

Abstract
Background. Many insurance companies require obese patients to lose weight prior to gastric bypass. From a previous study by the same authors, preoperative weight at surgery is strongly predictive of weight loss up to one year after surgery. This review aims to determine whether preoperative weight loss is also correlated with weight loss up to one year after surgery. Methods. Of the 186 results screened using PubMed, 12 studies were identified. A meta-analysis was performed to further classify studies (A class, B class, regression, and rejected). Results. Of all 12 studies, one met the criteria for A class, six were B class, four were regression, and one was rejected. Six studies supported our hypothesis, five were inconclusive, and no study refuted. Conclusions. Preoperative weight loss is additive to postsurgery weight loss as predicted from the weight at the time of surgery.
1. Introduction
According to the latest statistics, one out of every three adults (33.8%) in US is obese. Additionally, the rate of morbid obesity is 5.7% in adults [1]. Bariatric surgery is a very effective intervention for the morbidly obese. More than 220,000 people underwent some form of bariatric surgery in 2008 [2]. Age, gender, race, height, initial body weight, postoperative behaviors, type of operation, and surgeon have been reported to affect weight loss following surgery. However, no consideration of factors impacting weight loss outcomes would be complete without attention to the importance of preoperative weight loss. Although the California Department of Managed Care explicitly states that “there is no literature presented by any authority that mandated weight loss, once a patient has been identified as a candidate for bariatric surgery, is indicated,” yet the majority of insurance payers continue to require prolonged dietary efforts as a prerequisite to surgical treatment [3]. A reduction in the size of the liver after four weeks of dieting and an increase in ease of surgical exposure are well documented [4, 5]. The impact on overall weight loss is less clear. Numerous papers dealing with the subject provide an array of experimental models that make a comparison of results difficult. Our paper evaluates the existing publications and separates them into four groups for comparison.
In a previous publication, we showed that weight loss in the first year after gastric bypass is a percent of initial body weight [6]. The following review attempts to determine the effect of short-term preoperative weight loss on weight loss following surgery and the effect of initial body weight.
2. Methods
The study was done using PubMed search for those papers which dealt with aspects of preoperative weight loss before bariatric surgery. The search terms used were (“preoperative weight loss” or “pre-operative weight loss” or “preoperative weight” or “pre-operative weight”) and (“gastric bypass” (meSH) or “bariatric surgery” (meSH) or “obesity surgery” or “weight reduction surgery” or “predicting”).
Each abstract was analyzed to include only those studies which satisfied all set criteria. Criteria for abstract review were as follows. All studies reviewed were from a peer-reviewed source and published either in English or Spanish. Studies were required to have one of the following designs: randomized control trials, case control studies, or series/cohort studies. Additionally, the majority of study participants had to be greater than 18 years old. Accepted abstracts included both open and laparoscopic cases.
Articles were obtained for the remaining abstracts and were further analyzed. Each article was expected to have more than ten patients in each group of study (preoperative weight loss versus weight gain) or >20 patients in a regression analysis. Information on pre/post-operation weight loss had to be available for article selection. Papers were also excluded that did not stratify the data such that gastric bypass weight loss results were separated from alternate weight loss procedures such as gastric banding or sleeve gastrectomy (Figure 1). The selected studies were further searched for their references to identify more papers pertaining to our study.
Figure 1.

Diagram representing the inclusion and exclusion of PubMed search results.
The selected studies were divided into different classes: class A, class B, and regression studies. The classification was based on the patient's weight at initial consultation and the weight at surgery. Both class A and class B studies grouped patients into two follow-up cohorts, one that lost weight and the other that did not.
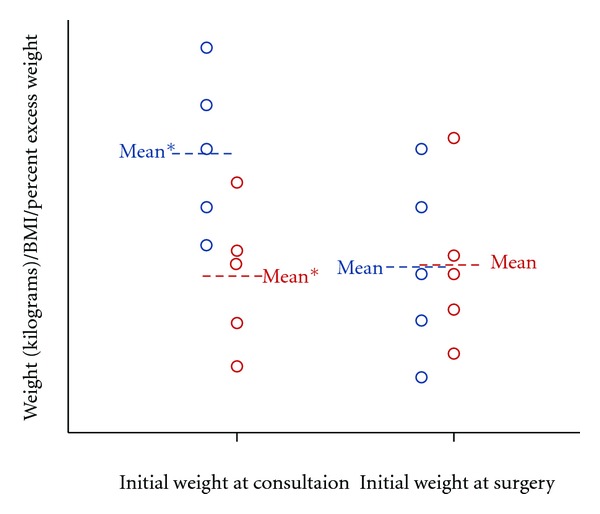
In class A studies, the weight loss and weight gain groups both had the same mean weight at initial consultation but different at the time they went for surgery. This is demonstrated in Figure 2 by using two groups with five hypothetical patients in each group. Both groups initially begin with similar mean weights and differ directly prior to surgery with different average weights (confidence interval 95%).
Figure 2.

Example of Class A study. Graph showing ten hypothetical patients in Class A study that have been divided into weight loss (blue) and weight gain (red) groups. The weight loss group was statistically different from the weight gain group at surgery. *Confidence Interval 95%.
2.1. Class A Study Supporting/Refuting Criteria
Studies were deemed to support our hypothesis if both groups of patients had a persistent statistical difference in the average weight within the first 12 months, and the mean weight values did not crossover in this time frame. Refuting studies would have crossing over of the means (e.g., the weight loss group having a higher mean weight after surgery at six months than the weight gain group). Inconclusive studies lacked 50% followup during the first year or proper notation to elicit a definitive conclusion.
In class B studies weight loss and weight gain groups had different mean weights (P < 0.05) at initial consultation but similar means at the time of surgery. This is demonstrated in Figure 3 by using two groups with five hypothetical patients in each who begin with different weights at initial consultation but eventually enter the surgery with similar mean weights.
Figure 3.
Example of class B study. Graph showing ten hypothetical patients in class B study who have been divided into weight loss (blue) and weight gain (red) groups. The weight loss group was statistically different from the weight gain group at initial consultation. *Confidence interval 95%.
2.2. Class B Study Supporting/Refuting Criteria
Studies were deemed to support our hypothesis if both groups of patients did not have any statistical difference in their mean weight for the first 12 months. Refuting studies would have a statistically different differences between the weight loss and weight gain group. Inconclusive studies lacked 50% followup during the first year or proper notation to elicit a definitive conclusion.
2.3. Regression Studies
Regression studies do not have to utilize groups of patients and may look at preoperative weight loss as a variable. In regression studies the patients are no longer grouped into weight loss/gain groups or dieters/nondieters groups. The focus is on individual performance of each patient. The following concept has been explained by using six hypothetical patients who undergo gastric bypass surgery (P1, P2, P3, P4, P5, and P6). Each of these hypothetical patients had different amounts of preoperative weight loss with the exception of one patient who did not lose or gain weight.
The preoperative weight loss is considered to be a continuous variable and can be plotted on the x-axis (Figure 4). The outcome is also a continuous variable percent of initial weight loss, plotted on y-axis (Figure 5) for a period of one year after surgery. For explanation and standardization, we use percent of initial weight at surgery as the outcome for y-axis.
Figure 4.

Example of regression. Study includes six hypothetical patients who lost weight preoperatively. The preoperative weight loss is graphed against their complete program weight loss (from initial consultation to one year after operation).
Figure 5.

Flow chart depicting the classification of the selected studies into Class A, B, and regression studies. WL: weight loss; WG: weight gain.
2.4. Regression Study Supporting/Refuting Criteria
Regression studies were judged based on the variables included and the results reported by the authors. Analysis was hampered due to absence of data or modeling protocol. Inconclusive studies were defined as <50% followup or too complex for us to interpret without additional input from the author.
Classification of studies was required to define criteria needed to support and refute our hypothesis.
A flow chart used to arrive at the chosen classification is provided in Figure 5.
3. Results
3.1. Class A Studies
The study by Solomon et al. [7] and Alami et al. [19] was a randomized control trial conducted at Stanford Medical University. The study was done for a year comparing postoperative weights between two groups, one which lost weight preoperatively and other which gained weight. The statistical difference between both groups was maintained up to 3 months. At one year, the patients in both arms of the study showed no difference in excess weight loss. But when patients were divided according to those who had lost at least five percent of their excess body weight preoperatively, the one-year results for excess weight loss were much lower for the weight-loss group. This class-A study shows that weight loss is a percent of initial body weight at the time of surgery (Table 1).
Table 1.
Class A studies.
| Lead author | Study design | Group | Patients | Mean age (yr) | Female (%) | Results |
|---|---|---|---|---|---|---|
| Solomon [7] | RCT | WL | 26 | 42.4 | 88.5% | Supportive |
| WG | 35 | 44.9 | 80.0% |
WL: weight loss; WG: weight gain; RCT: randomized controlled trial.
3.2. Class B Studies
In the study by Martin et al. [8], the subjects were divided into dieters and nondieters. Here, also the data show that weight loss after surgery is a percent of body weight at the time of surgery. The only statistically significant difference in mean weight between the two groups was at initial presentation (Table 2). The study by Still et al. [9] was done at Geisinger Medical Center in Danville, Pennsylvania. This study was considered inconclusive because its postoperative assessment was carried out in percentages of patients meeting their weight loss goal as opposed to actual weight values making analysis difficult.
Table 2.
Class B studies.
| Lead author | Study design | Group | Patients | Mean age | Female (%) | Results |
|---|---|---|---|---|---|---|
| Martin [8] | Prospective | WL (dieters) | 47 | 40.2 | 74.5% | Supportive |
| WG (nondiet) | 53 | 38.8 | 92.5% | |||
|
| ||||||
| Still [9] | Prospective | 5–10% EBWL | 67 | 43 | 77.6% | Inconclusive |
| 5% EBWL | 86 | 43 | 74.4% | |||
| 0–5% EBWG | 137 | 43 | 78.8% | |||
| >5% EBWG | 169 | 45 | 79.9% | |||
|
| ||||||
| Ali [10] | Retrospective | WL > 10% TBW | 23 | 42.7 | 73.9% | Supportive |
| WL 5–10% TBW | 102 | 43 | 87.3% | |||
| WL 0–5% TBW | 135 | 42.8 | 95.5% | |||
| WG % TBW | 91 | 42.1 | 96.7% | |||
|
| ||||||
| Fujioka [11] | Retrospective | WL (>0 lbs) | 55 | 49 | 80.0% | Supportive |
| WG (<0 lbs) | 66 | 48 | 86.4% | |||
|
| ||||||
| Harnisch [12] | Retrospective | WL (≥10 lbs) | 88 | 44 | 84.1% | Supportive |
| WG (≥10 lbs) | 115 | 41.4 | 85.2% | |||
|
| ||||||
| Huerta [13] | Retrospective | WL | 15 | 50 | 33.3% | Inconclusive |
| WG (non-WL) | 25 | 50 | 28.0% | |||
WL: weight loss; WG: weight gain; EBW: excess body weight; TBW: total body weight.
Ali et al. [10] had 351 subjects who were divided into 4 groups based on the percent EWL (excess weight loss). At surgery, no significant differences were found among the 4 groups in total body weight and BMI or EBW except for a BMI difference in group 1 and 3. At 6 and 12 months, no significant difference was found in the total body weight or BMI among the 4 groups indicating again that weight loss is a function of weight at the time of surgery (Table 2).
The study by Fujioka et al. [11] divided the patients into two groups based on whether patients lost or gained weight preoperatively. Both groups had similar mean weights at surgery. When these patients were followed after surgery, no significant differences in the mean EWL were found at any follow-up point in the first 12 months thus supporting our hypothesis. Harnish's et al. [12] study also had similar structure and findings to that of Fujioka (Table 2).
The B class study by Huerta et al. [13] was considered inconclusive as the followup was less than 50% during the first year and only had postoperative data for the second and fourth years after surgery.
3.3. Regression Studies
The study by Alger-Mayer et al. [16], which was done at Albany, NY, was analyzed using regression. Even though the year 3 and 4 results supported our hypothesis, the results were considered inconclusive because the paper lacked postoperative data in the first year after gastric bypass.
The study by Jantz et al. [14] was inconclusive because they were not looking at immediate preoperative weight loss.
Carlin et al. [17] published a paper that changed weight loss requirements based on the initial BMI. Those individuals that had BMI greater than 60 had to lose more than those that were less than 50 kg/m2. Thus, the study was considered inconclusive due to difficulty interpreting the methodology.
The study by Alvarado et al. [15] identified a 1.8% increase in the % EWL one year after gastric bypass with each 1% total body weight lost preoperatively. This retrospective study was considered supportive due to the positive effect preoperative weight loss would have on postoperative weight loss in the absence of controlling for initial weight at surgery. Results are summarized in Table 3.
Table 3.
Regression studies.
| Lead author | Study design | Patients | Mean age | Operation type | Female (%) | Results |
|---|---|---|---|---|---|---|
| Jantz [14] | Retrospective | 384 | 43.3 | LRYGB | 82.5 | Inconclusive |
| Alvarado [15] | Retrospective | 90 | 42 | LRYGB | 90 | Supportive |
| Sharon Alger [16] | Prospective | 150 | 45.3 | RYGB* | 80 | Inconclusive |
| Carlin [17] | Retrospective | 295 | 45 | LRYGB | 88.8 | Inconclusive |
LRYGB: laparoscopic roux-en-y gastric bypass; *RYGB: Roux en Y Gastric Bypass. the roux-en-y gastric bypass was an open procedure.
3.4. Rejected Studies
The study by Riess et al. [18] was rejected as a study because the weight loss group and the weight gain group had statistically significant difference in mean weight at both initial consultation and the time before surgery. The difference was preserved postoperatively (see Table 4).
Table 4.
Rejected Studies
| Lead author | Study design | Group | Patients | Age | Female (%) |
|---|---|---|---|---|---|
| Riess et al. [18] | Retrospective | WL | 74 | 43.4 | 70.3% |
| WG (non-WL) | 279 | 42.7 | 86.4% |
WL: weight loss; WG: weight gain.
4. Discussion
Our study found that weight at the time of surgery, rather than the amount of weight lost preoperatively, determines the weight loss outcome postoperatively. Stated differently, weight at a given time period after surgery is the same percent of initial body weight independent of starting weight. For example, if a patient weighs 160 kg at the time of surgery, he will weigh approximately 62% of that at one year after surgery or 100 kg. If he lost 22.5 kg preoperatively and weighed 136 kg at the time of surgery, he would weigh 62% of his initial body weight or 81.5 kg. His overall weight loss would be 13.5 kg greater for having lost 22.5 kg preoperatively. Since weight loss following gastric bypass tends to be negligible after one year, this probably represents a real gain. In this paper, we have detailed two classes of studies, A and B. Combining review data with previous work by Sczepaniak et al. [6], it is possible to create visual representation of both studies. Class A and class B studies are shown in Figures 2 and 3, respectively. Both groups changed in mean weight at initial consultation, one group gaining weight and the other losing weight. Preoperative weight gain and loss were arbitrarily set for explanation purposes. In a B class study it is observed that the means of both the weight loss and weight gain groups is not different for the first year.
With regards to regression study, in the six hypothetical patients, the relationship to preoperative weight loss can now be clearly seen from Figure 6. The more preoperative percent initial body weight loss (based on initial weight at surgery), the more the percent total body weight loss (calculated from subtracting percent total body weight at initial consultation from achieved percent total body weight after surgery), see Figure 6.
Figure 6.

Hypothetical regression model. This model demonstrates the effect of preoperative weight loss in gastric bypass patients.
From the graph on the hypothetical patients in Figure 4, it is now possible to see the benefit of losing preoperative weight on an individual level.
Our study has only dealt with studies having gastric bypass surgeries, but the preoperative weight loss might have a similar role in sleeve gastrectomy and sleeve plication (also current methods for weight reduction).
Losing weight leads to better outcomes because a patient entering surgery with a lower weight than someone entering surgery without weight loss will have more weight loss in total.
5. Conclusion
Our review of the literature supports the idea that weight loss after surgery for gastric bypass, and by extension other procedures as well, is a percent of initial body weight. Moreover, the literature is generally supportive of the idea that short-term preoperative weight loss is additive, that is, increases the total amount of weight lost.
Conflict of Interests
The authors have no commercial associations that might be a conflict of interest in relation to this paper.
Acknowledgments
The authors are grateful to San Diego University, CA; St. George's University Grenada, WI; Amit Kulkarni, MBBS—Mayo Clinic, Rochester; Adel Youssef MD, Gastroenterology Clinic,Warren, OH. They would also like to thank the many others who made this work possible.
References
- 1.Centers for disease control and prevention. Data from the National Health and Examination Survey (NHANES) 2007-2008.
- 2.American society for Metabolic and Bariatric Surgery Statistics. 2008.
- 3.Department of Managed Healthcare. California, http://www.dmhc.ca.gov.
- 4.Edholm D, Kullberg J, Haenni A, et al. Preoperative 4-week low-calorie diet reduces liver volume and intrahepatic fat, and facilitates laparoscopic gastric bypass in morbidly obese. Obesity Surgery. 2011;21(3):345–350. doi: 10.1007/s11695-010-0337-2. [DOI] [PubMed] [Google Scholar]
- 5.Lewis MC, Phillips ML, Slavotinek JP, Kow L, Thompson CH, Toouli J. Change in liver size and fat content after treatment with Optifast very low calorie diet. Obesity Surgery. 2006;16(6):697–701. doi: 10.1381/096089206777346682. [DOI] [PubMed] [Google Scholar]
- 6.Sczepaniak JohnP, Owens MiltonL, Garner William, et al. A SimplerMethod for PredictingWeight Loss in the First Year after Roux-en-Y Gastric Bypass. Journal of Obesity. 2012;2012:5 pages. doi: 10.1155/2012/195251. Article ID 195251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Solomon H, Liu GY, Alami R, Morton J, Curet MJ. Benefits to patients choosing preoperative weight loss in gastric bypass surgery: new results of a randomized trial. Journal of the American College of Surgeons. 2009;208(2):241–245. doi: 10.1016/j.jamcollsurg.2008.09.028. [DOI] [PubMed] [Google Scholar]
- 8.Martin LF, Tan TL, Holmes PA, Becker DA, Horn J, Bixler EO. Can morbidly obese patients safely lose weight preoperatively? The American Journal of Surgery. 1995;169(2):245–253. doi: 10.1016/s0002-9610(99)80145-7. [DOI] [PubMed] [Google Scholar]
- 9.Still CD, Benotti P, Wood GC, et al. Outcomes of preoperative weight loss in high-risk patients undergoing gastric bypass surgery. Archives of Surgery. 2007;142(10):994–998. doi: 10.1001/archsurg.142.10.994. [DOI] [PubMed] [Google Scholar]
- 10.Ali MR, Baucom-Pro S, Broderick-Villa GA, et al. Weight loss before gastric bypass: feasibility and effect on postoperative weight loss and weight loss maintenance. Surgery for Obesity and Related Diseases. 2007;3(5):515–520. doi: 10.1016/j.soard.2007.05.002. [DOI] [PubMed] [Google Scholar]
- 11.Fujioka K, Yan E, Wang HJ, Li Z. Evaluating preoperative weight loss, binge eating disorder, and sexual abuse history on Roux-en-Y gastric bypass outcome. Surgery for Obesity and Related Diseases. 2008;4(2):137–143. doi: 10.1016/j.soard.2008.01.005. [DOI] [PubMed] [Google Scholar]
- 12.Harnisch MC, Portenier DD, Pryor AD, Prince-Petersen R, Grant JP, DeMaria EJ. Preoperative weight gain does not predict failure of weight loss or co-morbidity resolution of laparoscopic Roux-en-Y gastric bypass for morbid obesity. Surgery for Obesity and Related Diseases. 2008;4(3):445–450. doi: 10.1016/j.soard.2007.09.016. [DOI] [PubMed] [Google Scholar]
- 13.Huerta S, Dredar S, Hayden E, et al. Preoperative weight loss decreases the operative time of gastric bypass at a veterans administration hospital. Obesity Surgery. 2008;18(5):508–512. doi: 10.1007/s11695-007-9334-5. [DOI] [PubMed] [Google Scholar]
- 14.Jantz EJ, Larson CJ, Mathiason MA, Kallies KJ, Kothari SN. Number of weight loss attempts and maximum weight loss before Roux-en-Y laparoscopic gastric bypass surgery are not predictive of postoperative weight loss. Surgery for Obesity and Related Diseases. 2009;5(2):208–211. doi: 10.1016/j.soard.2008.08.015. [DOI] [PubMed] [Google Scholar]
- 15.Alvarado R, Alami RS, Hsu G, et al. The impact of preoperative weight loss in patients undergoing laparoscopic Roux-en-Y gastric bypass. Obesity Surgery. 2005;15(9):1282–1286. doi: 10.1381/096089205774512429. [DOI] [PubMed] [Google Scholar]
- 16.Alger-Mayer S, Polimeni JM, Malone M. Preoperative weight loss as a predictor of long-term success following Roux-en-Y gastric bypass. Obesity Surgery. 2008;18(7):772–775. doi: 10.1007/s11695-008-9482-2. [DOI] [PubMed] [Google Scholar]
- 17.Carlin AM, O’Connor EA, Genaw JA, Kawar S. Preoperative weight loss is not a predictor of postoperative weight loss after laparoscopic Roux-en-Y gastric bypass. Surgery for Obesity and Related Diseases. 2008;4(4):481–485. doi: 10.1016/j.soard.2007.09.010. [DOI] [PubMed] [Google Scholar]
- 18.Riess KP, Baker MT, Lambert PJ, Mathiason MA, Kothari SN. Effect of preoperative weight loss on laparoscopic gastric bypass outcomes. Surgery for Obesity and Related Diseases. 2008;4(6):704–708. doi: 10.1016/j.soard.2008.05.007. [DOI] [PubMed] [Google Scholar]
- 19.Alami RS, Morton JM, Schuster R, et al. Is there a benefit to preoperative weight loss in gastric bypass patients? A prospective randomized trial. Surgery for Obesity and Related Diseases. 2007;3(2):141–145. doi: 10.1016/j.soard.2006.11.006. [DOI] [PubMed] [Google Scholar]