

Anomalous origin of the right coronary artery (RCA) arising from the pulmonary trunk (PT) is rare, with an expected incidence of 0.002%. Numerous modalities are available to aid in establishing the diagnosis, including echocardiography, digital subtraction angiography, magnetic resonance angiography, and computed tomography coronary angiography (CTCA). We describe a case of anomalous origin of the RCA in a 14-year-old girl, which was diagnosed with electrocardiographically gated CTCA.
CASE PRESENTATION
A 14-year-old girl presented for outpatient cardiologic evaluation with the chief complaint of dizziness for several months. The dizziness was exacerbated by physically demanding activities such as volleyball and soccer. She denied symptoms such as headache, chest pain, or apparent cardiac arrhythmias.
Physical examination revealed no abnormality. A baseline 12-lead electrocardiogram demonstrated normal sinus rhythm. The origin of the RCA could not be visualized on echocardiography. Electrocardiographically gated CTCA performed on a GE Lightspeed VCT scanner demonstrated an anomalous origin of the RCA from the PT (Figures 1 and 2).
Figure 1.

(a) Axial and (b) coronal oblique images from an electrocardiographically gated computed tomography coronary angiography demonstrate an anomalous origin of the right coronary artery (small arrow), which arises from the right aspect of the pulmonary trunk (large arrow).
Figure 2.
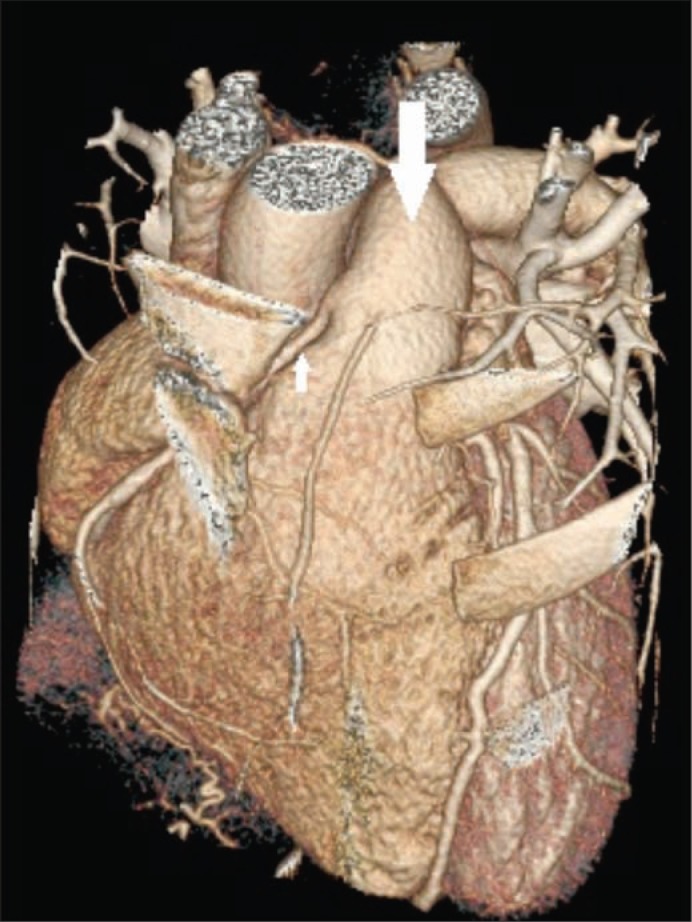
Three-dimensional maximum intensity projection–reformatted image from electrocardiographically gated computed tomography coronary angiography demonstrates anomalous origin of the right coronary artery (small arrow) off of the pulmonary trunk (large arrow).
The patient underwent surgical reimplantation of the anomalous RCA into the aorta (Figure 3). Six weeks following reimplantation, a cardiac stress test was normal, and she was released to resume full activities.
Figure 3.
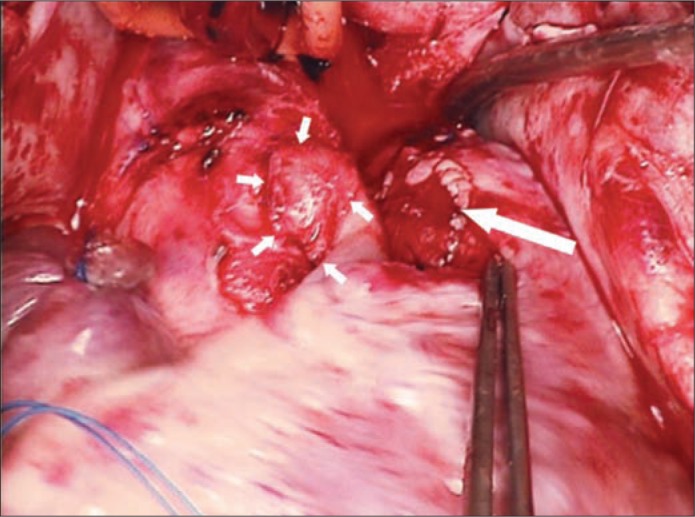
Intraoperative photograph shows the reimplanted anomalous right coronary artery (small arrows) as well as the pericardial patch on the pulmonary trunk (large arrow).
DISCUSSION
Variations in coronary artery anatomy are common in the general population. However, the term anomalous is used to describe any variation that is present in <1% of the population. Congenital coronary artery anomalies are present in approximately 0.6% to 1.3% of adults undergoing coronary angiography and rarely involve the RCA (1). Of anomalies involving the RCA, a high anterior take-off from the aorta is most common and is usually asymptomatic. Ectopic origin of the RCA from the noncoronary sinus, left coronary sinus, and PT also occur, though less frequently.
Anomalous origin of a coronary artery from the PT, of which four types have been described, is extremely rare in the general population. An anomalous left coronary artery arising from the PT is the most common of these and typically results in left ventricular ischemia and heart failure early in life. Anomalous RCA arising from the PT is rarer still, with an estimated incidence in the general population of 0.002% (2, 3). Only about 70 cases have been reported (4). Anomalous origin of both coronary arteries from the PT and an accessory coronary artery that arises from the PT have also been described and are usually fatal early in life.
Cases of anomalous origin of the RCA from the PT are usually treated surgically. The most common surgical procedure, performed on over half of all documented cases, is a button-type excision of the anomalous RCA in the PT with reimplantation into the aorta (4). Intrapulmonary tunnel repair, consisting of an intrapulmonary artery baffle with an autologous pericardial patch, has also been described. Additional surgical techniques include complete ligation of the anomalous RCA proximally with insertion of a saphenous vein conduit from the aorta to the distal RCA (5–9).
References
- 1.Misuraca L, Rutigliano D, Pestrichella V, Contegiacomo G, Balbarini A. A very rare congenital abnormality: double right coronary artery. A case report. J Cardiovasc Med (Hagerstown) 2009;10(8):643–645. doi: 10.2459/JCM.0b013e32832ce97d. [DOI] [PubMed] [Google Scholar]
- 2.Brooks HSJ. Two cases of an abnormal coronary artery of the heart arising from the pulmonary artery: with some remarks upon the effect of this anomaly in producing cirsoid dilatation of the vessels. J Anat Physiol. 1885;20(Pt 1):26–29. [PMC free article] [PubMed] [Google Scholar]
- 3.Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21(1):28–40. doi: 10.1002/ccd.1810210110. [DOI] [PubMed] [Google Scholar]
- 4.Williams IA, Gersony WM, Hellenbrand WE. Anomalous right coronary artery arising from the pulmonary artery: a report of 7 cases and a review of the literature. Am Heart J. 2006;152(5):1004.e9–e17. doi: 10.1016/j.ahj.2006.07.023. [DOI] [PubMed] [Google Scholar]
- 5.Luisi SV, Ashraf MH, Gula G, Radley-Smith R, Yacoub M. Anomalous origin of the right coronary artery with aortopulmonary window: functional and surgical considerations. Thorax. 1980;35(6):446–448. doi: 10.1136/thx.35.6.446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rowe GG, Young WP. Anomalous origin of the coronary arteries with special reference to surgical treatment. J Thorac Cardiovasc Surg. 1960;39:777–780. [PubMed] [Google Scholar]
- 7.Chantepie A, Lavigne G, Marchand M, Hazan E, Morand P. Right coronary artery arising from the pulmonary artery. Surgical treatment. Arch Mal Coeur Vaiss. 1982;75(8):925–932. [PubMed] [Google Scholar]
- 8.Kautzner J, Veselka J, Rohac J. Anomalous origin of the right coronary artery from the pulmonary trunk: is surgical reimplantation into the aorta a method of choice? Clin Cardiol. 1996;19(3):257–259. doi: 10.1002/clc.4960190324. [DOI] [PubMed] [Google Scholar]
- 9.Veselka J, Widimský P, Kautzner J. Reimplantation of anomalous right coronary artery arising from the pulmonary trunk leading to normal coronary flow reserve late after surgery. Ann Thorac Surg. 2003;76(4):1287–1289. doi: 10.1016/s0003-4975(03)00561-7. [DOI] [PubMed] [Google Scholar]