

Abstract
Background. In Traditional Chinese Medicine (TCM), most of the algorithms are used to solve problems of syndrome diagnosis that only focus on one syndrome, that is, single label learning. However, in clinical practice, patients may simultaneously have more than one syndrome, which has its own symptoms (signs). Methods. We employed a multilabel learning using the relevant feature for each label (REAL) algorithm to construct a syndrome diagnostic model for chronic gastritis (CG) in TCM. REAL combines feature selection methods to select the significant symptoms (signs) of CG. The method was tested on 919 patients using the standard scale. Results. The highest prediction accuracy was achieved when 20 features were selected. The features selected with the information gain were more consistent with the TCM theory. The lowest average accuracy was 54% using multi-label neural networks (BP-MLL), whereas the highest was 82% using REAL for constructing the diagnostic model. For coverage, hamming loss, and ranking loss, the values obtained using the REAL algorithm were the lowest at 0.160, 0.142, and 0.177, respectively. Conclusion. REAL extracts the relevant symptoms (signs) for each syndrome and improves its recognition accuracy. Moreover, the studies will provide a reference for constructing syndrome diagnostic models and guide clinical practice.
1. Introduction
Although Traditional Chinese Medicine (TCM) and Western Medicine diagnose cases in clinical applications, their theoretical systems are totally different. The hard targets such as laboratory and imaging tests are very important for diagnosing diseases in Western Medicine whereas soft targets are much more important in the clinical diagnosis of TCM.
The so-called soft targets [1] mainly refer to targets that cannot be accurately measured and with poor repeatability. These targets are subjective and are collected through clinical observation of a doctor or the patient's self-report, which cannot be accurately measured using instruments or directly through other means.
Therefore, collecting information in the diagnosis of TCM is difficult because it cannot be measured accurately, with poor measurement repeatability, and are easily influenced by the study sample and environmental factors.
Given that the soft targets of TCM are subjective, fuzzy, and multidimensional, TCM has been considered as a mystical experience in the scientific world and has not been identified in a wide range.
In recent years, the standardization and objectification of TCM diagnosis have gradually become a research hotspot with the development of mathematical statistics, data mining, and pattern recognition technology.
The studies are revealing the rules between syndromes and the information of four diagnosis: inspection, auscultation and olfaction, inquiring, and palpation, and seeking information of four diagnosis for differential diagnosis or extracting classification rules for syndrome differentiation. The research can provide a reference for clinical syndrome differentiation and reduce the subjectivity and ambiguity of diagnosis.
Some researchers have applied the structural equation model in studying chronic atrophic gastritis. The results show that chronic atrophic gastritis resulting from the most common syndromes correspond with diagnostic targets, which is agreement with the clinical practice of TCM [2]. An improved conjugate gradient learning algorithm is used to create the BP model with three layers for diabetes and nephropathy. The results show its advantages in predicting diabetes and nephropathy [3]. An entropy-based partition method for complex systems is applied to establish endothelial dysfunction diagnostic criteria for Yin deficiency syndrome. Moreover, the experimental results are highly consistent with the findings of clinical diagnosis [4]. Multilabel learning [5] combined with the frequency method is presented to select the symptoms that greatly contribute to coronary heart disease. The results show the improvement in the diagnosis of coronary heart disease. Su et al. [6] employed the correlation coefficient, similarity D, the angle cosine, and spectral similarity to study the correlation between the symptoms (signs) and the five syndromes of liver cirrhosis. The research can provide a basis for differentiating patients with nonspecific clinical manifestations.
Our research group focuses on the standardization and objectification of syndrome in TCM. We applied latent structure models [7] to study the association between symptoms of the spleen system. According to a social network theory, we used the associated density method [8, 9] to analyze the correlation between syndrome-syndrome of coronary heart disease and symptom-syndrome of chronic gastritis.
In the studies on syndrome standardization and objectification mentioned above, most of the algorithms were used to solve problems in diagnosing patients with disjoint syndromes, which belong to single-label learning. However, in clinical practice, strong relevance may be observed among different syndromes. Traditional single-label data-mining techniques, which could only build one model at a time, ignore the fact that one patient may be associated with more than one syndrome. In this study, a novel multilabel learning (MLL) technique is explored to solve this problem. Our group [5] applied a multilabel learning algorithm (ML-kNN) to construct a syndrome model for diagnosing CHD in TCM. The ML-kNN produces better results than the ranking Support Vector Machine (Rank-SVM), BPMLL, and kNN based on three criteria, namely, average precision, coverage, and ranking loss.
Compared with traditional learning methods, multilabel learning more effectively identifies syndrome information in TCM and solves problems such as single samples with several syndromes. However, the relationship between features and class labels is not concerned in multilabel learning.
Chronic gastritis (CG) is a common disease and is classified under spleen and stomach diseases in TCM. According to preliminary studies, we applied the feature selection methods to select significant symptoms (signs) associated with each syndrome in CG. In addition, we further applied multilabel learning algorithm to construct the syndrome models of inquiry diagnosis for CG in TCM to provide a reference for the syndrome standardization and objectification of CG.
In this paper, the first section includes the introduction of the research progress in the field of TCM diagnosis, the purpose of the study, and its significance. In Section 2, we introduce the data-collecting methods, which include a variety of feature selection methods and a multilabel learning method designated as REAL. Standardizing a scale of inquiry information is discussed in the results section. The optimal symptom set is obtained for each syndrome using feature selection. The results of diagnostic models constructed are discussed based on the REAL method. Then the results of REAL are compared with other multilabel learning algorithms. Section 3, the results of feature selection and diagnostic models are analyzed based on TCM theory. The last section concludes and indicates several issues for future studies.
2. Material and Methods
2.1. Research Subjects
Chronic gastritis (CG) samples were collected from a clinic, in-patient department, and gastroscopy room of the digestive system department of the Longhua Hospital and the Shuguang Hospital of Shanghai University of Traditional Chinese Medicine, the Xinhua Hospital, the Putuo District Central Hospital, and the Shanghai Hospital of Traditional Chinese Medicine. This work was approved by the Shanghai Society of Medical Ethics. All patients signed an informed consent form. A total of 919 valid subjects were enrolled after excluding cases with TCM inquiry diagnosis scales that lacked information or cannot be diagnosed with CG. Among the 919 patients, 354 were male (38.5%, with an average age of 44.61 yr ± 14.54 yr) and 565 were female (61.5%, with an average age of 48.70 yr ± 12.74 yr).
2.1.1. Inclusion Criteria
Including criteria were
patients who meet the diagnostic standards for CG and TCM syndromes, and
patients who were informed and have agreed to join this investigation.
2.1.2. Diagnostic Standards
Western Diagnostic Standards —
The Consensus of National Seminar on CG held by the Chinese Medical Association Digestive Diseases Branch in 2006 [10] was refered to diagnose whether a patient has CG based on gastroscopy results, pathologic results, and clinical performance.
Chinese Diagnosis Standard —
Diagnosis Standard includes the following eight syndromes (patterns) referring to “Guideline for Clinical Research of New Traditional Chinese Medicine” [11] issued by the Ministry of Health and “National Standard of People's Republic of China: Syndrome Part of TCM Clinical diagnosis and Treatment Terminology” [12] issued by the China State Bureau of Technical Supervision,
damp heat accumulating in the spleen-stomach,
dampness obstructing the spleen-stomach,
spleen-stomach qi deficiency,
spleen-stomach cold deficiency,
liver stagnation,
stagnated heat in the liver-stomach,
stomach yin deficiency,
blood stasis in the stomach collateral.
2.1.3. Exclusion Criteria
Excluding criteria were
mentally ill patients and patients with other severe systemic diseases,
patients who have difficulty in describing their conditions, and
patients who are not informed or refuse to cooperate.
2.2. Method for Establishing TCM Inquiry Diagnosis Scales
The research group was composed of Shanghai senior clinical experts on the digestive system, clinical doctors, and researchers. The final TCM inquiry diagnosis scales were drafted based on past experience in the production of scales [13], a wide range of literature about TCM spleen and stomach diseases, related documents in core magazines, and journals for over 15 years and reports about the frequency of symptoms associated with syndromes in CG diseases in TCM. The scales were also amended and fixed by two rounds of expert consultation and statistical tests. The scales include eight dimensions such as cold or heat, sweat, head, chest and abdomen, urine and stool, diet and taste, sleep, mood, woman aspects and contents of disease history, inspection, and palpation. More than 113 variables were ultimately included in these scales.
2.3. Investigation Methods
The clear definitions of symptoms, the specific methods, and the order of inquiry diagnosis are given in the scales. All samplers must have undergone unified training. The group members assemble regularly and discuss the information of typical patients to ensure the consistency of the collected data.
2.4. Diagnosis Methods
Three senior chief doctors with plenty of experience in clinical practices were invited for inquiry diagnosis of the cases in terms of the CG diagnostic standards made by our research group. If two of them have the same diagnosis results, the case was included. Otherwise, the case was not adopted until at least two of them came to the same conclusion.
2.5. Data Input and Process Methods
We have the following methods
Build a database with Epidata software.
Input data two times independently.
The Epidata software compares the two data sets and checks out mistakes.
Check the investigation form logically in case of filling errors.
2.6. Feature Extraction Methods
To obtain the proper set of symptoms for each syndrome, we employed four feature selection methods, namely, mutual information (MI) [14], information gain (IG) [15, 16], conditional mutual information method (CMIM) [17], and minimum redundancy maximum relevance (MRMR) [18], to investigate the relationship between the symptoms and the six common syndromes (patterns), such as the accumulation of damp heat in the spleen-stomach, dampness obstructing the spleen-stomach, spleen-stomach qi deficiency, spleen-stomach cold deficiency, liver stagnation, and stagnated heat in the liver-stomach.
2.7. Multilabel Learning Methods
Many real-world problems involving ambiguous objects lose useful information when analyzed using the traditional single-label algorithm. Thus, it will be harmful to the learning performance. To minimize this information loss, multilabel learning was proposed.
Most traditional multilabel classification approaches to learning methods in vector spaces are used based on the assumption that the instances should have the same set of features in the input space for each label. However, for specific labels, not all the features have strong correlations. ML-kNN is the lazy multilabel learning algorithm based on k-nearest neighbor techniques (kNN) [19]. Similar to the kNN algorithm, it finds the k nearest neighbors for each test instance; however, in ML-kNN, the label of each test instance is estimated directly using the k nearest neighbors in instance. We applied a new algorithm called REAL to fit the characteristics for inquiry diagnosis in TCM based on ML-kNN. The REAL algorithm extracts the best feature subset correlated with a certain label as its input space and then calculates the posterior probability combined with the ML-kNN algorithm. The REAL algorithm is shown in Algorithm 1.
Algorithm 1.
REAL algorithm.
2.8. Experimental Design and Evaluation
Different characteristics were selected using the REAL algorithm. We selected 112, 100, 70, 60, 50, 40, 30, 20, 10, and 5 symptoms (signs), which correlated with each syndrome to build a syndrome model to study the influence of the different symptoms (signs) on the diagnostic model.
Considering each example could simultaneously be associated with multiple labels, performance evaluation in multilabel learning is different from single-label learning. The following five multilabel evaluation parameters presented in [20] are used in this paper.
Average Precision —
It evaluates the average fraction of labels ranked above a particular label y ∈ Y, which actually are in Y. The performance is perfect when avgprecS(f) = 1; the bigger the value of avgprecS(f), the better the performance one has.
(1)
Coverage —
It evaluates how far on the average we need to go down the list of labels to cover all the proper labels of the instance. It is loosely related to precision at the level of perfect recall. The smaller the value of coverageS(f), the better the performance one has.
(2)
Ranking Loss —
It evaluates the average fraction of label pairs that are reversely ordered for the instance. The performance is perfect when rlossS(f) = 0; the smaller the value of rlossS(f), the better the performance,
(3) where denotes the complementary set of Y in y · y = {1,2,…, Q} be the finite set of labels.
Hamming Loss —
It evaluates how many times instance-label pairs are misclassified; that is, a label not belonging to the instance is predicted, or a label belonging to the instance is not predicted one has,
(4) where Δ denotes the symmetric difference between two sets.
One-Error —
It evaluates how many times the top-ranked label is not in the set of proper labels of the instance. The performance is perfect when one-errorΓ(f) = 0 we have.
(5) For any predicted π, ⟦π⟧ equals 1 if π holds and 0 if otherwise. Note that, for single-label classification problems, a one-error is identical to an ordinary classification error.
3. Results and Discussion
3.1. The Results of the Finest Symptoms (Signs) Subsets
3.1.1. The Results of Finest Subsets of Specific Symptoms (Signs)
In the research of multilabel classification of syndrome diagnosis for CG, feature selection methods such as mutual information, IG, CMIM, and MRMR were combined with multilabel learning. The prediction accuracy was highest when 20 features were selected for classification. Based on the results, the features selected by IG are more suitable for TCM theory than those using other algorithms.
12 specific symptoms (signs), including yellow tongue coating and greasy tongue coating, were extracted for the pattern of damp heat accumulating in the spleen-stomach.
12 specific symptoms (signs), including white and greasy tongue coating, were extracted for the pattern of dampness obstructing the spleen-stomach.
11 specific symptoms (signs), including fatigue and tongue with teeth marks, were extracted for the pattern of spleen-stomach qi deficiency.
8 specific symptoms (signs), including cold limbs and preference for warm temperature, were extracted for the pattern of spleen-stomach cold deficiency.
9 specific symptoms (signs), including white aggravating after anxiety or anger, distending pain in the chest, and hypochondriac area, were extracted for the pattern of liver stagnation.
12 specific symptoms (signs), including burning pain and red tongue, were extracted for the pattern of stagnated heat in liver-stomach.
The detailed information about symptoms (signs) is displayed in Table 1.
Table 1.
The finest subsets of specific symptoms (signs).
| Symptoms (signs) | Syndromes (patterns) | |||||
|---|---|---|---|---|---|---|
| Damp-heat accumulating in the spleen-stomach | Dampness obstructing the spleen-stomach | Spleen-stomach qi deficiency | Spleen-stomach deficiency cold | Liver stagnation | Stagnated heat in liver-stomach | |
| 1 | Yellow tongue coating | Greasy tongue coating | Fatigue | Cold limbs | Aggravating after anxiety or anger | Red tongue |
|
| ||||||
| 2 | Greasy tongue coating | Thick tongue coating | White tongue coating | Preference for warm | Distending pain in the chest and hypochondriac area | Burning pain |
|
| ||||||
| 3 | Red tongue | White tongue coating | Tongue with teethmarks | White tongue coating | Belching | Distending pain in the chest and hypochondriac area |
|
| ||||||
| 4 | Thick tongue coating | Whitish tongue | Pale-white tongue | Cold pain | Pain of unfixed location | Preference for cold |
|
| ||||||
| 5 | Retrosternal burning sensation | Tongue with teethmarks | Fat tongue | Whitish tongue | Gastric distension | Yellow tongue coating |
|
| ||||||
| 6 | Dry tongue coating | Fat tongue | Whitish lips | Loose stool | Aggravating after diet | An empty sensation in the stomach |
|
| ||||||
| 7 | Greasy taste | Dark-red tongue | Loose stool | Heaviness of the body | Preference for pressure | Dry stool |
|
| ||||||
| 8 | Dark-red tongue | Slippery tongue coating | Dizziness | Thin tongue coating | Preference for warm | Thin tongue |
|
| ||||||
| 9 | Mixed yellow and white tongue coating | Slippery pulse | Thin tongue coating | Fixed pain | Thirsty | |
|
| ||||||
| 10 | Bitter taste in the mouth | Cold limbs | Heaviness of the body | Red lips | ||
|
| ||||||
| 11 | Preference for cold | Bluish or purple tongue | Whitish complexion | Soure taste | ||
|
| ||||||
| 12 | Slippery pulse | Hesitant pulse | Insomnia | |||
3.1.2. The Results of Finest Subsets of Negative Symptoms (Signs)
They are as follows
8 negative symptoms (signs) including white and thin tongue coating were extracted for the pattern of damp-heat accumulating in the spleen-stomach.
12 negative symptoms (signs) including red and dark red tongue were extracted for the pattern of dampness obstructing the spleen-stomach.
11 negative symptoms (signs) including thick tongue coating, mixed yellow, and white tongue coating were extracted for the pattern of spleen-stomach qi deficiency.
8 negative symptoms (signs) including red lips and good appetite, but easily gets hungry, were extracted for the pattern of spleen-stomach cold deficiency.
9 negative symptoms (signs), including fatigue and pain when exposed to cold, were extracted for the pattern of liver stagnation.
12 negative symptoms (signs) including tongue with teeth marks and fat tongue were extracted for the pattern of stagnated heat in liver-stomach.
The detailed information about negative symptoms (signs) is displayed in Table 2.
Table 2.
The finest subsets of negative symptoms (signs).
| Symptoms (Signs) | Syndromes (Patterns) | |||||
|---|---|---|---|---|---|---|
| Damp-heat accumulating in the spleen-stomach | Dampness obstructing the spleen-stomach | Spleen-stomach qi deficiency | Spleen-stomach deficiency cold | Liver stagnation | Stagnated heat in liver-stomach | |
| 1 | White tongue coating | Red tongue | Red lips | Red lips | Fatigue | Tongue with teethmarks |
|
| ||||||
| 2 | Thin tongue coating | Dark-red tongue | Thick tongue coating | Stabbing pain | Thick tongue coating | Thick tongue coating |
|
| ||||||
| 3 | Fat tongue | Thin tongue coating | Mixed yellow and white tongue coating | Good appetite but fast hunger | Bitter taste | Greasy tongue coating |
|
| ||||||
| 4 | Tongue with teethmarks | Yellow tongue coating | Greasy tongue coating | Thick tongue coating | Cold pain | Fat tongue |
|
| ||||||
| 5 | Whitish Lips | Distending pain in the chest and hypochondriac area | Red tongue | Fetid mouth odor | Greasy tongue coating | Whitish tongue |
|
| ||||||
| 6 | Whitish complexion | Wiry pulse | Dark-red tongue | Red tongue | Rapid pulse | White tongue coating |
|
| ||||||
| 7 | Whitish tongue | Whitish lips | Yellow tongue coating | Heat sensation in both palms and soles | Thin tongue coating | Slippery pulse |
|
| ||||||
| 8 | Dark -purple lips | Yellow urine | Retrosternal burning sensation | Thin tongue | Loose stool | Cold limbs |
|
| ||||||
| 9 | Large pulse | Yellow tongue coating | Deep pulse | |||
|
| ||||||
| 10 | Preference for eating cold food | Heaviness of the body | ||||
|
| ||||||
| 11 | Dry tongue coating | Rotten tongue coating | ||||
|
| ||||||
| 12 | Hesitant pulse | |||||
3.2. The Results of Syndrome Classification Using Multilabel Learning Methods
3.2.1. Comparison of Average Accuracy with Different Number of Features
Using the REAL algorithm, we selected 112, 100, 70, 60, 50, 40, 30, 20, 10, and 5 symptoms (signs), which correlated with each syndrome to build a syndrome classification model to study the influence of the different symptoms (signs) on the diagnostic model.
The abscissa represents the number of the selected features, and the vertical axis represents their prediction accuracy in Figure 1.
Figure 1.
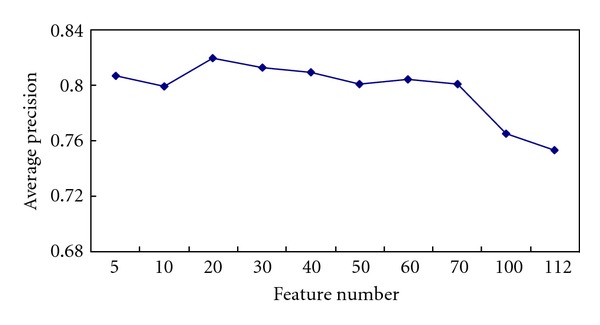
The average accuracy rate with different number of symptoms (signs) by using REAL methods.
As shown in Figure 1, the average accuracy changes with the number of symptoms (signs). When the number of selected symptoms (signs) was 20, the average accuracy peaked at 82%. Then, it decreased gradually with increasing number of symptoms (signs).
3.2.2. Comparison of Performance of Different Multilabel Learning Algorithms
We selected 20 symptoms (signs) to build the models and compared the five evaluation parameters obtained using ML-kNN, Ensembles of Classifier Chains (ECCs), BSVM, BP-MLL, Rank-SVM, and REAL algorithms. The result is shown in Table 3.
Table 3.
Performance of different multilabel learning algorithms.
| Group (mean ± std) | ML-kNN | ECC | BSVM | BP-MLL | RANK-SVM | REAL |
|---|---|---|---|---|---|---|
| Average precision | 0.759 ± 0.029 | 0.802 ± 0.016 | 0.802 ± 0.016 | 0.540 ± 0.023 | 0.707 ± 0.022 | 0.820 ± 0.029 |
| Coverage | 0.200 ± 0.023 | 0.186 ± 0.019 | 0.174 ± 0.023 | 0.345 ± 0.039 | 0.237 ± 0.016 | 0.160 ± 0.020 |
| Hamming loss | 0.167 ± 0.014 | 0.148 ± 0.016 | 0.156 ± 0.014 | 0.304 ± 0.014 | 0.214 ± 0.014 | 0.142 ± 0.019 |
| One error | 0.375 ± 0.050 | 0.261 ± 0.024 | 0.307 ± 0.022 | 0.755 ± 0.029 | 0.449 ± 0.034 | 0.283 ± 0.055 |
| Ranking loss | 0.167 ± 0.025 | 0.190 ± 0.025 | 0.130 ± 0.017 | 0.334 ± 0.040 | 0.206 ± 0.014 | 0.117 ± 0.018 |
As indicated in Table 3, the highest was 82%, obtained by REAL, whereas the lowest average precision was 54%, obtained using BP-MLL. For the indicators coverage, hamming loss, and ranking loss, the values obtained using the REAL algorithm were lowest at 0.160, 0.142, and 0.177, respectively. In summary, the results obtained using the REAL algorithm were the most accurate.
3.2.3. The Comparison of Accuracy Rates of Various Syndromes Using Different Multilabel Methods (the 20 Features Are Selected in REAL Method)
The results of the REAL method were compared with the other multilabel learning methods, namely, BP-MLL, Rank-SVM, ECC, BSVM, and ML-kNN. The recognition accuracies of the six common syndromes of CG are shown in Table 4.
Table 4.
Comparison of recognition accuracy for six common syndromes.
| Syndromes (Patterns) |
ML-kNN | ECC | BSVM | BP-MLL | Rank-SVM | REAL |
|---|---|---|---|---|---|---|
| Damp-heat accumulating in the spleen-stomach | 0.869 ± 0.036 | 0.899 ± 0.025 | 0.884 ± 0.025 | 0.247 ± 0.035 | 0.880 ± 0.028 | 0.901 ± 0.030 |
| Dampness obstructing the spleen-stomach | 0.737 ± 0.044 | 0.789 ± 0.052 | 0.800 ± 0.035 | 0.683 ± 0.052 | 0.762 ± 0.044 | 0.830 ± 0.038 |
| Spleen-stomach qi deficiency | 0.689 ± 0.065 | 0.741 ± 0.037 | 0.712 ± 0.023 | 0.538 ± 0.039 | 0.679 ± 0.068 | 0.699 ± 0.041 |
| Spleen-stomach deficiency cold | 0.966 ± 0.017 | 0.958 ± 0.019 | 0.943 ± 0.027 | 0.966 ± 0.017 | 0.793 ± 0.036 | 0.966 ± 0.023 |
| Liver stagnation | 0.827 ± 0.056 | 0.820 ± 0.043 | 0.826 ± 0.049 | 0.831 ± 0.054 | 0.801 ± 0.047 | 0.840 ± 0.063 |
| Stagnated heat in liver-stomach | 0.908 ± 0.023 | 0.906 ± 0.034 | 0.901 ± 0.030 | 0.910 ± 0.022 | 0.799 ± 0.048 | 0.910 ± 0.019 |
As shown in Table 4, for the pattern of damp heat accumulation in the spleen-stomach, the REAL algorithm achieved the highest accuracy rate, followed by ECC, BSVM, Rank-SVM, ML-kNN, and BP-MLL. For the pattern of dampness obstructing the spleen-stomach, the REAL algorithm also had the highest accuracy rate, followed by BSVM, ECC, Rank-SVM, ML-kNN, and BP-MLL.
For the pattern of spleen-stomach qi deficiency, the accuracy rate obtained from ECC was the highest, followed by BSVM, REAL, ML-kNN, Rank-SVM, and BP-MLL. For the pattern of spleen-stomach cold deficiency, REAL, ML-kNN and BP-MLL had the highest accuracy rate at 96.6%, followed by ECC, BSVM, and Rank-SVM. For the pattern of liver stagnation, the REAL algorithm achieved the highest accuracy rate, followed by BP-MLL, ML-kNN, BSVM, ECC, and Rank-SVM. For the pattern of stagnated heat in the liver-stomach, BP-MLL and REAL algorithm achieved the highest accuracy rate, followed by ML-kNN, ECC, BSVM, and Rank-SVM.
From the results, the comprehensive performance of REAL method was the best, with the accuracy rates in the six syndromes, except for the pattern of spleen-stomach qi deficiency.
3.3. Discussion
A syndrome is a unique TCM concept. It is an abstractive conception of a variety of symptoms and signs. It is a pathological summarization of a certain stage of a disease, and it covers disease location, etiology, and the struggle between the body's resistance and pathogenic factors. Different syndromes have different clinical manifestations.
Symptoms, which are the external manifestations of a disease and a syndrome, refer to subjective abnormalities and the abnormal signs of patients elicited by doctors using the four diagnostic methods.
The etiology, location, nature, the struggle between the body's resistance and pathogenic factors, and the condition at a certain stage of the disease process are highly summarized using syndrome differentiation. Syndrome differentiation involves three steps: (a) determining symptoms and signs through inspection, auscultation, inquiry, and palpation; (b) making an overall analysis of the information; (c) making a diagnostic conclusion. All these steps are based on TCM theory.
Figure 2 shows the TCM diagnosis of the network structure diagram. Network structure can be compared to a tree, where the root node is composed of a number of leaf nodes. X1, X2,…, X7 leaf nodes are directly observed, and we call them manifest variables, which denote the symptoms and signs in TCM. Z1, Z2, Z3, and Z4 are the root nodes that are indirectly measured through their manifestations, and we call them latent variables, which represent the syndromes of chronic gastritis in TCM. The syndrome can be observed alone or with others, such as Z1 and Z2, or Z2 and Z3, which may appear together.
Figure 2.
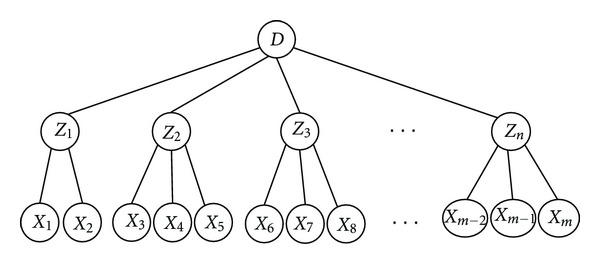
Syndrome diagnostic schemes.
D denotes the disease. In this study, it represents chronic gastritis, which is a disease defined in Western Medicine. Chinese medical diagnosis of chronic gastritis may contain syndromes like latent variables Z1, Z2, Z3 … and so on.
3.3.1. The Finest Symptoms (Signs) Feature Subsets for Each Syndrome
Feature selection is a hot topic in the field of machine learning. It studies how to select the most effective feature subset from a set of original feature sets to reduce the feature space dimension and enhance the generalization ability of the model.
Feature selection not only removes the redundant and irrelevant features of the data, but also significantly reduces the cost of data mining.
Information gain is a widely used feature selection method [21]. It was first proposed for text classification and was then used in other areas such as image processing and bioinformatics.
Currently, those feature selection methods [22] have been used in TCM diagnosis for selecting symptoms (signs) and building diagnostic models. Many studies have shown that these feature selection methods select key features effectively and also remove irrelevant features. Some symptoms and signs in TCM have certain specific meanings that can be used for determining the syndrome.
When making a diagnosis is difficult using positive aspects, doctors can diagnose by eliminating symptoms and signs of similar syndromes.
Negative information [23] denotes some symptoms that have a negative meaning in the diagnosis of certain diseases, or some information that are impossible to be observed in some diseases.
The purpose of this study is to recognize the common syndromes of CG using IG combined with multilabel learning. The six finest symptoms (signs) subsets were selected by correlating the six common syndromes of CG, which include the specific and negative symptoms (signs). The experimental results show that the six finest symptoms (signs) subsets are basically in accordance with the TCM theory, clinical practice, and the previous Chinese diagnostic standard.
However, individual symptoms (signs) such as the preference for pressure and warm temperature, fixed pain with the syndrome of liver depression and qi stagnation do not agree with the TCM theory, which may be due to the fact that several syndromes appear together.
3.3.2. Comparison between REAL and Other Multilabel Learning Methods
Compared with conventional learning methods, multilabel learning identifies syndromes in TCM more effectively and solves problems of one sample being associated with several syndromes.
In clinical practice, relevance among different syndromes may exist. The syndrome complex of one patient is mainly composed of several syndromes. For example, spleen-stomach qi deficiency syndrome usually exists with dampness obstructing the middle energizer syndrome, qi stagnation syndrome, turbid phlegm syndrome, or blood stasis syndrome.
In multilabel data, there is a relationship among labels. However, this relationship may be bound to be ignored inevitably by using the single-label learning. For this reason, multilabel learning algorithms are developed to facilitate the correlation of the labels.
Compared with other traditional multilabel learning methods, the REAL algorithm found the relevant symptom subset of each syndrome with feature selection. Moreover, the REAL algorithm identified the syndrome information of CG in TCM more effectively and accurately.
In addition, the REAL algorithm assisted in extracting the corresponding specificity and negative symptoms (signs) through feature selection. Extracted features are not only used for identifying the syndrome of chronic gastritis, but it also improves the syndrome diagnostic accuracy of chronic gastritis.
4. Conclusions
To fully understand the characteristics of multilabel data of TCM in syndrome diagnosis, feature selection was combined with a multilabel learning algorithm.
Applying the REAL method extracts the relevant symptoms (signs) for each syndrome and improves the accuracy of syndrome diagnosis in CG.
The study showed that the six finest symptoms (signs) subsets agree with the theory and clinical practice of TCM. In addition, the study will serve as references for establishing diagnostic criteria and a diagnostic model for CG and a better guide for clinical practice. Further studies will focus on building an intelligent diagnostic system for CG with application of the method on biomedical data sets.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (Grant no. 30901897 and 81173199), the Shanghai 3th Leading Academic Discipline Project (Grant no. S30302), and the National Natural Science Foundation of China (Grant no. 30701072.)
References
- 1.Zheng SM, Hu LS, Li YL, Biao R. Screening methods of traditional Chinese medicine. Chinese Journal of Basic Medicine in Traditional Chinese Medicine. 2008;14:304–305. [Google Scholar]
- 2.Li GC, Li CT, Huang LP, et al. An investigation into regularity of syndrome classification for chronic atrophic gastritis based on structural equation model. Journal of Nanjing University of Traditional Chinese Medicine. 2006;22:217–220. [Google Scholar]
- 3.Bai YJ, Meng QG, Shen HB, et al. Study on non-linear modelling of TCM syndrome of DN based on improved BP neural network model. Journal of Beijing University of Traditional Chinese Medicine. 2008;31:308–311. [Google Scholar]
- 4.Gao HL, Wu YL, Chen J, et al. The complex system based on entropy method to partition the syndrome diagnosis standard research of application. China Journal of Traditional Chinese Medicine and Pharmacy. 2008;23:307–309. [Google Scholar]
- 5.Liu GP, Li GZ, Wang YL, Wang YQ. Modelling of inquiry diagnosis for coronary heart disease in traditional Chinese medicine by using multi-label learning. BMC Complementary and Alternative Medicine. 2010;10, article 37 doi: 10.1186/1472-6882-10-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Su Y, Wang L, Zhang H. Posthepatitic cirrhosis of TCM syndrome and disease information similarity analysis. Chinese Journal of Integrated Traditional and Western Medicine. 2009;29:398–402. [PubMed] [Google Scholar]
- 7.Liu GP, Wang YQ, Xu ZX, et al. Based on the structure of traditional Chinese medicine of spleen hidden information objectified by analysis. Journal of Traditional Chinese Medicine. 2011;52:1372–1375. [Google Scholar]
- 8.Liu GP, Wang YL, Wang YQ, et al. Coronary Heart Disease of TCM syndrome association. Journal of Liaoning University of Traditional Chinese Medicine. 2011;38:821–824. [Google Scholar]
- 9.Liu GP, Wang YQ, Li FF, et al. Association analysis and distribution of chronic gastritis syndromes based on associated density. In: Proceedings of the IEEE International Conference on Bioinformatics and Biomedicine Workshops (BIBMW '10); December 2010; pp. 790–794. [Google Scholar]
- 10.Chinese Medical Association Digestive Diseases Branch. Consensus of national seminar on chronic gastritis. Chinese Journal of Digestive Endoscopy. 2007;24:58–63. [Google Scholar]
- 11.Zheng XY. Chinese Herbal Medicine Clinical Research Guiding Principles (for Trial Implementation) Beijing, China: China Medical Science and Technology Press; 2004. [Google Scholar]
- 12.State Bureau of Technical Supervision. National Standards of Peoples Republic of China: Syndrome Part of TCM Clinical Diagnosis and Treatment. Beijing, China: Standards Press of China; 1997. [Google Scholar]
- 13.Liu GP, Wang YQ, Dong Y, et al. Development and evaluation of Scale for heart system Inquiry of TCM. Journal of Chinese Integrative Medicine. 2009;7:1222–1225. doi: 10.3736/jcim20090103. [DOI] [PubMed] [Google Scholar]
- 14.Kenneth WC, Patrick H. Word association norms, mutual information, and lexicography. In: Proceedings of the 27th Annual Meeting on Association for Computational Linguistics (ACL '89), vol. 27; 1989; Vancouver, Canada. pp. 76–83. [Google Scholar]
- 15.Quinlan JR. Induction of decision trees. Machine Learning. 1986;1(1):81–106. [Google Scholar]
- 16.Mitchell T. Machine Learning. McCraw Hill; 1996. [Google Scholar]
- 17.Fleuret F. Fast binary feature selection with conditional mutual information. Journal of Machine Learning Research. 2004;5:1531–1555. [Google Scholar]
- 18.Peng H, Long F, Ding C. Feature selection based on mutual information: criteria of Max-Dependency, Max-Relevance, and Min-Redundancy. IEEE Transactions on Pattern Analysis and Machine Intelligence. 2005;27(8):1226–1238. doi: 10.1109/TPAMI.2005.159. [DOI] [PubMed] [Google Scholar]
- 19.Schapire RE, Singer Y. BoosTexter: a boosting-based system for text categorization. Machine Learning. 2000;39(2):135–168. [Google Scholar]
- 20.Zhang ML, Zhou ZH. ML-KNN: a lazy learning approach to multi-label learning. Pattern Recognition. 2007;40(7):2038–2048. [Google Scholar]
- 21.You MY, Chen Y, Li GZ. Disequilibrium problem of the new feature selection algorithm: Im-IG. Shandong University Journal. 2010;40:123–128. [Google Scholar]
- 22.Shao H, Li GZ, Liu GP. Symptom selection for multi-label data of inquiry diagnosis in traditional Chinese medicine. Science China Information Sciences. 2011;41:1372–1387. [Google Scholar]
- 23.Xu YJ. TCM tongue pulse diagnosis system and tongue diagnosis digital pulse. Beijing University of Chinese Medicine; Ph.D. thesis. [Google Scholar]