

Isfahan province of Iran is now globally well known for its high prevalence of Multiple Sclerosis (MS).[1–3] Fifteen years ago, this fact was in spite of primary north–south based expectations (MS gradient hypothesis) in which Isfahan, as a part of Iran, could only be a low-risk area with prevalence of less than 5/100,000.[4–6] During the last decade, serial population-based studies by Isfahan MS society (IMSS) reformed our knowledge about MS epidemiology in our province. The first IMSS study was performed between 2004 and 2005, reporting a period prevalence of 35.5/100,000. This report put Isfahan as a medium- to high-risk area.[1] The following year, a more comprehensive study was performed reporting a period prevalence of 43.8/100,000 between April 2003 and July 2006. This study also reported an incidence rate of 3.64/100,000 for the year 2005.[2] IMSS final study was performed in 2010, reporting a period prevalence of 73.3/100,000 between April 2003 and July 2010 and an incidence rate of 9.1/100,000 in 2009. These values were dramatically higher than previous reports, and of course, harbinger of a disaster. According to the latter report, Isfahan was addressed as one of the most high-risk regions for MS in Asia and Oceania.[3] During the period from July 2010 to date (end of July 2011), IMSS has identified 443 new cases (unpublished data), providing an incidence figure of ~ 9.22/100,000.
Indeed, the incidence of MS in our province is still increasing and this horrible fact should be a subject of prevention and plan. To prevent, we need to know the causal factors; and to plan, we need to know how this process will progress, and probably, when it will be terminated. As highlighted in an article in this issue of International Journal of Preventive Medicine, MS prevention is limited to control of its environmental risk factors in which vitamin D deficiency is of crucial importance.
We recommend a screening program for this deficiency throughout the province and request the National Ministry of Health of I. R. Iran to provide adequate fundamentals to it. In the above-mentioned study, we introduce the general and particular candidates for such a program.
Here, in this editorial, we aimed to trace and justify the epidemiologic changes of MS in our province. Monitoring the age-based structure of Isfahan population over a short duration can provide interesting clues about this issue. In Figure 1, we have evaluated the age distribution of the population of our province by extracting data from two Iranian census studies in 1996 and 2006. Comparing these two populations, we could highlight an age-based structural shift between 1996 and 2006. In 1996 [point “A” in Figure 1], the age group of 10–14 years was responsible for the uttermost proportion of the general population; and interestingly, in 2006 [point “B” in Figure 1], this distributional peak was shifted to the age group of 20–24 years. The origin of this structural peak is attributable to the population explosion of Iran in the 80s. In the meantime, i.e. the first and second decades of 21st century, our public health system is coping with the burden of diseases that affect this large young-aged population. Indeed, MS mostly affects young adults (i.e. 20–40 years old) [the pink-colored section in Figure 1]; hence, this structural shift can be considered as one of the most important determinants for MS increase. Now, in 2011 [point “C” in Figure 1] in comparison to 2009, the population peak has been shifted from 23–27 to 25–29 years, and as mentioned above, the incidence has approximately changed from 9.1/100,000 to ~9.22/100,000. Unfortunately, we postulate that this trend of increase is ongoing in the coming years [points “D” and “E” in Figure 1]. According to one of our previous reports, MS in people of Isfahan has the highest rates among 30–39 year age group and then decreases in the older age ranges.[1] This might suggest that MS incidence remains at high rates until the population peak is located in the 20–40 years range (i.e. until year 2023) and then will slowly decrease [point “F” in Figure 1]. In this respect, we anticipate that the period for downward slope of MS incidence would be the period between 2023 and 2026. Taken together, these epidemiologic anticipations about the future of MS in Isfahan would be worth considering for their potential in leading the governmental health policy in managing the crisis.
Figure 1.
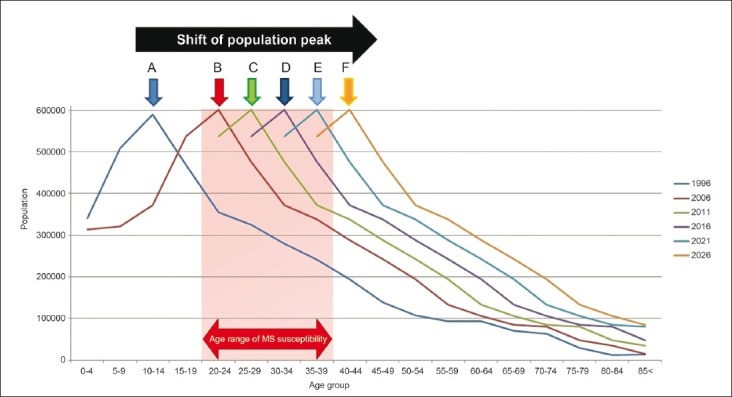
Distribution of the population of Isfahan in two Iranian censuses (1996 and 2006) and four epidemiologic anticipations for the years 2011, 2016, 2021, and 2026
ACKNOWLEDGMENT
The authors are very grateful to Drs. Ziba Farajzadegan and Peyman Roomizadeh (Isfahan University of Medical Sciences, Medical school) for their valuable advices on the manuscript.
Footnotes
Source of Support: Isfahan University of Medical Sciences, Medical school
Conflict of Interest: None declared.
REFERENCES
- 1.Etemadifar M, Janghorbani M, Shaygannejad V, Ashtari F. Prevalence of multiple sclerosis in Isfahan, Iran. Neuroepidemiology. 2006;27:39–44. doi: 10.1159/000094235. [DOI] [PubMed] [Google Scholar]
- 2.Saadatnia M, Etemadifar M, Maghzi AH. Multiple sclerosis in Isfahan, Iran. Int Rev Neurobiol. 2007;79:357–75. doi: 10.1016/S0074-7742(07)79016-5. [DOI] [PubMed] [Google Scholar]
- 3.Etemadifar M, Maghzi AH. Sharp increase in the incidence and prevalence of multiple sclerosis in Isfahan, Iran. Mult Scler. 2011;17:1022–7. doi: 10.1177/1352458511401460. [DOI] [PubMed] [Google Scholar]
- 4.Kurtzke JF. A reassessment of the distribution of multiple sclerosis.Part one. Acta Neurol Scand. 1975;51:110–36. doi: 10.1111/j.1600-0404.1975.tb01364.x. [DOI] [PubMed] [Google Scholar]
- 5.Kurtzke JF. Epidemiologic contributions to multiple sclerosis: An overview. Neurology. 1980;30:61–79. doi: 10.1212/wnl.30.7_part_2.61. [DOI] [PubMed] [Google Scholar]
- 6.Compston A. Distribution of multiple sclerosis. In: Compston A, Ebers G, Lassman H, MacDonald I, Matthews B, Wekerle H, editors. McAlpine's Multiple Sclerosis. Edinburgh: Churchill Livingston; 1998. pp. 63–100. [Google Scholar]