

Abstract
Aims:
This study aims to review the economic cost of childhood (0-18 years) unintentional injuries (UI) and focuses upon comparing the cost burden between developing and developed countries.
Methods:
Articles were selected from PUBMED using the search words “Economic Cost”, “Unintentional injuries” and “Children”. Nine articles were selected.
Results:
Studies in China focused upon cost to hospitals, in Bangladesh they focused on personal payment in rural areas, and in Vietnam they focused upon community-based cost analysis. There was one study from Norway on UI at home. There were 5 articles from the USA focusing on submersion injury, UI insurance, unintentional traumatic brain injury, UI due to firearms and UI medical costs. The cost of childhood UI is enormous, ranging from US $516,938 to US $9,550,704 per year. This represents a large economic burden on society. Additionally, there is a large gap between lower-middle income countries (LMIC) and high income countries (HIC) in the burden of injury, injury health care and insurance systems.
Conclusion:
Different bases and contexts of studies make it difficult to draw a solid conclusion about the amount of costs of UI among children. Therefore, more studies of children's unintentional injuries should be carried out in low and middle income countries.
Keywords: Children, cost, high-income countries, low and middle income countries, unintentional injuries
INTRODUCTION
Childhood injuries have emerged as leading global public health problem with direct and indirect economic burdens related to premature morbidity and mortality of the children.[1] Large numbers of children and youths over the world are killed as a result of unintentional injuries (UIs), and are estimated to represent 90% of 950,000 annual deaths, which makes them the primary cause of death for children aged 10–19 years.[2,3]
The top five causes of unintentional injuries published by the WHO are traffic accidents, drowning, poisoning, burns and falls. Other injuries include fractures, joint and muscle injuries, open wounds, and internal organ injuries. Children's unintentional injuries are usually affected by economic situations, cultural, habitual and living conditions and have obvious regional and demographical features.[4] For instance, in rural Bangladesh, because of poor economic status, cutting was the major cause of childhood unintentional injuries, since farming or household work is common in that area.[5]
Many risk factors lead to unintentional injuries. Poverty is one of the leading factors contributing to high UI incidence, even in high income countries. However, the burden of childhood injury is heaviest in the poorer countries with lower family incomes.[3] Another important risk factor is unsafe environment settings and facilities. Additionally, lack of safety education and training for children and parents raises the risk of unintentional injuries in children.
Injuries as a major public health problem increase disability and death, and also represent a great economic burden.[2] The direct and indirect costs of unintentional injuries in children were categorized as follows: medical care treatment, length of stay (LOS) in hospital, medical insurance, vehicle repair costs, legal costs, loss of schooling, and loss of income to parents resulting from absence from work to care for the child. Moreover, long-term economic costs should consider premature death; rehabilitation; loss of healthy years in children (permanent disabilities); and the inability of those with serious disabilities to work to the full extent.[3] In relation to losses of healthy days, child unintentional injuries represent a much larger portion than adult injuries, and disability adjusted life years (DALY) is higher in this age group. However, lack of global data on the cost of unintentional child injuries means there is a great need for the analysis of unintentional injuries costs among children.[6]
The objective of this study is to review the economic cost of unintentional injuries focusing on children aged 0 to 18 years. In addition, the cost burden of childhood unintentional injuries in both low-and-middle-income countries and high-income countries will also be examined.
METHODS
The articles were searched from database Pubmed. “Economic Cost”, “unintentional injuries” and “children” as the initial search words identified in total 47 articles. The search was then further refined to indentify only English language articles. The number of articles thus was reduced to 46. The procedure is described in Figure 1.
Figure 1.
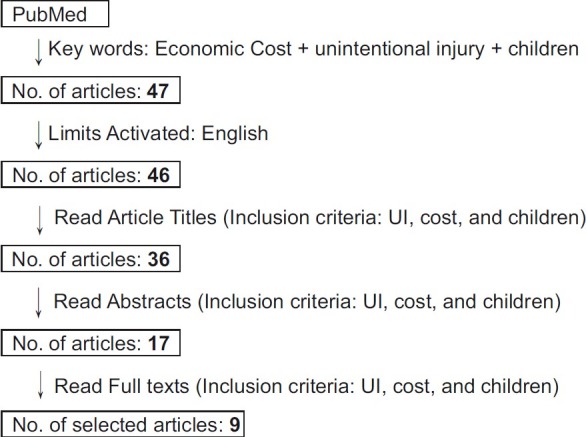
Number of articles used for review (PubMed)
Inclusion criteria
Firstly, unintentional injury is one of the principle baselines to identify the types of injuries. We have used the following definition of unintentional injuries: “damage to the body resulting from acute exposure to thermal, mechanical, electrical, or chemical energy or from the absence of such essentials as heat or oxygen.”[7] Causations of unintentional injuries are defined in ICD-10 codes: V01-V85, X00-X19, W00-W19, V90/V92/W65-W74, X40-X49, W75-W84, and W53-W59/X20-X27/X29, including motor vehicle crash injuries, fires and burns, falls, drowning, poisoning, suffocation, and animal bites.[8]
Secondly, economic cost refers to direct costs (e.g. cost of hospital treatment, rehabilitation/LOS and medical insurance) and indirect cost (e.g. productivity loss), and also other economic burdens of injuries, such as DALY and non-medical expenditures.
Thirdly, this report used the definition of a child as “every human being below the age of 18 years”, thus specifying the age range from 0 to 18 years.[9]
With the inclusion criteria, the title selection excluded 10 articles, especially articles on non-unintentional injuries. Abstract filtering identified 17 papers, which did not match the inclusion criteria. Finally, 9 articles were selected which matched all the requirements, including economic cost, or other economic burden of unintentional injuries for children or teenagers.
RESULTS
In total, 9 studies were included. There are 3 studies focusing upon costs of childhood unintentional injuries (UI) in low and middle income countries and 6 articles from high income countries as per income group definition of the World Bank.[10]
Jiang and his colleagues’ study (2010) indicated different types and external causes of UI varied according to gender, to different age groups among children aged 0-14 years old, and to different living areas in Northwest China.[11] The total hospitalization cost from January 1, 2002 to December 31, 2003 was US $1,033,876.0, and the mean cost was US $166.3 per case. The total length of stay (LOS) in hospital was 106,915.2 days, and the mean of LOS was 17.2 days per case. Three main cost categories were fractures (US $306,572.0) as the highest, followed by internal organ and encephalic injuries (US $279,725.6). But the average largest mean of hospitalization cost was due to internal organ and encephalic injuries (US $248.5 per case.) The mean LOS relating to blood vessel and nerve injuries was the highest, at 30.1 days per case.
A study in rural Bangladesh focusing on Out-of-pocket payments for unintentional injuries demonstrated that, most rural Bangladeshi people paid from their own pocket for the treatment of unintentional injuries, rather than depending on the available governmental or public health care facilities.[12] Children age 0 to 19 years were the highest risk group, comprising 57% of the total number of the UIs, specifically in teenagers between 15 and 19 years old (31%). For children (0 to 19 years old), cut related injuries were the main cause. 88% of the UI victims did not receive any treatment and 94% patients paid for medicine from their own pockets. The mean of out of pocket expenditure was US $4 (whether or not this was per case was not mentioned) while half of the Bangladeshis are living on less than US $1 per day. Cutting and falling comprised the main proportion of the out of pocket costs for treatments, 45% and 26% respectively.
The study of Economic burden of unintentional injuries in Vietnam was based on community-based surveys, especially in rural areas.[13] The total cost of unintentional injury was US $23,842 per year, and the mean of cost was US $13.7 per case. Direct costs paid by victims accounted for 76.14% of the costs for health care. Health insurance and government payments accounted for only 4% and 16% of costs for health care, separately. Home and traffic injuries were two main types of injuries in Bavi, accounting for 45% and 38% of total cost, respectively. School injuries, which mostly occur in the 0 to 18 age group revealed gender differences, with the figure for males’ cases being 80%. The highest cost unit was associated with very serious injuries, especially traffic injuries (US $103.5 per case). Additionally, very serious injuries, which represented 2.5% of all injuries, cost 17% of the total costs. Patients with the most serious injuries have to work for 7.3 months in order to cover the costs.
A study of Home unintentional injury was took place in Norway.[14] Based upon 8,580 individuals (22.0 per 1,000 populations annually) with unintentional home injuries requiring medical treatment. The age group 5 months to 6 years had the highest per-population incidence of unintentional home injuries. This group accounted for 22% of all injuries, since they spent more h awake at home. Falls were the main cause for children aged 6 years and younger (57%). The total annual cost for children aged less than 14 years was US $165.211, with US $1856.30 per case. People aged 14 years and younger accounted for 31% of all injury cases, representing 6% of the total cost.
Most of the unintentional injuries cost studies analysis came from the USA. There are 5 articles in this review are from the USA, and they focus upon different themes: submersion injury, insurance of UI, unintentional traumatic brain injury, firearm related UI and medical costs of UI.
The paper Unintentional pediatric submersion-injury-related hospitalizations showed 1,475 cases were related to unintentional submersion injury in patients less than 20 years in the USA in 2003.[15] The age group 1 to 4 years has the highest level of pediatric patients hospitalized for submersion (53%). Children under 10 years comprised 78% of the actual samples. Cases for boys were 1.8 times higher than the cases for girls. However, there was no difference in outcomes by gender. Private insurance and Medicaid represented 49% and 39% of the expected primary payers. Self-pay represented only 8% of the total. There was no difference between income groups of the number of actual samples. Swimming pool injuries and other unintentional submersions had the highest rate of the activities related to submersion events (65%). 91% of patients were hospitalized for 7 days, with the highest in patient stay being for 0-1 days. The permanent morbidity increased when the length of stay (LOS) increased. The total hospital costs for patients younger than 20 years in 2003 was US $9,550,704, with the mean costs US $8,651 per case. The mean cost of permanent morbidity was the highest at US $52,429 per case.
The study of Insurance coverage, medical care use, and short-term health changes stated that more uninsured persons had fair or poor health status and had a federal poverty level of family income below 100%.[16] The figures were also higher for racial and ethnic minorities and for the less educated. Almost one fifth (18%) of the unintentional injury sample comprised uninsured individuals. There were fewer clinician visits and recommended follow-up care procedures with uninsured individuals. Decreasing health status was reported in the majority of uninsured individuals at approximately 3.5 months after the incident in the unintentional injuries uninsured group (10%). Unintentional injuries-related uninsured individuals were more likely to report not being fully recovered and to be no longer having treatment. Individuals with insurance were more likely to visit a clinician, representing 9% of the UI group.
Unintentional traumatic brain injuries represented 814 head trauma patients among 1,097 patients aged less than 3 years in the annual 1993-2000 Colorado State mandated hospital discharge database.[17] There were significant differences between unintentional and inflicted injuries, for incidence, length of stay (LOS) and insurance types. Unintentional injuries peaked at the severity level 1 and accounted for 67% of all unintentional injuries cases, thereafter decreasing quickly from the severity level 1 to 4. On the other hand, inflicted injuries peaked at severity level 2. Severity level 4 had the highest average total changes and length of stay per case in the unintentional group and accounted for over US $ 70,000 and 24 days, compared with the inflicted injuries group; US $55,000 and 19 days.
A population-based study of Firearm injury was conducted in Connecticut, USA for mortality and morbidity caused by firearms amongst Connecticut children and youths.[18] There represented 6% of unintentional cases in 219 firearm deaths of Connecticut residents aged 0-19 years. There were 39% of unintentional cases out of 533 hospitalizations for gunshot wounds. For unintentional injuries caused by firearms, the majority of cases occurred amongst males, who represented 100% of deaths, and 94% of hospitalizations. Youths aged 15-19 years were the highest risk group, accounting for approximately 75% of both deaths and hospitalizations. In unintentional shootings, handguns were most common in urban areas while long guns were more often in non-urban areas. Unintentional gun injury constituted 47% of the total cost (US $4,321,653 between 1986 and 1990), accounted for US $2,015,187, and 47.18% of the total LOS (3,491 days in 5 years). The mean of total cost and LOS per case in unintentional cases was US $9,643 and 7.88 days.
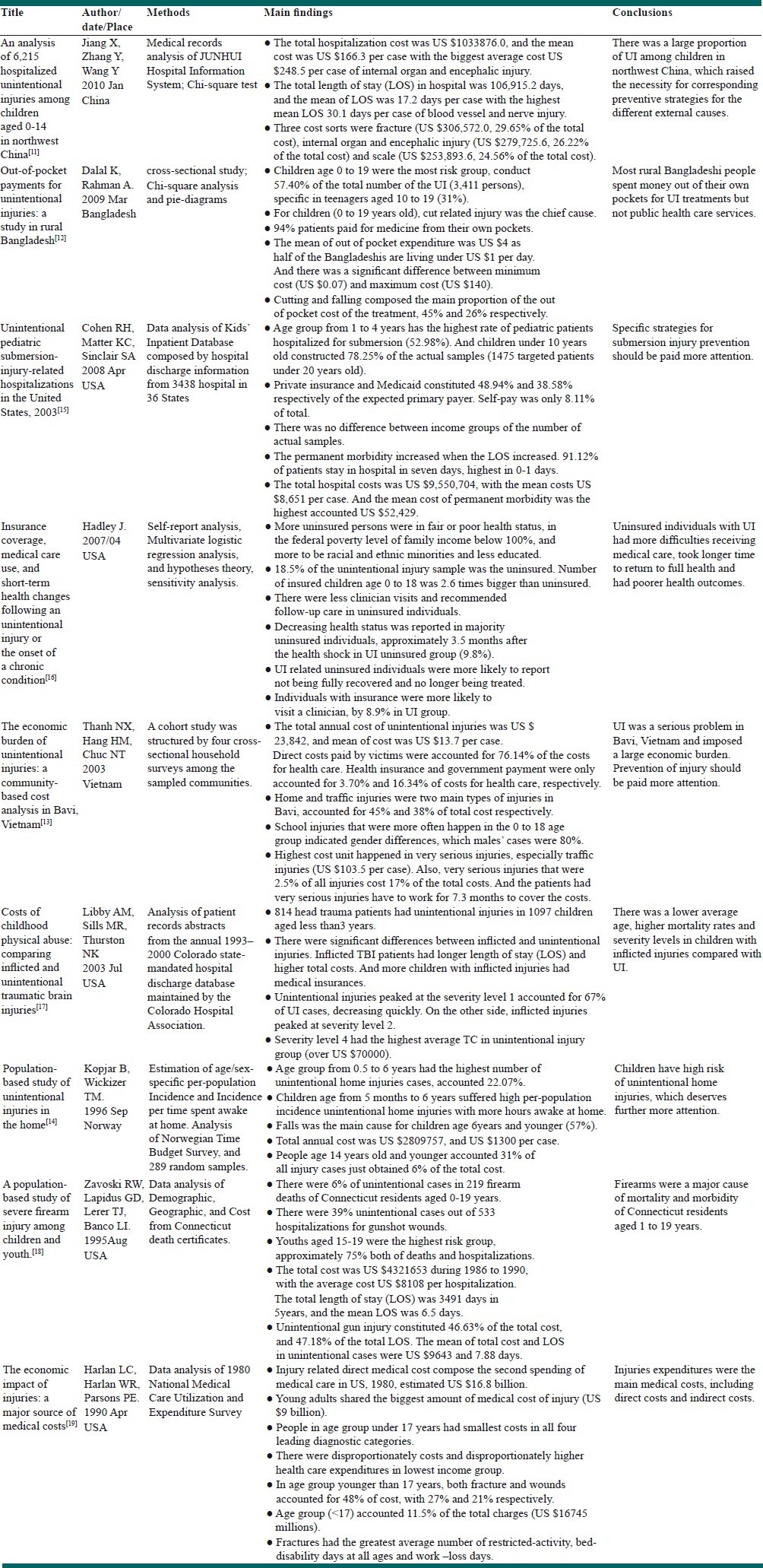
The economic impact of injuries study confirmed that young adults (17 to 44 years old) shared the biggest amount (US $9 billion) of medical cost of injury.[19] People in the age group under 17 years had the smallest costs in all four leading diagnostic categories, which were termed: injury or poisoning, no or unknown diagnosis, respiratory and nervous system/sense organ. There were disproportionately higher costs and higher health care expenditures in the lowest income group. There was an increasing trend of the age groups from under 17 years (27%) to over 65 years (43%) in the costs of fractures. Females’ fracture costs were greater than those of males′. In the age group younger than 17 years, both fracture and wounds accounted for 48% of the costs, with 27% and 21%, respectively. Age group (<17) accounted 12% (US $16,745 million), of the total charges (US $1,926 million). Fractures had the greatest average number of restricted-activity, bed-disability days for all ages and work –loss days [Table 1].
Table 1.
Economic costs of unintentional injuries among children
DISCUSSION
In general, the burden of unintentional injuries among children is considerable all over the world, inflicting great economic losses on society, ranging from US $516,938 to US $9,550,704 per year (Jiang X et al.,[11]; Cohen et al.,[15] ), US $4 to US $1,856 per case[12,14] and 7.88 to 17.2 days of LOS per case.[11,18] In all the reviewed articles, children as a risk group shared a higher rate of different kinds of unintentional injuries, especially those aged under 4 years. The direct and indirect economic costs of childhood unintentional injuries were mainly calculated by referring to medical treatment, length of stay (LOS) and loss of healthy years. These factors represent a huge economic expenditure of the studied countries, particularly low-and-high income countries. Additionally, there are large differences in childhood unintentional injuries between the genders, different age groups of children, low-and-middle income countries and high income countries.
The reviewed articles indicated that boys have more unintentional injuries than girls do and consequently the costs in relation to boys are also higher. The world report of child injuries from the WHO also shows the same trend: boys seem to have more frequent and more severe injuries than girls. It is possible to speculate why boys have a higher risk than girls. Boys may be more active and adventurous in the environment; and boys engage in more risky behaviors than girls.[20] The Chinese study showed that boys had higher rates of fractures, and girls had higher rate of scald/burns. The preponderance of boys in injuries has been widely reported to be an international phenomenon[21] with boys representing more cases and higher severity levels of injuries, which are associated with greater medical expenditure, longer LOS and more loss of healthy days.
Age groups differences were significant in relation to type of injury and causes. Children under 4 year s old constituted half of the incidences of submersion-injury-related hospitalizations in the USA.[15] However, other research found that teenagers aged 15–19 years have higher rates of submersion-related mortality.[22] Zavoski et al., found that USA teenagers aged 15 to 19 years old had the highest risk of unintentional firearm related injuries.[18] The differences in the statistics may be caused by the varied activities, increasing experiences and knowledge within age groups. Economic burden, LOS and loss of healthy years would be heavier for the younger groups among children with the similar injury severe level.
There are significant differences of UI burden between low- and middle-income countries and high-income countries.
Poverty as one of the important contributors to childhood unintentional injuries has a significant role in low-and-middle income countries. The burden of injury is much greater in low-and-middle income countries: over 95% of injury deaths among children occurred in these countries.[3] Besides, costs of unintentional injuries are not well covered by health care and insurance systems, which means most of the people living in low-and-middle income countries paid for treatment with their own money, as being indicated in the study of Bangladesh, which refers to the ‘injury poverty trap’.[13] Unlike high income countries, there is lack of data and research in low-and-middle income countries into the scale and cost of injuries.
The main problem is an absence of or undeveloped national health care and insurance systems in low-and-middle income countries. For instance, the study in China and Vietnam indicated that the absence of a national monitoring network, an imperfect or poorly-functioning health care system, low coverage of insurance, no comprehensive injury register system, few injury cost effectiveness research programs, and poor allocation of resources were common in low and middle income countries. In contrast, high income countries with developed social systems (e.g. complete medical records systems, public and/or private insurance) would have larger direct medical costs and lengths of hospital stays, since people are more liable to seek medical care and treatments.
Researchers suggested that adverse effects on medical care use and health caused be uninsured statements.[23] Almost, 70% of the participants of an American insurance study of unintentional injuries or chronic disease showed individuals with insurance were more likely to report being fully recovered and were more likely to visit a clinician. An uninsured person who experienced an unintentional injury had greater difficulty receiving recommended medical care and had a longer recovery time to full health. These studies indicated that uninsured individuals gain significantly less health care than those with insurance and also have poorer health outcomes, which would increase the indirectly economic cost resulting from, for example, loss of manufacturing due to days off work related to injuries.[16]
In low and middle income countries, there is a lack of educational opportunities for both children and parents, poor neighborhood setting and poverty, which may be major risk factors leading to the childhood unintentional injuries. To take drowning as an example: There are significant differences in drowning mortality numbers between different income countries.[3] Some researchers also found that rural children have much higher drowning rates than those in urban areas and child drowning risk increased as maternal age and family size increased.[24,25] Explanations of these phenomena include a low level of swimming ability, lack of opportunities to learn to swim and to acquire experience swimming, and a lack of supervision in swimming environments.[26]
As mentioned above, location differences (rural area and urban area) appear in these reviewed articles, which may result in different society setting, facilities and resources in different areas based on their particular development levels. Differences in family financial conditions, housing, parents’ educational levels and parents’ relationship in varied locations are also social and economic factors which may contribute to children's unintentional injuries.[27] What is more, some researchers indicate that the occurrence of children's unintentional injuries in rural areas have associations with child abuse and ignorance of UI,[28] thus producing a malignant interaction of family factors and risk for injury in the poor families. Because of crowded surroundings, higher urbanization and more hectic life styles, urban areas are associated with a higher risk of road traffic injuries, which then lead to larger social and medical costs.[3]
A substantial literature suggests that developing countries have disadvantages in relation to undertaking quality research. There has been limited research into the availability, price and affordability of child-safety, family-safety devices, cost-effectiveness of poisoning, cost-effectiveness of injury prevention measures, and injury epidemiology and the efficacy of interventions, especially in the case of low-income and middle-income countries.[3,29] Therefore, the current review has also revealed the paucity of studies in this important filed for preventing childhood injuries. The warrants further studies, especially from the low and middle income countries.
There are some limitations in this review. Firstly, most of the selected articles used ICD-9 codes to define different types of unintentional injuries which we defined by ICD-10 codes. Secondly, the limitation of age ranges varied in these articles. For instance, the Bangladesh study used 10-19 years as one of the age ranges, while the Norway study used 15-24 years as the age range. In undertaking this review, both of the age ranges were used for the analysis of children's unintentional injuries. Thirdly, depending on the health system of different targeted countries, the different study designs and the different study purposes, the measurement of cost (including direct and indirect cost) and length of stay (LOS) varied between the selected articles. For example, the unintentional pediatric submersion injury study targeted specifically unintentional injuries, while all types of unintentional injuries were mentioned in the Chinese study. Fourthly, there are limited explanations of research questions in the reviewed articles, such as in the study of the situation in Vietnam, patients who were not identified as patients themselves, their parents or families have to work for 7.3 months to cover the medical expenditure. Fifthly, this study searched only one database, PUBMED. Therefore, there were possible limitations to the amount of research information we examined.
Unintentional injuries among young people are one of the top public health issues and they are associated with a large amount of premature morbidity and mortality. The economic cost of UI is enormous and it imposes a large economic burden on societies, ranging from US $0.5 million to US $9.5 million per year. In addition, there is large difference between different income countries in relation to factors such as higher burden of injury (injury incidence, self-payment, loss of healthy days), and a lack of injury health care services and insurance systems in low-and-middle income countries. In conclusion, more studies of the economic burdens of child unintentional injuries should be carried out in low and middle income countries. Additionally, unintentional injuries intervention and prevention strategies should be speedily developed. For example, road safety improvements, the use of bicycle helmets, child restraints, and smoke alarms could all make significant differences to the numbers of accidental injuries.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Sleet DA, Ballesteros MF, Borse NN. A review of unintentional injuries in adolescents. Annu Rev Public Health. 2010;31:195–212. doi: 10.1146/annurev.publhealth.012809.103616. [DOI] [PubMed] [Google Scholar]
- 2.Manual for estimating the economic costs of injuries due to interpersonal and self-directed violence. Geneva: WHO; 2008. WHO. [DOI] [PubMed] [Google Scholar]
- 3.Peden M, Oyegbite K, Ozanne-Smith J, Hyder AA, Branche C, Rahman AK, et al. World report on child injury prevention. Geneva: WHO; 2008. [PubMed] [Google Scholar]
- 4.Braddock M, Lapidus G, Gregorio D, Kapp M, Banco L. Population, income and ecological correlates of child pedestrian injury. Pediatrics. 1991;88:1242–7. [PubMed] [Google Scholar]
- 5.SEARO. Disability, Injury Prevention and Rehabilitation. 2009. [Last accessed on 2010 Sept 10]. Available from: http://www.searo.who.int/en/Section1174/section1461.htm .
- 6.Doll LS, Bonzo S, Sleet D, Mercy J, Haas EN. Handbook of Injury and Violence Prevention. Atlanta, GA: Springer; 2007. [Google Scholar]
- 7.CDC Childhood Injury Report: Patterns of Unintentional Injuries Among 0–19 Year Olds in the United States, 2000–2006. Atlanta, GA: Division of Unintentional Injury Prevention, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention, US Department of Health and Human Services; 2008. [Google Scholar]
- 8.WHO International Statistical Classification of Diseases and Related Health Problems 10th Revision Version for 2007. [Last accessed on 2010 Sept 18]. Available from: http://www.apps.who.int/classifications/apps/icd/icd10online/
- 9.Convention on the rights of the child. New York, NY, United Nations. 1989. [Last accessed on 2010 Oct 21]. Available from: http://www.unhchr.ch/html/menu3/b/k2crc.htm .
- 10.World Bank. Income Category, World Bank estimates of 2008 Gross National Income (GNI) per capita. 2008. [Last accessed on 2011 Jul 20]. Available from: http://www.web.worldbank.org/WBSITE/EXTERNAL/WBI/WBIPROGRAMS/KFDLP/EXTUNIKAM/0,,contentMDK:20584355~menuPK:1433295~pagePK:64168445~piPK:64168309~theSitePK:1414721,00.html .
- 11.Jiang X, Zhang Y, Wang Y, Wang B, Xu Y, Shang L. An analysis of 6215 hospitalized unintentional injuries among children aged 0-14 in northwest China. Accid Anal Prev. 2010;42:320–6. doi: 10.1016/j.aap.2009.08.012. [DOI] [PubMed] [Google Scholar]
- 12.Dalal K, Rahman A. Out-of-pocket payments for unintentional injuries: A study in rural Bangladesh. Int J Injury Contr Saf Promot. 2009;16:41–7. doi: 10.1080/17457300802475992. [DOI] [PubMed] [Google Scholar]
- 13.Thanh NX, Hang HM, Chuc NT, Lindholm L. The economic burden of unintentional injuries: A community-based cost analysis in Bavi, Vietnam. Scand J Public Health Suppl. 2003;62:45–51. doi: 10.1080/14034950310015103. [DOI] [PubMed] [Google Scholar]
- 14.Kopjar B, Wickizer TM. Population-based study of unintentional injuries in the home. Am J Epidemiol. 1996;144:456–62. doi: 10.1093/oxfordjournals.aje.a008951. [DOI] [PubMed] [Google Scholar]
- 15.Cohen RH, Matter KC, Sinclair SA, Smith GA, Xiang H. Unintentional pediatric submersion-injury-related hospitalizations in the United States, 2003. Inj Prev. 2008;14:131–5. doi: 10.1136/ip.2007.016998. [DOI] [PubMed] [Google Scholar]
- 16.Hadley J. Insurance coverage, medical care use, and short-term health changes following an unintentional injury or the onset of a chronic condition. JAMA. 2007;297:1073–84. doi: 10.1001/jama.297.10.1073. [DOI] [PubMed] [Google Scholar]
- 17.Libby AM, Sills MR, Thurston NK, Orton HD. Costs of childhood physical abuse: Comparing inflicted and unintentional traumatic brain injuries. Pediatrics. 2003;112:58–65. doi: 10.1542/peds.112.1.58. [DOI] [PubMed] [Google Scholar]
- 18.Zavoski RW, Lapidus GD, Lerer TJ, Banco LI. A population-based study of severe firearm injury among children and youth. Pediatrics. 1995;96:278–82. [PubMed] [Google Scholar]
- 19.Harlan LC, Harlan WR, Parsons PE. The economic impact of injuries: A major source of medical costs. Am J Public Health. 1990;80:453–9. doi: 10.2105/ajph.80.4.453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Turner C, McClure R. Age and gender differences in risk-taking behavior as an explanation for high incidence of motor vehicle crashes as a driver in young males. Inj Control Saf Promot. 2003;10:123–30. doi: 10.1076/icsp.10.3.123.14560. [DOI] [PubMed] [Google Scholar]
- 21.Chan CC, Cheng JC, Wong TW, Chow CB, Luis BP, Cheung WL. An international comparison of childhood injuries in Hong Kong. Injury Prev. 2000;6:20–3. doi: 10.1136/ip.6.1.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Quan L, Cummings P. Characteristics of drowning by different age groups. Inj Prev. 2003;9:163–8. doi: 10.1136/ip.9.2.163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hadley J. Sicker and poorer: The consequences of being uninsured: A review of the research on the relationship between health insurance, medical care use, health, work, and income. Med Care Res Rev. 2003;60(2 suppl):3S–112S. doi: 10.1177/1077558703254101. [DOI] [PubMed] [Google Scholar]
- 24.Rahman A, Giashuddin SM, Svanström L, Rahman F. Drowning – a major but neglected child health problem in rural Bangladesh: implications for low income countries. Int J Inj Contr Saf Promot. 2006;13:101–5. doi: 10.1080/17457300500172941. [DOI] [PubMed] [Google Scholar]
- 25.Ahmed MK, Rahman M, van Ginneken J. Epidemiology of child deaths due to drowning in Matlab, Bangladesh. Int J Epidemiol. 1999;28:306–11. doi: 10.1093/ije/28.2.306. [DOI] [PubMed] [Google Scholar]
- 26.Saluja G, Brenner RA, Trumble AC, Smith GS, Schroeder T, Cox C. Swimming pool drownings among US residents aged 5-24 years: Understanding racial/ethnic disparities. Am J Public Health. 2006;96:728–33. doi: 10.2105/AJPH.2004.057067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Braddock M, Lapidus G, Gregorio D, Kapp M, Banco L. Population, income, and ecological correlates of child pedestrian injury. Pediatrics. 1991;88:1242–7. [PubMed] [Google Scholar]
- 28.Rivara FP. Prevention of injuries to children and adolescents. Injury Prev. 2002;8:5–8. doi: 10.1136/ip.8.suppl_4.iv5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Waters H, Hyder AA, Phillips TL. Economic evaluation of interventions to reduce road traffic injuries: A review of literature with applications to low and middle income countries. Asia Pac J Public Health. 2004;16:23–31. doi: 10.1177/101053950401600105. [DOI] [PubMed] [Google Scholar]