

Abstract
The principle of stretching wound margins for primary wound closure is commonly practiced and used for various skin defects, leading at times to excessive tension and complications during wound closure. Different surgical techniques, skin stretching devices and tissue expanders have been utilized to address this issue. Previously designed skin stretching devices resulted in considerable morbidity. They were invasive by nature and associated with relatively high localized tissue pressure, frequently leading to necrosis, damage and tearing of skin at the wound margins. To assess the clinical effectiveness and performance and, to determine the safety of TopClosure® for gradual, controlled, temporary, noninvasive and invasive applications for skin stretching and secure wound closing, the TopClosure® device was applied to 20 patients for preoperative skin lesion removal and to secure closure of a variety of wound sizes. TopClosure® was reinforced with adhesives, staples and/or surgical sutures, depending on the circumstances of the wound and the surgeon’s judgment. TopClosure® was used prior to, during and/or after surgery to reduce tension across wound edges. No significant complications or adverse events were associated with its use. TopClosure® was effectively used for preoperative skin expansion in preparation for dermal resection (e.g., congenital nevi). It aided closure of large wounds involving significant loss of skin and soft tissue by mobilizing skin and subcutaneous tissue, thus avoiding the need for skin grafts or flaps. Following surgery, it was used to secure closure of wounds under tension, thus improving wound aesthetics. A sample case study will be presented. We designed TopClosure®, an innovative device, to modify the currently practiced concept of wound closure by applying minimal stress to the skin, away from damaged wound edges, with flexible force vectors and versatile methods of attachment to the skin, in a noninvasive or invasive manner.
Keywords: Wound closure, Skin stretching, Tissue expansion, Viscoelastic properties of skin, Mechanical creep, Stress relaxation
Introduction
Wounds that have been closed under excessive tension or which must be reexplored, skin defects that cannot be primarily closed and large lesions that need to be excised pose a daily challenge for the reconstructive surgeon. Many techniques have been applied for closure of large skin defects: skin grafts, local flaps, tissue stretching and expansion, free flaps and closure by secondary intention. Some of these modalities carry considerable morbidity, complexity and risks associated with lengthy healing time; they are costly to the patient and are often aesthetically inferior in comparison to tensionless primary wound closure.
Mechanical forces play a significant role in the formation and structuring of tissues, mainly the skin, during human development, through life and during repair processes, determining their three-dimensional shape, as well as structural and remodeling properties affecting tissue on cellular and subcellular levels [1–3]. Shear stress, tension, compression and hydrostatic pressure are conducted through the extracellular matrix or extracellular fluid to individual cells. It has been proposed that cells convert these mechanical stimuli into electrical signals through biochemical mechanoreceptors (mechanosensors) such as mechanosensitive ion channels, cell adhesion molecules including integrins and actin filaments in the cytoskeleton [4–6]. It was also proven that there is a vast intracellular effect created by mechanical stretching—for example, mechanical stretching modulates growth direction and MMP-9 release in human keratinocyte monolayer [7].
The mechanical properties of soft tissues have been widely investigated [8]. Tension is a principal force experienced by the skin, and with optimal amplitude and waveform, it may aid in facilitating its growth and expansion for early wound closure. Extensible connective tissues (e.g., skin, blood vessels, fascia) contain networks of fibrous collagen and elastin within the extracellular matrix and in an amorphous matrix, and are affected during mechanical loading [9]. Skin exhibits load history-dependent behavior. The epidermal and dermal layers of skin consist largely of collagen (about 75% of dry weight) and elastin (4% of dry weight) fibers embedded and floating in a gel-like base [10]. The reorientation of this interwoven network of elastin and mainly collagen fibers provides the skin with the ability to stretch and expand [11], hence displaying a viscoelastic nature with their nonlinear stress–strain curves [12].
Biomechanical properties of the skin, specifically mechanical creep and stress relaxation, allow skin to stretch beyond its inherent extensibility within a relatively short period of time. Mechanical creep is the phenomenon where skin will stretch and elongate with time as long as force is applied. If the skin is stretched to a constant distance in a state of stress relaxation, it will expand, leading to a gradually reduced tension on the skin. As a result of skin stretching and elongation, wound closing tension decreases, allowing primary closure of relatively large defects [13]. In 1993, a new technique was introduced by Hirshowitz et al. [14] based on the use of the Sure-Closure® skin-stretching system. This skin stretching device was designed to harness the viscoelastic properties of skin by invasively applying controlled and evenly distributed tension along the wound margins, using incremental traction over a period of time, thereby allowing primary closure of relatively small- to medium-size skin defects.
However, some of the main drawbacks of this device and similar ones [15, 16] are the sole invasive nature of their use and the application of relatively high stress close to the wound edges, leading at times to pressure ischemia, necrosis and tearing of tissue.
In this study, we present our clinical experience with the Topclosure® 3S System, an innovative, simple, skin stretching and wound closure-secure system designed to harness both mechanical creep and stress relaxation principles. This new concept uses distribution of the force necessary to stretch the skin over a relatively wide area of adherence, away from the traumatized wound edges, using selective vector-oriented forces, continuously or cyclically, in both noninvasive and invasive manners.
Materials and methods
Device structure and mechanical characteristics
The TopClosure® 3S System (Figs. 1 and 2) comprises two attachment plates (AP) that are interconnected by a long, flexible approximation strap (AS). The APs are adhered to the skin by hypoallergenic, biocompatible adhesive on their undersurface for noninvasive application. Multiple pairs of oval openings along the longitudinal axis of the AP were designed for invasive attachment to the skin, using either staples or sutures. An additional horizontal cylindrical opening at the proximal end of the AP allows insertion of K-wire (KW) that is longitudinally attached to the wound margins. The AP comprises a specially designated polypropylene polymer mixture designed to adapt and maintain its shape to match the curvature of the treated area by bending it at the horizontal slits prior to application to the skin.
Fig. 1.
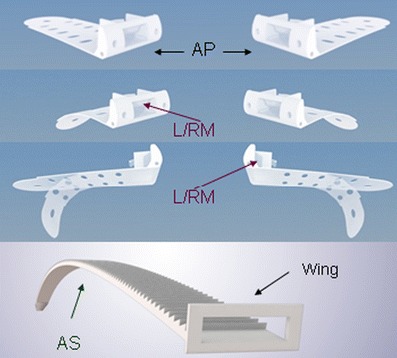
The TopClosure® 3S System comprising two APs that are interconnected by a long, flexible AS. AP, attachment plates; L/RM, lock/release ratchet mechanism; AS, approximation strap
Fig. 2.
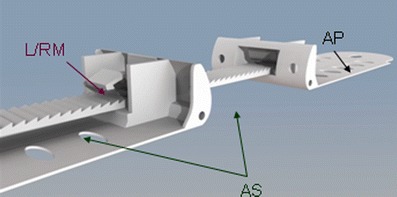
The TopClosure® 3S System comprising two APs that are interconnected by a long, flexible AS. AP, attachment plates; L/RM, lock/release ratchet mechanism; AS, approximation strap
The AS links the opposing APs, enabling approximation and advancing the APs by incremental pull on the AS. The AS is completely inserted through the lock/release ratchet mechanism (L/RM) on the proximal AP until being secured by the AS’s wings. Next, it is inserted into the L/RM on the opposing AP to allow gradual controlled stretching of the underlying skin. The AS is locked or released by lightly pressing or lifting the L/RM’s lever. The TopClosure® 3S System is provided in three sizes of matching AS and designated L/RM. The L/RM is positioned in the center front of the APs to selectively fit 4-, 6-, or 8-mm-wide ASs.
The TopClosure® 3S System was designed with inherent safety features that restrict unintentional application of excessive tension to the skin. The L/RM and AS wings are structured to collapse at maximal predetermined forces.
Following approval by the institutional ethics committee, the TopClosure® device was applied to 21 wounds in 20 patients 6 years and older for various clinical applications: preoperative skin lesion removal, closure of a variety of surgical wounds, following trauma and also securing the wound closure (Table 1). TopClosure® was reinforced noninvasively with an adhesive and a drape, and in an invasive manner by staples and/or surgical sutures, depending on the circumstance of the wound and the surgeon’s judgment.
Table 1.
Summary data of 21 wounds in 20 patients treated with TopClosure® aPR, preoperative application; PO, postoperative application; INT, intraoperative application
| Indication | No. of Wounds | Gap Size Range (cm) | Avg. no. of TopClosure® Sets Applied | Mode of Operation of TopClosure®* | TopClosure® Substituting for | Mean Treatment Duration (days) | Comments, Evaluation of Results & Complications |
|---|---|---|---|---|---|---|---|
| Scar secure | 8 | Indicated for scar secure | 1.25 | PO = 8 | Sutures/Staples/Tension sutures | 7.75 | Resulting in a fine scar, no need to replace the device |
| Skin tumors/Scars | 7 | 1.2–18 | 1.43 | PR = 6, INT = 2, PO = 6 | Heavy sutures/Tension sutures/Skin graft/Skin flap | 13.14 | Fine scar, minimizing the need for skin graft. One patient presented with blisters as a minor complication of TC treatment |
| Traumatic wounds | 3 | 2.5–5 | 1.67 | PR = 2, INT = 1, PO = 3 | Tension sutures/Skin graft/Skin flap | 27.33 | Fine scar |
| Fasciotomy | 2 | 4–6 | 1.5 | PO = 2 | Tension sutures/Skin graft/Skin flap | 15 | Closure of wound with fine scar on one side and complete skin graft take on the other |
| Infected post-operative wound | 1 | 15 | 1 | PO = 1 | Tension sutures/Re-operation | 37 | Fine scar |
| Total | 21 | – | – | – | – | – | – |
Noninvasive application
When used noninvasively, the TopClosure® 3S System APs are attached to the shaved dried skin surface on both sides of the lesion or wound by the adhesive on the undersurface of the plates. Once the plates are firmly adhered to the skin, the AS is inserted into the L/RMs of the plates, secured by the AS’s wings and locked by the L/R/M, and then gradually tightened to enable skin stretching. Additional drape can be utilized to further secure the AP to the skin.
Invasive application
In most trauma circumstances, TopClosure® may have to be secured to the skin by invasive means. Once the APs are firmly adhered to the skin, the attachment can be further secured by staples or sutures using the designated pairs of oval openings on each plate. The AS is then inserted into the L/RMs of the plates and tightened gradually to enable skin stretching. When applied invasively in conjunction with KW, once the APs are attached to the skin, a 1.8- or 1.6-mm KW is inserted through the wound’s edges into the designated horizontal opening across the proximal base of the AP and then back into the skin. Additional staples or sutures may be applied when indicated. The AS is then inserted into the L/RMs of the plates and tightened gradually to allow skin stretching.
Measurement of stress implication by sutures and TopClosure®
In our laboratory, we measured the force needed to tear nylon sutures of different diameters and the force needed to detach the AP from the skin using an electronic tension scale.
Results
After measuring, we calculated the stress inflicted on the skin by sutures and the shear stress imposed on the skin by the AP. Tables 2 and 3 describe the stress inflicted by various diameter nylon sutures (Dermalon®, monofilament nylon) and by the AP when applying the maximal possible forces (tear of sutures, detachment of AP and collapse of L/RM), and the force commonly used in clinical application, respectively.
Table 2.
Maximal stresses that can be inflicted on the skin by sutures at their tearing force by the AP at its detachment shear stress* from the skin and at the collapse of L/RM at 2.9 kg
| Suture type | Suture diameter (mm) | Tearing force (kg) | Maximal (normal/shear*) stress (kg/mm2) |
|---|---|---|---|
| 6/0 | 0.07 | 0.873 | 6.24 |
| 5/0 | 0.1 | 1.75 | 8.75 |
| 4/0 | 0.15 | 2.6 | 8.67 |
| 3/0 | 0.2 | 4.063 | 10.16 |
| 2/0 | 0.3 | >8.8 | 14.67 |
| TopClosure® 3S System | At a maximal detaching force of 8 kg | 0.008* | |
| TopClosure® 3S System | At a detaching force of 2.9 kg | 0.0029* | |
Table 3.
Stress inflicted by various sutures and shear stress* imposed on the skin by AP at a clinical application of 0.8 kg
| Suture type | Suture diameter (mm) | Maximal (normal/shear*) stress (kg/mm2) |
|---|---|---|
| 5/0 | 0.1 | 4.00 |
| 4/0 | 0.15 | 2.67 |
| 3/0 | 0.2 | 2.00 |
| 2/0 | 0.3 | 1.33 |
| TopClosure® 3S System | 0.0008* | |
Case presentations
Case 1
A 62-year-old man presented with a 3 × 2 cm oval squamous cell carcinoma (SCC) of the left distal leg (Fig. 3a). As the defect after excision of the tumor was expected to be too big to be closed primarily, and in order to avoid skin grafting, the TopClosure® 3S System was applied in a noninvasive manner for gradual stretching of the skin for 16 days until sufficient skin laxity was achieved to enable surgical resection of the lesion with primary closure (Fig. 3b). Preoperative skin stretching enabled complete excision of the tumor and primary edge-to-edge wound closure in layers with sutures and staples. Because the skin defect still required closure under relatively high tension, the TopClosure® 3S System was applied over the dressed closed wound and tightened with minimal force in order to secure wound closure by reducing tension on the suture line (Fig. 3c, d). The patient was only confirmed to bed for one postoperative day and could fully ambulate with the attached TopClosure® 3S System during the rest of the preoperative and postoperative periods. Figure 3e shows complete wound closure with a satisfactory aesthetic scar.
Fig. 3.

a SCC of the left distal leg. b The TopClosure® 3S System was applied in a noninvasive manner. c-d Following surgery, the TopClosure® 3S System was applied over the dressings to relieve tension and secure wound closure. e Complete wound closure with satisfactory aesthetic scar
Case 2
A 52-year-old woman with a depressed lower abdominal scar following TRAM breast reconstruction requested revision of the scar (Fig. 4a). The TopClosure® 3S System was applied noninvasively prior to surgery in order to stretch the skin to avoid excessive tension on the newly formed scar. Two 8-mm TopClosure® 3S Systems were positioned at the edge of the 7 × 8 cm depressed scar (Fig. 4b). In an attempt to reach a quick approximation, minimal blistering was observed on the underlying skin of the distal ends of the AP (Fig. 4c). This required removal of the systems only 2 days following application and attachment of another system at an alternative, adjacent site. Skin was now stretched by gradual approximation of the plates from 7 to 0.5 cm over a 5-day period. During surgery, the scar was excised and wound edges were sutured in layers. Gauze was placed over the wound with two 8-mm TopClosure® 3S Systems positioned across the incision edges for an additional 6-day period to support and secure closure, relieving tension from the wound’s edges, thus enhancing the aesthetics of the scar (Fig. 4d). The blisters at the attachment site were treated topically, resulting in no residual marks. Figure 4e shows complete wound closure with a satisfactory aesthetic scar.
Fig. 4.

a Depressed lower abdominal scar following TRAM breast reconstruction. b The TopClosure® 3S System was applied noninvasively prior to surgery. c Minimal blistering was observed and treated topically. During surgery, the scar was excised and wound edges were sutured in layers. d Gauze was placed over the wound with two 8-mm TopClosure® 3S Systems for an additional 6-day period. e Complete wound closure with satisfactory aesthetic scar
Case 3
A 26-year-old male patient sustained a fourth-degree high-voltage electric burn with severe soft tissue damage to his left lower limb. Following demarcation of the necrotic tissue at high left leg level, a below-knee amputation was performed. Wound edges were sutured in layers and stapled (Fig. 5a + c). Two 8-mm TopClosure® 3S Systems were attached invasively to the skin by staples, 3 cm from the wound edges as substitute to tension sutures (Fig. 5b, c). Gauze was placed over the wound, and the ASs were then inserted into the L/RMs and lightly tightened to support and secure closure by relieving the tension from the wound edges and distributing the stress away from the scar (Fig. 5d). The wound was topically treated periodically by temporary removal of the ASs and reapplying them after dressing change. The postoperative period was uneventful and the wound healed well (Fig. 5e).
Fig. 5.

a + c Wound edges were sutured in layers and stapled. b, c Two 8-mm TopClosure® 3S Systems were invasively attached to the skin by staples. d Gauze was placed over the wound, and the ASs were then inserted into the L/RMs and tightened lightly. e The postoperative period was uneventful, and the wound healed well
Case 4
A 12-year-old girl presented with a congenital nevus on her right thigh (Fig. 6a). As excessive tension was expected with direct primary closure, TopClosure® (6 mm) was applied 5 days prior to excision and was gradually stretched daily (Fig. 6b). Following application of topical anesthesia, the lesion was excised and closed in layers under tension (Fig. 6c–e). In order to secure the wound closure and to improve the aesthetics of the scar, TopClosure® was applied for an additional 2 weeks following surgery (Fig. 6f, g), resulting in a narrow aesthetically pleasing scar (Fig. 6h).
Fig. 6.

a A 12-year-old girl presented with a big congenital nevus on her right thigh. b TopClosure® (6 mm) was applied 5 days prior to excision. c–e The lesion was excised and closed in layers under tension. f, g TopClosure® was applied to secure wound closure for an additional 2 weeks following surgery. h The wound healed well, resulting in a narrow aesthetically pleasing scar
Case 5: infected surgical wound following gynecological surgery
A 29-year-old woman presented with a dehisced, infected, abdominal surgical wound following dilatation and curettage for a missed abortion that was complicated by acute massive retroperitoneal hemorrhage (Fig. 7a). The wound was treated by combined regulated negative pressure-assisted wound therapy (RNPT) and an 8-mm TopClosure® 3S System that was used to approximate wound edges (Fig. 7b, c). Wound dressings were changed every third day by releasing the AS, cleansing the wound and applying the RNPT again. The TopClosure® 3S System was attached to the skin by staples and could be cleaned together with the wound with every change of dressing (Fig. 7d, e). As the patient refused additional surgery to close the wound, further treatment was provided in the outpatient clinic. The wound was closed by approximation of the wound edges by the TopClosure® 3S System with a final acceptable result (Fig. 7f).
Fig. 7.
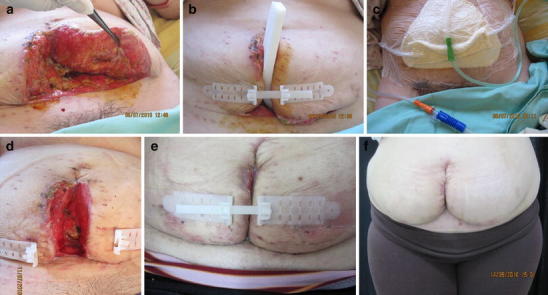
a A 29-year-old woman presented with a dehisced, infected, surgical wound following dilatation and curettage for a missed abortion that was complicated by acute massive retroperitoneal hemorrhage. b, c The wound was treated by RNPT and an 8-mm TopClosure® 3S System that was fixed to the skin by staples and used to approximate wound edges. d, e The TopClosure® 3S System could be cleaned together with the wound with every change of dressing. f The wound was closed by approximation of the wound edges by the TopClosure® 3S System, with a final acceptable result
Case 6: removal of SCC from an elderly woman with aging skin
An 88-year-old woman presented with a relatively large oval SCC (2.5 cm in diameter) of the left distal leg (Fig. 8a). As the defect after excision of the tumor was expected to be too large to be closed primarily and in order to avoid skin grafting, two 8-mm TopClosure® 3S Systems were applied in a noninvasive manner for gradual stretching of the skin over a period of 12 days until the sufficient skin laxity was achieved to enable surgical resection of the lesion with primary closure (Fig. 8b). During surgery, the patient underwent cyclical skin stretching using the TopClosure® 3S Systems for 2-min skin stretching followed by 1-min relaxation, for about 30 min. Preoperative and intraoperative skin stretching enabled complete excision of the tumor and primary edge-to-edge wound closure in layers, under tension with sutures and staples (Fig. 8c). Two TopClosure® 3S Systems were applied over the dressing for two days. The patient was only confined to bed for two postoperative days and could fully ambulate with the attached TopClosure® 3S Systems during the rest of the preoperative and postoperative periods. Figure 8d shows complete wound closure.
Fig. 8.

a An 88-year-old woman presented with a relatively large oval SCC of the left distal leg. b Two 8-mm TopClosure® 3S Systems were applied in a noninvasive manner for gradual stretching of the skin for 12 days until skin laxity was achieved to enable surgical resection of the lesion with primary closure. c Preoperative and intraoperative cyclical skin stretching enabled complete excision of the tumor and primary edge-to-edge wound closure in layers under tension. d Complete wound closure about 6 months following surgery
Discussion
Mechanism of action
The TopClosure® 3S System has been designed and applied to harness the viscoelastic properties of the skin by both mechanical creep and stress-relaxation principles in both noninvasive and invasive manners. The mechanical creep properties of the skin were utilized by preoperative continuous skin stretching for skin lesion removal. TopClosure® was also useful in acute skin stretching by stress relaxation through intraoperative, invasive, cyclical skin elongation and for postoperative invasive or noninvasive scar tension release to secure wound closure.
At the core of the new concept applied by the TopClosure® 3S System is the distribution of forces needed to stretch the skin on a relatively wide area of adherence, away from the traumatized wound edges, using selective vector-oriented forces. TopClosure’s strong topical adherence to the underlying skin enables the application of significant pull to the skin with relatively minimal tangential shear stress, avoiding pain and excessive skin damage. The applied local tangential force needed to detach the TopClosure® 3S System’s AP from the skin was measured in our laboratory to be 8 kg, and shear stress was calculated to be applied for suturing and at the AP (Table 3), indicating the 0.0008 kg/mm2. Although specific modulation factors should be applied when comparing detachment shear stress of the AP to the normal stress inflicted on tissues by sutures, the magnitude of order of these shear stress is in the range of 10−3–10−5 times the maximal stress that can be inflicted to the skin by the various nylon sutures, indicating a substantial difference in the stress applied to tissue by the TopClosure® 3S System compared with sutures (Table 2). About the same difference in magnitude of order (10−3–10−5) was determined for the shear stress and normal stress when 0.8 kg was applied for suturing and for pull on the AP (Table 3), indicating the advantage of the use of this system in relieving scar tension.
Application of mechanical creep for skin stretching
Experimental studies of tissue stretching by expansion over the course of a few weeks revealed histological changes in soft tissue during gradual expansion [17–22]. Qualitative microscopic analysis of the skin covering the tissue expander revealed a rapid thinning of the dermis and the panniculus carnosus muscle, mainly in the first 2 weeks, with no significant change in the epidermis. More compact and larger bundles of collagen fibers were observed in the thinned expanded dermis [23].
The TopClosure® 3S Systems can, in many instances, replace tissue expanders by using gradual and slow skin stretching paced over a few days to several weeks (Table 1; Fig 6a–h). When indicated for scar or tumor removal, an integrated constant force over time is expected to affect the skin in a manner similar to tissue expanders. This is achieved by utilizing the mechanical creep properties of tissues but with much more flexible distance, close to and/or distant from the lesion’s edges. TopClosure® can be applied to stretch skin in various body sites and in multidirectional, multiforce vectors, more specifically applied to affect the needed stretch direction, for skin relaxation, elongation and expansion. The TopClosure® 3S System has been applied in clinical cases for noninvasive preoperative treatment, replacing tissue expanders.
Application of stress relaxation for skin stretching
Stress relaxation is another biomechanical property of soft tissue behavior which describes the time-dependent decay of stress as the applied strain is held constant. The quasilinear viscoelastic constitutive model is one of the methods of characterizing stress relaxation behavior of skin. Stress relaxation allows skin to stretch intraoperatively beyond its inherent extensibility in a short period of time. As a result of skin stretching, wound closing tension decreases over time, allowing primary closure of relatively large defects [24]. Load cycling of skin implies an incremental increase in the length of the skin [25].
It has been shown that cyclical stretching of the skin can result in biochemical changes within a short period of time. Ryan’s [26] research manifests an immunohistochemical analysis for epidermal proliferation, which showed a strong response to cyclical stretch as soon as one hour following stimulation, and significantly greater EGF elevation occurred in the cyclical stretch group. These results support previous suggestions that cyclical force is preferable for stimulating growth than static force.
In this research, Ryan [26] indicates that an increased vascularity during pulsed tissue expansion may be attributed to temporary hypoxia. The reverse transcriptase polymerase chain reaction analysis for HIF-1a, a known transcriptional factor for both hypoxia and angiogenesis that was done in this research, demonstrated an 11-fold increase two days after cyclical stretch. This robust response to cyclical stretch may be due to the repeated high-frequency stimulation of transient hypoxia.
We learn that cyclically stretched skin led to increased tissue oxygenation and improved skin viability. Due to the structural composition of the skin, the resultant viscoelastic capability produces a unique mechanical behavior when subject to repeated mechanical loading. Preconditioning of skin, therefore, should be considered a necessary step toward optimal tissue stretching and elongation [27]. Such a procedure orients the molecular structure of the skin to its optimal in vivo alignment, allowing tissues to gradually adapt to loading, resulting in low-tension wound closure.
TopClosure® was applied during surgery to acutely, tangentially stretched skin over a period of 20–30 min, in intermittent, repetitive cycles of 3-min stretching, applying a constant strain (with force less than 2.7 kg) with an apparent period of tissue blanching (ischemia), followed by 1-min relaxation with capillary refilling (reperfusion). By using intermittent application of tension to the skin, this preconditioning multivector cyclic loading led to an incremental skin elongation through the stress relaxation mechanism, facilitating primary skin closure (case 6).
Application for wound secure
TopClosure® was applied following surgery where skin has been closed under relatively high tension to secure skin closure, to avoid dehiscence following pacemaker implantations and expanding hematomas, as well as to reduce tension on the scar and to improve scar aesthetics (Table 1; Figs. 3f, 6h, and 8d).
There is a significant advantage in the use of TopClosure® in the pediatric group of patients for revision of scars and for the excision of big congenital nevi by reducing the need for serial excisions as a substitute for tissue expanders and for the alleviation of pain when used noninvasively.
In trauma settings, TopClosure® enabled a selective distribution of a minimal load on the injured skin edges to meet its specific clinical condition (case 3). It is recommended that the least possible tension be applied to the injured skin, to position the APs away from wound edges or at various distances, and to adhere the APs to the underlying skin with staples or sutures to allow for thorough cleansing of the wound during and following surgery. TopClosure® is of special merit in surgery in those cases where a second look is indicated for exploration and treatment of wounds after primary surgery. AS can be detached by releasing the lever of the L/RM and can be reapplied if indicated.
Local skin irritation and blistering can be avoided by slow, gradual skin stretching in the noninvasive mode of preoperative skin stretching and by the application of minimal pull on the skin for post-operative wound securing. Topical skin irritation from the adherent glue could be easily detected under the semitransparent AP and could be treated early by releasing tension, topical cream and/or relocation of AP with the use of staples if indicated.
Summary
The TopClosure® 3S System is an innovative device, having been designed to harness the viscoelastic properties of the skin by both mechanical creep and stress relaxation principles. Application of TopClosure® can be utilized to modify and improve the current practice of wound closure by enabling preconditioning of the skin to gradually adapt to loading, applying minimal stress to the skin away from the damaged wound edges, using flexible, multidirectional force vectors and versatile methods of attachment to the skin, using either a noninvasive or invasive method of skin stretching, elongation, securing wound edges, and improved scar aesthetics.
Acknowledgments
Disclosure
Dr. Topaz is one of the developers of TopClosure® and is the chairperson of I.V.T. Medical Ltd., manufacturer of the device.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution and reproduction in any medium, provided the original author(s) and source are credited.
Contributor Information
Moris Topaz, Phone: +972-9-7463737, FAX: +972-9-7604506, Email: topazmd@netvision.net.il.
Ming Sen Li, Email: lms_1963@163.com.
Yong Zhong Li, Email: laofu62@qq.com.
References
- 1.Reichelt J. Mechanotransduction of keratinocytes in culture and in the epidermis. Eur J Cell Biol. 2007;86:807–816. doi: 10.1016/j.ejcb.2007.06.004. [DOI] [PubMed] [Google Scholar]
- 2.Gormar FE, Bernd A, Bereiter-Hahn J, Holzmann H. A new model of epidermal differentiation: induction by mechanical stimulation. Arch Dermatol Res. 1990;282:22–32. doi: 10.1007/BF00505641. [DOI] [PubMed] [Google Scholar]
- 3.Nasca MR, Shih AT, West PD, Martinez WM, Micali G, Landsman AS. Intermittent pressure decreases human keratinocyte proliferation in vitro. Skin Pharmacol Physiol. 2007;20:305–312. doi: 10.1159/000108146. [DOI] [PubMed] [Google Scholar]
- 4.Ryan TJ. Biochemical consequences of mechanical forces generated by distention and distortion. J Am Acad Dermatol. 1998;21:115–130. doi: 10.1016/S0190-9622(89)70156-0. [DOI] [PubMed] [Google Scholar]
- 5.Chin MS, Ogawa R, Lancerotto L, Pietramaggiori G, Schomacker KT, Mathews JC, Scherer SS, Van Duyn P, Prsa MJ, Ottensmeyer MP, Veves A, Orgill DP. In vivo acceleration of skin growth using a servo-controlled stretching device. Tissue Eng Pt C-Meth. 2010;16(3):397–405. doi: 10.1089/ten.tec.2009.0185. [DOI] [PubMed] [Google Scholar]
- 6.Ryan TJ. Biochemical consequences of mechanical forces generated by distention and distortion. J Am Acad Dermatol. 1989;21(1):115–30. doi: 10.1016/S0190-9622(89)70156-0. [DOI] [PubMed] [Google Scholar]
- 7.Renò F, Traina V, Cannas M. Mechanical stretching modulates growth direction and MMP-9 release in human keratinocyte monolayer. Cell Adh Migr. 2009;3(3):239–242. doi: 10.4161/cam.3.3.8632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Woo SLY, Gomez MA, Akeson WH. The time and history-dependent viscoelastic properties of the canine viscoelastic characteristics, which could be a result of fluid flow and/or structural medial collateral ligament. J Biomech Eng. 1981;103:293–298. doi: 10.1115/1.3138295. [DOI] [PubMed] [Google Scholar]
- 9.Purslow PP, Wess TJ, Hukins DWL. Collagen orientation and molecular spacing during creep and stress-relaxation in soft connective tissues. J Exp Biol. 1998;201:135–142. doi: 10.1242/jeb.201.1.135. [DOI] [PubMed] [Google Scholar]
- 10.Hsu S, Jamieson AM, Blackwell AM. Viscoelastic studies of extracellular matrix interactions in a model native collagen gel system. Biorheology. 1994;31:21–36. doi: 10.3233/bir-1994-31103. [DOI] [PubMed] [Google Scholar]
- 11.Elsner P, Wilhelm KP, Maibach HI, Berardesca E. Bioengineering of the skin: skin biomechanics. New York: CRC Press; 2001. [Google Scholar]
- 12.Wainwright SA, Biggs WD, Currey JD, Gosline JM. Mechanical design in organisms. London: Edward Arnold; 1976. [Google Scholar]
- 13.Liang MD, Briggs P, Heckler FR, Futrell JW. Presuturing—a new technique for closing large skin defects: clinical and experimental studies. Plast Reconstr Surg. 1988;81(5):694–702. doi: 10.1097/00006534-198805000-00008. [DOI] [PubMed] [Google Scholar]
- 14.Hirshowitz B, Lindenbaum E, Har-Shai Y. A skin-stretching device for harnessing of the viscoelastic properties of the skin. Plast Reconstr Surg. 1993;92:260. doi: 10.1097/00006534-199308000-00010. [DOI] [PubMed] [Google Scholar]
- 15.Marek DJ, Copeland GE, Ziowodzki M, Cole PA. The application of dermatotraction for primary skin closure. Am J Surg. 2005;190:123–126. doi: 10.1016/j.amjsurg.2005.05.038. [DOI] [PubMed] [Google Scholar]
- 16.Abramson DL, Gibstein LA, Pribaz JJ. An inexpensive method of intraoperative skin stretching for closure of large cutaneous wounds. Ann Plast Surg. 1997;38:540–542. doi: 10.1097/00000637-199705000-00019. [DOI] [PubMed] [Google Scholar]
- 17.Austad ED, Pasyk KA, McClatchey KD, Cherry GW. Histomorphologic evaluation of guinea pig skin and soft tissue after controlled tissue expansion. Plast Reconstr Surg. 1982;70(6):704–710. doi: 10.1097/00006534-198212000-00008. [DOI] [PubMed] [Google Scholar]
- 18.Timmenga EJ, Schoorl R, Klopper PJ. Biomechanical and histomorphological changes in expanded rabbit skin. Br J Plast Surg. 1990;43(1):101–106. doi: 10.1016/0007-1226(90)90052-2. [DOI] [PubMed] [Google Scholar]
- 19.Pasyk KA, Austad ED, McClatchey KD, Cherry GW. Electron microscopic evaluation of guinea pig skin and soft tissues “expanded” with a self-inflating silicone implant. Plast Reconstr Surg. 1982;70(1):37–45. doi: 10.1097/00006534-198207000-00008. [DOI] [PubMed] [Google Scholar]
- 20.Wee SS, Logan SE, Mustoe TA. Continuous versus intraoperative expansion in the pig model. Plast Reconstr Surg. 1992;90(5):808–814. doi: 10.1097/00006534-199211000-00012. [DOI] [PubMed] [Google Scholar]
- 21.Johnson TM, Kowe L, Brown MD, Sullivan MJ, Nelson BR. Histology and physiology of tissue expansion. J Dermatol Surg Oncol. 1993;19:1074. doi: 10.1111/j.1524-4725.1993.tb01002.x. [DOI] [PubMed] [Google Scholar]
- 22.Kim KH, Hong C, Futrell JW. Histomorphologic changes in expanded skeletal muscle in rats. Plast Reconstr Surg. 1993;92(4):710–716. doi: 10.1097/00006534-199309001-00022. [DOI] [PubMed] [Google Scholar]
- 23.Pasyk KA, Austad ED, McClatchey KD, Cherry GW. Electron microscopic evaluation of guinea pig skin and soft tissues “expanded” with a self-inflating silicone implant. Plast Reconstr Surg. 1982;70(1):37–45. doi: 10.1097/00006534-198207000-00008. [DOI] [PubMed] [Google Scholar]
- 24.Marek DJ, Copeland GE, Ziowodzki M, Cole PA. The application of dermatotraction for primary skin closure. Am J Surg. 2005;190:123–126. doi: 10.1016/j.amjsurg.2005.05.038. [DOI] [PubMed] [Google Scholar]
- 25.Melis P, Noorlander ML. Rapid alignment of collagen fibers in the dermis of undermined and not undermined skin stretched with a skin-stretching device. Plast Reconstr Surg. 2002;109(2):674–680. doi: 10.1097/00006534-200202000-00038. [DOI] [PubMed] [Google Scholar]
- 26.Ryan TJ. Biochemical consequences of mechanical forces generated by distention and distortion. J Am Acad Dermatol. 1998;21:115–130. doi: 10.1016/S0190-9622(89)70156-0. [DOI] [PubMed] [Google Scholar]
- 27.Liu Z, Yeung K. The preconditioning and stress relaxation of skin tissue. J Biomech Eng. 2008;2(1):22–28. [Google Scholar]