

Abstract
Objectives:
The objective of the study was to assess the quality of life in patients with skin disease.
Subjects and Methods:
A 6-month cross-sectional study was conducted in the Dermatology Clinic at King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia. The study sample consisted of all 297 adult patients with dermatological conditions attending clinic but without associated psychiatric disease. They completed a self-administered Arabic version of the Dermatology Life Quality Index questionnaire (DLQI), containing ten items. The data was analyzed according to disease, age and gender.
Results:
The gender distribution of the study sample was 73% female and 27% male. The mean age was 29.4 years. The proportions of patients with various diagnoses were: sebaceous and apocrine gland disorders 31.3%, eczematous dermatitis 18.5%, cutaneous infections 13.5%, and pigmentary disorders 10.8%. The mean DLQI of all patients was 8.32. Patients with papulosquamous disorders recorded the highest mean DLQI score of 15.28, followed by immunological disorders with 11.11, eczematous dermatitis with 9.55, and miscellaneous disorders with 10.91. The mean DLQI was higher among females (9.02) than males (6.46). Age had no influence on the degree of impairment.
Conclusion:
Measuring the impairment of the quality of life in dermatology patients is an important aspect of management. It allows clinicians to assess the extent and nature of the disability so that an appropriate management regimen can be implemented and its effectiveness assessed.
Keywords: Dermatology Life Quality Index, Impairment, Quality of life, Skin disease
INTRODUCTION
Most dermatologic conditions do not constitute a direct threat to life, but their chronic and incurable character has a powerful negative impact on the quality of life of the afflicted patients.1 Virtually all aspects of patients’ lives can be affected. The financial burden of disease include direct medical costs, out-of-pocket expenses, lost productivity, and others.2
Patients may experience severe symptoms especially itching, pain and discomfort that can have profound psychological impact. Social and physical activities including sports and work may be adversely affected because of reluctance to let other people see their skin disease. Employers are concerned about the possible reaction of their customers to their employees with skin disease.3 In extreme cases, some teenage patients with acne commit suicide because of their appearance.4 At times, some treatment modalities can worsen the quality of life because of the difficulties involved in the use of topical creams and ointments.3
Measuring the impact of dermatologic disease on the quality of life is very useful for several reasons. It allows patients to express their feelings and appreciate their physicians’ concerns. It improves doctor-patient communication. It also helps in disease management, including the risk/benefit assessment of alternative therapeutic interventions. Measurement of the quality of life can be used in clinical research as well as for political and financial purposes relating to the development of dermatological services. Quality of life measures may also be effectively used in auditing clinical activities.3,5,6
Few studies have been carried out on the quality of life in patients with skin disease in developing countries,7 and in Saudi Arabia in particular.8 The present study looks at the impact of skin disease on the quality of life among adult patients attending the dermatology outpatient clinics at King Fahad Medical City, Riyadh, Saudi Arabia. It is hoped that the results will help in assessing the impact of skin disease on the quality of life of patients and the possible interventions that can help to improve that quality.
SUBJECTS AND METHODS
This is a cross-sectional study conducted in the dermatology clinic at King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia. The study subjects were all the adult patients, aged 16 years and above, not currently suffering from any psychiatric morbidity, who attended the dermatology clinic during the period between 5th January and 30th June 2006.
The subjects completed a translated, validated, pre-tested Arabic version of the English version of the Dermatology Life Quality Index (DLQI) to measure the effect of skin disorders on the quality of their lives.9 The DLQI questionnaire is simple and brief, containing ten questions, each with four possible answers scored 0 to 3, covering the last seven days of the patient's life. The DLQI is calculated as the sum of these scores, up to a maximum possible value of 30. The higher the total score is, the greater the impact of the disease. The ten questions are attributes relating to different aspects of the patient's life, and are grouped into the following categories: physical symptoms such as pain (1), feelings such as embarrassment (2), everyday activities (3 and 4), leisure (5 and 6), work and school (7), personal relationship (8 and 9) and therapy (10). The detailed definitions of these attributes are found in the source cited above.
The skin diagnoses were classified in eight categories: 1) papulosquamous disorders, 2) connective tissue and immunological disorders, 3) eczematous dermatitis, 4) sebaceous and apocrine gland disorders, 5) disorders of hair follicles and related disorders, 6) cutaneous infections, 7) pigmentary disorders, and 8) miscellaneous (sexually transmitted diseases, tumors, etc).
Participation in the study was totally voluntary. The investigator explained the purpose of the research and how the survey was to be conducted. The subjects were then asked to fill out the questionnaire immediately in the presence of trained Arabic-speaking nurses who would help those who might have difficulty in understanding the questionnaire. Confidentiality was maintained throughout the study and subjects were assured that results would be used only for the stated scientific research purposes.
Data collected were checked for completeness and consistency. They were then entered in a personal computer and were analyzed using the Statistical Package for Social Sciences (SPSS) version 10.010. Means with 95% confidence intervals were computed. Associations between and among variables were explored using the Student t-test statistic, the chi-square statistic, with Yate's correction, analysis of variance, and bivariate correlations.
RESULTS
A total of 297 patients participated in the study, 80 (27%) males and 217 (73%) females. Their mean age was 29.4 + 0.7 years, with a minimum of 16 and maximum of 71 years. The majority, 71.8%, were aged 21-40 years.
Table 1 shows proportions of diagnoses and DLQI scores. The most frequent diagnoses were: sebaceous and apocrine gland disorders 31.3%, eczematous dermatitis 18.5%, cutaneous infections 13.1%, and papulosquamous disorders 4.7%. The mean DLQL score was 8.3 and the median score was 6. The scores in order of magnitude for the main diagnoses were: papulosquamous, connective tissue disorders, immunological disorders, and pigmentary disorders.
Table 1.
Means of DLQL scores in different dermatological diseases by sex
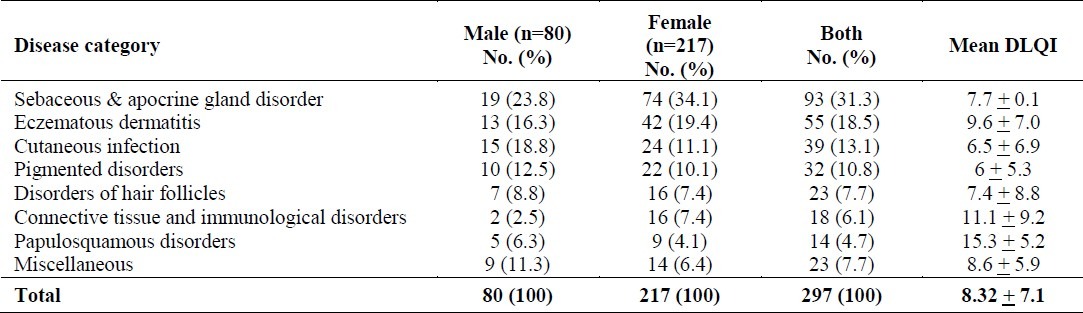
Table 2 compares DLQL scores of males and females for various attributes/aspects of impairment. Females had significantly higher total scores and also significantly higher scores for 7 out of 10 attributes. There was no significant difference on the remaining attributes.
Table 2.
Comparison between males and females’ dermatology life quality index
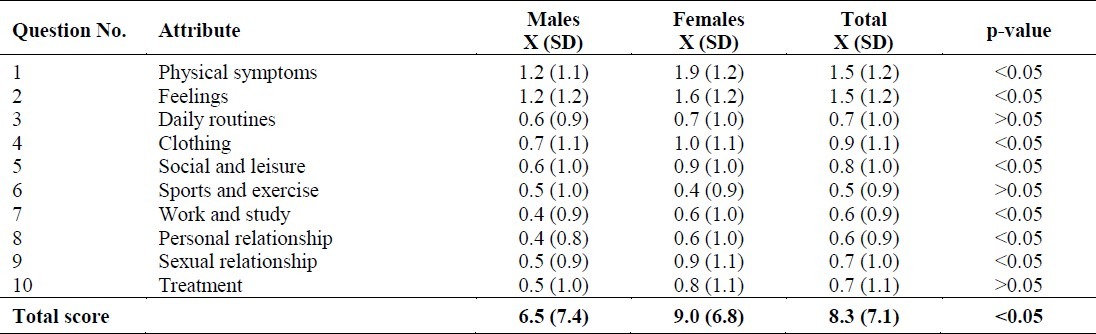
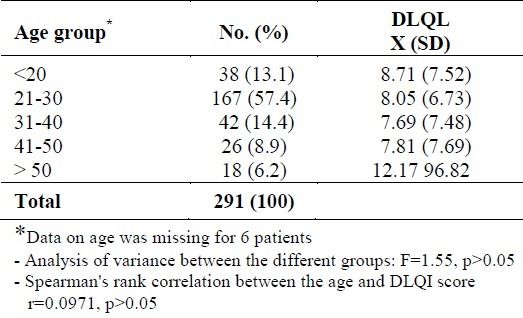
Table 3 shows DLQI scores by age group. There was no significant relation between age and total DLQI score.
Table 3.
Relatioship between DLQL scores and age group
DISCUSSION
Finlay and Khan together with other researchers have developed, used, and validated the DLQI for measuring and comparing disability in a variety of common dermatological conditions in different populations and settings.11–17 This study revealed high levels of dermatological disability among the studied subjects. The mean DLQI score for all patients was 8.42. The item with the highest score among new patients was item 1 (pain), while that among treated patients was item 4 (clothes choice). These findings are higher than those reported by Harlow et al18 who found that the overall DLQI score was 7.4 ± 5.7. This is not unexpected as their patients were primary care patients and ours were patients attending a tertiary health care facility and were likely to be suffering from more severe disease compared with subjects from general dermatology clinics or the community. Papulosquamous disorders and connective tissue & immunological disorders were the more disabling conditions (scores of 15.3 ± 5.2 and 11 .1 ± 9.2 respectively). Unpleasant symptoms and feeling of embarrassment and self-consciousness were the most important items causing the distress. In some studies, the itchy sensations had the highest mean DLQI score translating into the highest negative impact on the quality of life.2,19
The disability suffered by female patients was significantly more than that suffered by males, the mean ± SD total DLQI scores being 9.0 ± 6.8 and 6.5 ± 7.4 respectively. This finding is in conformity with findings of international studies which reported higher DLQI for females.20–22 Other studies found higher DLQI for males.23 A study conducted in the Qassim province of Central Saudi Arabia24 found no significant gender differences in the quality of life in patients with vitiligo, a skin disease, in agreement with some international studies which reported that gender did not have a major impact on quality of life.11,25 Gender differences, however, were not consistent in all studies. These differences may be due to differences in populations, sampling methods, settings of study and the spectrum of diseases studied.
The relationship between age and the impairment caused by skin disease was studied. It was found that DLQI Scores did not vary significantly with age (table 3). These results are in conformity with the findings of Harlow et al18 Linnet and Jemee,17 and Poon et al13 who stated that there was no significant correlation between age and DLQI Score in patients with skin diseases. Other studies, however, reported that for some diseases, younger patients suffered the greatest impairment in the quality of life.24
Measuring the impairment of the quality of life in dermatology patients can be an important aspect of management. This explains why during the last decade there has been a gradual increase in the international use of the DLQI. The brevity and simplicity of the use of the DLQI have resulted in its popularity both in clinical practice and in research.26 The use of a quality of life index allows clinicians to assess the extent and nature of disability suffered, so that an appropriate management regimen can be implemented. Its use helps clinicians to gain an insight into the degree of impairment experienced and therefore, the resulting treatment decisions made would be more focused on the patient's preferences and priorities.27 The effectiveness of these regimens can then be estimated by using the quality of life index after treatment.
REFERENCES
- 1.Del Pozo MD, Lobera T. Quality of life in dermatology. Allergol. Immunol. Clin. 2001;16:239–63. [Google Scholar]
- 2.Qureshi AA, Freedberg I, Goldsmith L, Moshell A. Burden of skin disease: then and now. Journal of Investigative Dermatology Symposium Proceedings. 2004;9:111–9. doi: 10.1046/j.1087-0024.2003.09104.x. [DOI] [PubMed] [Google Scholar]
- 3.Finlay AY. Quality of life indices. Indian J Dermatol Venerol Leprol. 2004;70(3):143–8. [PubMed] [Google Scholar]
- 4.The Times. London, UK: 2004. Jan 8, [Google Scholar]
- 5.Finlay AY. Quality of life measurement in dermatology: a practical guide. Br J Dermatol. 1997;136:305–14. [PubMed] [Google Scholar]
- 6.All Party Parliamentary Group on Skin. Report on the enquiry into the impact of skin diseases on people's lives. London: 2003. Jul, [Google Scholar]
- 7.Etemesi BA. Impact of chronic skin disease on the quality of life of Tanzanian adults. Br J Dermatol. 2003;149(suppl. 64):19–56. [Google Scholar]
- 8.Alakloby OM, Wahass SH. Quality of life in patients with chronic skin diseases. J Saudi Soc Dermatol Surgery. 2008;12(1):26–6. [Google Scholar]
- 9.Finlay AY, Khan GK. Dermatology life quality index (DLQI) – a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19:210–6. doi: 10.1111/j.1365-2230.1994.tb01167.x. [DOI] [PubMed] [Google Scholar]
- 10.Illinois 60611, USA: SPSS Inc; 1999. [Google Scholar]
- 11.Kent G, Al-Abadie M. Factors affecting responses on dermatology life quality index among vitiligo sufferers. Clin Exp Dermatol. 1996;21:330–3. [PubMed] [Google Scholar]
- 12.Finlay AY. In: Dermatology life quality index: initial experience of a simple practical measure in: Care management of skin diseases: life quality and economic impact. Rajagopalan R, Sheretz EF, Anderson RT, editors. New York: Marcel Dekker; 1998. pp. 85–94. [Google Scholar]
- 13.Poon E, Seed PT, Greaves MW, Kobza-Black A. The Extent and nature of disability in different urticarial conditions. Br J Dermatol. 1999;140:667–71. doi: 10.1046/j.1365-2133.1999.02767.x. [DOI] [PubMed] [Google Scholar]
- 14.Herd RM, Tidman MJ, Ruta DA, Hunter JAA. Measurement of quality of life in atopic dermatitis: correlation and validation of two different methods. Br J Dermatol. 1997;136:502–7. [PubMed] [Google Scholar]
- 15.Badia X, Mascaró JM, Lozano R. Measuring health-related quality of life in patients with mild to moderate eczema and psoriasis: clinical validity, reliability, and sensitivity tochange of the DLQI. Br J Dematol. 1999;141:698–702. doi: 10.1046/j.1365-2133.1999.03112.x. [DOI] [PubMed] [Google Scholar]
- 16.Finlay AY. Measures of the effect of adult severe atopic eczema on quality of life. J Eur Acad Dermatol Venerol. 1996;34:1016–21. [Google Scholar]
- 17.Linnet J, Jemec GBE. An assessment of anxiety and dermatology life quality in patients with atopic dermatitis. Br J Dermatol. 1999;140:268–72. doi: 10.1046/j.1365-2133.1999.02661.x. [DOI] [PubMed] [Google Scholar]
- 18.Harlow D, Poyeer T, Finlay AY, Dykes PJ. Impaired quality of life of adults with skin disease in primary care. Br J Dermatol. 2000;143:979–82. doi: 10.1046/j.1365-2133.2000.03830.x. [DOI] [PubMed] [Google Scholar]
- 19.Kulthanan K, Chiawsirikajorn Y, Jiamton S. Acute urticaria: etiologies, clinical course and quality of life. Asian Pac J Allergy Immunol. 2008;26(1):1–9. [PubMed] [Google Scholar]
- 20.Meding B, Swanbeck G. Consequences of having hand eczema. Contact Dermatitis. 1990;23(1):6–14. doi: 10.1111/j.1600-0536.1990.tb00076.x. [DOI] [PubMed] [Google Scholar]
- 21.Zachariae R, Zachariae C, Ibsen HH, Mortensen JT, Wulf HC. Psychological symptoms and quality of life of dermatology outpatients and hospitalized dermatology patients. Acta Dermato –Venereologica. 2004;84(3):205–12. doi: 10.1080/00015550410023284. [DOI] [PubMed] [Google Scholar]
- 22.Gelford J, Feldman S, Stern R, Thomas J, Rolsted T, Margolis D. Determinants of quality of life in patients with psoriasis: A study from US population. J Am Acad Dermatol. 2004;51:704–8. doi: 10.1016/j.jaad.2004.04.014. [DOI] [PubMed] [Google Scholar]
- 23.Borimnejad L, Parsa Yekta Z, Nikbakht-Nasrabadi A, Firooz A. Quality of life with vitilligo: comparison of male and female Muslim patients in Iran. Gend Med. 2006;3:124–30. doi: 10.1016/s1550-8579(06)80201-9. [DOI] [PubMed] [Google Scholar]
- 24.Al Rabaee A. Assessment of quality of life in Saudi patients with vitilligo in a medical school in Qassim province, Saudi Arabia. Saudi Med J. 2007;28(9):1414–7. [PubMed] [Google Scholar]
- 25.Skoet R, Zachariae R, Agner T. Contact dermatitis and quality of life: A structured review of the literature. Br J Dermatol. 2003;149:452–6. doi: 10.1046/j.1365-2133.2003.05601.x. [DOI] [PubMed] [Google Scholar]
- 26.Basra MKA, Fenech R, Gatt RM, Salek MS, Finlay AY. The Dermatology life quality index 1994-2007: a comprehensive review of validation data and clinical results. Br J Dermatol. 2008;159(5):997–1035. doi: 10.1111/j.1365-2133.2008.08832.x. [DOI] [PubMed] [Google Scholar]
- 27.Salek S, Roberts A, Finlay A. The practical reality of using a patient-reported outcome measure in a Routine Dermatology Clinic. Dermatology. 2007;215:315–9. doi: 10.1159/000107625. [DOI] [PubMed] [Google Scholar]