

Abstract
Growing research finds that social capital is associated with smoking. However, most studies focus on white populations and do not take into account potential differences between genders. The present study examines the associations between social capital and self-report smoking status and assesses the moderating role of gender among a national representative sample of Asian American adults. Social capital consisted of measures of individual social connectedness (i.e. social ties with relatives and friends) and subjective evaluation of family and neighborhood environment (i.e. family and neighborhood cohesion, family conflict). Asian men were almost three times more likely to be current smokers than women (20.1% vs. 7.0%). Results of multivariate logistic regression analyses showed that family conflicts or higher levels of connectedness with family members were associated with increased odds of being a current smoker among Asian Americans as a whole. Further stratified analysis revealed significant gender differences in several aspects of social capital: there were stronger effects of social connectedness with family members on increasing the odds of smoking for women than for men. In addition, women who had closer connections to friends had greater odds of being current smokers, whereas the opposite was true for men. The findings of this study provide new evidence for the differential effects of social capital by gender, suggesting that more studies are needed to understand social capital’s effects in different racial/ethnic populations and the mechanisms by which the effects vary with gender.
Keywords: Smoking, Social capital, Gender, Asian Americans
INTRODUCTION
Tobacco use is the single most preventable cause of disease and death in the United States. Each year, an estimated 443,000 people die prematurely from smoking or exposure to secondhand smoke, and the productivity loss is as high as $96.8 billion (CDC 2008). One recent national survey found that Asian Americans had the lowest smoking prevalence (9.9%) when compared to other racial/ethnic groups (Dube, Asman, Malarcher, Carabollo 2009). However, researchers have long pointed out that national surveys often fail to take into account the heterogeneity that exists among Asian Americans (Lew and Tanjasiri 2003) and English-only instruments often result in more acculturated samples than the actual populations. In addition, there is limited information on the correlates and predictors of tobacco use among Asian American populations (Lew and Tanjasiri 2003; Maxwell, Bernaards, McCarthy 2005).
Over the past decade, a growing number of studies suggest that social capital is a significant factor for understanding smoking behaviors. For example, Lindström and his colleagues showed in several articles that high levels of individual social capital, measured by social participation or political trust, were beneficial for smoking cessation, risk reduction, and the occurrence of cannabis smoking in Sweden (Lindström 2003; Lindström, Isacsson, The Malmö Shoulder–Neck Study 2002; Lindström 2009). Similarly, Lundborg (2005) revealed that social capital, measured with individual’s social participation and trust, was negatively related with the probability of smoking and illicit drug use among Swedish adolescents. Other studies conceptualizing social capital at ecological levels reached similar conclusions. Greiner et al. (2004) found that higher community rating was negatively associated with individual smoking. Patterson et al. (2004) reported that higher ‘area level’ social cohesion and safety was inversely associated with smoking above and beyond individual characteristics. Smoking is also less prevalent in communities that had a higher level of social participation, trust and safety at community level (Siahpush et al. 2006).
However, research about social capital and smoking is very nascent and suffers several major limitations. First, study samples are often restricted to the general population in European countries and the U.S., few studies have been carried out with racial/ethnic minority populations and virtually no studies have ever been conducted among Asian Americans. As one of the fastest growing groups in the U.S., the Asian American population is highly diversified, providing an ideal backdrop for testing the generalizability of the social capital concept for understanding smoking behaviors. Secondly, this body of work often fails to take into account the moderating effects of gender. It is reasonable to hypothesize that social capital may not necessarily work uniformly across males and females since they may either be more resistant to, or be affected differently by, the contextual influences of social capital (Kavanagh, Turrell, Subramanian 2006; Chuang and Chuang 2008).
To address this gap in knowledge, the present study uses a national representative sample of Asian Americans in the United States to (1) describe the prevalence and patterns of smoking among Asian Americans as a whole and separately by gender, ethnicity, and other characteristics; (2) assess the relationship between social capital and smoking behaviors; and (3) examine whether the relationship is moderated by gender.
METHODS
Sample
This study uses data from the National Institute on Mental Health (NIMH)-funded National Latino and Asian American Study (NLAAS 2002-2003), the first national representative survey of mental health and service use among Asian Americans and Latinos in the United States (Alegria, et al. 2004). The survey population included all non-institutionalized Latinos and Asian Americans who met self-identified racial/ethnic group criteria, and who were 18 years of age or older, residing in households in any of the 50 states and Washington DC. Based on a stratified probability sample design, NLAAS successfully surveyed 2,095 Asian American adults, with a weighted response rate of 65.6% (Heeringa et al. 2004). With 24 missing values eliminated, the final analytic sample for this study consisted of 2,071 respondents, including 1,084 women and 987 men.
Measures
Current smoking status
The dependent variable was determined by whether respondents identified themselves as smokers at the time of the interview, a valid indicator of smoking status in large population studies (Rebagliato 2002; Vartiainen et al. 2002). Respondents were coded as current smokers if they reported being “current smokers”, and others (ex-smokers, never smoked or smoked on a few occasions) coded as “non-current smokers”.
Social capital
Social capital is widely viewed as a multidimensional concept, not easy to measure. To capture this multidimensionality, we used exploratory factor analysis to uncover the structure of individuals’ objective social network and their subjective evaluation of family and neighborhood environment. Specifically, an exploratory factor analysis was conducted among twelve items pertaining to the individuals’ connectedness and mutual concern with relatives and friends, an important part of an individual’s social network structure. Two orthogonal factors corresponded respectively to relationship with friends and relatives (Eigenvalue>1.0). Using a factor loading of 0.60 as the cutoff for inclusion, three items concerning the ties with friends (i.e. Frequency of talk on phone/get together with friends; reliance on friends for serious problem; and open up to friends and talk about worries) and three items concerning the ties with relatives (i.e. frequency of talk on phone with relatives; reliance on relatives for serious problem; open up to relatives to discuss worries) were retained. Cronbach’s alpha for the retained items in both factors was above 0.70.
The same approach was utilized for a factor analysis of twenty-four items related to the individuals’ perception of their social environment. Three factors (Eigenvalue>1.0) were retained and termed respectively as “Neighborhood Cohesion”, “Family Cohesion”, and “Family Conflict”. While neighborhood and family cohesion measures provided a positive value of social capital, family conflict ipso facto reflects the lack of social capital, an alternative way of measuring social capital as proposed by social capital theorist Francis Fukuyama (Fukuyama 1997). The Neighborhood Cohesion construct consisted of five items (i.e. people in the neighborhood can be trusted, help in emergency, feel safe alone at night, etc., Cronbach’s alpha=0.81). The Family Cohesion construct consisted of 10 items (e.g., family members respect one another, share values, work well as a family, etc., Cronbach’s alpha=0.92), and the Family Conflict construct consisted of five items (e.g. argue with family, personal goals conflict with family, etc., Cronbach’s alpha=0.75). Ultimately, five composite indicators of social capital were created by calculating the statistical mean from the retained items in each extracted factor, a methodological approach consistent with that used by other investigators (Patterson et al. 2004). For statistical analysis, each indicator was dichotomized to represent low and high levels of social capital with the mean of as the cutoff.
Socioeconomic, demographics and acculturation
Besides the social capital variables, we also included variables that have been shown to be related with smoking in the literature (i.e., socioeconomic status, demographics and acculturation). Socioeconomic status (SES) was measured by education levels (“less than high school”, “high school graduate”, “some college”, and “university graduate and above”) and annual household income (1st Quartile ≤$24,999, 2nd Quartile=$25,000-62,499, 3rd Quartile=$62,500-107,498, and 4th Quartile=$107,499 and above). Another SES factor, everyday discrimination is also included because prior research has found the people who report greater experiences of everyday discrimination are more likely to report substance use (Gee, Delva, Takeuchi 2007). The measure was derived from nine question items (Cronbach’s alpha=0.91) originally used in the Detroit Area Study to measure perceptions of chronic and routine unfair treatment (Williams et al. 1997). We used tertiles to create a three-category variable of everyday discrimination.
The demographic characteristics included in the study were ethnicity, age, gender, marital status, and religion. There were four ethnic categories in the study: Vietnamese, Filipinos, Chinese, and Others. The “Others” category, consisting of people from over a dozen Asian backgrounds, was a residual category without particular theoretical significance, but included in the analysis for sample completeness. Age was collapsed into three categories (18/24; 25/39; 40/64; 65+) to match the age distribution in the data. Religious belief was assessed by asking respondents how often they seek religious/spiritual comfort during difficult times. The variable was dichotomized into “often or sometimes seek religious comfort” vs. “rarely or never seek religious comfort”. Marital status is categorized into “married (currently married/cohabiting)” vs. “other than married (divorced/separated/widowed/never married)”.
Acculturation, a variable also shown to be correlated with smoking among Asian Americans (Ma et al. 2004), was measured by the respondents’ ability to speak, read and write in English (Cronbach’s alpha=0.97), and duration of stay in the U.S.A. Individuals who responded poor/fair on all three items were coded as having poor English proficiency. Duration of stay in the U.S. was measured with a 5-year cut-point, since it typically takes immigrants at least 5 years to obtain citizenship in the U.S. A summary of social capital indicators and covariates is included in the Appendix.
Analysis
Following the estimation of current smoking prevalence for the entire sample and by gender, multivariate logistic regression analyses were conducted to test whether social capital was significantly associated with smoking. We chose to enter social capital indicators with SES, demographics, and acculturation variables in a step-wise fashion in order to discern possible changes of the associations between social capital and smoking in the presence of different groups of covariates. Then, we tested all two-way interactions between gender and each indicator of social capital controlling for SES, demographics, and acculturation. Only significant interactions were included and reported in the final model for presentation in this paper. We also checked for potential multicollinearity problem by calculating the Variance Inflation Factor (VIF) for all the variables in the baseline model, which ranged from 1.09 to 3.70, suggesting that multicollinearity is not a significant issue for this study. In addition, survey design effects were taken into account in the estimation of standard errors in the presence of stratification and clustering (Kish 1965). All analyses were conducted with STATA 10.0 (StataCorp 2007).
RESULTS
Table 1 presents the weighted percentage of Asian American adults who were classified as current smokers by gender. The overall current smoking prevalence among Asian adult populations was estimated at 13.2%, slightly higher than the 11.7% reported by the CDC for the same period (CDC 2004). Consistent with previous findings (Lew and Tanjasiri 2003; Ma et al. 2004; Shelley et al. 2004; Tang, Shimizu, Chen 2005), the proportion of Asian men who smoke was almost three times that of Asian women (20.1% vs. 7.0%, p<0.01). By ethnicity, although the overall smoking prevalence was not statistically significant (p=0.12), there were significant differences among men and women from different Asian ethnic groups (p=0.03). For example, Chinese men (16.3%) had the lowest level of smoking rates when compared to Vietnamese (29.6%) and Filipino (25.5%) men. However, Vietnamese women had the lowest prevalence (2.3%) when compared to Chinese (5.7%), Filipinas (8.3%), and other Asian American women (8.9%).
Table 1.
Current smoking status among Asian American by gender, NLAAS, 2002-03 (N=2,071)
| % Male (SE) | p-value | % Female (SE) | p-value | % Overall (SE) | p-value | |
|---|---|---|---|---|---|---|
| Current Smoking | 20.1(2.2) | 7.0 (1.4) | 13.2(1.0) | <0.01 | ||
| Social Capital | ||||||
| Ties with Relatives | 1.00 | <0.01 | 0.41 | |||
| Low | 20.1(3.0) | 3.2(0.7) | 12.2(1.6) | |||
| High | 20.1(2.6) | 9.2(2.0) | 13.9(1.1) | |||
| Ties with Friends | 0.60 | <0.01 | 0.24 | |||
| Low | 21.0(2.9) | 2.9(0.8) | 12.0 (1.3) | |||
| High | 19.4(2.5) | 9.6(2.0) | 14.0 (1.3) | |||
| Family Cohesion | 0.43 | 0.75 | 0.61 | |||
| Low | 22.3(4.6) | 6.4(1.6) | 14.2(2.5) | |||
| High | 18.9(1.8) | 7.3(2.0) | 12.7(1.2) | |||
| Neighborhood Cohesion | 0.02 | 0.26 | <0.05 | |||
| Low | 23.9(2.9) | 8.5(2.7) | 15.5(1.6) | |||
| High | 17.3(2.3) | 5.8(0.9) | 11.4(1.1) | |||
| Family Conflict | 0.07 | 0.04 | 0.01 | |||
| Low | 18.3(2.2) | 5.6(1.5) | 11.8(0.9) | |||
| High | 23.3(3.1) | 9.1(1.5) | 15.4(1.5) | |||
| Socioeconomic Status (SES) | ||||||
| Education | <0.01 | 0.17 | <0.01 | |||
| Less than High School | 35.8(7.2) | 3.1(1.8) | 16.5(3.0) | |||
| High School Graduate | 29.9(3.2) | 10.9(4.1) | 20.2(2.9) | |||
| Some College | 18.8(3.8) | 7.6(1.4) | 12.2(1.8) | |||
| University Graduates and Above | 12.8(2.0) | 6.5(1.7) | 9.8(1.1) | |||
| Household Income | <0.01 | 0.25 | 0.04 | |||
| 1st Quartile | 27.6(6.5) | 3.8(1.7) | 13.3(3.2) | |||
| 2nd Quartile | 34.2(6.9) | 11.5(3.8) | 21.0(3.3) | |||
| 3rd Quartile | 11.2(2.1) | 7.0(3.0) | 9.0(1.7) | |||
| 4th Quartile | 18.8(2.4) | 7.3(1.4) | 13.2(1.3) | |||
| Demographics | 0.03 | 0.33 | 0.12 | |||
| Ethnicity | ||||||
| Vietnamese | 29.6(3.5) | 2.3(0.9) | 15.2(1.8) | |||
| Filipinos | 25.5(3.0) | 8.3(1.6) | 16.4(1.7) | |||
| Chinese | 16.3(2.9) | 5.7(1.5) | 10.7(1.4) | |||
| Others | 16.5(3.9) | 8.9(3.4) | 12.5(2.1) | |||
| Marital Status | 0.38 | 0.03 | 0.03 | |||
| Married | 19.2(1.8) | 5.5(1.2) | 15.9(1.8) | |||
| Not Married | 21.8(3.9) | 10.4(2.6) | 12(12.0) | |||
| Religion | 0.14 | 0.84 | 0.05 | |||
| Religious | 17.1(1.8) | 6.9(1.6) | 15.2(1.6) | |||
| Not Religious | 22.2(3.4) | 7.2(1.5) | 11.1(1.1) | |||
| Acculturation | ||||||
| English Proficiency | <0.01 | <0.01 | 0.45 | |||
| Poor/Fair | 31.4(5.3) | 1.8(0.7) | 14.7(2.4) | |||
| Excellent/Very Well/Well | 16.2(1.7) | 9.2(2.0) | 12.6(1.0) | |||
| Duration of Stay in US | 0.24 | 0.04 | 0.53 | |||
| US born | 17.2 (2.5) | 12.1 (2.7) | 14.6(2.2) | |||
| 1-4 years | 10.0 (5.9) | 2.8 (1.5) | 10.4(3.0) | |||
| 5-10 years | 28.0 (5.3) | 2.3 (1.5) | 14.7(2.7) | |||
| 11-20 years | 22.6 (4.8) | 7.2 (2.3) | 14.3(1.7) | |||
| 20+years | 16.7(2.2) | 6.6(2.8) | 11.3(1.8) | |||
Different gender patterns of smoking were identifiable across other domains. Among men, there was a clear education gradient of smoking (p<0.01). About 35.8% of men with less than 12 years of education were current smokers, compared with 12.8% for university graduates and above. However, such pattern was not observed among women (p=0.17). With regard to income, Asian men with income below the 50% cutoff ($62,499) had much higher prevalence of smoking than those above the 50%. In addition, men with better English proficiency had significantly lower smoking prevalence, while the reverse was true for women.
In terms of social capital and smoking prevalence, the stratified data by gender showed that the prevalence of current smoking among women having high levels of ties with friends or relatives was significantly higher than those with low level of these two types of social capital (Relatives: 9.2% vs. 3.2%, p<0.01; Friends, 9.6% vs. 2.9%, p<0.01). Secondly, living in a highly cohesive neighborhood was associated with significantly lower prevalence of smoking than those living in a neighborhood with low cohesion for men (17.3% vs. 23.9%, p=0.02), but these associations were not observed for women (p=0.26). On the other hand, women experiencing high level of family conflict were significantly more likely to be current smokers (9.1% vs. 5.6%, p=0.04); for men, the effects were not significant, though a trend was observed (p=0.07).
To discern the relative associations between social capital and smoking behaviors and to assess whether the associations were moderated by gender, a series of logistic regression models were tested. Table 2 shows the results of the multivariate logistic regressions. The first model included only the social capital indicators, which showed that only family conflict was significantly and positively associated with being a current smoker (OR=1.32; 95% CI=1.05-1.65). In fact, such positive associations were robust regardless of adjustments for other covariates in the rest of the models, suggesting the strong associations between family conflicts and smoking. Although other social capital indicators in this model were not statistically significant, there was some evidence that higher levels of ties with relatives/friends were associated with increased likelihood of smoking, while the reverse was true for family and neighborhood cohesion.
Table 2.
Logistic Regression Results: Current smoking status (N=2,071; 0=non-smokers; 1=smokers)
| Characteristics | Model 1 | Model 2 | Model 3 | Model 4 (Baseline model) | Model 5 (Interaction Model) |
|---|---|---|---|---|---|
| OR(95%CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Social Capital | |||||
| Ties with Friends (low=ref.) | |||||
| High | 1.19(0.84-1.68) | 1.25(0.86-1.82) | 1.18(0.81-1.73) | 1.23(0.86-1.78) | 0.86(0.57-1.29) |
| Ties with Relatives (low=ref.) | |||||
| High | 1.20(0.84-1.71) | 1.35(0.96-1.91) | 1.58(1.09-2.29)b | 1.62(1.12-2.37)b | 1.34(0.85-2.12) |
| Family Cohesion (low=ref.) | |||||
| High | 0.98(0.57-1.69) | 1.00(0.57-1.78) | 1.21(0.69-2.11) | 1.24(0.73-2.13) | 1.21(0.72-2.01) |
| Neighborhood Cohesion (low=ref.) | |||||
| High | 0.69(0.46-1.03) | 0.71(0.48-1.03) | 0.71(0.45-1.11) | 0.69(0.43-1.10) | 0.69(0.43-1.10) |
| Family Conflict (Low=ref.) | |||||
| High | 1.32(1.05-1.65)a | 1.47(1.16-1.86)a | 1.64(1.25-2.16)a | 1.65(1.26-2.15)a | 1.61(1.23-2.10)a |
| Socioeconomic Status (SES) | |||||
| Education (less than HS=ref) | |||||
| High School Graduate | 1.19(0.60-2.36) | 0.98(0.45-2.12) | 1.02(0.48-2.15) | 0.99(0.44-2.22) | |
| Some College | 0.64(0.43-0.95)b | 0.55(0.36-0.84)b | 0.59(0.39-0.89)b | 0.56(0.35-0.89)b | |
| University Graduate and Above | 0.47(0.28-0.79)a | 0.36(0.19-0.67)a | 0.42(0.24-0.73)a | 0.38(0.20-0.72)a | |
| Income (1st Quartile=ref) | |||||
| 2nd Quartile | 1.60(0.64-3.99) | 1.49(0.65-3.43) | 1.50(0.68-3.33) | 1.53(0.69-3.38) | |
| 3rd Quartile | 0.66(0.33-1.30) | 0.50(0.23-1.11) | 0.50(0.24-1.02) | 0.51(0.26-1.02) | |
| 4th Quartile | 1.15(0.71-1.86) | 0.84(0.51-1.41) | 0.83(0.51-1.34) | 0.85(0.52-1.39) | |
| Discrimination (low=ref) | |||||
| Medium | 1.32(0.74-2.36) | 1.30(0.70-2.43) | 1.38(0.73-2.60) | ||
| High | 1.26(0.65-2.42) | 1.22(0.60-2.46) | 1.26(0.63-2.52) | ||
| Demographics | |||||
| Ethnicity (Vietnamese=ref) | |||||
| Filipinos | 1.27(0.79-2.04) | 1.37(0.87-2.17) | 1.30(0.81-2.09) | ||
| Chinese | 0.70(0.42-1.17) | 0.71(0.43-1.16) | 0.68(0.42-1.12) | ||
| Others | 0.96(0.52-1.79) | 1.03(0.55-1.93) | 0.98(0.53-1.80) | ||
| Age (<24=ref), Years | |||||
| 25-39 | 1.52(0.80-2.89) | 1.48(0.81-2.70) | 1.45(0.79-2.66) | ||
| 40-64 | 1.22(0.73-2.02) | 1.10(0.66-1.83) | 1.12(0.67-1.88) | ||
| ≥65 | 0.32(0.11-0.93)b | 0.27(0.09-0.86)b | 0.29(0.09-0.96)b | ||
| Gender (male=ref) | |||||
| Female | 0.26(0.15-0.47)a | 0.26(0.15-0.46)a | 0.05(0.02-0.14)a | ||
| Marriage (not Married=ref) | |||||
| Married | 0.83(0.66-1.04) | 0.84(0.66-1.07) | 0.83(0.64-1.07) | ||
| Religion (Not Religious=ref) | |||||
| Religious | 0.68(0.48-0.96)b | 0.68(0.48-0.96)b | 0.68(0.47-0.98)b | ||
| Acculturation | |||||
| English (poor/fair=ref) | |||||
| Excellent/Very Well/Well | 0.74(0.47-1.15) | 0.74(0.47-1.18) | |||
| Year in US (Native Born=ref) | |||||
| >5 years | 0.59(0.24-1.47) | 0.62(0.25-1.53) | |||
| 5-10 years | 0.87(0.52-1.45) | 0.91(0.55-1.52) | |||
| 11-20 years | 0.97(0.63-1.49) | 0.97(0.63-1.50) | |||
| 20+ | 0.93(0.52-1.67) | 0.88(0.49-1.57) | |||
| Interactions | |||||
| Gender* Friends Ties | 3.93(1.59-9.72)a | ||||
| Gender*Relatives Ties | 2.34(1.16-4.73)a | ||||
Notes:
<0.01;
<0.05;
OR: Odds Ratio; Ref.: Reference Group
The introduction of SES in Model 2 changed the odds ratio of the social capital variables slightly, but not the significance level of any of the variables, indicating that education and income barely moderated the association between smoking and social capital. However, education itself had a significant depressing effect on smoking: people with some college education (OR=0.64; 95% CI=0.43-0.95) or a university degree (OR=0.47; 95%CI=0.28-0.79) had much lower odds of smoking when compared with individuals with less than a high school education. Somewhat unexpected, income was not significantly associated with smoking.
After additionally adjusting for socio-demographics characteristics in Model 3, ties with relatives became significantly associated with being a current smoker. Specifically, the odds of smoking for individuals with a high level of ties with relatives were 1.58 times greater than for individuals with a low level of ties with relatives. In addition, compared with respective reference groups, Asian females (OR=0.26; 95%CI=0.15-0.47), individuals who sought religious comfort during difficulties (OR=0.68, 95%CI=0.48-0.96), and people who were over 65 years old (OR=0.32; 95%CI=0.11-0.93), were significantly less likely to be a current smoker. Lastly, Model 4 showed that neither English proficiency nor duration of stay in America was significantly associated with smoking, incicating that acculturation did not have an independent effect on smoking behaviors among Asian Americans in this sample.
The last step was to investigate the differential effects of social capital. Five two-way interaction terms of gender and each indicator of social capital were added separately to the baseline model (i.e., Model 4) to test whether the effects of social capital on smoking behavior were modified by gender. Results showed that only two interactions--gender and relatives’ ties, gender and friends’ ties--were significant. Subsequently, Model 5 included these two significant interaction terms simultaneously and both remained significant, suggesting that ties with friends and relatives were independently and differentially associated with smoking behavior across Asian American men and women.
To better illustrate the interaction effects, predicted probabilities of smoking were calculated and plotted in Figures 1 and 2 below. With all other variables held at their reference level, Figure 1 showed that although women had a much lower smoking prevalence than men (3% v. 38%), the rate of increase of the predicted probability of smoking was significantly faster for women than for men, meaning that ties with relatives had stronger effects on women than on men. Figure 2 demonstrated that the effects of ties with friends on smoking by gender: the upward slope for females showed that friends’ connections had an increasing effect on smoking for women, whereas the opposite was true for men.
Figure 1.
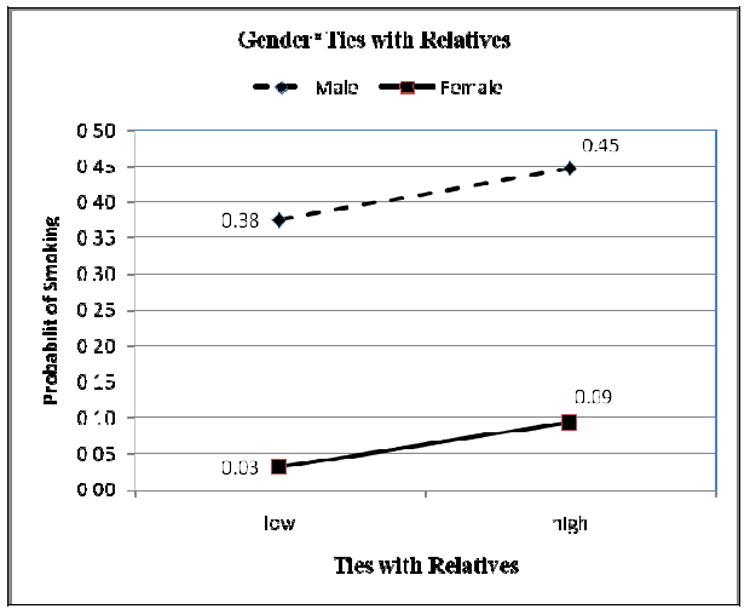
Predicted Probability of Smoking by Gender and Level of Ties with Relatives
Figure 2.
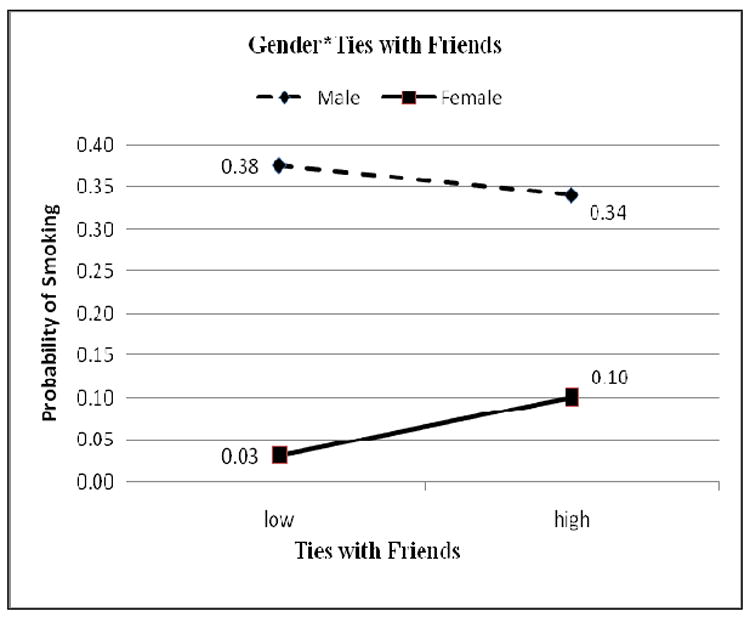
Predicted Probability of Smoking by Gender and Level of Ties with Friends
DISCUSSION
Health statistics aggregated across broad gender or ethnic categories may mask disparities between specific sub-populations. Although many national surveys have found that Asian Americans as a whole have the lowest levels of smoking prevalence among all racial groups (CDC 2004; Dube et al. 2009), researchers who have conducted more culturally and linguistically appropriate studies agree that smoking may be much more common and that there exists tremendous heterogeneity in smoking patterns within Asian populations, particularly by gender, ethnicity and other characteristics (Lew and Tanjasiri 2003; Maxwell et al. 2005). The present study provides additional evidence of the extensive intra-group differences in smoking among Asian American populations. Asian males, particularly Vietnamese males, were far more likely to be current smokers. Nevertheless, the challenge of promoting tobacco control among Asian males is compounded by both an Asian American culture in which smoking by males tends to be an accepted, or at least tolerated, social practice (Chuang and Chuang 2008), and a smoking epidemic in their original countries where about 62% of men are smokers (Lew and Tanjasiri 2003). Thus, how to prevent and reduce smoking among Asian American men remains a serious public health challenge.
Though Asian females are far less likely to smoke as found in this study, there is some evidence that increasingly more Asian females are taking up smoking. One national study found that there were dramatic increases in smoking among Asian American girls from the 7th through 12th grades (Appleyard, Messeri, Haviland 2001). Others pointed out that smoking rates were especially high among U.S.-born Filipino-American women (Maxwell et al. 2005). Recently, Romero et al. (2008) showed that, compared with a significant decline of smoking prevalence among Filipino men and non-Hispanic white females from 1990 to 2002 in California, the rate for Filipino women remained stable during this same period (Romero et al. 2008). The current study shows that smoking rate is the highest among women born in the U.S. and among those with better English skills and higher levels of social networks. The findings suggest that in a less restrictive environment, Asian American women might be more likely to smoke and to ignore traditional cultural double standard pressures that discourage them from smoking (Maxwell et al. 2005).
Social capital researchers postulate that higher levels of social capital may help reduce the prevalence of smoking via a number of pathways, such as rapid diffusion of anti-smoking messages, promotion of social norms and social control against smoking, controlling over deviant behaviors or/and enhancing trust in public institutions that offer anti-smoking campaigns (Lindström et al. 2003; Siahpusha et al. 2006). In our examination of the association between social capital and smoking, we found various dimensions of social capital to be differentially associated with smoking behaviors among Asian American populations. Specifically, closer ties with relatives were associated with increased likelihood of being a current smoker, while relationship with friends was not statistically associated with smoking among the aggregated Asian American populations. Another finding is that lack of social capital, as measured by family conflict in this analysis, was strongly and significantly related with an increased probability of smoking. Methodologically, as Fukuyama (1997) has argued, while measuring social capital is difficult, measuring the lack of social capital, such as family conflict, crimes rates, etc, might be a good alternative measurement strategy given such data are usually more readily available. Research is needed to test if among Asian American smokers a reduction in family conflict impact smoking behaviors.
There are few studies that examine gender differences in the relationship between social capital and smoking among Asian American populations. But outside the U.S., Chuang and Chuang (2008) showed that community social capital had a greater depressing effect on smoking among women than men in Taiwan. In the present study we found significant gender differences. Females with close ties with relatives and friends were at greater risk to become smokers as compared with men. One possible explanation is that women are more likely than the men to be under chronic and daily stress (Matud 2004)—a factor contributing to increased smoking (Pomerleau and Pomerleau 1987). At the same time, women are more likely than men to share their distress with family members and friends. Thus, it might be the stress per se that led women to smoke rather than ties/concern with those in their social network. Another possible explanation is related to the experience of immigration. Smoking in many Asian cultures is not as acceptable as in the U.S., but as Asian women migrate to the U.S. and expand their network of friends, some of their behaviors may change, including smoking (Romero et al. 2008). One meta analysis suggested that acculturated Asian American women were five times more likely to smoke than traditional women, while acculturated men were 53% less likely to smoke than non-acculturated men (Choi et al. 2008). Thus, with expanded social network with friends and relatives, better acculturated women were more likely to take up smoking. Further research is needed to more closely examine the mechanisms that may explain the gender differences in social capital and smoking among Asian American populations.
CONCLUSION
Our findings should be considered in light of the following limitations. First, our data are cross-sectional. Therefore, the relationships found between social capital and smoking should be cautiously interpreted as associations rather than as evidence of causality by social capital. Second, the data of this study are based on self-reports and are restricted to the limitation inherent in self-reports. These data may be an underestimate of tobacco use among Asians, particularly among women. Third, given the secondary nature of the study, data were not available on other important aspects of social capital (i.e., linking social capital, social participation, and association membership). However, unlike prior studies which tend to use one or at most two measures of social capital, we measured five aspects including social ties with friends and relatives, family cohesion, family conflict, neighborhood cohesion, and assessed their influences separately. Future research should consider both the individual and higher levels of social capital.
Nevertheless, the study represents the first attempt to examine how social capital is related to smoking behaviors among Asian-American populations and adds to the growing literature on the health effects of social capital. The findings suggest that the different dimensions of social capital are not uniformly associated with individual smoking behavior, and the effects may be direct and interactive. The finding that gender plays a moderating role on the association between social capital and smoking behaviors should inform policies and interventions (i.e., increased tobacco taxes, effective tobacco cessation treatments, comprehensive ban on tobacco advertising, mandated graphic warning labels on tobacco products) that are under consideration (Fiore and Baker 2009).
Acknowledgments
This publication was made possible by Grant Numbers P60 MD000538 (NIH National Institute for Minority Health and Health Disparities) and U58DP001022 (CDC REACH U.S. Program). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH and the CDC.
References
- Alegria M, Takeuchi D, Canino G, Duan N, Shrout P, Meng XL. Considering context, place and culture: the National Latino and Asian American Study. International Journal of Methods in Psychiatric Research. 2004;13(4):208–220. doi: 10.1002/mpr.178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Appleyard J, Messeri P, Haviland M. Smoking among Asian American and Pacific Islander youth: data from the 2000 National Youth Tobacco Survey. Asian American and Pacific Islander Journal of Health. 2001;9(1):3–12. [PubMed] [Google Scholar]
- CDC. Prevalence of cigarette use among 14 racial/ ethnic populations—United States, 1999–2001. Morb Mortal Wkly Rep. 2004;53:49–52. [PubMed] [Google Scholar]
- CDC. Smoking-attributable mortality, years of potential life lost, and productivity losses--United States, 2000-2004. Morb Mortal Wkly Rep. 2008;57:1226–1228. [PubMed] [Google Scholar]
- Choi S, Rankin S, Stewart A, Oka R. Effects of acculturation on smoking behavior in Asian Americans: A meta-analysis. Journal of Cardiovascular Nursing. 2008;23(1):67–73. doi: 10.1097/01.JCN.0000305057.96247.f2. [DOI] [PubMed] [Google Scholar]
- Chuang YC, Chuang KY. Gender differences in relationships between social capital and individual smoking and drinking behavior in Taiwan. Social Science and Medicine. 2008;67(8):1321–1330. doi: 10.1016/j.socscimed.2008.06.033. [DOI] [PubMed] [Google Scholar]
- Dube S, Asman K, Malarcher A, Carabollo R. Cigarette smoking among adults and trends in smoking cessation-United States, 2008. Morbidity and Mortality Weekly Report. 2009;58(44):1227–1232. [PubMed] [Google Scholar]
- Fiore M, Baker T. Stealing a march in the 21st century: accelerating progress in the 100-year war against tobacco addiction in the United States. American Journal of Public Health. 2009;99(7):1–6. doi: 10.2105/AJPH.2008.154559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fukuyama F. Social capital. The Tanner Lectures on Human Values. 1997;19:375–484. [Google Scholar]
- Gee GC, Delva J, Takeuchi DT. Relationships between self-report unfair treatment and prescription medication use, illicit drug use, and alcohol dependence among Filipino Americans. American Journal of Public Health. 2007;97(5):933–940. doi: 10.2105/AJPH.2005.075739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greiner KA, Li C, Kawachi I, Hunt DC, Ahluwalia JS. The relationships of social participation and community ratings to health and health behaviors in areas with high and low population density. Social Science and Medicine. 2004;59(11):2303–2312. doi: 10.1016/j.socscimed.2004.03.023. [DOI] [PubMed] [Google Scholar]
- Heeringa SG, Wagner J, Torres M, Duan N, Adams T, Berglund P. Sample designs and sampling methods for the Collaborative Psychiatric Epidemiology Studies (CPES) International Journal of Methods in Psychiatric Research. 2004;13(4):221–240. doi: 10.1002/mpr.179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kavanagh AM, Turrell G, Subramanian SV. Does area-based social capital matter for the health of Australians? A multilevel analysis of self-rated health in Tasmania. International journal of epidemiology. 2006;35(3):607–613. doi: 10.1093/ije/dyl010. [DOI] [PubMed] [Google Scholar]
- Kish L. Survey sampling. New York: Wiley; 1965. [Google Scholar]
- Lew R, Tanjasiri SP. Slowing the epidemic of tobacco use among Asian Americans and Pacific Islanders. American Journal of Public Health. 2003;93(5):764–768. doi: 10.2105/ajph.93.5.764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindström M. Social capital and the miniaturization of community among daily and intermittent smokers: a population-based study. Preventive Medicine. 2003;36(2):177–184. doi: 10.1016/s0091-7435(02)00049-x. [DOI] [PubMed] [Google Scholar]
- Lindström M. Social capital, political trust and daily smoking and smoking cessation: A population-based study in southern Sweden. Public health. 2009;123(7):496–501. doi: 10.1016/j.puhe.2009.06.010. [DOI] [PubMed] [Google Scholar]
- Lindström M, Isacsson SO. The Malmö Shoulder–Neck Study G, 2002. Smoking cessation among daily smokers, aged 45–69 years: a longitudinal study in Malmö, Sweden. Addiction. 2002;97(2):205–215. doi: 10.1046/j.1360-0443.2002.00036.x. [DOI] [PubMed] [Google Scholar]
- Lindström M, Moghavedassi M, Bolin K, Lingren B, Merlo J. Social Participation, social capital and daily tobacco smoking: A population-based multilevel analysis in Malmo, Sweden. Scandinavian Journal of Public Health. 2003;31:444–450. doi: 10.1080/14034940310006203. [DOI] [PubMed] [Google Scholar]
- Lundborg P. Social capital and substance use among Swedish adolescents—an explorative study. Social Science and Medicine. 2005;61(6):1151–1158. doi: 10.1016/j.socscimed.2004.12.031. [DOI] [PubMed] [Google Scholar]
- Ma GX, Tan Y, Toubbeh JI, Su X, Shive SE, Lan Y. Acculturation and smoking behavior in Asian-American populations. Health Education Research. 2004;19(6):615–625. doi: 10.1093/her/cyg070. [DOI] [PubMed] [Google Scholar]
- Matud MP. Gender differences in stress and coping styles. Personality and individual differences. 2004;37(7):1401–1415. [Google Scholar]
- Maxwell A, Bernaards C, McCarthy W. Smoking prevalence and correlates among Chinese- and Filipino-American adults: findings from the 2001 California Health Interview Survey. Preventive Medicine. 2005;41(2):693–699. doi: 10.1016/j.ypmed.2005.01.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patterson JM, Eberly LE, Ding Y, Hargreaves M. Associations of smoking prevalence with individual and area level social cohesion. Journal of Epidemiology and Community Health. 2004;58(8):692–697. doi: 10.1136/jech.2003.009167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pomerleau CS, Pomerleau OF. The Effects of a Psychological Stressor on Cigarette Smoking and Subsequent Behavioral and Physiological Responses. Psychophysiology. 1987;24(3):278–285. doi: 10.1111/j.1469-8986.1987.tb00295.x. [DOI] [PubMed] [Google Scholar]
- Rebagliato M. Validation of self report smoking. Journal of Epidemiology and Community Health. 2002;56:163–164. doi: 10.1136/jech.56.3.163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Romero RA, Messer K, West JH, White MM, Trinidad DR. Smoking trends among Filipino adults in California, 1990–2002. Preventive Medicine. 2008;46:336–339. doi: 10.1016/j.ypmed.2007.12.004. [DOI] [PubMed] [Google Scholar]
- Shelley D, Fahs M, Scheinmann R, Swain S, Qu J, Burton D. Acculturation and tobacco use among Chinese Americans. American Journal of Public Health. 2004;94(2):300–307. doi: 10.2105/ajph.94.2.300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Siahpush M, Borland R, Taylor J, Singh GK, Ansari Z, Serraglio A. The association of smoking with perception of income inequality, relative material well-being, and social capital. Social Science and Medicine. 2006;63(11):2801–2812. doi: 10.1016/j.socscimed.2006.07.015. [DOI] [PubMed] [Google Scholar]
- StataCorp. Stata Statistical Software: Release 10. College Station, TX: StataCorp LP; 2007. [Google Scholar]
- Tang H, Shimizu R, Chen MS. English language proficiency and smoking prevalence among California’s Asian Americans. Cancer. 2005;104(12 Suppl):2982–2988. doi: 10.1002/cncr.21523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vartiainen E, Seppala T, Lillsunde P, Puska P. Validation of self report smoking by serum cotinine measurement in a community-based study. Journal of Epidemiology and Community Health. 2002;56:167–170. doi: 10.1136/jech.56.3.167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams DR, Yan Y, Jackson JS, Anderson NB. Racial differences in physical and mental health. Journal of Health Psychology. 1997;2(3):335–351. doi: 10.1177/135910539700200305. [DOI] [PubMed] [Google Scholar]