80:346–55. doi: 10.1016/j.clpt.2006.06.009. [DOI] [PubMed] [Google Scholar]
- 48.Wen MS, Lee MTM, Chen JJ, Chuang HP, Lu LS, Chen CH, Lee TH, Kuo CT, Sun FM, Chang YJ, Kuan PL, Chen YF, Charng MJ, Ray CY, Wu JY, Chen YT. Prospective study of warfarin dosage requirements based on CYP2C9 and VKORC1 genotypes. Clin Pharmacol Ther. 2008;84:83–9. doi: 10.1038/sj.clpt.6100453. [DOI] [PubMed] [Google Scholar]
- 49.Wu AH, Wang P, Smith A, Haller C, Drake K, Linder M, Valdes R. Dosing algorithm for warfarin using CYP2C9 and VKORC1 genotyping from a multi-ethnic population: comparison with other equations. Pharmacogenomics. 2008;9:169–78. doi: 10.2217/14622416.9.2.169. [DOI] [PubMed] [Google Scholar]
- 50.Yang J, Huang C, Shen Z, Miao L. Contribution of 1173C>T polymorphism in the VKORC1 gene to warfarin dose requirements in Han Chinese patients receiving anticoagulation. Int J Clin Pharmacol Ther. 2011;49:23–9. doi: 10.5414/cpp49023. [DOI] [PubMed] [Google Scholar]
- 51.Chan SL, Suo C, Lee SC, Goh BC, Chia KS, Teo YY. Translational aspects of genetic factors in the prediction of drug response variability: a case study of warfarin pharmacogenomics in a multi-ethnic cohort from Asia. Pharmacogenomics J. doi: 10.1038/tpj.2011.7. [Epub ahead of print] 2011. doi: 10.1038/tpj.2011.7. [DOI] [PubMed] [Google Scholar]