

Abstract
Background
Shoulder injuries in rugby players are common, but the mechanisms of injury are less well understood. This study aims to elucidate common mechanisms of injury and identify the patterns of injury they produce.
Materials and methods
Twenty-four elite rugby players, referred to the senior author for diagnosis and management of shoulder injuries, were selected. Videos of the injuries were independently reviewed by rugby-medical experts to describe the mechanisms of injury. The mechanisms reported were collated and analysed to determine the level of agreement between reviewers and conclude an overall description of injury mechanisms.
Results
The authors identified three mechanisms of shoulder injury from the video analysis. These are the ‘Try-Scorer’, characterised by hyperflexion of the outstretched arm such as when scoring a try; the ‘Tackler’, extension of the abducted arm behind the player while tackling; and the ‘Direct Impact’, a direct blow to the arm or shoulder when held by the side in neutral or slight adduction. The Try Scorer and Tackler mechanisms both involve a levering force on the glenohumeral joint (GHJ). These mechanisms predominantly cause GHJ dislocation, with Bankart, reverse Bankart and superior labrum anterior–posterior tears. The Try-Scorer Mechanism also caused the majority (83%) of rotator cuff tears. The Direct Hit mechanism resulted in GHJ dislocation and labral injury in 37.5% of players and was most likely to cause acromioclavicular joint dislocation and scapula fractures, injuries that were not seen with the other mechanisms.
Conclusion
Greater understanding of the mechanisms involved in rugby shoulder injury is useful in understanding the pathological injuries, guiding treatment and rehabilitation and aiding the development of injury-prevention methods.
Background
Rugby football is a physical game characterised by multiple high-energy contacts during the course of a match. Foul play accounts for only 6% of injuries,1 demonstrating that most injuries occur in normal play.2 The shoulder is a frequently injured joint in amateur and professional rugby union3–5 and rugby league,6 with the tackle accounting for 49–72% of injuries.1 2 5 7 8 Shoulder dislocations are common and severe injuries in rugby players leads to considerable time away from training and matches. They account for 14% of all shoulder injuries, with 62% of dislocations occurring during tackling.5
Headey et al5 reported on shoulder injuries occurring in 17 000 player hours of match play and 200 000 player hours of training. First-team players from 12 of 13 English professional Rugby Football Union clubs involved in the 2002–2003 and 2003–2004 seasons were surveyed. Injuries reported were shoulder haematoma (12%), dislocation or instability (14%), acromioclavicular joint injury (32%), rotator cuff injury or impingement (23%) and fracture (1%). Acromioclavicular joint injuries were therefore the most common, with shoulder dislocations and instability accounting for the most severe injuries and greatest period of absence from scheduled training and matches. Contact was responsible for 97% of injuries, with tackling or being tackled accounting for 65%. One study of professional rugby players undergoing shoulder arthroscopy in a 3-year period found superior labrum anterior–posterior (SLAP) lesions in 35%, of which 17% were associated with an anterior labral Bankart-type injury, 11% with posterior labral injury and 11% with both anterior and posterior labral involvement.9 Prevalence of isolated posterior labral injury in professional and semiprofessional players in a 4-year period is 7.7%.10 Rotator cuff tears were found in 9% of professional or semiprofessional rugby players undergoing shoulder surgery with minimum 12-month follow-up in a 2-year period.11
Though the shoulder injuries sustained in rugby have been described previously, the specific mechanisms that cause the injuries are less well understood. Understanding the exact mechanistic cause would aid the understanding of the injuries and assist with injury prevention. The aims of this study are to elucidate and describe patterns of shoulder injury mechanism in elite rugby players and to correlate injury-producing mechanisms with specific patterns of injury.
Materials and methods
All participants were professional rugby league or rugby union players aged 19–35, referred to the senior author for definitive diagnosis and treatment, having sustained their injury during match play. The study, therefore, only included serious shoulder injuries requiring specialist opinion and management. Injuries were diagnosed using clinical history and examination, imaging and during operative procedures. Permission was sought for use of the videos and medical records in the study, with all players consenting to the use of their data. None of the authors were involved in the video analysis. Videos were obtained either from the players themselves or from prerecorded television footage.
Videos of each player's injury were independently reviewed by a range of experts, including an orthopaedic surgeon, a sports medicine physician, three rugby club physiotherapists, a physiotherapist specialising in shoulder injuries and a rugby player with a degree in sports science. Each video had one camera angle of the injury. Two club physiotherapists reviewed the videos together, as did the other club physiotherapist and the player. All other reviewers viewed the videos independently and all were blinded to the others' results. An injury proforma was completed for each injury as shown in table 1. This was explained to the reviewers before commencing video analysis, to clarify any points of confusion. The different movements and directions of force were demonstrated to ensure consistency between reviewers. Reviewers were shown each clip at full speed, then allowed to view in slow motion or frame-by-frame as necessary. Reviewers were blinded to details of each player's injury.
Table 1.
The injury proforma criteria for describing mechanism of injury
| Was the injured player? | Tackler | Tackled | In open play | ||||
|---|---|---|---|---|---|---|---|
| Which shoulder was injured? | Left | Right | |||||
| What type of play? | Open play | Tackle | Ruck/maul | Scrum | Line-out | Foul Play | |
| Direction travelling? | To opposition try-line | To own try-line | Across field | ||||
| Body position? | Upright | Prone | Supine | On side | |||
| Where was the arm at initiation of injury? | Flexion | Extension | Neutral | ||||
| Abduction | Adduction | Neutral | |||||
| External rotation | Internal rotation | Neutral | |||||
| How was the arm moved during injury? | Flexed | Extended | Neither | ||||
| Abducted | Adducted | Neither | |||||
| Externally rotated | Internally rotated | Neither | |||||
| Which direction was the force? | Superior | Inferior | Neither | ||||
| Anterior | Posterior | Neither | |||||
| Medial/compressive | Lateral/wrenching | Neither | |||||
The mechanisms reported by each reviewer were collated and analysed by the authors to determine the level of agreement between reviewers and conclude an overall description of injury mechanism. Where there was overwhelming support for one selection, for example, the arm being in flexion at initiation of injury, this was taken as the definitive selection for description of injury mechanism. Where there was disagreement over the position or movement of the arm, the selection with five or more reviewers' support was used. Where there was disagreement over the direction of force, the most common selection for each option (for example, superior versus inferior) was chosen. Note was made also of qualitative descriptions of mechanism by reviewers during the process to guide the identification and description of mechanisms. Having summarised the results of the proformas for each injury, mechanisms with at least three features in common were identified, including position of the arm at initiation of injury, movement of arm during injury and direction of force. This was aided by subjective descriptions of the injury mechanism by reviewers during video analysis.
Results
A total of 24 elite rugby players with 24 injury events were identified. The characteristics of the participants are shown in table 2.
Table 2.
Player characteristics (n=24)
| Mean | Range | |
|---|---|---|
| Age (years) | 27.6 | 19–35 |
| Height (m) | 1.86 | 1.75–1.98 |
| Weight (kg) | 98.7 | 80–121 |
| Body mass index | 28.6 | 24.7–32.5 |
The left shoulder was injured in 9 (37%) of the injury events and the right shoulder in 15 (63%). The injury occurred during a tackle in 17 (71%), ruck or maul in 3 (12.5%), open play in 3 (12.5%) and scrum in 1 (4%). Players were travelling towards the opposition try line in 20 (83%), towards their own line in 2 (8%), both towards opposition try line and across the field in 1 (4%) and stationary in 1 (4%). Of the players injured in a tackle, 13 (76%) were tackled and 4 (24%) were tacklers.
Injuries incurred included acute, primary glenohumeral dislocation, Bankart and reverse Bankart tears, SLAP tears, full-thickness rotator cuff tears, Hill-Sachs-type fractures of the humeral head, scapula fractures, acromioclavicular joint (ACJ) dislocations, injury to nerves of the shoulder and a humeral avulsion of the glenohumeral ligament (HAGL). The numbers of individual injuries identified following injury event for all players are displayed in figure 1.
Figure 1.
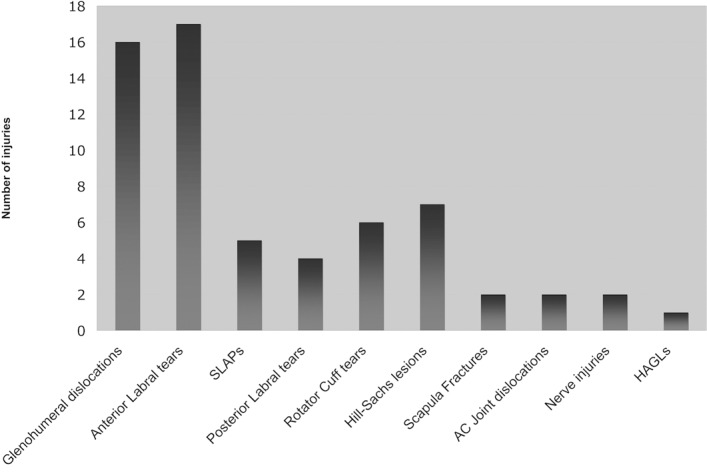
Numbers of individual injuries for all players. GHJ, glenohumeral Joint; SLAP, superior labrum anterior – posterior; ACJ, acromioclavicular joint; HAGL, humeral avulsion of glenohumeral ligament.
Three mechanisms of injury were identified. The first is termed Try Scorer, as the mechanism occurred commonly while diving and reaching the ball-carrying hand forward to score a try. A total of 10 players were injured by this mechanism. The characteristics of these players when the injury was sustained are shown in tables 3 and 4. The mechanism involves the injured arm in flexion, specifically flexion above 90°. A posterior force drives the arm backwards and exerts leverage on the glenohumeral joint with the arm either remaining in fixed flexion by contact with the ground, or forced into further flexion. This may be compounded by opposing players falling on top of the injured player, providing additional loading that forces the arm into greater flexion. Figure 2 demonstrates this mechanism.
Table 3.
Characteristics of players injured by the Try-Scorer Mechanism (n=10)
| 1. Tackler/ed/open play | 2. Side of injury | 3. Type of play | 4. Direction travelling | 5. Position of body |
|---|---|---|---|---|
| Tackled: 6 | Right: 7 | Tackle: 6 | Opposition try-line: 7 | Prone: 7 |
| Open play: 3 | Left: 3 | Ruck/maul: 1 | Own try-line: 2 | Upright: 2 |
| NA: 1 | Open: 2 | Not moving: 1 | On side: 1 | |
| Scrum: 1 |
Table 4.
Characteristics of players injured by the Try-Scorer Mechanism (n=10)
| At initiation of injury | Further movement | ||||
|---|---|---|---|---|---|
| Flexion/extension | Rotation | Ab/adduction | Flexed/extended | Rotated | Ab/adducted |
| Flexion: 10 | Neutral: 8 | Abducted: 5 | Flexed: 6 | Externally: 2 | Abducted: 2 |
| External: 2 | Neutral: 5 | No further: 4 | Internal: 1 | Adducted: 1 | |
| No further: 7 | No further: 7 | ||||
Figure 2.

The Try Scorer mechanism. The flexed arm of a player diving forward is driven over the head by contact with the ground, exerting leverage on the glenohumeral joint.
The second mechanism is termed Tackler, seen in four players. This occurs most commonly when the player made a tackle on an opponent travelling towards them. Characteristics of these players are shown in tables 5 and 6. The arm is held abducted to 90°. A posteriorly directed force, resulting from contact with the ball-carrying player for example, extends the abducted arm behind the player in the plane of abduction, again exerting a levering force on the glenohumeral joint. This is shown in figure 3.
Table 5.
Characteristics of players injured by the Tackler mechanism (n=4)
| 1. Tackler/ed/open play | 2. Side of injury | 3. Type of play | 4. Direction travelling | 5. Position of body |
|---|---|---|---|---|
| Tackled: 1 | Right: 4 | Tackle:4 | Opposition try-line: 4 | Prone: 1 |
| Tackler: 3 | On side: 1 | |||
| Upright: 2 |
Table 6.
Characteristics of players injured by the Tackler mechanism (n=4)
| At initiation of injury | Further movement | ||||
|---|---|---|---|---|---|
| Flexion/extension | Rotation | Ab/adduction | Flexed/extended | Rotated | Ab/adducted |
| Flexion: 3 | Neutral: 2 | Abducted: 4 | Flexed: 1 | Externally: 1 | Abducted: 2 |
| Neutral: 1 | External: 2 | Extended: 2 | No further: 3 | Adducted: 1 | |
| No further: 1 | No further: 1 | ||||
Figure 3.

The Tackler mechanism. The abducted arm of the tackling player is forcibly extended behind the player, exerting leverage on the glenohumeral joint.
The third mechanism is termed Direct Impact and was seen in eight players. This was seen in ball-carrying players sustaining direct impact from a tackling opponent directly on the shoulder and in tackled players falling onto the shoulder. The arm is held flexed below 90° (six players) or in neutral, with internal rotation, such as when carrying a ball by the side. A medially directed compressive force caused by direct impact to the shoulder results in injury, as shown in figure 4. Features of these players are shown in tables 7 and 8.
Figure 4.

The Direct Hit mechanism. Medially directed compressive force to the adducted arm by contact with another player or the ground results in injury.
Table 7.
Characteristics of players injured by the Direct-Hit mechanism (n=8)
| 1. Tackler/ed/open play | 2. Side of injury | 3. Type of play | 4. Direction travelling | 5. Position of body |
|---|---|---|---|---|
| Tackled: 7 | Right: 3 | Tackle: 6 | Opposition try-line: 7 | Upright: 4 |
| Tackler: 1 | Left: 5 | Ruck/maul: 1 | Across: 1 | On side: 3 |
| Open: 1 | NA: 1 |
Table 8.
Characteristics of players injured by the Direct-Hit mechanism (n=8)
| At initiation of injury | Further movement | ||||
|---|---|---|---|---|---|
| Flexion/extension | Rotation | Ab/adduction | Flexed/extended | Rotated | Ab/adducted |
| Flexion: 5 | Internal: 5 | Adducted: 2 | Flexed: 1 | No further: 8 | Adducted: 6 |
| Neutral: 3 | Neutral: 3 | Neutral: 6 | No further: 7 | No further: 2 | |
Two players were injured by mechanisms that could not be characterised into one of the three groups described above. Features of these mechanisms are shown in tables 9 and 10.
Table 9.
Characteristics of players injured by the other mechanisms (n=2)
| 1. Tackler/ed/open play | 2. Side of injury | 3. Type of play | 4. Direction travelling | 5. Position of body | |
|---|---|---|---|---|---|
| Open: 1 | Left: 1 | Ruck/maul: 1 | Opposition try-line: 2 | Upright: 2 | |
| Tackler: 1 | Right: 1 | Tackle: 1 |
Table 10.
Characteristics of players injured by the other mechanisms (n=2)
| At initiation of injury | Further movement | ||||
|---|---|---|---|---|---|
| Flexion/extension | Rotation | Ab/adduction | Flexed/extended | Rotated | Ab/adducted |
| Flexion: 2 | Neutral: 2 | Neutral: 2 | Extended: 2 | No further: 2 | Abducted: 1 |
| No further: 1 | |||||
The numbers of individual injuries seen with each mechanism are shown in table 11. Glenohumeral dislocations, associated labral and humeral head injuries and rotator cuff tears were most common in the Try-Scorer and Tackler groups. Scapula fractures and ACJ dislocations only occurred in the Direct Impact group. Glenohumeral dislocations and labral injuries were also seen, though these occurred less frequently than by the other mechanisms.
Table 11.
Numbers of individual injuries for each mechanism
| Injury | Try scorers (n=10) | Tacklers (n=4) | Direct hits (n=8) | Other (n=2) | Total (n=24) |
|---|---|---|---|---|---|
| GHJ dislocation | 8 (80%) | 3 (75%) | 3 (37.5%) | 2 (100%) | 16 (67%) |
| Bankart | 8 (80%) | 4 (100%) | 3 (37.5%) | 2 (100%) | 17 (71%) |
| Reverse bankart | 2 (20%) | 1 (25%) | 2 (25%) | 0 | 5 (21%) |
| SLAP | 3 (30%) | 2 (50%) | 0 | 0 | 5 (21%) |
| Rotator cuff tear | 5 (50%) | 1 (25%) | 0 | 0 | 6 (25%) |
| Hill-sachs | 4 (40%) | 1 (25%) | 1 (12.5%) | 1 (50%) | 7 (30%) |
| Scapula fracture | 0 | 0 | 2 (25%) | 0 | 2 (8%) |
| ACJ dislocation | 0 | 0 | 2 (25%) | 0 | 2 (8%) |
| Nerve injury | 1 (10%) | 0 | 1 (12.5%) | 0 | 2 (8%) |
| HAGL | 1 (10%) | 0 | 0 | 0 | 1 (4%) |
The number in bold refers to the number of players sustaining each injury. The percentage value is as a proportion of all the players suffering their injury due to the mechanism specified at the top of each column.
ACJ, acromioclavicular joint; GHJ, glenohumeral joint; HAGL, humeral avulsion of the glenohumeral ligament; SLAP, superior labrum anterior–posterior.
Discussion
Few studies have addressed the specific mechanisms of shoulder injury in rugby players. The authors undertook a larger video analysis than previous studies and also used a range of reviewers from the sports-rugby arena to independently analyse the injuries. The authors also investigated serious injuries only which required a specialist referral and led to the longest time off play. Glenohumeral joint dislocations were found to be the most common injury in 67% of players. Dislocations were accompanied by associated injuries such as anterior, posterior or SLAP-type labral tears and Hill-Sachs lesions. ACJ dislocations were seen in only 8% of players in this study. Headey et al reported ACJ injuries as the most common shoulder injury in elite rugby players, followed by rotator cuff injuries and subacromial impingement, then glenohumeral dislocation.5 This study only included injuries referred to a specialist shoulder surgeon, which would account for this difference, as it is likely that many ACJ injuries in rugby often settle and do not require specialist opinion.
SLAP lesions were less common in this study than previously described, at 21% compared to 37%,6 although rotator cuff tears were more common, seen in 25%, compared to the rate of 9.9% previously reported.10 The tackle was responsible for injury in 71% of our cohort, similar to Headey et al's 67%.5 Six rotator cuff tears occurred in our study, five of which were in the Try Scorer group. Rotator cuff tears are traditionally found in older populations, but are now more commonly being reported in younger contact athletes and are associated with high-energy anterior traumatic shoulder dislocations. Bankart tears were predictably seen in all players who sustained an anterior glenohumeral dislocation. One Bankart tear occurred in the apparent absence of dislocation. This may be due to a subclinical subluxation.
Longo et al describe the first study of shoulder dislocation mechanism in elite rugby players. Videos of four professional rugby players sustaining a primary shoulder dislocation during match play were retrospectively analysed to describe the shoulder affected; position of the shoulder and elbow; direction of force and direction in which the injured shoulder was moved during the injury event. Three of the four players sustained anterior shoulder dislocation, with two injuring it during tackling with the arm abducted and externally rotated. The other fell on the flexed, internally rotated arm with another player on top of him, levering the humerus away from the glenoid. The final player fell on the point of the flexed elbow, longitudinally loading the humerus and dislocating the humeral head posteriorly. The authors acknowledged abduction and external rotation as the accepted mechanism of anterior dislocation and suggested that rugby players are also at risk of anterior dislocation by hyperflexion with internal rotation.12 These correspond with the Tackler and Try Scorer mechanisms in this study.
Understanding the mechanisms by which injuries occur in rugby can guide the processes of rehabilitation and prevention. In a physical game such as rugby, where high force collisions are commonplace, some injuries will remain inevitable despite efforts to prevent them. It is difficult to see how to modify the game of rugby to reduce risk of shoulder injury without losing the essence of the game itself. Players should be advised to avoid tackling opposing players with the outstretched abducted arm only, instead concentrating on contacting the opposing player with their shoulder, to minimise the risk of Tackler-type injuries. Similarly, players can be advised to avoid diving for the try line with the ball in the outstretched flexed arm, as this places them at a high risk of dislocation and rotator cuff injury. In the competitive game of rugby, however, this may prove challenging to implement. The Direct Hit-type mechanism is also difficult to avoid. With foul play responsible for only a small proportion of injuries,1 high-impact forces will always be encountered and it follows that preparation of players with dedicated shoulder strength and conditioning must improve to minimise risk of shoulder injury.
A limitation of the study is the quality of video footage acquired for analysis. All videos provided at least one angle that showed the injury mechanism. Due, however, to the dynamic nature of rugby and the number of players involved in any one sequence of play, establishing the exact sequence of events with accuracy required careful, repeated analysis from reviewers and was difficult at times. Only injuries occurring during match play were reviewed, due to the availability of footage for video analysis. It is acknowledged by the authors that training includes match-play scenarios and also off-the-field preparation such as strength and conditioning that have the potential for different mechanisms of injury to those described herein. Differences exist between Rugby Union and Rugby League in terms of the type of plays and roles of the players; however, the mechanisms and injuries described by this study were common to both sports. In addition, only serious injuries requiring specialist investigation and management were included. Other mechanisms that produce more minor injuries may not have been elucidated. It may be, however, that the same mechanisms described herein are also responsible for less severe injuries, occurring at slower speeds or with less force.
Conclusion
Three mechanisms of shoulder injury in rugby players have been identified from this study. These are the Try Scorer, comprising hyperflexion of the outstretched arm leading to glenohumeral dislocation, labral injuries and rotator cuff tears; the Tackler, comprising extension of the abducted arm resulting in dislocation and labral injuries; and the Direct Impact, comprising a compressive force to adducted, internally rotated arm resulting in acromioclavicular injury, scapula fractures and, less commonly, glenohumeral dislocation. Greater understanding of the mechanisms involved in shoulder injury in rugby players is useful both for understanding how injuries occur and also to guide the rehabilitation and injury-prevention processes.
Acknowledgments
The authors acknowledge Rob Conlan, Carl Chapman, Ross Divorty, Dr Stan Baltezak, Jamie Fulton, Simon Edwards, Charlie Talbot, Christine Holmes, Andy Vail for their help with this paper.
Footnotes
Contributors J Crichton, DR Jones and L Funk were all involved in study conception and design, data acquisition and analysis, and drafting and approval of the final article. All three meet BJSM criteria for authorship.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
References
- 1.Bathgate A, Best JP, Craig G, et al. A prospective study of injuries to elite Australian rugby union players. Br J Sports Med 2002;36:265–9; discussion 269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Brooks JH, Fuller CW, Kemp SP, et al. Epidemiology of injuries in English professional rugby union: part 1 match injuries. Br J Sports Med 2005;39:757–66 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brooks JH, Kemp SP. Injury-prevention priorities according to playing position in professional rugby union players. Br J Sports Med 2011;45:765–75 [DOI] [PubMed] [Google Scholar]
- 4.Haseler CM, Carmont MR, England M. The epidemiology of injuries in English youth community rugby union. Br J Sports Med 2010;44:1093–9 [DOI] [PubMed] [Google Scholar]
- 5.Headey J, Brooks JH, Kemp SP. The epidemiology of shoulder injuries in English professional rugby union. Am J Sports Med 2007;35:1537–43 [DOI] [PubMed] [Google Scholar]
- 6.Gibbs N. Injuries in professional rugby league. A three-year prospective study of the South Sydney Professional Rugby League Football Club. Am J Sports Med 1993;21:696–700 [DOI] [PubMed] [Google Scholar]
- 7.Quarrie KL, Hopkins WG. Tackle injuries in professional Rugby Union. Am J Sports Med 2008;36:1705–16 [DOI] [PubMed] [Google Scholar]
- 8.Sundaram A, Bokor DJ, Davidson AS. Rugby Union on-field position and its relationship to shoulder injury leading to anterior reconstruction for instability. J Sci Med Sport 2011;14:111–14 [DOI] [PubMed] [Google Scholar]
- 9.Funk L, Snow M. SLAP tears of the glenoid labrum in contact athletes. Clin J Sport Med 2007;17:1–4 [DOI] [PubMed] [Google Scholar]
- 10.Badge R, Tambe A, Funk L. Arthroscopic isolated posterior labral repair in rugby players. Int J Shoulder Surg 2009;3:4–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tambe A, Badge R, Funk L. Arthroscopic rotator cuff repair in elite rugby players. Int J Shoulder Surg 2009;3:8–12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Longo UG, Huijsmans PE, Maffulli N, et al. Video analysis of the mechanisms of shoulder dislocation in four elite rugby players. J Orthop Sci 2011;16:389–97 [DOI] [PubMed] [Google Scholar]