

Abstract
Background:
Rotational malalignment after intramedullary tibial nailing is rarely addressed in clinical studies. Malrotation (especially >10°)of the lower extremity can lead to development and progression of degenerative changes in knee and ankle joints. The purpose of this study is to determine the incidence and severity of tibial malrotation after reamed intramedullary nailing for closed diaphyseal tibial fractures.
Materials and Methods:
Sixty patients (53 males and 7 females) with tibial diaphyseal fracture were included in this study. The mean age of the patients was 33.4±13.3 years. All fractures were manually reduced and fixed using reamed intramedullary nailing. A standard method using bilateral limited computerized tomography was used to measure the tibial torsion. A difference greater than 10° between two tibiae was defined as malrotation.
Results:
Eighteen (30%) patients had malrotation of more than 10°. Malrotation was greater than 15° in seven cases. Good or excellent rotational reduction was achieved in 70% of the patients. There was no statistically significant relation between AO tibial fracture classification and fibular fixation and malrotation of greater than 10°.
Conclusions:
Considering the high incidence rate of tibial malrotation following intramedullary nailing, we need a precise method to evaluate the torsion intraoperatively to prevent the problem.
Keywords: Computerized tomography, intramedullary nailing, malrotation
INTRODUCTION
Tibial diaphyseal fractures are the most common long bone fractures.1 The goal of treatment in these cases is to attain rapid union with acceptable axial and rotational alignment, while initial bone length is preserved.2 Several studies have shown that tibial nailing is associated with superior outcomes and less complication compared to those obtained with open reduction and internal fixation (ORIF), external fixation, or nonoperative treatment in case of closed stable or unstable fractures.3,4 Also, intramedullary (IM) nailing is the most common method of fixation for most open tibial shaft fractures.5 Closed techniques using indirect reduction in an injured limb can be challenging and cause higher rates of malalignment.6
Tibial torsion is the anatomical twist of the proximal versus distal articular axis of the tibial bone in the transverse plane around the longitudinal axis.7,8 Any change in the tibial torsion, either in the internal or in the external direction, is considered a malrotation and can be seen after fixation of the tibial shaft fractures by closed IM nailing.4,9
Rotational malalignment after IM tibial nailing is rarely specifically addressed and most clinical studies have measured axial malalignment using plain radiography. There is not enough accurate information about the incidence and severity of tibial malrotation after IM nailing.4,6–8
In many studies, tibial malrotation has been measured clinically and the incidence is reported to be 0–6%;6 whereas such incidence is reported to be 22–36% by using other measurement methods such as computerized tomography (CT) scanning.4,9
To date, several methods have been described to measure tibial torsion,4,6,8–12 and CT scan is the investigation of choice with good inter- and intra-observer reliability and repeatability.4
The purpose of this study was to determine the incidence and severity of tibial malrotation using CT scan in a consecutive series of patients who underwent closed reamed IM nailing for diaphyseal fractures. To our knowledge, there is only one similar previous study that has assessed tibial malrotation in a consecutive series of patients.4
MATERIALS AND METHODS
This study was performed from January 1, 2010 to June 30, 2010. A total of 60 patients (53 males and 7 females) with tibial mid-diaphyseal fractures, who were admitted and underwent closed IM nailing, were enrolled in this study consecutively. Exclusion criteria were fresh or old contralateral tibial fracture, previous ipsilateral tibial fracture, ipsilateral proximal or distal tibial fracture, fractures extending to knee or ankle joints, multiple trauma, and pregnancy. The study was approved by the ethical committee and a written consent form was signed by all the patients.
All of the fractures were manually reduced and operated within 3 days. Under spinal or general anesthesia, and in supine position, the fractures were fixed by the parapatellar approach. The fractures were stabilized with two interlocking screws on each side of the fracture. All of the operations were performed by the same surgeon.
A limited (few cuts) bilateral CT scan imaging was performed before each patient was discharged. A standard method similar to previous studies was used to determine tibial torsion.4,6,7,9 In supine position, both legs were gently strapped together to minimize the movement. CT scan images were prepared from 3–4 axial cuts in the proximal and 3–4 axial cuts in the distal part of tibia. Proximal cuts were taken 2–3 mm above the proximal tibiofibular joint and distal cuts were taken just proximal to the tibiotalar articulation. The proximal reference line is a line drawn as tangent to posterior tibial cortex in the cut just proximal to the fibular head. The distal reference line is a line that connects the tibial and fibular centers in the cut just proximal to the tibial plafond. The torsion angle is the angle between perpendicular lines to two reference lines [Figures 1 and 2]. The unaffected side was used as the control. Malrotation was defined as torsional difference greater than 10° between the fractured and unaffected sides. Positive values were considered as external rotation and negative values as internal rotation. The intra-observer reliability determined in a pilot study was 0.9 approximately.
Figure 1.
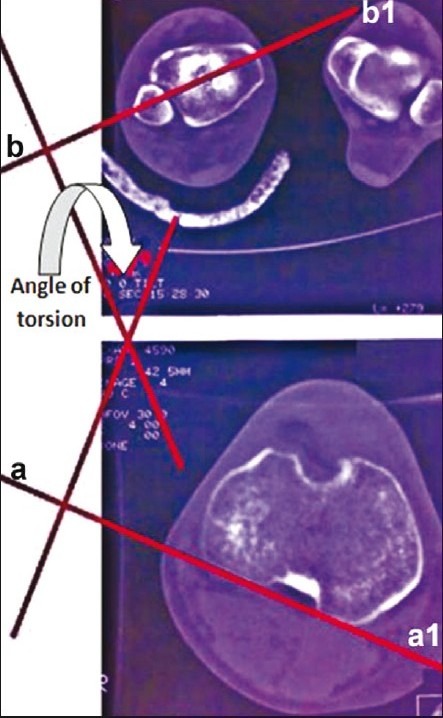
Measurement of tibial torsion using CT scanning. The proximal reference line is a line drawn as tangent to posterior tibial cortex in the cut just proximal to the fibular head (a, a1). The distal reference line is a line that connects the tibial and fibular centers in the cut just proximal to the tibial plafond (b, b1). The torsion angle is the angle between perpendicular lines to two reference lines
Figure 2.

A case with malrotation. (a) preoperative AP X-ray. (b) Preoperative lateral X-ray. (c) Postoperative AP X-ray. (d) Postoperative lateral X-ray. (e) Postoperative CT-scan shows proximal and distal reference lines. The torsion angle is the angle between perpendicular lines to two reference lines. This patient had 12° malrotation as compared to normal side CT scan
RESULTS
The mean age was 33.4 ± 13.3 years (range 17-67 years). Thirty-two cases had injured their right tibia and 28 cases had injured their left tibia. Based on the AO (Arbeitsgemeinschaft fuer Osteosynthesefragen) fracture classification, 30 fractures were AO type A, 21 AO type B, and 9 AO type C. All fractures were closed. Fifty-one fractures were caused by motor vehicle accident, seven by falling from a height, and two were the result of fights. In all cases, tibial fracture was associated with fibular fracture. However, fibula was not fixed in 53 patients. In 7 cases, fibula was fixed by plate and screws. All these 7 cases had very distal tibial fractures.
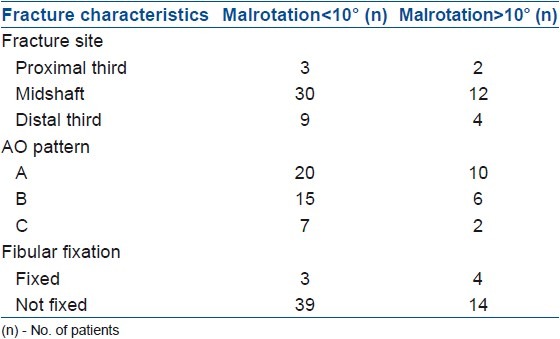
The mean torsional difference between the two tibiae was 8.2 ± 5.3° (23° external rotation to 18° internal rotation). Eighteen (30%) patients had malrotation of more than 10°. Malrotation was greater than 15° in 7 (11.6%) cases. Based on the classification described by Johner and Wruhs,13 the results were excellent (0°–5°) in 24, good (6°–10°) in 18, fair (11°–20°) in 16, and poor (>20°) in 2 cases. In other words, good or excellent rotational reduction was achieved in 70% of the patients. In the current study, we did not find any statistically meaningful relation between AO classification and fibular fixation, with malrotations greater than 10° (P<0.05) [Table 1].
Table 1.
Distribution of the patients based on the fracture site, AO pattern, and fibular fixation
DISCUSSION
To date, there is no clear definition of tibial torsion in the literature.9 Mikulicz and Le Damany defined it as a rotation of the proximal versus the distal articular axis in the transverse plane,10 which is currently used by several authors. Torsional malalignment following closed IM nailing for tibial fractures has been reported in several studies.4,7,9 However, the incidence and severity of tibial malrotation after IM nailing is not well documented. Also, definition of an acceptable range of deformity is contradictory.4 Usually, shortenings greater than 1 cm and angular or rotational deformities greater than 10° are considered to be malunion.4 Malrotations after using the locked tibial nails are rarely reported.7
It is believed that rotational malalignment(>10°) of the lower extremity can affect knee and ankle joints biomechanics and consequently leads to development and progression of degenerative changes.14 Some studies have documented the clinical association between torsional malalignment of tibia and osteoarthritis of knee and ankle, patellofemoral instability, patellar compression syndrome, pes planus, and gait abnormalities.4,6,8,9,15 Any of these conditions can seriously decrease the quality of life.4,6 Also, two separate studies by Puno et al. and Jend et al. reported that tibial malalignment is associated with poor functional outcomes.8,16 Despite these reports, there are several other studies that found no or poor correlation between malunion and osteoarthritis. Van der Schoot et al.17 and Bonnevialle et al.18 demonstrated that there was no correlation between tibial malrotation and arthrosis.
Probably the lack of a reliable and standard technique for clinical or radiographic assessment of tibial torsion contributes to the difficulty of accurately detecting this condition.4 Velazco et al.,19 Court-Brown et al.,20 and Puno et al.16 reported 0, 3, and 1 cases of clinically detected malrotation after tibial IM nailing in groups of 50, 125, and 51 patients, respectively. Alho et al. defined rotational malalignment as a difference greater than 15° between normal and injured tibiae, and reported two cases with malrotation after IM nailing of 93 tibial fractures.21 Williams et al.,22 Krishan et al.,23 Freedman and Johnson,24 O’Dwyer et al.,25 Pintore et al.,26 Lambiris et al.,27 and Tu et al.28 also reported similar findings. In a study of 21 patients with closed tibial shaft fractures treated with unreamed nailing, Krettek et al. reported 15% clinically detected malrotation.29 Detecting tibial malrotation clinically is very difficult and occult problems in many patients may lead to underestimation of the extent of the problem. In 1949, Hutter and Scott described the radiographic method using X-rays to measure the torsion11 which is a more accurate method compared to clinical investigation. Since then, several techniques have been described. In 1980, Jakob et al. described a method using CT scanning.10 Jend et al. proposed a similar method in 1981.8 Currently, CT is the gold standard for quantifying the torsion with excellent accuracy, and good inter- and intra-observer reliability and repeatability.4,8,10,30
There are few studies which measured tibial malrotation following IM nailing. Prasad et al. measured tibial torsion in 22 patients with tibial diaphyseal fractures treated with closed IM nailing. They found a difference of 8° or greater in 8 (36%) patients.9 In a study by Bonnevialle et al., torsional abnormalities and length discrepancies after diaphyseal tibial fractures were measured in 89 patients using the CT scanning method. They found that in 73% of the patients, the rotational alignment in fractured and intact limbs was the same, but the mean difference between injured and intact limbs in the remaining 27% of patients was 6.84°.18 Also, Poluski et al. determined the incidence and severity of torsional malalignment in 25 consecutive patients with tibial shaft fractures who underwent reamed IM nailing using CT scan. Their results revealed a mean absolute difference of 6.7° between injured and uninjured tibia. They found five cases with more than 10° malrotation.4 In the present study, we found 18 (30%) patients with malrotation of more than 10°. Incidence of tibial malrotation in our study is similar to that reported in previous studies. These findings suggest that current methods of intraoperative assessment of tibial torsion are not efficient, and it is crucial to develop new methods for accurate intraoperative measurement. Clementz and Magnusson described a method for measuring tibial torsion intraoperatively using fluoroscopy. They compared the rotational alignment of the knee in a true anteroposterior view with that of the ankle in a true mortise view.12 Although, they have shown good accuracy and repeatability of this method, there is no report of practical use of this technique yet.
We believe that our study had an acceptable sample size, but it was performed during a short period of time. A clinical and biomechanical long term followup study on the malrotated group would be helpful to improve our insight about the effects of tibial malrotation on the patient's gait and quality of life. We plan on performing a multicentric study to evaluate the incidence rate in other centers as well as investigate the causes of high incidence rate of malrotations in this study.
CONCLUSION
Tibial malrotation following IM nailing is a common finding. Postoperative CT scanning is the gold standard for measurement of the torsion, but the need for a method to evaluate the torsion intraoperatively is greatly felt. In this way we will be able to prevent malrotation and subsequent knee and ankle joint degeneration.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Lang GJ. Fractures of the tibial diaphysis. In: Kellam JF, editor. Orthopaedic Knowledge Update: Trauma. Rosemont, IL: AAOS; 2000. pp. 177–89. [Google Scholar]
- 2.Fortis AP, Dimas A, Lamprakis AA. Expandable nailing system for tibial shaft fractures. Injury. 2008;39:940–6. doi: 10.1016/j.injury.2008.01.022. [DOI] [PubMed] [Google Scholar]
- 3.Weninger P, Tschabitscher M, Traxler H, Pfafl V, Hertz H. Intramedullary nailing of proximal tibia fractures–an anatomical study comparing three lateral starting points for nail insertion. Injury. 2010;41:220–5. doi: 10.1016/j.injury.2009.10.014. [DOI] [PubMed] [Google Scholar]
- 4.Puloski S, Romano C, Buckley R, Powell J. Rotational malalignment of the tibia following reamed intramedullary nail fixation. J Orthop Trauma. 2004;18:397–402. doi: 10.1097/00005131-200408000-00001. [DOI] [PubMed] [Google Scholar]
- 5.Koo H, Hupel T, Zdero R, Tov A, Schemitsch EH. The effect of muscle contusion on cortical bone and muscle perfusion following reamed, intramedullary nailing: A novel canine tibia fracture model. J Orthop Surg Res. 2010;5:89. doi: 10.1186/1749-799X-5-89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Buckley R, Mohanty K, Malish D. Lower limb malrotation following MIPO technique of distal femoral and proximal tibial fractures. Injury. 2011;42:194–9. doi: 10.1016/j.injury.2010.08.024. [DOI] [PubMed] [Google Scholar]
- 7.Kahn KM, Beals RK. Malrotation after locked intramedullary tibial nailing: Three case reports and review of the literature. J Trauma. 2002;53:549–52. doi: 10.1097/00005373-200209000-00025. [DOI] [PubMed] [Google Scholar]
- 8.Jend HH, Heller M, Dallek M, Schoettle H. Measurement of tibial torsion by computer tomography. Acta Radiol Diagn (Stockh) 1981;22:271–6. doi: 10.1177/028418518102203a10. [DOI] [PubMed] [Google Scholar]
- 9.Prasad CV, Khalid M, McCarthy P, O’Sullivan ME. CT assessment of torsion following locked intramedullary nailing of tibial fractures. Injury. 1999;30:467–70. doi: 10.1016/s0020-1383(99)00132-1. [DOI] [PubMed] [Google Scholar]
- 10.Jakob RP, Haertel M, Stüssi E. Tibial torsion calculated by computerised tomography and compared to other methods of measurement. J Bone Joint Surg Br. 1980;62:238–42. doi: 10.1302/0301-620X.62B2.7364840. [DOI] [PubMed] [Google Scholar]
- 11.Hutter CG, Jr, Scott W. Tibial torsion. J Bone Joint Surg Am. 1949;31:511–8. [PubMed] [Google Scholar]
- 12.Clementz BG, Magnusson A. Fluoroscopic measurement of tibial torsion in adults. A comparison of three methods. Arch Orthop Trauma Surg. 1989;108:150–3. doi: 10.1007/BF00934258. [DOI] [PubMed] [Google Scholar]
- 13.Johner R, Wruhs O. Classification of tibial shaft fractures and correlation with results after rigid internal fixation. Clin Orthop Relat Res. 1983;178:7–25. [PubMed] [Google Scholar]
- 14.Eckhoff DG. Effect of limb malrotation on malalignment and osteoarthritis. Orthop Clin North Am. 1994;25:405–14. [PubMed] [Google Scholar]
- 15.Turner MS. The association between tibial torsion and knee joint pathology. Clin Orthop Relat Res. 1994;302:47–51. [PubMed] [Google Scholar]
- 16.Puno RM, Vaughan JJ, Stetten ML, Johnson JR. Long-term effects of tibial angular malunion on the knee and ankle joints. J Orthop Trauma. 1991;5:247–54. doi: 10.1097/00005131-199109000-00001. [DOI] [PubMed] [Google Scholar]
- 17.van der Schoot DK, Den Outer AJ, Bode PJ, Obermann WR, van Vugt AB. Degenerative changes at the knee and ankle related to malunion of tibial fractures.15-year follow-up of 88 patients. J Bone Joint Surg Br. 1996;78:722–5. [PubMed] [Google Scholar]
- 18.Bonnevialle P, Andrieu S, Bellumore Y, Challé JJ, Rongières M, Mansat M. Torsional abnormalities and length discrepancies after intramedullary nailing for femoral and tibial diaphyseal fracture. Computerized tomography evaluation of 189 fractures. Rev Chir Orthop Reparatrice Appar Mot. 1998;84:397–410. [PubMed] [Google Scholar]
- 19.Velazco A, Fleming LL. Open fractures of the tibia treated by the Hoffmann external fixator. Clin Orthop Relat Res. 1983;180:125–32. [PubMed] [Google Scholar]
- 20.Court-Brown CM, Christie J, McQueen MM. Closed intramedullary tibial nailing.Its use in closed and type I open fractures. J Bone Joint Surg Br. 1990;72:605–11. doi: 10.1302/0301-620X.72B4.2380211. [DOI] [PubMed] [Google Scholar]
- 21.Alho A, Ekeland A, Strømsøe K, Follerås G, Thoresen BO. Locked intramedullary nailing for displaced tibial shaft fractures. J Bone Joint Surg Br. 1990;72:805–9. doi: 10.1302/0301-620X.72B5.2211761. [DOI] [PubMed] [Google Scholar]
- 22.Williams J, Gibbons M, Trundle H, Murray D, Worlock P. Complications of nailing in closed tibial fractures. J Orthop Trauma. 1995;9:476–81. doi: 10.1097/00005131-199509060-00004. [DOI] [PubMed] [Google Scholar]
- 23.Krishan A, Peshin C, Singh D. Intramedullary nailing and plate osteosynthesis for fractures of the distal metaphyseal tibia and fibula. J Orthop Surg (Hong Kong) 2009;17:317–20. doi: 10.1177/230949900901700315. [DOI] [PubMed] [Google Scholar]
- 24.Freedman EL, Johnson EE. Radiographic analysis of tibial fracture malalignment following intramedullary nailing. Clin Orthop Relat Res. 1995;315:25–33. [PubMed] [Google Scholar]
- 25.O’Dwyer KJ, Chakravarty RD, Esler CN. Intramedullary nailing technique and its effect on union rates of tibial shaft fractures. Injury. 1994;25:461–4. doi: 10.1016/0020-1383(94)90273-9. [DOI] [PubMed] [Google Scholar]
- 26.Pintore E, Maffulli N, Petricciuolo F. Interlocking nailing for fractures of the femur and tibia. Injury. 1992;23:381–6. doi: 10.1016/0020-1383(92)90012-h. [DOI] [PubMed] [Google Scholar]
- 27.Lambiris E, Tyllianakis M, Megas P, Panagiotopoulos E. Intramedullary nailing: Experience in 427 patients. Bull Hosp J Dis. 1996;55:25–7. [PubMed] [Google Scholar]
- 28.Tu YK, Lin CH, Su JI, Hsu DT, Chen RJ. Unreamed interlocking nail versus external fixator for open type III tibia fractures. J Trauma. 1995;39:361–7. doi: 10.1097/00005373-199508000-00029. [DOI] [PubMed] [Google Scholar]
- 29.Krettek C, Schandelmaier P, Tscherne H. Nonreamed interlocking nailing of closed tibial fractures with severe soft tissue injury. Clin Orthop Relat Res. 1995;315:34–47. [PubMed] [Google Scholar]
- 30.Sayli U, Bölükbasi S, Atik OS, Gündogdu S. Determination of tibial torsion by computed tomography. J Foot Ankle Surg. 1994;33:144–7. [PubMed] [Google Scholar]