

Abstract
Objectives To examine mortality and revision rates among patients with osteoarthritis undergoing hip arthroplasty and to compare these rates between patients undergoing cemented or uncemented procedures and to compare outcomes between men undergoing stemmed total hip replacements and Birmingham hip resurfacing.
Design Cohort study.
Setting National Joint Registry.
Population About 275 000 patient records.
Main outcome measures Hip arthroplasty procedures were linked to the time to any subsequent mortality or revision (implant failure). Flexible parametric survival analysis methods were used to analyse time to mortality and also time to revision. Comparisons between procedure groups were adjusted for age, sex, American Society of Anesthesiologists (ASA) grade, and complexity.
Results As there were large baseline differences in the characteristics of patients receiving cemented, uncemented, or resurfacing procedures, unadjusted comparisons are inappropriate. Multivariable survival analyses identified a higher mortality rate for patients undergoing cemented compared with uncemented total hip replacement (adjusted hazard ratio 1.11, 95% confidence interval 1.07 to 1.16); conversely, there was a lower revision rate with cemented procedures (0.53, 0.50 to 0.57). These translate to small predicted differences in population averaged absolute survival probability at all time points. For example, compared with the uncemented group, at eight years after surgery the predicted probability of death in the cemented group was 0.013 higher (0.007 to 0.019) and the predicted probability of revision was 0.015 lower (0.012 to 0.017). In multivariable analyses restricted to men, there was a higher mortality rate in the cemented group and the uncemented group compared with the Birmingham hip resurfacing group. In terms of revision, the Birmingham hip resurfacings had a similar revision rate to uncemented total hip replacements. Both uncemented total hip replacements and Birmingham hip resurfacings had a higher revision rate than cemented total hip replacements.
Conclusions There is a small but significant increased risk of revision with uncemented rather than cemented total hip replacement, and a small but significant increased risk of death with cemented procedures. It is not known whether these are causal relations or caused by residual confounding. Compared with uncemented and cemented total hip replacements, Birmingham hip resurfacing has a significantly lower risk of death in men of all ages. Previously, only adjusted analyses of hip implant revision rates have been used to recommend and justify use of cheaper cemented total hip implants. Our investigations additionally consider mortality rates and suggest a potentially higher mortality rate with cemented total hip replacements, which merits further investigation.
Introduction
Sir John Charnley’s1 introduction of low friction total hip replacement2 3 50 years ago revolutionised the treatment of hip arthritis. Today, hundreds of combinations of stems and cups are successfully used. The different systems, however, are simply categorised by their mode of fixation as cemented or uncemented implants.
In patients under the age of 55, total hip replacements have not been such a success, and hip resurfacing was developed as a conservative alternative. Several reports show better medium term implant survival and hip function4 5 with resurfacing than with replacement6 7 in these younger patients.8 9 Initially hip resurfacing was carried out in women as well, but reported results were poor.10 Data from the National Joint Registry shows that the cumulative failure rate of Birmingham hip resurfacing in women is 1% per year,11 which borders on the edge of acceptability according to guidelines from the National Institute for Health and Clinical Excellence (NICE). This has resulted in reduced acceptance of this procedure in women. There are therefore three classes of hip arthroplasty that have gained widespread acceptance and use: cemented and uncemented total hip replacement in men and women and hip resurfacing in men. The appendix provides details of the hip replacement and hip resurfacing techniques with x ray images.
The number of procedures for hip arthroplasty is increasing as the size of the elderly population increases. The availability of various devices, with their differing materials and design features, makes it essential to monitor their safety and efficacy.12 13 Towards this end, orthopaedic associations in many countries14 15 16 17 18 have been advocating the establishment of national arthroplasty registers to acquire and analyse data. The National Joint Register of England and Wales19 is currently the world’s largest dataset of arthroplasty procedures. This contains over 400 000 records of patients who underwent hip arthroplasty and includes vital information such as age, sex, primary diagnosis, and ASA grade (the American Society of Anesthesiologists classification system20 for assessing the fitness of patients before surgery, from grade 1 (fit and healthy) to grade 5 (expected to die within 24 hours with or without an operation)), all of which can influence implant revision and mortality rates. Although information relating to other risk factors such as obesity and smoking might not be specified in the register, this information is indirectly captured through the ASA grading system, which takes these into account.21 With excellent compliance in data entry and linking of procedures to the hospital episode statistics database in England and its equivalent in Wales (PEDW), the National Joint Registry constitutes a powerful evidence base to inform the decision making of clinicians, healthcare providers, patients, and implant manufacturers.
The registry is already being used to make recommendations for the choice of procedure on the basis of implant survival alone. That is, just analyses examining the time from primary surgery until a revision hip replacement. In contrast, comparison of mortality rates has received little attention. In its 2011 annual report,19 the registry provided unadjusted and adjusted results comparing revision rates for prosthesis type and bearing surface. Only unadjusted comparisons of mortality rates were provided, and adjusted analyses to control for differences in baseline characteristics were not considered. In relation to unadjusted death rates, they state that “the highest death rates were among the cemented group and the lowest were among the resurfacing group, reflecting the age distribution of these groups.” This statement, however, does not recognise that there might be a genuine difference in mortality rates between groups, even after adjustment for age. Furthermore, the report does not calculate absolute differences (such as in percentage revised at particular times) between groups but rather presents results separately for each group. It also says that “overlapping 95% confidence intervals mean that differences are not statistically significant”; this is not correct, as significant differences between groups can still occur even when confidence intervals for each group overlap.22 Thus it is clear that the report is an incomplete summary of the current evidence.
Results from the National Joint Registry suggest significant differences in implant survival between cemented and uncemented total hip replacement and hip resurfacing, leading the registry to conclude that “resurfacing has a higher revision rate than stemmed total hip replacement regardless of brand.”19 They also recommend that in patients aged over 70, cemented total hip replacements have the best revision rates and, being the cheapest available option, these should be the preferred choice unless good clinical reasons indicate otherwise. The current NICE guidelines on total hip replacement also recommend that cemented prostheses have better long term viability and state that there are no data to support the use of generally more costly uncemented and hybrid prostheses for primary total hip replacement.23 Neither NICE nor the National Joint Registry offer quantified advice on the relative safety in terms of mortality rates with these different classes of device.
We examined this issue using the National Joint Registry’s database to examine mortality and revision rates among patients with osteoarthritis undergoing hip arthroplasty and to compare these rates for the cemented, uncemented, and hip resurfacing procedures. Furthermore, as current mortality comparisons from the registry are based primarily on unadjusted results, we produced adjusted results (including differences in absolute survival probabilities) to allow a fairer comparison after accounting for available potential confounding factors.
Methods
Primary and secondary objectives
Our primary objective was to determine whether there are any differences in the mortality and revision rates over time between patients with osteoarthritis undergoing cemented and uncemented hip replacement surgery. Secondary objectives were to compare mortality and revision rates for cemented and uncemented procedures in each ASA grade separately and to compare mortality rates and revision rates for cemented and uncemented procedures and Birmingham hip resurfacing in all men (as this is used predominately in men alone, as explained above) and then in men aged under 55 (the group at highest risk of implant failure with conventional arthroplasty).14
Obtaining data and exclusions
In August 2011, the National Joint Registry provided us up to date raw patient level data without prior condition or prejudice. This information included linkage of the National Joint Registry dataset to the hospital episode statistics dataset (PEDW in Wales) providing further information on time of any subsequent revision and time of subsequent death if it occurred. Out of 423 287 hip arthroplasty procedures in the dataset, we removed records of 14 281 hips for which the primary procedure was not identified and 37 309 patients with a diagnosis other than primary osteoarthritis. We also excluded records of all patients who received a “hybrid” hip replacement as these use a variable combination of cemented and uncemented fixation methods.
In its 2011 annual report the National Joint Registry showed that the results of metal-on-metal total hip replacements are highly design specific and that failure rates of some brands, such as the ASR XL, are unacceptably high.19 The results of these poorly performing designs, however, continue to contaminate the data and the results on the registry. In view of this, the report19 recommends the separation of metal-on-metal total hip replacements from the remaining total hip replacements and the analysis of them as a different class to the cemented and uncemented groups. In keeping with that, we considered it appropriate to exclude all 13 833 large diameter metal-on-metal procedures.
The National Joint Registry data19 and the Australian Register24 show that the results of resurfacing are highly implant specific. Birmingham hip resurfacing predominates in worldwide use and is the only device with 10 year registry follow-up24 and a 10A UK ODEP (Orthopaedic Data Evaluation Panel) rating).25 As our secondary analyses were to just compare Birmingham hip resurfacing with cemented and uncemented total hip replacements, we excluded all non-Birmingham hip resurfacings.
The dataset obtained from the National Joint Registry contained duplicate entries for patients who underwent hip replacement/resurfacing of both hips on the same date. We removed the duplicate entry for these patients and created a “both sides” variable to identify these patients from those who underwent a single hip operation. We entirely excluded any patient who had both hips replaced on the same date but underwent a different procedure on each side.
We excluded 11 patients with missing data for age, sex, or ASA grade. As these represented a tiny proportion of the total number of patients, more sophisticated methods (such as multiple imputation) for dealing with missing data were considered unnecessary. This left a final total of 283 365 patients available for analysis (154 996 receiving cemented total hip replacements, 120 017 receiving uncemented total hip replacements, and 8352 receiving Birmingham hip resurfacing).
Summarising baseline data
We summarised baseline characteristics of patients and follow-up information (such as number censored and number of deaths) for the dataset as a whole as well as by type of procedure. We reported mean, standard deviation, median, interquartile range, and the minimum and maximum values for continuous variables, and total numbers and proportions for categorical variables.
Statistical analysis
Primary objectives
For each patient in the dataset, their date of primary surgery and their length of follow-up or time to end date (revision or death) were available. As each of our two outcomes of interest were time to event (that is, time to mortality and time to revision), we used survival analysis methods to compare the cemented and uncemented types of arthroplasty with potential adjustment for five other variables (covariates) available in the database: sex, age at primary surgery (in years), ASA grade before the operation (1-5), complexity of procedure (either “primary” or “complex primary”), and “both sides” replaced (either yes or no).
Separate survival models were fitted for time to death and time to revision. When analysing time to death, we censored those patients alive or revised at the end of their follow-up; follow-up information after revision was not available in the database. Thus our inferences about, and comparisons of, mortality rates at any time relate to patients without a revision before that time. Similarly, when analysing time to revision we censored those patients alive without revision or dead at the end of their follow-up. Thus our inferences about, and comparisons of, revision rates at any time relate to patients who are not already dead at that time.
We used the Royston-Parmar method for our survival modelling26 to obtain both unadjusted and adjusted results for each covariate, with the “stpm2” command within the Stata statistical software package.27 28 These models are flexible parametric models that have advantages over Cox regression29 as the baseline cumulative hazard function is explicitly modelled with restricted cubic splines. This allows hazard ratios to be calculated, as the Cox model does, but additionally enables absolute effects to be estimated (such as mortality rate per 1000 person years at time t and probability of survival at time t). The hazard ratios estimated with this approach were similar to those obtained through fitting a Cox regression model. We assumed that the hazard ratio was a constant over time for each variable as there was no indication to the contrary when we checked “log-log” plots (in which log(−log(S(t)) is plotted against time, where S(t) is the probability of not having the event up until at least time t).
When modelling the baseline hazard in each Royston-Parmar model, we tested different numbers of knots (which control the number of different splines being used and where they connect) and five knots were sufficient for the data. The multivariable (adjusted) model was fitted with a backward stepwise selection approach, which included type of procedure by default and any other variables that were significant (as conservatively defined by P<0.1). Age was included as a continuous variable and modelled linearly.
Using the estimates from the multivariable model, we plotted adjusted survival curves by predicting the population averaged survival curve for each procedure. Essentially, a predicted survival curve was obtained for each person in the database and all the survival curves were averaged. Unlike Kaplan-Meier curves, which are unadjusted, these survival curves allow a fairer comparison of survival probabilities across procedures after adjustment for other potential confounding covariates. We thus used them to calculate and graphically display the difference in the predicted population averaged survival probabilities during the whole follow-up period. At any time point, the difference in these survival probabilities can be used to calculate the number needed (n) to change procedures to save one event (n=1/difference in survival probability). In the results presented below we calculate n at six or eight years for illustration, as these times are toward the end of the follow-up period.
Secondary objectives
To assess differences between surgery procedures in each ASA grade separately, we refitted the multivariable Royston-Parmar model (excluding ASA grade) for each of the grades separately, and estimated the differences between cemented and uncemented groups for each.
In the examination of Birmingham hip resurfacing compared with cemented and uncemented procedures, we included only men and thus refitted the multivariable model excluding the sex covariate, but with no adjustment required for sex, and an adjusted survival curve estimated for each of the three surgery procedures. This was then repeated for just men aged under 55.
Results
In the dataset, between April 2003 and July 2011 a total of 154 996 patients received cemented hip replacement surgery and 120 017 patients received uncemented hip replacement surgery. The median follow up time was 3.6 years in the cemented group (range 0.001-9.7 years) and 2.6 years in the uncemented group (0.001-8.6 years). During follow-up, 11 745 (7.6%) patients died and 1589 (1.0%) had a revision in the cemented group compared with 3728 (3.1%) and 1917 (1.6%), respectively, in the uncemented group.
Table 1 shows that baseline characteristics were not balanced between the cemented and uncemented groups. In the cemented group people were on average almost 7 years older. In the uncemented group there was a higher proportion of men (42.1% v 34.5%), a higher proportion with ASA grade 1 (20.2% v 14.4%), and a lower proportion were considered as complex (0.7% v 8.5%).
Table 1.
Summary of baseline characteristics and follow-up data by procedure type in patients undergoing cemented or uncemented hip arthroplasty. Figures are numbers (percentage) unless stated otherwise
| Cemented (n=154 996) | Uncemented (n=120 017) | Overall (n=275 013) | |
|---|---|---|---|
| Baseline characteristics | |||
| Age (years): | |||
| Mean (SD) | 73.2 (8.7) | 66.7 (10.1) | 70.4 (9.9) |
| Median | 73.8 | 67.0 | 71.2 |
| Interquartile range | 68.0-79.2 | 60.5-73.7 | 64.2-77.3 |
| Range | 15.9-103.4 | 15.4-106.2 | 15.4-106.2 |
| Sex: | |||
| Men | 53 409 (34.5) | 50 529 (42.1) | 103 938 (37.8) |
| Women | 101 587 (65.5) | 69 488 (57.9) | 171 075 (62.2) |
| ASA (American Society of Anesthesiologists) grade: | |||
| 1 | 22 336 (14.4) | 24 276 (20.2) | 46 612 (17.0) |
| 2 | 107 395 (69.3) | 82 104 (68.4) | 189 499 (68.9) |
| 3 | 24 369 (15.7) | 13 151 (11.0) | 37 520 (13.6) |
| 4 | 852 (0.6) | 456 (0.4) | 1308 (0.5) |
| 5 | 44 (0.03) | 30 (0.02) | 74 (0.03) |
| Surgery | |||
| Approach: | |||
| Anterior | 485 (0.3) | 429 (0.4) | 914 (0.4) |
| Anterolateral | 12 223 (8.6) | 7161 (6.1) | 19 384 (7.5) |
| Hardinge | 34 366 (24.1) | 28 834 (24.7) | 63 200 (24.3) |
| Lateral (incl Hardinge) | 30 137 (21.1) | 14 321 (12.3) | 44 458 (17.1) |
| Posterior | 59 855 (41.9) | 61 086 (52.3) | 120 941 (46.6) |
| Trochanteric osteotomy | 1164 (0.8) | 96 (0.1) | 1260 (0.5) |
| Other | 4620 (3.2) | 4989 (4.3) | 9609 (3.7) |
| Missing | 12 146 (7.8) | 3101 (2.6) | 15 247 (5.5) |
| Complexity of procedure: | |||
| Primary | 141 825 (91.5) | 119 172 (99.3) | 260 997 (94.9) |
| Complex primary | 13 171 (8.5) | 845 (0.7) | 14 016 (5.1) |
| Both sides: | |||
| No | 154 798 (99.9) | 119 497 (99.6) | 274 295 (99.7) |
| Yes | 198 (0.1) | 520 (0.4) | 718 (0.3) |
| Follow-up | |||
| Endpoint: | |||
| Death | 11 745 (7.6) | 3728 (3.1) | 15 473 (5.6) |
| Revision | 1589 (1.0) | 1917 (1.6) | 3506 (1.3) |
| Unrevised | 141 662 (91.4) | 114 372 (95.3) | 256 034 (93.1) |
| Total length of follow-up, person years | 535 035 | 323 477 | 858 512 |
Primary analyses
Mortality
The Royston-Parmar model for mortality as the endpoint, with procedure type as the only variable, gave an unadjusted hazard ratio of 1.83 (95% confidence interval 1.76 to 1.90), suggesting a higher mortality rate for cemented than uncemented procedures. Because of the imbalance in baseline characteristics between the groups, however, such unadjusted results are subject to potential confounding.
Multivariable analysis showed that procedure type, age, sex, ASA grade, and complexity of procedure were all significant and were thus included in the final model. The “both sides” variable, however, was not important. The adjusted hazard ratio estimates from the model are smaller than the unadjusted results, but still suggest that the mortality rate is 1.11 (1.07 to 1.16) times higher in the cemented group than in the uncemented group (table 2). This significant comparison relates to any time point and to patients without a revision before that time. For the other variables, the results suggest the mortality rate increases with increasing age, generally increases as ASA grade increases, is higher for men than women, and is higher for those considered a “complex primary” procedure.
Table 2.
Adjusted hazard ratios from multivariable analysis with mortality as endpoint in patients undergoing total hip replacement
| Variable | Hazard ratio (95% CI) | P value |
|---|---|---|
| Surgery: | ||
| Uncemented | — | — |
| Cemented | 1.11 (1.07 to 1.16) | <0.001 |
| Age (years) | 1.09 (1.09 to 1.09) | <0.001 |
| ASA (American Society of Anesthesiologists) grade: | ||
| 1 | — | — |
| 2 | 1.19 (1.13 to 1.26) | <0.001 |
| 3 | 2.15 (2.03 to 2.28) | <0.001 |
| 4 | 3.52 (3.09 to 4.00) | <0.001 |
| 5 | 2.94 (1.70 to 5.07) | <0.001 |
| Sex: | ||
| Women | — | — |
| Men | 1.54 (1.49 to 1.59) | <0.001 |
| Complexity: | ||
| Primary | — | — |
| Complex primary | 1.40 (1.33 to 1.46) | <0.001 |
Figure 1 shows the predicted population averaged survival curves for cemented and uncemented procedures, with adjustment for differences in age, sex, ASA grade, and complexity. This shows a significant but small difference in the probability of survival between the cemented and uncemented groups. For example, at eight years after surgery the probability of being alive was 0.013 higher (0.007 to 0.019) in the uncemented group than in the cemented group for patients with no revision before this time. At earlier times, the difference is even smaller. This suggests that, in a hypothetical scenario in which no patients undergo a revision by eight years, 77 patients (53 to 143) need to be treated with an uncemented rather than cemented procedure to result in one less death by eight years.

Fig 1 Population averaged (adjusted) survival curves (with 95% confidence intervals shown by dashed lines) for cemented versus uncemented with mortality or revision as endpoint
Revision
For revision as the endpoint, the unadjusted hazard ratio was 0.53 (0.50 to 0.57), suggesting a lower revision rate for cemented than uncemented. Multivariable analysis showed that procedure type, age, sex, and ASA grade were all significant and were thus included in the final model, but not complexity of procedure or the “both sides” variable. The adjusted hazard ratio estimates from the model suggest that, at any time point, the revision rate is 0.58 (0.54 to 0.62) times lower in the cemented group than in the uncemented group (table 3); this is similar to the unadjusted result.
Table 3.
Adjusted hazard ratios from multivariable analysis with revision as endpoint in patients undergoing total hip replacement
| Variable | Hazard ratio (95% CI) | P value |
|---|---|---|
| Surgery: | ||
| Uncemented | — | — |
| Cemented | 0.58 (0.54 to 0.62) | <0.001 |
| Age (years) | 0.99 (0.98 to 0.99) | <0.001 |
| ASA (American Society of Anesthesiologists) grade: | ||
| 1 | — | — |
| 2 | 1.09 (1.00 to 1.19) | 0.064 |
| 3 | 1.38 (1.22 to 1.55) | <0.001 |
| 4 | 0.60 (0.30 to 1.20) | 0.151 |
| 5* | — | — |
| Sex: | ||
| Female | — | — |
| Male | 1.15 (1.08 to 1.23) | <0.001 |
*Not estimable because there were too few patients and events in this group
As for mortality, the impact of this hazard ratio can be translated to the absolute probability scale by considering the adjusted survival curve (fig 1), which shows the probability of not having a revision for each procedure group over time for patients who had not died previously. At any time, the curve shows only small differences in this probability between groups—for example, at eight years the probability of a revision is increased by only 0.015 (0.012 to 0.017) in the uncemented group. This suggests that, in a hypothetical scenario in which no patients have died by eight years, 67 patients (58 to 84) need to be treated with a cemented rather than uncemented procedure to result in one less revision by eight years.
Secondary analyses
Mortality and revision rates for each ASA grade separately
We examined mortality rates separately for each ASA grade, with adjustment made for age, sex, and complexity of procedure. There were too few patients in ASA grade 5 for the model to be fitted in this subgroup. The adjusted hazard ratio comparing cemented and uncemented procedures was significant for ASA grade 2 (hazard ratio 1.15, 1.10 to 1.21) and ASA grade 4 patients (1.37, 1.03 to 1.83), indicating the cemented procedure is associated with an increased mortality rate. There was no significant effect for grade 1 (0.99, 0.88 to 1.11) or grade 3 (1.04, 0.96 to 1.12) patients.
Revision rates were adjusted for age and sex but not for complexity of procedure as it was not significant. There was a significant difference in revision rates between cemented and uncemented procedures in grade 1 (hazard ratio 0.61, 0.51 to 0.72), grade 2 (0.60, 0.55 to 0.66), and grade 3 (0.46, 0.38 to 0.55), suggesting a lower hazard of revision for patients who received the cemented procedure compared with the uncemented procedure. Models could not be fitted for ASA grade 4 or 5 because of the small patient numbers in these subgroups.
Birmingham hip resurfacing in all men
We compared mortality and revision rates in all men for cemented, uncemented, and Birmingham hip resurfacing procedures. There were again baseline differences between groups: the men undergoing Birmingham hip resurfacing men were younger and a higher proportion were ASA grade 1 (47.9%) and ASA grade 2 (48.9%) (table 4). Multivariable analysis including the significant variables of age, ASA grade, and complexity of procedure, estimated that the hazard of death was 1.64 (1.33 to 2.02) times higher for the cemented group and 1.47 (1.19 to 1.82) times higher for the uncemented group when compared with Birmingham hip resurfacing (table 5). The population averaged survival curve shows that the highest probability of survival is seen for the Birmingham hip resurfacing group, with 92.1% (90.6% to 93.6%) predicted to be alive at six years, conditional on patients not undergoing revision before this time (fig 2). At six years, the probability of survival for patients who have not undergone revision is 0.044 (0.029 to 0.060) higher in those undergoing Birmingham hip resurfacing rather than cemented procedures. This suggests that, in a hypothetical scenario in which no patients undergo revision by six years, 23 men (17 to 35) need to be treated with Birmingham hip resurfacing rather than a cemented procedure to result in one less death by six years.
Table 4.
Summary of baseline characteristics and follow-up information by procedure type in men undergoing hip arthroplasty, including Birmingham hip resurfacing. Figures are numbers (percentage) unless stated otherwise
| Birmingham hip resurfacing (n=8352) | Uncemented (n=50 529) | Cemented (n=53 409) | |
|---|---|---|---|
| Baseline characteristics | |||
| Age (years): | |||
| Mean (SD) | 55.9 (8.6) | 66.2 (9.9) | 72.3 (8.6) |
| Median | 56.6 | 66.7 | 72.9 |
| Interquartile range | 50.4-61.9 | 60.3-73.1 | 67.2-8.1 |
| Range | 19.0-85.0 | 17.1-98.8 | 18.1-101.7 |
| ASA (American Society of Anesthesiologists) grade: | |||
| 1 | 3999 (47.9) | 10 761 (21.3) | 8246 (15.4) |
| 2 | 4087 (48.9) | 33 594 (66.5) | 35 838 (67.1) |
| 3 | 256 (3.1) | 5918 (11.7) | 8947 (16.8) |
| 4 | 8 (0.1) | 246 (0.5) | 360 (0. 7) |
| 5 | 2 (0.02) | 10 (0.02) | 18 (0.03) |
| Procedure type: | |||
| Primary | 8262 (98.9) | 50 176 (99.3) | 48 743 (91.3) |
| Complex primary | 90 (1.1) | 353 (0.7) | 4666 (8.7) |
| Both sides: | |||
| No | 8297 (99.3) | 50 304 (99.6) | 53 319 (99.8) |
| Yes | 55 (0.7) | 225 (0.5) | 90 (0.2) |
| Follow-up | |||
| Endpoint: | |||
| Death | 93 (1.1) | 1872 (3.7) | 4821 (9.0) |
| Revision | 159 (1.9) | 830 (1.6) | 645 (1.2) |
| Unrevised | 8100 (97.0) | 47 827 (94.7) | 47 943 (89.8) |
| Total length of follow-up, person years | 27 961 | 134 702 | 183 101 |
Table 5.
Adjusted hazard ratios from multivariable analysis of men undergoing hip arthroplasty, including those undergoing Birmingham hip resurfacing, with mortality as endpoint
| Variable | Hazard ratio (95% CI) | P value |
|---|---|---|
| Surgery: | ||
| Birmingham hip resurfacing | — | — |
| Cemented | 1.64 (1.33 to 2.02) | <0.001 |
| Uncemented | 1.47 (1.19 to 1.82) | <0.001 |
| Age (years) | 1.09 (1.09 to 1.09) | <0.001 |
| ASA (American Society of Anesthesiologists) grade: | ||
| 1 | — | — |
| 2 | 1.17 (1.09 to 1.26) | <0.001 |
| 3 | 2.14 (1.97 to 2.33) | <0.001 |
| 4 | 3.58 (2.98 to 4.30) | <0.001 |
| 5 | 0.54 (0.08 to 3.80) | 0.532 |
| Complexity: | ||
| Primary | — | — |
| Complex primary | 1.31 (1.22 to 1.41) | <0.001 |

Fig 2 Population averaged (adjusted) survival curves (with 95% confidence intervals shown by dashed lines) for men comparing cemented, uncemented, and Birmingham hip resurfacing patients, with mortality or revision as endpoint
For revision, the cemented group performs best with a hazard ratio of 0.65 (0.54 to 0.79) compared with Birmingham hip resurfacing. There was no significant difference between Birmingham hip resurfacing and uncemented procedures, with a hazard ratio of 1.04 (0.87 to 1.25; P=0.657) (table 6). The adjusted survival curve for revision (fig 2) shows that the men in the cemented group have the highest probability of no revision over time. At all times, however, the absolute differences in the predicted population averaged probability of revision are small between all groups.
Table 6.
Adjusted hazard ratios from multivariable analysis of men undergoing hip arthroplasty, including those undergoing Birmingham hip resurfacing, with revision as endpoint
| Hazard ratio (95% CI) | P value | |
|---|---|---|
| Surgery: | ||
| Birmingham hip resurfacing | — | — |
| Cemented | 0.65 (0.54 to 0.79) | <0.001 |
| Uncemented | 1.04 (0.87 to 1.25) | 0.657 |
| Age (years) | 1.00 (0.99 to 1.00) | 0.091 |
| ASA (American Society of Anesthesiologists) grade: | ||
| 1 | — | — |
| 2 | 1.10 (0.97 to 1.24) | 0.153 |
| 3 | 1.24 (1.04 to 1.48) | 0.015 |
| 4 | 0.54 (0.20 to 1.45) | 0.220 |
| 5* | — | — |
*Not estimable because too few patients and events in this group
Birmingham hip resurfacing in men aged under 55
In men under the age of 55 only, there were still baseline differences between groups (table 7). The adjusted survival curve shows (fig 3) that the differences in patient mortality between those undergoing Birmingham hip resurfacing and cemented and uncemented total hip replacement remain, with significantly higher predicted population averaged survival in the Birmingham hip resurfacing group. For patients who have not undergone revision at six years, the predicted probability of being alive in the Birmingham hip resurfacing group is 0.018 higher (0.008 to 0.029) than in the cemented group and 0.013 higher (0.006 to 0.020) than in the uncemented group. There were no significant differences between the groups for revision rates (fig 3), although this could reflect a low power.
Table 7.
Summary of baseline characteristics and follow-up information by procedure type in men aged under 55. Figures are numbers (percentage) unless stated otherwise
| Birmingham hip resurfacing (n=3560) | Uncemented (n=6193) | Cemented (n=1730) | |
|---|---|---|---|
| Baseline characteristics | |||
| Age (years): | |||
| Mean (SD) | 47.9 (5.5) | 48.5 (6.1) | 49.1 (5.9) |
| Median | 49.2 | 50.3 | 51.0 |
| Interquartile range | 44.7-52.3 | 45.8-53.0 | 46.7-53.4 |
| Range | 19.0-55.0 | 17.1-55.0 | 18.10-55.0 |
| ASA (American Society of Anesthesiologists) grade: | |||
| 1 | 2077 (58.3) | 2595 (41.9) | 692 (40.0) |
| 2 | 1421 (39.9) | 3225 (52.1) | 925 (53.5) |
| 3 | 59 (1.7) | 360 (5.8) | 108 (6.2) |
| 4 | 2 (0.1) | 12 (0.2) | 4 (0.2) |
| 5 | 1 (0.03) | 1 (0.02) | 1 (0.1) |
| Procedure type: | |||
| Primary | 3511 (98.6) | 6119 (98.8) | 1525 (88.2) |
| Complex primary | 49 (1.4) | 74 (1.2) | 205 (11.9) |
| Both sides: | |||
| No | 3531 (99.2) | 6143 (99.2) | 1716 (99.2) |
| Yes | 29 (0.8) | 50 (0.8) | 14 (0.2) |
| Follow-up | |||
| Endpoint: | |||
| Death | 10 (0.3) | 56 (0.9) | 32 (1.9) |
| Revision | 60 (1.7) | 107 (1.7) | 28 (1.6) |
| Unrevised | 3490 (98.0) | 6030 (97.4) | 1670 (96.5) |
| Total length of follow-up, person years | 11 637 | 15 886 | 5991 |

Fig 3 Population averaged (adjusted) survival curves for men aged under 55 comparing cemented, uncemented, and Birmingham hip resurfacing patients, with mortality or revision as endpoint
Discussion
In addition to well known differences in revision rates, our multivariable analyses showed significant differences in mortality rates after different surgical procedures for hip replacement. The lowest mortality rate was in men with Birmingham hip resurfacing, followed by all patients with uncemented total hip replacement, and with the highest rate in all patients with cemented total hip replacement. The primary endpoint of most arthroplasty registers originally was implant survival. Effective linkage to other health related registers, such as the National Joint Registry linkage to hospital episode statistics (and the Welsh equivalent), now promises to widen their scope to other endpoints. The database of over 400 000 entries for primary hip surgery in the registry offers a unique opportunity to compare implant survival and mortality rates between cemented and uncemented total hip replacement and also to compare these procedures with Birmingham hip resurfacing in men.
The strengths of our study are the large number of patients and events in the National Joint Registry database linked to mortality records from the hospital episode statistics (and the Welsh equivalent) datasets; the ability to adjust for five potential confounding factors (age, sex, complexity, ASA grade, bilaterality); and the advanced statistical methods that allowed us to calculate both relative effects (hazard ratios) and differences in absolute survival probabilities, so that we could produce adjusted (population averaged) survival curves.30
Based on comparisons of revision rates alone, the cemented procedure is currently recommended. It is clear, however, that with comparisons of unadjusted mortality rate, one should actually recommend the uncemented procedure. The baseline differences between cemented and uncemented groups clearly show there is a selection mechanism being used to allocate individuals to a particular procedure. For this reason, unadjusted comparisons are not reasonable and should be abandoned.
Our study is an attempt to redress the balance with appropriate adjustment for all the known confounding factors in the National Joint Registry data and simultaneous estimation of differences in implant survival and patient survival in the different classes of devices. We used the flexible parametric method, which gives the same results as a Cox regression but adjusts for confounding factors and additionally models the underlying hazard of an event over time.
Key results
Differences in mortality rate between cemented and uncemented total hip replacement
In keeping with previous studies we excluded diagnoses other than osteoarthritis,31 hybrid and reverse hybrid fixed total hip replacement,32 and metal-on-metal total hip replacement19 to clearly delineate the differences between cemented and uncemented hip replacement. Unadjusted figures from the National Joint Registry19 show estimated mortality rates of 0.4% and 0.2% at 30 days, 0.8% and 0.5% at 90 days, and 21.8% and 12.3% at eight years in cemented and uncemented procedures, respectively. These figures compare well with Medicare information relating to 61 568 primary total hip replacements, which showed a 90 day mortality rate of 0.97%,33 and a review of 7478 uncemented total hip replacements from a specialist centre, which reported overall 30 and 90 day mortality rates of 0.2% and 0.6%, respectively.34
A report based on the Australian and Norwegian registers35 with 106 254 total hip replacements shows that there is an increase in mortality in the first 26 postoperative days of 0.1% compared with the baseline. The Danish register showed that the 30 day mortality after a total hip replacement was higher than matched controls and the 90 day mortality was lower.36 Studies from Norwegian and Finnish registers showed that compared with the general population, total hip replacement was associated with a higher mortality during the first 60 days and a lower mortality during the subsequent 10 years.37 38 Another Finnish study39 extending to 30 years confirmed the reduced mortality in patients with total hip replacement in the first decade, equalling the general population in the second decade, and higher mortality than the general population during the third.39 The numbers in this study were relatively low compared with those in the National Joint Registry.
The above reports do not show a direct comparison of mortality rates between cemented and uncemented total hip replacement, except the Norwegian study, which showed a lower mortality (relative mortality rate ratio of 0.84) in patients with an uncemented total hip replacement compared with cemented procedure with high viscosity cement.37 In our large cohorts of patients we found a significant difference in mortality between cemented and uncemented total hip replacement after adjustment for diagnosis, age, sex, complexity, and fitness based on ASA grade. The unadjusted mortality rate ratio for cemented compared with uncemented procedures is 1.83 (1.76 to 1.90). After adjustment for the above variables the ratio is 1.11 (1.07 to 1.16), which is also significant (P<0.001). In a hypothetical scenario in which no patients undergo revision by eight years, the adjusted model results predict that 77 patients (53 to 143) need to be treated with an uncemented rather than a cemented procedure to attain one less death by eight years.
Implant survival differences between cemented and uncemented total hip replacement
Most national arthroplasty registers, including the National Joint Registry, show a benefit for implant survival with cemented compared with uncemented total hip replacement. A recent systematic review of registers showed that 10 year implant survival of cemented total hip replacements ranges from 88% in Finland to 95% in Norway,40 which is superior to the 10 year survival of uncemented procedures, ranging from 80% in Finland to 85% in Sweden. The unadjusted and adjusted hazard ratios for implant survival in the present study for cemented procedures compared with uncemented procedures are estimated as 0.53 and 0.57, respectively, and are both significant. When translated to the absolute probability scale the differences are small. The predicted population averaged probability of revision is estimated to increase by 0.015 in the uncemented group, which—in a scenario in which there are no deaths—suggests that 67 hips (58 to 84) need to be treated with cemented rather than uncemented total hip replacement to reduce one revision over eight years.
Implant survival and mortality rate differences in men
In a systematic review Santaguida et al showed that after total joint arthroplasty, being male is associated with increased risk of both implant revision and mortality.41 Younger men have an increased risk of revision, while older men have an increased risk of mortality. In short, younger men wear their hips out prematurely and older men die early after hip replacement compared with women.
Our analysis of the National Joint Registry data shows that, among men of all ages without a revision by six years, the unadjusted figures for six year patient survival and implant survival are 85% and 98% in cemented procedures, 91% and 97% in uncemented procedures, and 98% and 97% in Birmingham hip resurfacings, respectively. After adjustment for all known risk factors, patient survival with Birmingham hip resurfacing continues to be superior to survival in those with uncemented total hip replacement, which in turn is superior to those with cemented total hip replacement. Adjusted analyses also indicate that implant survival in cemented total hip replacement continues to be superior to uncemented total hip replacement and Birmingham hip resurfacing. There is no statistical evidence at any time point of a difference in implant survival between uncemented total hip replacement and Birmingham hip resurfacing.
Several national registers show that the risk of implant revision is highest in young patients (variably defined in different studies, under 60 in the Norwegian registry and under 55 in the Finnish and Swedish registries), especially in young men in whom it is increased threefold to fivefold.41 The 10 year Kaplan-Meier survival ranged from 72% in Finland to 86% in Sweden in younger patients (under 55) compared with 90% and 97% in older patients (55 and above) in the same countries.40 A Finnish register based study showed that survival of uncemented stems is superior to that of cemented stems in patients aged under 55, with aseptic loosening as the endpoint.42 The Swedish hip arthroplasty register reported 10 year survival of 66%, 67%, and 64% with cemented, uncemented, and hybrid total hip replacement, respectively, in young men with osteoarthritis43 and therefore considered young patients with hip arthritis to be the “supreme challenge” for hip replacement.44 The Birmingham hip resurfacing procedure was developed for this particular cohort of young patients with osteoarthritis.45 Our results show that at the six year stage there is no significant difference in adjusted implant survival between the three classes of device, though this could be because of low power, but the adjusted mortality rate shows that Birmingham hip resurfacing outperforms cemented and uncemented total hip replacement.
Two recent studies (postdating the original submission of this article) have also used flexible parametric survival analysis to interpret data from National Joint Registry. Smith et al highlighted higher failure rates with stemmed metal-on-metal hip replacements—that is, not resurfacings.46 We specifically excluded this metal-on-metal group from our study. The same investigators also assessed the risk of cancer in patients receiving metal-on-metal stemmed hips, metal-on-metal resurfacings, and other bearing stemmed total hips.47 They concluded “...our models indicated that patients undergoing resurfacing procedures were less likely than those with alternative bearings to get a diagnosis of prostate cancer, haematological cancers, or any cancer and had a lower risk of death.” This work supports the findings of our more detailed analysis suggesting lower adjusted mortality rates in patients undergoing resurfacing.
Limitations
There are limitations to our study. One of these is the potential for unknown confounders that were not recorded in the database. Registries by nature contain observational data with a potential for bias at different levels. Adjustment for known confounding factors was obtained with a flexible parametric survival analysis including potential confounders as covariates. An alternative approach to adjustment is to use propensity scores (for example, where the propensity to be given cemented or uncemented is first modelled and then each patient’s propensity score is included as an adjustment covariate), but this is not necessarily better at reducing confounding than our more standard approach.48 Compared with unadjusted analyses, our adjusted analyses reduced the estimated differences between groups both in terms of mortality and implant survival but the potential for other residual confounders cannot be ruled out. We included the complexity covariate (defined as “primary” or “complex primary” in the database) as an adjustment factor in our analyses of mortality as it was significant. Indeed, it is possible that this covariate is associated with another factor we have been unable to adjust for.
Although the terms primary and complex primary were introduced in the National Joint Registry forms in 2005, there has never been a clear definition of these terms. It seems they had not been included in the earlier version (2003) and have subsequently been removed from the version currently used. If the covariate had a significant effect on revision rates it could have validated itself, but in our analysis it did not have a significant association with revision rates (though it did have a significant association with mortality rates). There is therefore potential debate as to how it will have been routinely recorded across different hospitals. The National Joint Registry itself has not used it in their flexible parametric analysis. As complexity was recorded for all patients in the database and given that it was clearly imbalanced between groups, we considered it important to adjust for it when necessary (for instance, in the mortality rate analyses). If complexity is removed from the model, the hazard ratio for mortality between cemented and uncemented total hip replacement increases further from 1.11 (1.07 to 1.16) to 1.17 (1.13 to 1.22).
Secondly, although implant revision is a clearly definable endpoint, it is not an exclusive surrogate marker of a failing implant. A loose cemented hip in an elderly patient in poor health is likely to be treated non-operatively either because the patient is too ill to undergo revision surgery or simply prefers to put up with the pain and limitation of function rather than risk another major operation. It is more common to perform revision surgery when needed for younger patients.42 The former will be treated as a success and the latter a failure. Unrealistic expectations in patients and ease of revision place different thresholds for revision in different classes of implants.49 Therefore the place of revision focused survival analysis is being challenged in orthopaedic literature.50 Outcome measures51 and other markers of implant function need to be introduced.52
Thirdly, in the assessment of mortality, the cause of death was not available and thus could not be summarised. Furthermore, mortality data for patients having revisions are missing in the National Joint Registry database we were provided with. Thus our inferences about, and comparisons of, mortality rates at any time point are specific to patients without a revision before that time. We cannot therefore make any inferences about mortality rates in patients with a revision. Similarly, our analyses of revision rates censor patients who died without revision at their time of death. Thus our inferences about, and comparisons of, revision rates at any time point are specific to patients who have not died before that time. An alternative competing risks analysis could be used to examine revision rates with dead unrevised patients kept in the analysis (and thus not censored). This approach is taken by the National Joint Registry19 and others53 and will lead to lower estimates of revision rates than our analysis because they include people who have died, after which they clearly will not be revised. We will consider such analyses in further work, to make inferences about the predicted probability of revision at particular times for all patients, some of whom might have died previously. We have not done this here because the available data force us to present mortality rates conditional on being unrevised; so a direct contrast is to present revision rates conditional on not being dead.
Furthermore, ASA grade can be a poor yardstick of general health. None of the registers have a record of activity level. It could be argued that even after adjustment for ASA grade, there can be residual confounding, with the more active population being selected for uncemented rather than cemented total hip replacement. If increased activity level conferred longer life in the uncemented group, that same activity level could have also caused the higher failure rate in the uncemented group. When analysing the same effect in young men we find a paradox. If increased activity level confers a much higher life expectancy in the Birmingham hip resurfacing group, one would expect the higher activity to lead to an increased revision rate with Birmingham hip resurfacing compared with total hip replacement. The robust bearing with Birmingham hip resurfacing, the large head with low risk of dislocation, and the mechanically sound femoral reconstruction keeping the point of fixation coincident with the point of loading, unlike a stemmed total hip replacement, are some favourable design features.
The follow-up of eight years in the current National Joint Registry is also considered relatively short. Whether the differences in mortality between the groups decrease with time or whether they continue to diverge over a longer period remains to be seen. With respect to implant revision, published data in young patients show that while total hip replacement failures follow a sustained pace54 in the longer term, more failures with Birmingham hip resurfacing tend to occur in the early years from femoral neck fractures, etc.55 Our analysis shows that up to the six year stage, for men aged under 55 there is no significant difference in National Joint Registry revision rates between the three classes of device. Whether longer term results will show that this trend continues or whether significant differences develop later between the device classes, is not known. It is regrettable that although eight year results are currently available for total hip replacement on the National Joint Registry, the entries for Birmingham hip resurfacing extend only to six years even though such resurfacing has been performed in England and Wales for over 14 years.
Finally, an alternative approach to analysis could consider the time to either death or revision, whichever came sooner. A multivariable analysis for this composite outcome gives an adjusted hazard ratio that slightly favours the cemented procedure (0.94, 95% confidence interval 0.91 to 0.97). This approach, however, treats revision and death as equally unwelcome, which is highly debatable. Furthermore, there was evidence of non-proportional hazards in this analysis, indicating that the hazard ratio is not constant over time. For such reasons, and because death and revision are important clinical outcomes on their own, we focused on comparisons for death and revision separately in our investigations.
Epidemiological magnitude of the problem
The evidence in this analysis suggests there are differences between the outcomes of cemented and uncemented total hip replacements in terms of both revision and mortality rates. On average across the population, our model predicts that performing a cemented instead of an uncemented total hip replacement results in an extra death once in every 77 (95% confidence interval 53 to 143) procedures every eight years for patients who do not undergo revision before this time; conversely, the disadvantage of uncemented total hip replacement is that an extra revision is predicted within eight years for every 67 (58 to 84) procedures for patients alive at this time. Secondary analyses in men showed that the lowest death rate is associated with Birmingham hip resurfacing. By performing a cemented total hip replacement instead of resurfacing, our analysis predicts an extra death occurs within six years for every 23 (17 to 35) operations.
Although the hazard ratios and differences in survival probabilities for mortality between procedure types are small, a large number of people currently undergo hip arthroplasty and the number is increasing year on year. Therefore even small differences, if they are genuine, indicate potentially large numbers of avoidable deaths. For example, an estimated 1.2 million hip arthroplasties56 were performed worldwide in 2011 alone. If hypothetically 1.2 million planned cemented procedures were changed to uncemented procedures then, based on our model estimates, there would be a predicted 15 584 (8392 to 22 641) fewer deaths by eight years for patients who had not undergone revision by this time. As the baby-boomer generation ages the number of arthroplasties has been progressively increasing and therefore the number of potential avoidable deaths could also progressively increase if cemented hips continue to be used widely. If 40% of these 1.2 million are assumed to be men then, based on our estimates, switching 0.48 million cemented procedures to Birmingham hip resurfacing would lead to a predicted 20 869 fewer deaths (13 714 to 28 235) at six years for who had not undergone revision before this time.
This aspect of higher mortality with cemented total hip replacement has not been highlighted or investigated in detail in the past. The numbers of preventable deaths from cemented total hip replacement creates considerable public health interest. The small increased mortality is not restricted to the early postoperative period but continues to persist eight years after the operation. This is a cause for concern and a reason for further investigation. It is a priority to identify the reasons for the higher observed mortality in cemented total hip replacements. Recognising the fact that the consequences of death and revision are not in the same league, the real question that needs to be examined is to what extent is the observed higher death rate in cemented total hip replacement a result of selection bias (residual confounding) and to what extent it is a direct causal effect of the cement and cementing process?
The potential for residual confounding is strong, given the imbalances observed at baseline between groups, and the National Joint Registry should consider recording additional variables in the future to enable further adjustments for potential confounding. For example, although our adjustment for ASA grade will capture some of the comorbidities of individuals, it would be better if more detailed recording of existing diseases, conditions, and prognostic factors (such as smoking) were available to allow further more direct adjustment for confounding. Another suggestion that the difference in mortality might not be genuine is the lack of a significant hazard ratio within patients with ASA grades 1 and 3. Though there was a significant difference for grades 2 and 4, and most patients are grade 2, one would expect a true causal factor to impact on all types of patients but this was not observed. On the other hand, one cannot rule out that cement might be genuinely increasing the risk of death. If it is, then clearly it should be avoided as there must be an underlying causal mechanism. Several mechanisms might be suggested, though this of course is speculative.
Although polymethylmethacrylate (PMMA) bone cement is biocompatible, adverse cardiopulmonary effects57 58 59 60 61 62 have been widely documented during and after the cementation period. Modern cement techniques,63 including pressurisation, which were developed to improve cement penetration and fixation can exacerbate these events.64 During the reaming and pressurisation processes fat, marrow, air, particles of bone, cement, and aggregates of platelets and fibrin are driven into the systemic circulation57 with the potential for intraoperative and postoperative embolic events and adult respiratory distress syndrome. Embolic events have been found to correlate with haemodynamic changes suggesting pulmonary embolism65 and have been observed in over 90% of cases66 by transoesophageal echocardiography. Furthermore about 10% of normal patients have right to left shunt, giving the possibility of systemic embolisation with unknown long term effects.67 68 69 In comparison, the relative rarity of overt postoperative adult respiratory distress syndrome in patients suggests that the embolic insult is usually insufficient to cause important clinical symptoms immediately. The persistence of increased mortality over eight years, however, raises the question of whether the embolisation has the potential to reduce the normal respiratory reserve, making the patient prone to succumb to minor respiratory diseases in the longer term. A long term detrimental effect on other organ systems from systemic embolisation could also explain the continuing increased mortality.
We have had the opportunity of studying embolisation intraoperatively after cemented total hip replacement and Birmingham hip resurfacing using transoesophageal echocardiography.70 The embolisation of echogenic material into the right heart and lungs is markedly different with the two different procedures. With Birmingham hip resurfacing, there is momentary transient embolisation or no embolisation, whereas with cemented total hip replacement there is profound embolisation, which can persist for up to 20 minutes.
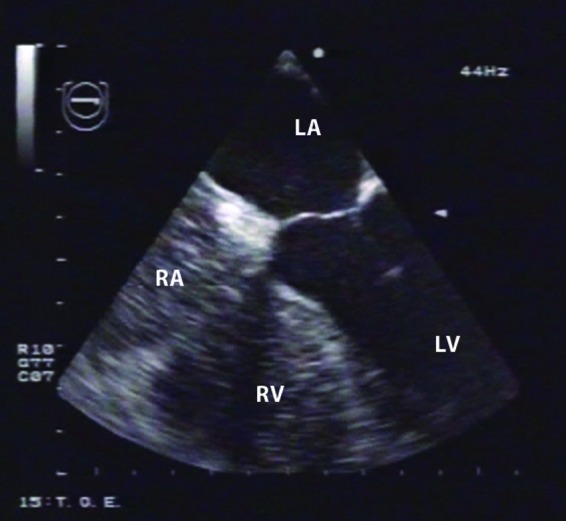
Fig 4 Transoesophageal echocardiogram in patient after cemented total hip replacement, showing fat and marrow echogenic material in right atrium and right ventricle. No echogenic material in left atrium or left ventricle, indicating that debris has been filtered in pulmonary vasculature
Furthermore, the potential long term detrimental effects from prolonged exposure to nephrotoxic agents such as gentamicin from the bone cement cannot be ruled out, and this matter is being actively investigated.
Direction of future research
Although much time and effort has been spent on research into potential concerns about cancer, chromosome changes, and metal ions with metal-on-metal bearings, it is ironic that the lowest death rate of any hip arthroplasty on the National Joint Registry is with metal-on-metal Birmingham hip resurfacing. The question of why cemented total hip replacement is associated with the highest death rate has not been adequately researched.
Death is the simplest of all outcomes to measure, is well documented and easily understood by the patient, and has profound implications for the patient and his or her family, but yet it is largely neglected by registries. Thus far, we have been comfortable to ignore it because patients with total hip replacement survive as long as or longer than non-operated controls, the differences between cemented and uncemented implants are small, any perceived differences have been explained away by different characteristics of patients at baseline, and the raw data have not previously been made available for analysis.
The registers should be congratulated on the collection of data but need to go further to make detailed recording of all relevant information to allow accurate analysis and conclusions. This must include measurement of the activity levels and any other potential confounding factors.
The evidence of lower risk of death after hip resurfacing independently arrived at by two research groups (our present study and Smith et al47) working on this large database should reassure patients with metal-on-metal resurfacing that this procedure is at least as safe and at best safer than total hip replacement in terms of overall mortality.
More work is necessary to determine whether the higher mortality rate after cemented total hip replacement is caused by the cementing procedure or if this is because of other as yet unknown confounding factors such as differences in activity level between the groups.
What is already known on this topic
Unadjusted and adjusted survival analyses suggest cemented total hip replacements are associated with better implant survival (improved revision rates) than uncemented total hip replacement and hip resurfacings.
NICE indicate there are no data to support the use of generally more costly uncemented total hip replacement, though adjusted comparisons of mortality rates have previously been lacking
What this study adds
In the National Joint Register, there are large baseline differences in characteristics of patients undergoing cemented, uncemented, or resurfacing procedures, which makes unadjusted comparisons inappropriate
Over eight years’ follow-up uncemented total hip replacement was associated with a small but significant increased revision rate compared with cemented total hip replacement at any time for patients alive and unrevised at that time, and cemented total hip replacement was associated with a small but significant increased mortality rate compared with uncemented total hip replacement at any time for patients without a revision at that time
Over six years’ follow-up, Birmingham hip resurfacing had a significantly lower mortality rate than uncemented and cemented total hip replacement in men of all ages, but a higher revision rate than cemented total hip replacement
This dataset was provided by the National Joint Registry for England and Wales. The views expressed represent those of the authors and do not necessarily reflect those of the National Joint Registry steering committee. We thank the two reviewers and the BMJ manuscript meeting committee for their helpful comments that have helped to considerably improve this paper.
Contributors: DJWMcM, JD, and RBCT observed clinical and registry differences and developed the idea for the paper, provided clinical input, and wrote extensive parts of the narrative. PBP provided initial statistical analyses and continued subsequent statistical and editorial advice. KIES undertook all data cleaning, performed all statistical analyses, produced all the table and figures, and helped to draft and revise the paper. RDR devised the statistical analysis plan, undertook initial statistical analyses, supervised the work done by KIES, wrote most of the first article draft, and helped to revise it accordingly. RDR is guarantor.
Funding: KIES is funded by the MRC Midlands Hub for Trials Methodology Research at the University of Birmingham (Medical Research Council Grant ID G0800808). RDR is also supported by funding from this Hub.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: DJWMcM and RBCT were designers of Birmingham hip resurfacing and were shareholders in Midland Medical Technologies before the company was sold to Smith and Nephew in 2004. DJWMcM is an unpaid consultant to Smith and Nephew Orthopaedics UK. The McMinn Centre receives institutional research funding for specific research projects but no funding has been received for the research or preparation of this manuscript.
Ethical approval: Not required. Existing anonymised data was used for this study.
Data sharing: This dataset was made available by the National Joint Registry for England and Wales.
Cite this as: BMJ 2012;344:e3319
Web Extra. Extra material supplied by the author
Appendix: Hip replacement and hip resurfacing techniques
References
- 1.Charnley J. Surgery of the hip joint. Present and future developments. BMJ 1960:i;821-6. [DOI] [PMC free article] [PubMed]
- 2.Charnley J. Low friction arthroplasty of the hip Berlin. Springer-Verlag, 1979.
- 3.Wroblewski BM, Siney PD, Fleming PA. Charnley low-friction arthroplasty. Survival patterns to 38 years. J Bone Joint Surg Br 2007;89:1015-8. [DOI] [PubMed] [Google Scholar]
- 4.McMinn DJ, Daniel J, Ziaee H, Pradhan C. Indications and results of hip resurfacing. Int Orthop 2011;35:231-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Treacy RB, McBryde CW, Shears E, Pynsent PB. Birmingham hip resurfacing: a minimum follow-up of ten years. J Bone Joint Surg Br 2011;93:27-33. [DOI] [PubMed] [Google Scholar]
- 6.Lingard EA, Muthumayandi K, Holland JP. Comparison of patient-reported outcomes between hip resurfacing and total hip replacement. J Bone Joint Surg Br 2009;91:1550-4. [DOI] [PubMed] [Google Scholar]
- 7.Baker RP, Pollard TC, Eastaugh-Waring SJ, Bannister GC. A medium-term comparison of hybrid hip replacement and Birmingham hip resurfacing in active young patients. J Bone Joint Surg Br 2011;93:158-63. [DOI] [PubMed] [Google Scholar]
- 8.Treacy RB. To resurface or replace the hip in the under 65-year-old: the case of resurfacing. Ann R Coll Surg Engl 2006;88:349-53. [PubMed] [Google Scholar]
- 9.Daniel J, Pynsent PB, McMinn DJ. Metal-on-metal resurfacing of the hip in patients under the age of 55 years with osteoarthritis. J Bone Joint Surg Br 2004;86:177-84. [DOI] [PubMed] [Google Scholar]
- 10.McBryde CW, Theivendran K, Thomas AM, Treacy RB, Pynsent PB. The influence of head size and sex on the outcome of Birmingham hip resurfacing. J Bone Joint Surg Am 2010;92:105-12. [DOI] [PubMed] [Google Scholar]
- 11.McMinn D. Resurfacing works. Presented at the Combined British Orthopaedic Association and Irish Orthopaedic Association Annual General Meeting. Dublin, Sept 2011.
- 12.Boyer P, Boutron I, Ravaud P. Scientific production and impact of national registers: the example of orthopaedic national registers. Osteoarthritis Cartilage 2011;19:858-63. [DOI] [PubMed] [Google Scholar]
- 13.Kolling C, Simmen BR, Labek G, Goldhahn J. Key factors for a successful national arthroplasty register. J Bone Joint Surg Br 2007;89:1567-73. [DOI] [PubMed] [Google Scholar]
- 14.Malchau H, Herberts P, Eisler T, Garellick G, Söderman P. The Swedish total hip replacement register. J Bone Joint Surg Am 2002;84-A(suppl 2):2-20. [DOI] [PubMed]
- 15.Rothwell AG. Development of the New Zealand Joint Register. Bull Hosp Jt Dis 1999;58:148-60. [PubMed] [Google Scholar]
- 16.Verhaar JA. [Prognosis of total hip replacement: the importance of an implant register]. Ned Tijdschr Geneeskd 2007;151:1915-7. [PubMed] [Google Scholar]
- 17.Gorenoi V, Schönermark MP, Hagen A. Arthroplasty register for Germany. GMS Health Technol Assess 2009;5:Doc13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Labek G, Böhler N. The European Arthroplasty Register (EAR), development and rationale for supranational cooperation of arthroplasty registers). Z Orthop Unfall 2009;147:151-7. [DOI] [PubMed] [Google Scholar]
- 19.8th Annual Report of the National Joint Registry of England and Wales 2011. www.njrcentre.org.uk/NjrCentre/Portals/0/Documents/NJR%208th%20Annual%20Report%202011.pdf.
- 20.Saklad M. Grading of patients for surgical procedures. Anesthesiology 1941;2:281-4. [Google Scholar]
- 21.Halaszynski TM, Juda R, Silverman DG. Optimizing postoperative outcomes with efficient preoperative assessment and management. Crit Care Med 2004;32(4 suppl):S76-86. [DOI] [PubMed] [Google Scholar]
- 22.Sedgwick P. Statistical significance and confidence intervals. BMJ 2009;339:b3401. [Google Scholar]
- 23.National Institute for Health and Clinical Excellence. Guidance on the selection of prosthesis for primary total hip replacement. TA2 Hip disease—replacement prostheses: guidance. 2003. http://guidance.nice.org.uk/TA2/Guidance/pdf/English.
- 24.Australian Orthopaedic Association, National Joint Replacement Registry. 2011 www.dmac.adelaide.edu.au/aoanjrr/documents/AnnualReports2011/AnnualReport_2011_WebVersion.pdf.
- 25.7th Annual Report of the National Joint Registry of England and Wales 2010. www.njrcentre.org.uk/NjrCentre/Portals/0/NJR%207th%20Annual%20Report%202010.pdf.
- 26.Royston P, Parmar MKB. Flexible parametric proportional-hazards and proportional-odds models for censored survival data, with application to prognostic modelling and estimation of treatment effects. Stat Med 2002;21:2175-97. [DOI] [PubMed] [Google Scholar]
- 27.Lambert PC, Royston P. Further development of flexible parametric models for survival analysis. Stata J 2009;9:265-90. [Google Scholar]
- 28.Royston P, Lambert PC. Flexible parametric survival analysis using Stata: beyond the Cox model. Stata Press, 2011
- 29.Cox DR. Regression models and life tables. J Roy Statist Soc (B) 1972;34:187-220. [Google Scholar]
- 30.Royston P, Parmar MKB. Flexible parametric-hazards and proportional-odds models for censored survival data, with application to prognostic modelling and estimation of treatment effects. Stat Med 2002;21:2175-97. [DOI] [PubMed] [Google Scholar]
- 31.Eskelinen A, Remes V, Helenius I, Pulkkinen P, Nevalainen J, Paavolainen P. Total hip arthroplasty for primary osteoarthrosis in younger patients in the Finnish arthroplasty register. 4,661 primary replacements followed for 0-22 years. Acta Orthop 2005;76:28-41. [DOI] [PubMed] [Google Scholar]
- 32.Hailer NP, Garellick G, Kärrholm J. Uncemented and cemented primary total hip arthroplasty in the Swedish Hip Arthroplasty Register. Acta Orthop 2010;81:34-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Mahomed NN, Barrett JA, Katz JN, Phillips CB, Losina E, Lew RA, et al. Rates and outcomes of primary and revision total hip replacement in the United States Medicare population. J Bone Joint Surg Am 2003;85:27-32. [DOI] [PubMed] [Google Scholar]
- 34.Aynardi M, Pulido L, Parvizi J, Sharkey PF, Rothman RH. Early mortality after modern total hip arthroplasty. Clin Orthop Relat Res 2009;467:213-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lie SA, Pratt N, Ryan P, Engesaeter LB, Havelin LI, Furnes O, et al. Duration of the increase in early postoperative mortality after elective hip and knee replacement. J Bone Joint Surg Am 2010;92:58-63. [DOI] [PubMed] [Google Scholar]
- 36.Pedersen AB, Baron JA, Overgaard S, Johnsen SP. Short- and long-term mortality following primary total hip replacement for osteoarthritis: a Danish nationwide epidemiological study. J Bone Joint Surg Br 2011;93:172-7. [DOI] [PubMed] [Google Scholar]
- 37.Lie SA, Engesaeter LB, Havelin LI, Furnes O, Vollset SE. Mortality after total hip replacement: 0-10-year follow up of 39,543 patients in the Norwegian Arthroplasty Register. Acta Orthop Scand 2000;71:19-27. [DOI] [PubMed] [Google Scholar]
- 38.Visuri T, Pulkkinen P, Turula KB, Paavolainen P, Koskenvuo M. Life expectancy after hip arthroplasty. Case-control study of 1018 cases of primary arthrosis. Acta Orthop Scand 1994;65:9-11. [DOI] [PubMed] [Google Scholar]
- 39.Visuri T, Borg H, Pulkkinen P, Paavolainen P, Pukkala E. A retrospective comparative study of mortality and causes of death among patients with metal-on-metal and metal-on-polyethylene total hip prostheses in primary osteoarthritis after a long-term follow-up. BMC Musculoskelet Disord 2010;11:78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Corbett KL, Losina E, Nti AA, Prokopetz JJ, Katz JN. Population-based rates of revision of primary total hip arthroplasty: a systematic review. PLoS One 2010;5:e13520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Santaguida PL, Hawker GA, Hudak PL, Glazier R, Mahomed NN, Kreder HJ, et al. Patient characteristics affecting the prognosis of total hip and knee joint arthroplasty: a systematic review. Can J Surg 2008;51:428-36. [PMC free article] [PubMed] [Google Scholar]
- 42.Mäkelä KT, Eskelinen A, Pulkkinen P, Paavolainen P, Remes V. Results of 3,668 primary total hip replacements for primary osteoarthritis in patients under the age of 55 years. Acta Orthop 2011;82:521-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hilmarsson S, Soderman P, Herbert P, Malchau H. An epidemiological analysis of a young total hip replacement population in Sweden. J Bone Joint Surg Br 2006;88:47-8. [Google Scholar]
- 44.Malchau P, Herberts P, Soderman P. Update and validation of results from the Swedish Hip Arthroplasty Registry 1979-1998. Department of Orthopaedics University of Goteborg, Sweden. Proceedings 67th Annual Meeting of American Academy of Orthopaedic Surgeons. Orlando, USA, 2000.
- 45.McMinn D, Treacy R, Lin K, Pynsent P. Metal on metal surface replacement of the hip. Experience of the McMinn prothesis. Clin Orthop Relat Res 1996;329(suppl):S89-98. [DOI] [PubMed] [Google Scholar]
- 46.Smith AJ, Dieppe P, Vernon K, Porter M, Blom AW. National Joint Registry of England and Wales. Failure rates of stemmed metal-on-metal hip replacements: analysis of data from the National Joint Registry of England and Wales. Lancet 2012;379:1199-204. [DOI] [PubMed] [Google Scholar]
- 47.Smith AJ, Dieppe P, Porter M, Blom AW. Risk of cancer in first seven years after metal-on-metal hip replacement compared with other bearings and general population: linkage study between the National Joint Registry of England and Wales and hospital episode statistics. BMJ 2012;344:e2383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Winkelmayer WC, Kurth T, Propensity scores: help or hype? Nephrol Dial Transplant 2004;19:1671-3. [DOI] [PubMed] [Google Scholar]
- 49.Goodfellow JW, O’Connor J, Murray DW. A critique of revision rate as an outcome measure: re-interpretation of knee joint registry data. J Bone Joint Surg Br 2010;92:1628-31. [DOI] [PubMed] [Google Scholar]
- 50.Wylde V, Blom AW. The failure of survivorship. J Bone Joint Surg Br 2011;93:569-70. [DOI] [PubMed] [Google Scholar]
- 51.Pynsent PB, Adams DJ, Disney SP. The Oxford hip and knee outcome questionnaires for arthroplasty: outcomes and standards for surgical audit. J Bone Joint Surg Br 2005;87:241-8 [correction in J Bone Joint Surg Br 2005;87:1166.] [DOI] [PubMed] [Google Scholar]
- 52.Wylde V, Blom AW, Whitehouse SL, Taylor AH, Pattison GT, Bannister GC. Patient-reported outcomes after total hip and knee arthroplasty: comparison of midterm results. J Arthroplasty 2009;24:210-6. [DOI] [PubMed] [Google Scholar]
- 53.Gillam MH, Salter A, Ryan P, Graves SE. Different competing risks models applied to data from the Australian Orthopaedic Association National Joint Replacement Registry. Acta Orthop 2011;82:513-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Garellick G, Kärrholm J, Rogmark C, Herberts P. Swedish Hip Arthroplasty Register, Annual Report 2010, Registercentrum VGR. www.shpr.se/Libraries/Documents/AnnualReport-2010-eng.sflb.ashx.
- 55.Pradhan C, Daniel J, Ziaee H, Complications and revisions of the Birmingham hip resurfacing. In: McMinn D, ed. Modern hip resurfacing. Springer, 2009:371-84.
- 56.Smith T, Data on file. Smith and Nephew Orthopaedics UK.
- 57.Donaldson AJ, Thomson HE, Harper NJ, Kenny NW. Bone cement implantation syndrome. Br J Anaesth 2009;102:12-22. [DOI] [PubMed] [Google Scholar]
- 58.Byrick RJ. Cement implantation syndrome: a time limited embolic phenomenon. Can J Anaesth 1997;44:107-11. [DOI] [PubMed] [Google Scholar]
- 59.Edmonds CR, Barbut D, Hager D, Sharrock NE. Intraoperative cerebral arterial embolisation during total hip arthroplasty. Anesthesiology 2000;93:315-8. [DOI] [PubMed] [Google Scholar]
- 60.Parvizi J, Holliday AD, Ereth MH, Lewallen DG. Sudden death during primary hip arthroplasty. Clin Orthop Relat Res 1999;369:39-48. [DOI] [PubMed] [Google Scholar]
- 61.Patterson B, Healey J, Cornell C, Sharrock N. Cardiac arrest during hip arthroplasty with a cemented long-stem component. A report of seven cases. J Bone Joint Surg 1991;73:271-7. [PubMed] [Google Scholar]
- 62.Peebles DJ, Ellis RH, Stride SDK, Simpson BRJ. Cardiovascular effects of methylmethacrylate cement. BMJ 1972;i:349-51. [DOI] [PMC free article] [PubMed]
- 63.Nedungayil SK, Mehendele S, Gheduzzi S, Learmonth ID. Femoral cementing techniques: current trends in the UK. Ann R Coll Surg Engl 2006;88:127-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Orsini EC, Byrick RJ, Mullen JBM, Kay JC, Waddell JP. Cardiopulmonary function and pulmonary microemboli during arthroplasty using cemented or non-cemented components the role of intramedullary pressure. J Bone Joint Surg 1987;69:822-32. [PubMed] [Google Scholar]
- 65.Issack PS, Lauerman MH, Helfet DL, Sculco TP, Lane JM. Fat embolism and respiratory distress associated with cemented femoral arthroplasty. Am J Orthop (Belle Mead NJ) 2009;38:72-6. [PubMed] [Google Scholar]
- 66.Pitto RP, Koessler M, Draenert K. The John Charnley Award. Prophylaxis of fat and bone marrow embolism in cemented total hip arthroplasty. Clin Orthop Relat Res 1998;355:23-34. [DOI] [PubMed] [Google Scholar]
- 67.Salem DN, O’Gara PT, Madias C, Pauker SG, American College of Chest Physicians. Valvular and structural heart disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. 8th edition. Chest 2008;133(6 suppl):593-629S. [DOI] [PubMed] [Google Scholar]
- 68.Lechat PH, Mas JL, Lascault G, Loron P, Theard M, KlimczacM, et al Prevalence of patent foramen ovale in patients with stroke. N Engl J Med 1988;318:1148-52. [DOI] [PubMed] [Google Scholar]
- 69.Lynch JJ, Schuchard GH, Gross CM, Wann LS. Prevalence of right-to-left shunting in the healthy population: detection by Valsalva maneuver contrast echocardiography. Am J Cardiol 1984;53:1478-80. [DOI] [PubMed] [Google Scholar]
- 70.Freeman JW. Anaesthesia, pain control and thromboprophylaxis. In: McMinn D, ed. Modern hip resurfacing. Springer, 2009:167-74.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix: Hip replacement and hip resurfacing techniques