

Abstract
Castleman's disease is a rare disorder characterized by benign tumors that may develop in the lymph node tissue throughout the body. Castleman's disease associated with myasthenia gravis is an especially rare disease. Only less than 10 cases have been reported in the world literature. The cause of Castleman's disease is associated with immune mediated reaction, and myasthenia gravis also develops due to an antibody-mediated process. The cause of myasthenia gravis is the immune activity of Castleman's disease, which may be the promoter of the antibody-mediated process. We report here a case of Castleman's disease, which was incidentally found in a patient diagnosed with myasthenia gravis.
Keywords: Myasthenia gravis, Thymectomy, Retroperitoneal neoplasms
CASE REPORT
A 51-year-old male was admitted to the hospital complaining of ptosis, dysarthria, difficult mastication, and general weakness for 2 months. The circulating antibody against acetylcholine receptor serum was markedly elevated. The findings of repeated nerve stimulation tests and single fiber electromyography were consistent with the diagnosis of myasthenia gravis. The chest computed tomography (CT) scan revealed a 6×7 cm left retroperitoneal mass (Fig. 1), and the thymus gland was not shown as enlarged, therefore, indicating thymic hyperplasia. We performed ultrasono-guided needle biopsy to confirm the diagnosis of the retroperitoneal mass. The pathological findings were suspicious for cortical type ectopic thymoma.
Fig. 1.

Chest computed tomography shows a 6×7 cm, well-enhanced round mass containing multiple calcifications in the left retroperitoneal area.
We concluded that the myasthenia gravis developed due to ectopic thymoma or thymus. A retroperitoneal mass excision and thymectomy were performed in order to relieve the myasthenic symptoms. The thoracotomy was first performed in the 11th intercostal space, and a 9×10 cm mass was located in the retroperitoneal space adjacent to the left kidney; the mass was excised. We then changed the position for the sternotomy, and the thymus gland and pericardial fat tissue were removed. The pathologic findings of the thymus suggested normal thymic tissue; there were no hyperplasia, inflammatory changes, or malignancies. The retroperitoneal mass showed a variant of hyaline-vascular type Castleman's disease (Fig. 2). After the surgery, muscle strength dramatically improved for six months; however, the symptoms recurred and were gradually aggravated. The patient was treated with steroids, and plasmapheresis was performed.
Fig. 2.
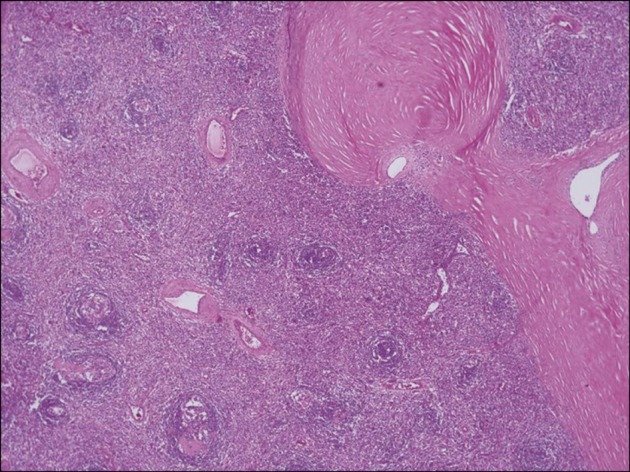
The microscopic findings show an increased number of lymphoid follicles with small, involuted, and partly collagenized germinal centers (H&E, ×40).
DISCUSSION
Castleman's disease is a rare disorder characterized by benign tumors that may develop in the lymph node tissue throughout the body. In some cases it is associated with various clinical conditions; Castleman's disease associated with myasthenia gravis is especially rare [1]. Only less than 10 cases have been reported in the world literature.
Myasthenia gravis is associated with an antibody-mediated process. Antibodies reduce the number of acetylcholine receptors according to three principle mechanisms: accelerated endocytosis and degradation of the acetylcholine receptors, functional blockade by the antibody on the acetylcholine receptors, and complement-mediated damage to the acetylcholine receptors. In particular, the antibody-mediated process was developed by autoimmune reaction [2]. Castleman's disease has been implicated in immune alterations. The overproduction of cytokines and interleukin is believed to play a central role in the development of Castleman's disease and it is also associated with many clinical conditions related to immune disease [3]. The immune activity of Castleman's disease may be the promoter of the antibody-mediated process of myasthenia gravis [4].
Castleman's disease cases associated with myasthenia gravis were mostly of the hyaline-vascular type. Of all the cases reported in the literature, three were the multi-centric type; the others were the localized type. There was no evidence of hyperplasia or malignancy of the thymus in any of the cases. One case was combined with other clinical symptoms including paraneoplastic pemphigus and bronchiolitis obliterans [4-7].
Surgical results have varied. Emson [5] reported on a 14-year-old girl who had undergone an incomplete resection of a retroperitoneal mass and a thymectomy; she had improved slightly. Chorzelski et al. [6] reported on a case of Castleman's disease with myasthenia gravis, paraneoplastic pemphigus, and bronchiolitis obliterans; the tumor was resected incompletely without thymectomy. Although myasthenia gravis was controlled with medication, the patient died due to aggravation of bronchiolitis obliterans, which had developed due to the deposition of immunoglobulin G to the bronchus. Pasaoglu et al. [4] reported on multicentric Castleman's disease that was completely removed by thymectomy. The patient immediately responded to surgery, but after several months, the symptoms recurred and plasmapheresis was needed. In our case, after complete resection of Castleman's node and thymectomy, muscle strength dramatically improved in the immediate postoperative period, but symptoms recurred after 3 months. According to these results, it is controversial to perform thymectomy for the treatment of Castleman's disease associated with myasthenia gravis. However, at minimum the excision of Castleman's lymph node is necessary.
References
- 1.Shahidi H, Myers JL, Kvale PA. Castleman's disease. Mayo Clin Proc. 1995;70:969–977. doi: 10.4065/70.10.969. [DOI] [PubMed] [Google Scholar]
- 2.Newsom-Davis J. Neuromuscular junction channelopathies: a brief overview. Acta Neurol Belg. 2005;105:181–186. [PubMed] [Google Scholar]
- 3.Dispenzieri A, Gertz MA. Treatment of Castleman's disease. Curr Treat Options Oncol. 2005;6:255–266. doi: 10.1007/s11864-005-0008-z. [DOI] [PubMed] [Google Scholar]
- 4.Pasaoglu I, Dogan R, Topcu M, Gungen Y. Multicentric angiofollicular lymph-node hyperplasia associated with myasthenia gravis. Thorac Cardiovasc Surg. 1994;42:253–256. doi: 10.1055/s-2007-1016500. [DOI] [PubMed] [Google Scholar]
- 5.Emson HE. Extrathoracic angiofollicular lymphoid hyperplasia with coincidental myasthenia gravis. Cancer. 1973;31:241–245. doi: 10.1002/1097-0142(197301)31:1<241::aid-cncr2820310132>3.0.co;2-t. [DOI] [PubMed] [Google Scholar]
- 6.Chorzelski T, Hashimoto T, Maciejewska B, Amagai M, Anhalt GJ, Jablonska S. Paraneoplastic pemphigus associated with Castleman tumor, myasthenia gravis and bronchiolitis obliterans. J Am Acad Dermatol. 1999;41(3 Pt 1):393–400. doi: 10.1016/s0190-9622(99)70111-8. [DOI] [PubMed] [Google Scholar]
- 7.Day JR, Bew D, Ali M, Dina R, Smith PL. Castleman's disease associated with myasthenia gravis. Ann Thorac Surg. 2003;75:1648–1650. doi: 10.1016/s0003-4975(02)04963-9. [DOI] [PubMed] [Google Scholar]