

Abstract
Background
Research has linked knee extensor moment and knee shear force to the non-contact anterior cruciate ligament injury during the landing motion. However, how these biomechanical performance factors relate to knee translations in vivo it is not known as knee translations cannot be obtained with traditional motion capture techniques. The purpose of this study was to combine traditional motion capture with high-speed, biplane fluoroscopy imaging to determine relationships between knee extensor moment and knee shear force profiles with anterior and lateral tibial translations occurring during drop landing in females athletes.
Methods
15 females performed drop landings from a height of 40 cm while being recorded using a high speed, biplane fluoroscopy system and simultaneously being recorded using surface marker motion capture techniques to estimate knee joint angle, reaction force and moment profiles.
Findings
No significant statistical relationships were observed between peak anterior or posterior knee shear force and peak anterior and lateral tibial translations; or, between peak knee extensor moment and peak anterior and lateral tibial translations. Although differences were noted in peak shear force (P = 0.02) and peak knee extensor moment (P < 0.001) after stratification into low and high shear force and moment cohorts, no differences were noted in anterior and lateral tibial translations (all P ≥ 0.18).
Interpretation
Females exhibiting high knee extensor moment and knee shear force during drop landings do not yield correspondingly high anterior and lateral tibial translations.
Keywords: Biomechanics, ACL injury risk factors, Neuromuscular Training, ACL Injury Prevention
Introduction
The annual rate of injury to the anterior cruciate ligament (ACL) is reported to be above 1 in 3000 in the United States with a large proportion (∼70%) of ACL injuries non-contact in nature (Boden et al., 2000, Miyasaka et al., 1991).
Considerable research has demonstrated that loading of the ACL is partly determined by the force in the muscles that cross the knee. In vitro research has shown that the force in the muscles that produce knee extension moment affect ACL loading and under certain conditions can cause ACL damage (Renstrom et al., 1986, Durselen et al., 1995, Demorat et al., 2004). Recent modeling and simulation studies have also shown that the ACL is loaded when the shear force applied to the tibia is in the anterior direction; indicating that the quadriceps muscles, via the patellar tendon, are contributors to ACL loading during dynamic activities such as walking (Shelburne et al., 2004, Shelburne et al., 2005).
Human performance studies utilizing traditional surface marker motion capture techniques have also attempted to isolate and identify biomechanical performance factors, including knee shear forces and extensor moments, which may be related to non-contact ACL injury (Chappell et al., 2007, Chappell et al., 2002, Decker et al., 2003b, Huston et al., 2000, Kernozek et al., 2005, Yu et al., 2006, Yu et al., 2005). Chappell et al. (2002) showed that female recreational athletes had increased peak anterior knee shear force and peak knee extension moment and decreased knee flexion angle during landings in comparison to their male counterparts. Yu et al. (2005) also showed that the peak knee extension moments and peak anterior knee shear forces are significantly correlated to each other, supporting their view that that anterior knee shear force and knee extension moment are indicators of ACL loading during dynamic tasks such as the drop landing which evokes large eccentric quadriceps forces. Thus, based on the collective summary of many of these in vivo performance studies, as well as epidemiological data that shows relatively few combined anterior cruciate ligament/medial collateral ligament injuries are observed across the non-contact anterior cruciate ligament injured athlete populations (Majewski and Kentsch, 2002, Miyasaka et al., 1991), Yu and Garret (2007) and others have reasoned that a sagittal plane, non-contact anterior cruciate ligament injury mechanism is plausible. However, the results of these articles should be treated with caution. First, the anterior shear force described in these articles represents only a portion of the shear forces acting at the knee and does not include the contribution of joint reaction, muscle, and ligament. Second, it has been questioned whether the anterior shear force quoted in many of these articles is not in fact the reaction load due to the posterior shear force applied to the tibia and thus would represent the net force applied by muscles, ligaments and joint contact, and not the joint shear force applied to the tibia (Van Den Bogert and Mclean, 2006, Shin et al., 2007).
While estimates of external knee shear forces and moments can be calculated in vivo via inverse dynamics, the determination of actual tibio-femoral translations in vivo using traditional motion analysis techniques is difficult due to the soft tissue surrounding the knee joint (Leardini et al., 2005). Thus, investigators have been unable to directly determine what affect external knee shear forces and extensor moments have on knee translations in vivo during dynamic activities such as drop landing. Understanding these relationships in vivo is critical to understanding how the knee functions under high demand activities; and, could provide further insight into the mechanism of the non-contact ACL injury.
The objectives of this study were to: 1) utilize traditional human motion analysis techniques in combination with high-speed, biplane fluoroscopic imaging to describe the relationships between knee shear force and knee extensor moment profiles with anterior and lateral tibial translations (ATT and LTT) during the drop landings; and, 2) to measure the ATT and LTT kinematic differences between subjects exhibiting higher versus lower knee shear force and knee extensor moments during drop landings. Based on the “sagittal plane, quadriceps load induced injury” theory (Yu and Garrett, 2007) of the non-contact ACL injury, we hypothesized individuals exhibiting high external knee shear forces and/or knee extensor moments would exhibit larger ATT values during the drop landing.
Methods
Subjects and Landing Protocol
Fifteen female recreational athletes (Age 26.1 years (SD = 6.3); Height 167.9 cm (SD = 6.3), Body Mass 58.2 Kg (SD = 5.2) volunteered to participate in this study. These participants had no history of lower extremity injury. All subjects provided written informed consent approved by the Vail Valley Medical Center in accordance with the National Institutes of Health's guidelines.
The subjects were instructed to perform a drop landing maneuver by stepping off a 40 cm high platform onto a force plate and then immediately performing a peak height vertical jump (Myer et al., 2007). No other verbal or visual instruction as to the landing style was given prior to testing. All subjects were provided tight-fitting shorts and top and standardized court shoes (Turntec, model no. TM08061). After a 5-minute warm-up period, the subjects completed 10 landing trials in which a single trial for each subject was collected by fluoroscopy for analysis. The foot of the dominant limb landed directly onto a force plate (Bertec Corp., Columbus, Ohio, USA) fixed to the laboratory floor. The force plate data was sampled at 1200Hz and synchronized with the fluoroscopy video images such that the specific fluoroscopy frame of ground contact could be determined.
The subjects then completed a slow (2 sec), unloaded knee extension motion from a seated position (hip angle at 90 degrees) starting at a knee flexion of 90 degrees to the fully extended position. The unloaded knee extension trial was recorded only with fluoroscopy and used as a reference for the translations and rotations of the tibia relative to the femur measured during the landing trials. Also, the location of the tibia and femur at full extension was used to define the zero reference position of the bones of the knee (Blankevoort et al., 1990).
Surface Marker Motion Analysis Data Capture
Lower extremity, three-dimensional kinematics and kinetics were collected using a 10-camera system (Motion Analysis Corporation, Santa Rosa, CA, USA) sampling at 240 Hz. The 3D kinematics of each trial were captured by securing 37 retroreflective spherical (10 mm diameter) markers to anatomical landmarks on each subject to produce a standard, 3-marker-per-segment configuration (Kernozek et al., 2005). Marker trajectories and force data were filtered at the same frequency (20Hz) using a fourth order Butterworth filter (Bisseling and Hof, 2006). An initial standing “neutral” (erect) standing position of the subject in the anatomical position was also collected to establish relative angle adjustments for the landing data set. Joint angular position, velocities, and accelerations were calculated from the filtered 3D marker coordinate data and estimates of the (external) joint forces and moments were calculated using The Motion Monitor software (The Motion Monitor, Version 7.79, Chicago, IL, USA) by combining the kinematic and force plate data with anthropometric data using an inverse dynamics solution.
Description and calibration of the biplane fluoroscopy system
The biplane fluoroscopy system consists of two commercially available BV Pulsera c-arms with 30 cm image intensifiers (Philips Medical Systems, Best, Holland) coupled with two synchronized, high-speed, high-resolution (1024 × 1024) digital cameras (Phantom V5.1, Vision Research, Wayne, NJ, USA) which were interfaced with the image intensifiers of the fluoroscopy systems.
Image distortion was corrected and the focus position of each fluoroscopy system and the 3D relationship between the two fluoroscopy systems were calculated with previously described techniques (Torry et al., 2010, Garling et al., 2005). The transformation from the distorted image to the corrected image was determined and applied to all subsequent images using Model-Based Roentgen Stereophotogrammetric Analysis (MBRSA) software (Medis Specials, BV, Leiden, The Netherlands)(Hurschler et al., 2009).
Collection of in vivo landing data using biplane fluoroscopy
For each subject, a supine, high-resolution (voxels: 0.7×0.7×0.5mm), static bone CT scan of the knee (12cm above and below the joint line) utilizing an Aquilion 64 (Toshiba America Medical Systems, Tustin, CA, USA) was obtained. For each landing, biplane fluoroscopy data was collected for 1.0 s at 500 frames/s with a shutter speed of 1/2000 of a second. The x-ray generators were operated in radiographic mode at 60mA and approximately 60kV.
Fluoroscopy data reduction
Three-dimensional bone geometry reconstruction of the femur and tibia/fibula from CT data were extracted using commercial software (Mimics, Materialize, Inc, Ann Harbor, MI, USA). The origin of the femoral coordinate system was placed at the midpoint between the medial and lateral femoral condyles on the center line of a cylinder fitted to the medial and lateral posterior condyles. The medial-lateral axis was placed on the axis of the cylinder, and the inferior/superior axis aligned with the long axis of the femoral shaft (Blankevoort et al., 1990). The origin and alignment of the tibial coordinate system was assigned to the femoral coordinate system at full extension (i.e., 0 deg) as recorded by the fluoroscopy system in the knee extension trial (Torry et al., 2011, Torry et al., 2010). ATT was measured anterior to the tibia by the anterior distance between the femoral and tibial coordinate frames. Similarly, LTT was measured lateral to the tibia by the lateral distance between the femoral and tibial coordinate frames (Torry et al., 2011, Torry et al., 2010).
Determination of the bone poses from the biplane fluoroscopy data were performed using MBRSA (Medis Specials, Leiden, The Netherlands). For each frame, both inner and outer contours of the femur and tibia/fibula were semi-automatically extracted from the biplane fluoroscopy images. A fully-automatic 6 degree-of-freedom optimization algorithm was used to determine the pose, which optimally matched the detected contours with the projected contours from the imported bone geometries. From these bone pose sequences, knee kinematics were calculated using methods described by Grood and Suntay (Grood and Suntay, 1983). Following the examples of precision motion measurements taken from cadaver knees (Ishibashi et al., 1997), tibial translations and rotations measured from each subject during landing were referenced to the unloaded knee extension motion data.
Kinematic accuracies for tracking tantalum beads and bones using this biplane fluoroscopy system were determined. Our accuracy and precision of tracking 1.0 mm diameter tantalum markers were -5.5 μm and 32.5μm, respectively (Braun et al., 2010). However, in the present study implanting tantalum beads in the volunteers was not practical and only bones were tracked. Based on the high accuracy of tracking tantalum beads, bead tracking can be used as the gold standard for bone tracking methods. Therefore, tantalum beads were placed in a cadaveric knee specimen (3 beads per bone) and the specimen was manually ranged and cycled through full flexion-extension, varus-valgus and internal-external rotation. The mean ± 1 standard deviation of the differences in joint kinematics between those determined by tantalum beads and those by bone tracking were 0.2 mm (SD = 0.3), -0.1 mm (SD = 0.1), -0.05 mm (SD = 0.1) in translations; and, 0.1° (SD = 0.1), 0.3° (SD = 0.2), 0.1° (SD = 0.3) in rotations (Torry et al., 2010). To validate methods specific to this high impact study protocol a cadaver drop test was conducted and the data has been previously described (Torry et al., 2011). In brief, the mean and 1 standard deviation of the differences in joint kinematics between those determined by tracking tantalum beads and those by bone tracking of a cadaveric knee dropped from a 40 cm height were 0.07 mm (SD = 0.7), 0.1 mm (SD = 0.6) in medial-lateral and anterior-posterior translations; and, 0.09° (SD = 0.4), 0.1° (SD = 0.05), 0.1° (SD = 0.8) in flexion, varus-valgus, internal-external rotations, respectively. These values are consistent with previous work using similar technology (Anderst et al., 2009, Bey et al., 2008).
Statistical Analysis
Linear regression analyses were conducted to determine if peak anterior knee shear force and/or peak knee extensor moment are significant predictors of peak ATT and/or LTT during the drop landing. In order investigate differences in ATT or LTT in individuals possessing higher and lower peak anterior knee shear force and/or peak knee extensor moment profiles, the subject pool (N = 15) was subdivided into upper (n=5) and lower (n=5) cohorts according to each of these variables. The peak ATT and LTT between these upper and lower subdivisions were then compared utilizing an independent t-test (α = 0.05).
Results
Regression Analyses
Means and 1 standard deviation (SD) for peak knee shear force and peak knee extensor moment as measured by motion analysis system as well as peak ATT and LTT as measured by the biplane fluoroscopy system are presented in Table 2.
Table 2.
Group means (±1SD) for peak shear force, peak knee extensor moment, anterior tibial translation and lateral tibial translations. Group means (±1SD) for the low and high stratification also provided within each column.
| Peak Shear F (N) | Peak ATT (mm) | Peak LTT (mm) | |
|---|---|---|---|
| Group | |||
| Mean (±1SD) | -526.2 (258.3) | 4.6 (1.7) | 0.4 (1.0) |
| Low Knee Shear F Group (n = 5) | |||
| Mean (±1SD) | -320.4 (258.3) | 5.6 (2.4) | 0.4 (1.0) |
| High Knee Shear F Group (n = 5) | |||
| Mean (±1SD) | -814.9 (254.4) | 3.9 (0.9) | 0.7 (1.1) |
| Comparison of Low vs High Knee Shear F Groups | p = .02 | p = .18, β = .14 | p = .66, β = .07 |
| Peak Ext Moment (Nm) | Peak ATT (mm) | Peak LTT (mm) | |
| Group | |||
| Mean (±1SD) | 121.5 (44.4) | 4.6 (1.7) | 0.4 (1.0) |
| Low Knee Ext. Moment Group (n = 5) | |||
| Mean (±1SD) | 82.3 (11.3) | 3.7 (0.8) | 0.2 (1.3) |
| High Knee Ext. Moment Group (n = 5) | |||
| Mean (±1SD) | 172.8 (32.0) | 4.4 (1.3) | 0.2 (1.0) |
| Comparison of Low vs High Knee Ext Moment Groups | p < .0001 | p = .34, β = .17 | p = .99, β = .05 |
p-values represent t-tests between low and high group stratifications (peak shear, peak knee extensor moment) and within each column heading. When not significant, post-hoc power analysis were conducted (β = values).
The subjects landed with resultant ground reaction forces of 1315.2 N (SD = 629.3 N) (22.3 N/Kg, SD = 9.4 N/Kg); and as measured by the motion capture system, exhibited knee (ground contact) flexion angles of 14.6° (SD = 4.6°), and experienced peak knee flexion angles of 83.6° (SD = 9.2°).
The knee shear force exhibited a positive value (anterior shear force) just after ground contact and then transitioned to a negative value (posterior shear force). There was no correlation of the peak ATT value and the peak anterior knee shear force occurring during the first 0.0-0.018 sec after ground contact (P = 0.73, Figure 1A). No significant relationship was observed between peak posterior knee shear force measured by the motion capture system and peak ATT or LTT measured by the fluoroscopy system (P = 0.40, P = 0.53, respectively, Table 1, Figure 1A).
FIGURE 1.
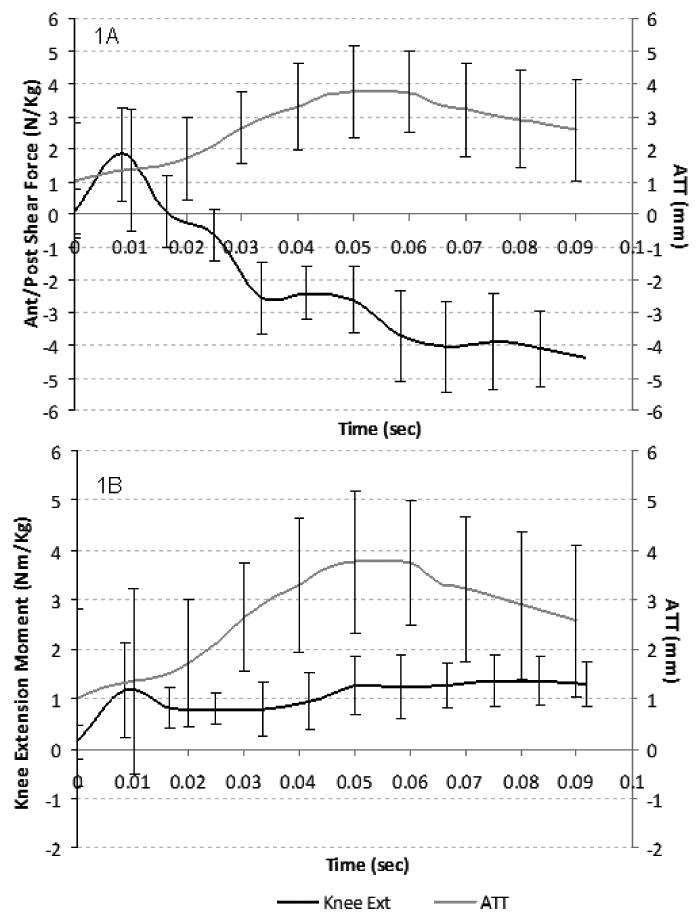
(1A): Time series plot of ATT (grey line) derived from fluoroscopy and knee shear force estimated from the motion capture system and the inverse dynamics process (black line). Positive values represent an anteriorly directed shear force. (1B) Time series plot of ATT derived from fluoroscopy (grey line) and the external knee extensor torque curve estimated from the motion capture system and the inverse dynamics process (black line). Positive torque values represent external knee extensor torque values. Deviations depicted in both time series data sets represent +/- 1 SD from the mean.
Table 1.
R-square values for peak shear force, peak knee extensor moment, peak anterior tibial translation and peak lateral translation.
| Variables | r2 | p-value |
|---|---|---|
| Peak ATT (mm), Peak Shear (N/Kg) | 0.06 | 0.4 |
| Peak ATT (mm), Peak Ext Torque (N*m/Kg) | 0.005 | 0.79 |
| Peak ATT (mm), Peak Ext Torque (N*m) | 0.002 | 0.89 |
| Peak ATT (mm), Peak Shear Force (N) | 0.06 | 0.4 |
| Peak LTT (mm), Peak Shear Force (N/Kg) | -0.03 | 0.53 |
| Peak LTT (mm), Peak Ext Torque (N*m/Kg) | -0.02 | 0.64 |
| Peak LTT (mm), Peak Ext Torque (N*m) | -0.01 | 0.71 |
| Peak LTT (mm), Peak Shear Force (N) | -0.03 | 0.51 |
No significant relationship was observed between peak knee extensor moment measured by the motion capture system and peak ATT or LTT measured by the fluoroscopy system (P = 0.89, P = 0.71, respectively; Table 1, Figure 1B).
Low versus High Risk Group Comparisons
When the group (N = 15) was subdivided into upper (n=5) and lower (n=5) cohorts based on each individual's peak knee shear force value, significant differences in the peak knee shear force as determined by the motion capture system were noted (P = 0.02, Table 2). However, no differences in peak ATT or LTT were observed (P = 0.18, P = 0.66, respectively). This non-significant finding remained after the knee shear force profiles were normalized to subject body mass (N*m/Kg).
When the group was subdivided into upper and lower cohorts based on each individual's peak knee extensor moment value, significant differences in the peak knee extensor moment as determined by the motion capture system were noted (P < 0.0001; Table 2). However, no differences in peak ATT or LTT were observed (P = 0.34, P = 0.99, respectively). This non-significant finding remained even after the knee extensor moment profiles were normalized to subject body mass (N*m/Kg).
Discussion
Yu and Garrett (2007) and others have reasoned that sagittal plane biomechanics play a key role in the non-contact ACL injury mechanism (Chappell et al., 2007, Chappell et al., 2002). Specifically, these authors have suggested that the peak external knee shear force and/or the peak knee extensor moment during landing or a deceleration motion may be the mechanical factors that incite the non-contact ACL injury. The present study found no relationship between peak knee shear (anterior or posterior) force or peak knee extensor moment with peak ATT or LTT during the drop landings. These non-significant findings in the knee translations remained even though significant differences in peak knee shear force and knee extensor moments were identified using the motion capture system to stratify the individuals into upper and lower bounds based on higher versus lower peak knee shear force and peak knee extensor moment values.
The sagittal plane injury theory is based largely on the premise that the ACL provides ∼80-85% of the total restraint to ATT when the knee is at low (20-30°) flexion angles(Markolf et al., 1976, Butler et al., 1980); and, anterior knee shear forces are expected to place loads on the ACL during deceleration motions such as landing from a jump in vivo (Sell et al., 2007, Chappell et al., 2002, Yu et al., 2002). Moreover, substantial cadaveric and computer modeling evidence has shown that the patellar tendon can cause ATT, increased ACL strains and even damage when the quadriceps produce high loads (Markolf et al., 1995, Renstrom et al., 1986, Demorat et al., 2004). The lack of association in ATT or LTT to knee extensor moment and/or external knee shear forces was in contrast to what was expected to occur at the knee during landings based on previous in vivo landing studies (Sell et al., 2007, Chappell et al., 2002, Yu et al., 2002); but, these results are not entirely unexpected based on modeling efforts (Pflum et al., 2004, Shin et al., 2007). In 2004, Pflum et al, showed that the pattern of ACL force in landing cannot be explained by the mechanism of quadriceps force alone. The maximum force transmitted to the model's ACL resulted from a complex interaction between the patellar tendon force, the compressive force acting at the tibiofemoral joint, and the ground reaction force. The external shear force calculated here and by others using inverse dynamics does not include the force in the muscles, ligaments, and bony contact. We believe that this incomplete summation of shear force explains why no correlation was found between ATT and LTT and the external knee shear force of the subjects. In addition, knee shear force was primarily directed posterior for much of the landing motion (Figure 1). Shin et al. (2007) (Shin et al., 2007) noted that when posterior forces that replicated in vivo conditions were applied to their model, the peak ACL strain was reduced. Likewise, utilizing cadavers limbs dropped from a known height, Withrow et al., (2006) (Withrow et al., 2006) reported ACL strain was larger for the impulsive compression loading in valgus and flexion compared to loading in isolated flexion.
Soft landings are thought to allow for less ground reaction force and greater energy dissipation through greater ranges of motion at the knee (Decker et al., 2003a) and are thus taught in many ACL prevention programs. If the knee is more fully extended during ground contact, the patellar tendon will be more anteriorly inclined relative to the long axis of the tibia. This, combined with a large quadriceps force developed in the eccentric contraction, causes a large anterior shear force to be applied to the lower leg (Decker et al., 2003b, Sell et al., 2007). An increase in anterior shear force is suggested to increase ATT, thereby causing an increase in ACL strain (Yu and Garrett, 2007). In the present study, no verbal cues were given to encourage either a soft or stiff landing. Instead, the females were allowed to land in a self-selected manner and to complete a peak vertical jump as described by previous ACL injury screening studies (Hewett et al., 2005, Myer et al., 2007). The females in this study landed with knee (contact) flexion angles that were ∼10° less flexed than reported by previous studies (Decker et al., 2003a, Sell et al., 2007, Yu et al., 2006); indicating a more erect landing style which should have increased our ability to observe ATT in these subjects. Thus, how soft versus stiff landings actually affect knee translations need to be more fully understood before recommendations regarding “how to land safely” are promoted.
The magnitudes of ATT and lateral translation found in this study are also reasonably close to the values in previous dynamic, in vivo reports (Li et al., 2009, Tashman et al., 2004). Li et al. reported peak ATT ranging from 4.23 mm - 4.89 mm and peak medio-lateral translations ranging from 5.58 mm - 5.80 mm during gait (speeds of 1.5 - 3.0 m/s). Extrapolating data published by Tashman et al. 2004 revealed that the healthy limbs experienced approximately 8 mm of A/P translation and approximately 1 mm of lateral translation when jogging downhill (10° slope) at 2.5 m/s. Deneweth et al. 2010, (Deneweth et al., 2010) using similar technology recently reported 12 mm of anterior tibial translation in the healthy limb of individuals with contralateral ACL repair.
Current knowledge regarding ACL stiffness and load mitigation are based primarily on in vitro investigations which are limited in physiologic load applications (Woo et al., 1991, Woo et al., 1992). Biplane fluoroscopy offers methods to overcome the inherent errors associated with traditional motion capture studies in understanding knee translations in vivo during dynamic tasks; as well bridge the insufficient physiologic load deficits gap employed by current in vitro technology in assessing joint stability. In such, biplane radiographic techniques in combination with traditional motion capture methods show promise in investigating how the underlying neuromuscular control mechanics are employed and are altered and/or related to knee joint function as the functional demand of the knee increases through both internal and external forces and moments.
Within the scope of this study, limitations are acknowledged. This study utilized a group of healthy females in a controlled setting for experimentation and as such, is a limitation in understanding knee motion during the actual non-contact ACL injury mechanism. Moreover, only double-legged landings were evaluated; single-limb landings may increase or otherwise alter the external loads and provide different results. Additionally, the subjects were not instructed to land softer or stiffer but rather in self selected manner. Enforcing the subjects to land with a more “stiff” landing profile emphasizing less knee flexion may elicit greater ATT and LTT values. The subjects in this study exhibited peak knee shear forces at 8 ± 3 N/Kg; which are similar to previous studies (Kernozek et al., 2008, Sell et al., 2007, Yu et al., 2006) but it is possible that these values did not reach sufficiently high thresholds to elicit significant ATT. The review process raised issues with our selected filtering methodology and we acknowledge that the inherent signal-to-noise error in the motion capture technique and our selected filtering parameters will have caused dampening of the peak shear force and moment data reported; and, the time series data for traditional motion capture (240 Hz) and fluoroscopy data (500Hz) were synchronized beginning at the point of ground contact.
After this point, however, the data do not always match time point for time point with the data synchronize every 50 msec with a maximum offset of 1 msec. A better choice of motion capture collection frequency would have precisely synchronized the data collected. Even so, both collection frequencies were high to characterize the changes that occur during landing. This was our goal given the fact that the focus was primarily on assessing relationships that exist between peak values of ATT and peak knee moment/joint reaction force.
Prospective cohort studies commonly use epidemiological research designs for determining injury and risk factors. These studies, however, are descriptive in nature and do not examine the cause-and-effect relationship between identified risk factors and the injury. The result of this study suggest that this may also be true for performance based studies where inverse dynamic analyses are utilized to isolate and label biomechanical factors as predictive or injurious. Without a good understanding of the injury mechanisms, the risk factors for sustaining non-contact ACL injuries identified from epidemiological or biomechanical performance studies could be misinterpreted and lead to the selection of non-optimal injury prevention programs. Thus, although high knee extensor moments and anterior knee shear forces have been associated with ACL loads in modeling and cadaveric studies, these parameters did not produce correspondingly high ATT values in vivo in the present study.
Conclusion
Although several studies have implicated high anterior knee shear forces and extensor quadriceps moment in causing strain on the ACL during landing motions, the present study found no association between peak anterior knee shear force or peak knee extensor moment with peak ATT or LTT during the drop landing in females athletes.
FIGURE 2.
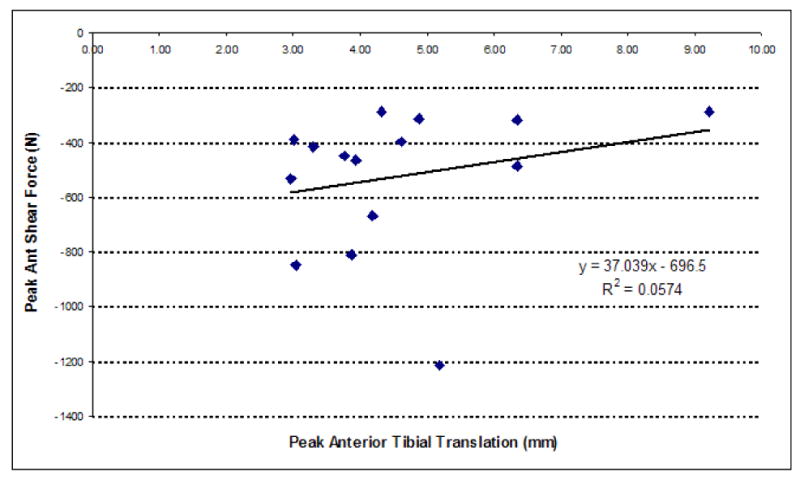
Regression plot and equation of peak knee shear force versus anterior tibial translation.
FIGURE 3.
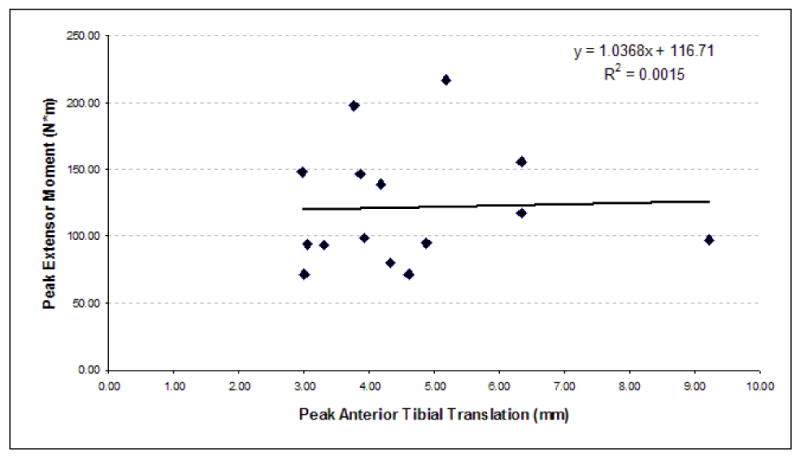
Regression plot and equation of peak knee extensor moment versus anterior tibial translation.
Acknowledgments
This study was funded by the National Institutes of Health (AR39683 to PI: Savio L-Y. Woo) and the Steadman Philippon Research Institute. The authors wish to thank Andrea North, Elizabeth Hageman and Nicole Pinwell for help with data collection and the reduction process. Medis Specials is acknowledged for use of MBRSA software.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Anderst W, Zauel R, Bishop J, Demps E, Tashman S. Validation of three-dimensional model-based tibio-femoral tracking during running. Med Eng Phys. 2009;31:10–6. doi: 10.1016/j.medengphy.2008.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bey MJ, Kline SK, Tashman S, Zauel R. Accuracy of biplane x-ray imaging combined with model-based tracking for measuring in-vivo patellofemoral joint motion. J Orthop Surg. 2008;3:38. doi: 10.1186/1749-799X-3-38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bisseling RW, Hof AL. Handling of impact forces in inverse dynamics. J Biomech. 2006;39:2438–44. doi: 10.1016/j.jbiomech.2005.07.021. [DOI] [PubMed] [Google Scholar]
- Blankevoort L, Huiskes R, De Lange A. Helical axes of passive knee joint motions. J Biomech. 1990;23:1219–29. doi: 10.1016/0021-9290(90)90379-h. [DOI] [PubMed] [Google Scholar]
- Boden BP, Griffin LY, Garrett WE., Jr Etiology and Prevention of Noncontact ACL Injury. Phys Sportsmed. 2000;28:53–60. doi: 10.3810/psm.2000.04.841. [DOI] [PubMed] [Google Scholar]
- Braun S, Millett PJ, Yongpravat C, Pault JD, Anstett T, Torry MR, Giphart JE. Biomechanical evaluation of shear force vectors leading to injury of the biceps reflection pulley: a biplane fluoroscopy study on cadaveric shoulders. Am J Sports Med. 2010;38:1015–24. doi: 10.1177/0363546509355142. [DOI] [PubMed] [Google Scholar]
- Butler DL, Noyes FR, Grood ES. Ligamentous restraints to anterior-posterior drawer in the human knee. A biomechanical study. J Bone Joint Surg Am. 1980;62:259–70. [PubMed] [Google Scholar]
- Chappell JD, Creighton RA, Giuliani C, Yu B, Garrett WE. Kinematics and electromyography of landing preparation in vertical stop-jump: risks for noncontact anterior cruciate ligament injury. Am J Sports Med. 2007;35:235–41. doi: 10.1177/0363546506294077. [DOI] [PubMed] [Google Scholar]
- Chappell JD, Yu B, Kirkendall DT, Garrett WE. A comparison of knee kinetics between male and female recreational athletes in stop-jump tasks. Am J Sports Med. 2002;30:261–7. doi: 10.1177/03635465020300021901. [DOI] [PubMed] [Google Scholar]
- Decker MJ, Tokish JM, Ellis HB, Torry MR, Hawkins RJ. Subscapularis muscle activity during selected rehabilitation exercises. Am J Sports Med. 2003a;31:126–34. doi: 10.1177/03635465030310010601. [DOI] [PubMed] [Google Scholar]
- Decker MJ, Torry MR, Wyland DJ, Sterett WI, Richard Steadman J. Gender differences in lower extremity kinematics, kinetics and energy absorption during landing. Clin Biomech (Bristol, Avon) 2003b;18:662–9. doi: 10.1016/s0268-0033(03)00090-1. [DOI] [PubMed] [Google Scholar]
- Demorat G, Weinhold P, Blackburn T, Chudik S, Garrett WE. Aggressive quadriceps loading can induce non-contact Anterior cruciate ligament injury. American Journal of Sports Medicine. 2004;32:477–483. doi: 10.1177/0363546503258928. [DOI] [PubMed] [Google Scholar]
- Deneweth JM, Bey MJ, Mclean SG, Lock TR, Kolowich PA, Tashman S. Tibiofemoral joint kinematics of the anterior cruciate ligament-reconstructed knee during a single-legged hop landing. Am J Sports Med. 2010;38:1820–8. doi: 10.1177/0363546510365531. [DOI] [PubMed] [Google Scholar]
- Durselen L, Claes L, Kiefer H. The influence of muscle forces and external loads on cruciate ligament strain. Am J Sports Med. 1995;23:129–36. doi: 10.1177/036354659502300122. [DOI] [PubMed] [Google Scholar]
- Garling EH, Kaptein BL, Geleijns K, Nelissen RG, Valstar ER. Marker Configuration Model-Based Roentgen Fluoroscopic Analysis. J Biomech. 2005;38:893–901. doi: 10.1016/j.jbiomech.2004.04.026. [DOI] [PubMed] [Google Scholar]
- Grood ES, Suntay WJ. A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng. 1983;105:136–44. doi: 10.1115/1.3138397. [DOI] [PubMed] [Google Scholar]
- Hewett TE, Myer GD, Ford KR, Heidt RS, Jr, Colosimo AJ, Mclean SG, Van Den Bogert AJ, Paterno MV, Succop P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33:492–501. doi: 10.1177/0363546504269591. [DOI] [PubMed] [Google Scholar]
- Hurschler C, Seehaus F, Emmerich J, Kaptein BL, Windhagen H. Comparison of the model-based and marker-based roentgen stereophotogrammetry methods in a typical clinical setting. J Arthroplasty. 2009;24:594–606. doi: 10.1016/j.arth.2008.02.004. [DOI] [PubMed] [Google Scholar]
- Huston LJ, Wojtys EM, Ashton-Miller JA. Gender differences in knee angle when landing from a jump. In: Andrish JT, Baker CL, editors. 67th Annual American Academy of Orthopedic Surgeons; March 17, 2000; Orlando, FL. 2000. pp. 157–159. Year. [Google Scholar]
- Ishibashi Y, Rudy TW, Livesay GA, Stone JD, Fu FH, Woo SL. The effect of anterior cruciate ligament graft fixation site at the tibia on knee stability: evaluation using a robotic testing system. Arthroscopy. 1997;13:177–82. doi: 10.1016/s0749-8063(97)90152-3. [DOI] [PubMed] [Google Scholar]
- Kernozek TW, Torry MR, H VANH, Cowley H, Tanner S. Gender differences in frontal and sagittal plane biomechanics during drop landings. Med Sci Sports Exerc. 2005;37:1003–12. [PubMed] [Google Scholar]
- Kernozek TW, Torry MR, Iwasaki M. Gender differences in lower extremity landing mechanics caused by neuromuscular fatigue. Am J Sports Med. 2008;36:554–65. doi: 10.1177/0363546507308934. [DOI] [PubMed] [Google Scholar]
- Leardini A, Chiari L, Della Croce U, Cappozzo A. Human movement analysis using stereophotogrammetry. Part 3. Soft tissue artifact assessment and compensation. Gait Posture. 2005;21:212–25. doi: 10.1016/j.gaitpost.2004.05.002. [DOI] [PubMed] [Google Scholar]
- Li G, Kozanek M, Hosseini A, Liu F, Van De Velde SK, Rubash HE. New fluoroscopic imaging techniques for investigation of 6DOF knee kinematics during treadmill walking. Journal Orthopedic Surgery and Research. 2009;4:1–5. doi: 10.1186/1749-799x-4-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Majewski M, Kentsch A. A new technique for arthroscopic management of painful stiff knee after anterior cruciate ligament reconstruction due to femoral malposition. Knee Surg Sports Traumatol Arthrosc. 2002;10:335–9. doi: 10.1007/s00167-002-0319-6. [DOI] [PubMed] [Google Scholar]
- Markolf KL, Burchfield DM, Shapiro MM, Shepard MF, Finerman GA, Slauterbeck JL. Combined knee loading states that generate high anterior cruciate ligament forces. J Orthop Res. 1995;13:930–5. doi: 10.1002/jor.1100130618. [DOI] [PubMed] [Google Scholar]
- Markolf KL, Mensch JS, Amstutz HC. Stiffness and laxity of the knee--the contributions of the supporting structures. A quantitative in vitro study. J Bone Joint Surg Am. 1976;58:583–94. [PubMed] [Google Scholar]
- Miyasaka K, Daniel DM, Stone ML, Hirschmann H. The incidence of knee ligament injuries in the general population. American Journal of Knee Surgery. 1991;4:3–8. [Google Scholar]
- Myer GD, Ford KR, Brent JL, Hewett TE. Differential neuromuscular training effects on ACL injury risk factors in“high-risk” versus “low-risk” athletes. BMC Musculoskelet Disord. 2007;8:39. doi: 10.1186/1471-2474-8-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pflum MA, Shelburne KB, Torry MR, Decker MJ, Pandy MG. Model prediction of anterior cruciate ligament force during drop-landings. Med Sci Sports Exerc. 2004;36:1949–58. doi: 10.1249/01.mss.0000145467.79916.46. [DOI] [PubMed] [Google Scholar]
- Renstrom P, Arms SW, Stanwyck TS, Johnson RJ, Pope MH. Strain within the anterior cruciate ligament during hamstring and quadriceps activity. Am J Sports Med. 1986;14:83–7. doi: 10.1177/036354658601400114. [DOI] [PubMed] [Google Scholar]
- Sell TC, Ferris CM, Abt JP, Tsai YS, Myers JB, Fu FH, Lephart SM. Predictors of proximal tibia anterior shear force during a vertical stop-jump. J Orthop Res. 2007;25:1589–97. doi: 10.1002/jor.20459. [DOI] [PubMed] [Google Scholar]
- Shelburne KB, Pandy MG, Anderson FC, Torry MR. Pattern of anterior cruciate ligament force in normal walking. J Biomech. 2004;37:797–805. doi: 10.1016/j.jbiomech.2003.10.010. [DOI] [PubMed] [Google Scholar]
- Shelburne KB, Torry MR, Pandy MG. Muscle, ligament, and joint-contact forces at the knee during walking. Med Sci Sports Exerc. 2005;37:1948–56. doi: 10.1249/01.mss.0000180404.86078.ff. [DOI] [PubMed] [Google Scholar]
- Shin CS, Chaudhari AM, Andriacchi TP. The influence of deceleration forces on ACL strain during single-leg landing: a simulation study. J Biomech. 2007;40:1145–52. doi: 10.1016/j.jbiomech.2006.05.004. [DOI] [PubMed] [Google Scholar]
- Tashman S, Collon D, Anderson K, Kolowich P, Anderst W. Abnormal rotational knee motion during running after anterior cruciate ligament reconstruction. Am J Sports Med. 2004;32:975–83. doi: 10.1177/0363546503261709. [DOI] [PubMed] [Google Scholar]
- Torry M, Myers C, Pennington W, Shelburne K, Krong J, Giphart J, Steadman J, Woo S. Relationship of anterior knee laxity to knee translations during drop landings: a bi-plane fluoroscopy study. Knee Surgery Sports Traumatology Arthroscopy. 2011 doi: 10.1007/s00167-010-1327-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Torry MR, Shelburne KB, Peterson DS, Giphart JE, Krong JP, Myers C, Steadman JR, Woo SL. Knee Kinematic Profiles During Drop Landings: A Biplane Fluoroscopy Study. Med Sci Sports Exerc. 2010 doi: 10.1249/MSS.0b013e3181f1e491. [DOI] [PubMed] [Google Scholar]
- Van Den Bogert AJ, Mclean SG. Letter To The Editor. Am J Sports Med. 2006;34:312–314. doi: 10.1177/0363546505283276. [DOI] [PubMed] [Google Scholar]
- Withrow TJ, Huston LJ, Wojtys EM, Ashton-Miller JA. The effect of an impulsive knee valgus moment on in vitro relative ACL strain during a simulated jump landing. Clin Biomech (Bristol, Avon) 2006;21:977–83. doi: 10.1016/j.clinbiomech.2006.05.001. [DOI] [PubMed] [Google Scholar]
- Woo SL, Hollis JM, Adams DJ, Lyon RM, Takai S. Tensile properties of the human femur-anterior cruciate ligament-tibia complex. The effects of specimen age and orientation. Am J Sports Med. 1991;19:217–25. doi: 10.1177/036354659101900303. [DOI] [PubMed] [Google Scholar]
- Woo SL, Livesay GA, Engle C. Biomechanics of the human anterior cruciate ligament. ACL structure and role in knee motion. Orthop Rev. 1992;21:835–42. [PubMed] [Google Scholar]
- Yu B, Garrett WE. Mechanisms of non-contact ACL injuries. Br J Sports Med. 2007;41(1):i47–51. doi: 10.1136/bjsm.2007.037192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yu B, Kirkendall DT, Taft TN, Garrett WE., Jr Lower extremity motor control-related and other risk factors for noncontact anterior cruciate ligament injuries. Instr Course Lect. 2002;51:315–24. [PubMed] [Google Scholar]
- Yu B, Lin CF, Garrett WE. Lower extremity biomechanics during the landing of a stop-jump task. Clin Biomech (Bristol, Avon) 2006;21:297–305. doi: 10.1016/j.clinbiomech.2005.11.003. [DOI] [PubMed] [Google Scholar]
- Yu B, Mcclure SB, Onate JA, Guskiewicz KM, Kirkendall DT, Garrett WE. Age and gender effects on lower extremity kinematics of youth soccer players in a stop-jump task. Am J Sports Med. 2005;33:1356–64. doi: 10.1177/0363546504273049. [DOI] [PubMed] [Google Scholar]