

Abstract
OBJECTIVES
To describe sleep patterns in older adults living in assisted living facilities (ALFs) and to explore the relationship between sleep disturbance and quality of life, functional status, and depression over 6 months of follow-up.
DESIGN
Prospective, observational cohort study. SETTING: Eighteen ALFs in the Los Angeles area. PARTICIPANTS: One hundred twenty-one ALF residents aged 65 and older (mean age 85.3, 86% female, 88% non-Hispanic white).
MEASUREMENTS
Data were collected at baseline and 3 and 6 months after enrollment. Data collected were demographics, physical and cognitive functioning, depression, quality of life, comorbidities, medications, and subjective (i.e., questionnaires) and objective (i.e., 3 days and nights of wrist actigraphy) measures of sleep.
RESULTS
Sixty-five percent of participants reported clinically significant sleep disturbance on the Pittsburgh Sleep Quality Index, and objective wrist actigraphy confirmed poor sleep quality. In regression analyses including sleep variables and other predictors, more self-reported sleep disturbance at baseline was associated with worse health-related quality of life (Medical Outcomes Study 12-item Short Form Survey Mental Component Summary score) and worse depressive symptoms five-item Geriatric Depression Scale at follow-up. Worse nighttime sleep (according to actigraphy) at baseline was associated with worse activities of daily living functioning and more depressive symptoms at follow-up.
CONCLUSIONS
Sleep disturbance is common in older ALF residents, and poor sleep is associated with declining functional status and quality of life and greater depression over 6 months of follow-up. Studies are needed to determine whether improving sleep in ALF residents will result in improvements in these outcomes. Well-established treatments should be adapted for use in ALFs and systematically evaluated in future research.
Keywords: sleep, assisted living facilities, depression, quality of life, functional status
Older people increasingly reside in assisted living facilities (ALFs) when they are unable to live independently but do not require nursing home (NH)-level care.1 The specific services offered at ALFs are somewhat variable but typically include congregate meals, housekeeping, and personal care assistance. ALFs typically provide private or semiprivate rooms. ALF residents typically function more independently than nursing home residents and have greater autonomy in their daily living. Estimates of the number of ALFs vary considerably based on how facilities are defined, ranging from 11,500 to 50,000 facilities nationwide. The reported number of ALF residents in the United States varies from 611,000 to more than 1 million.2,3 Evidence suggests that ALF residents are at a vulnerable period in their lives, with a high risk for further functional decline and subsequent nursing home placement;4,5 24% to 40% of ALF residents are discharged to a long-term care facility annually.6
A growing literature suggests that sleep disturbance is common in older people and is a significant risk factor for poor health, functional impairment, falls, depression, poor quality of life, and mortality in independently living and institutionalized older people.7–11 Although sleep impairment in the ALF setting has not been well studied, the few published studies have found that insomnia and daytime sleepiness have a significant negative effect on functioning.12,13 A cross-sectional pilot study found that ALF residents had more-fragmented nighttime sleep than home-dwelling older adults.14 In addition, the age and health status of ALF residents places them at high risk for sleepdisturbance and sleep disorders. Numerous studies demonstrate that longer sleep onset latency, more nighttime wakefulness, less deep sleep, earlier morning awakening, and more daytime napping are associated with advancing age15–19 and that most primary sleep disorders (e.g., sleep apnea, restless legs syndrome) increase in prevalence with age as well.20,21 A prospective, observational cohort study was performed in older people residing in ALFs in the Los Angeles area. The purpose of this study was to describe sleep patterns in older people residing in ALFs and to determine whether sleep disturbance is associated with a decline in quality of life, functional status, and depression over a 6month follow-up period. It was hypothesized that poor self-reported sleep quality, disrupted nighttime sleep, and excessive daytime sleeping (according to actigraphy) would be common in ALF residents; abnormal sleep–wake patterns at baseline (more daytime sleeping, less nighttime sleep) would be associated with worse quality of life, more functional impairment, and more depression at baseline; and sleep disturbance at baseline would be associated with quality of life, functional status, and depression at 3 and 6 months of follow-up.
METHODS
Study Design and Setting
The study design was a prospective, observational cohort study in older people residing in a sample of ALFs located in the Los Angeles area. Eighteen ALFs participated in the study. All but one facility were licensed by the state of California, and all but one facility were proprietary for-profit facilities. The number of beds in the ALF’s ranged from 60 to 239. All facilities offered congregate meals, housekeeping, laundry, and transportation services. Participant recruitment was performed between April 2006 and March 2008. The Veterans Affairs Greater Los Angeles Healthcare System institutional review board approved all research methods. Written informed consent was obtained from all participants.
Participants
The study was introduced to residents of participating ALFs during a 30-minute presentation about sleep research during which the principal investigator (CA) explained the study. Residents aged 65 and older were invited to participate. Residents were excluded from participation if they were unable to communicate with research staff (e.g., had aphasia or were unable to speak sufficient English to complete study measures) or were unable to provide informed consent.
Sleep Measures
Subjective sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI).22 The PSQI is an 18-item questionnaire that includes subscales to estimate subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction (score range 0–21; scores >5 indicate sleep disturbance). In this study, a three-subscale scoring system that has superior psychometric properties to the original seven-subscale version was used.23 The PSQI format asked participants to answer questions regarding their sleep over the previous month. Three questions were added to the PSQI to query specifically about noise, light, or other people causing awakenings from sleep, because these factors disrupt sleep in institutional settings such as nursing homes and hospitals.24,25 These additional items were not included in the scoring of the PSQI.
Participants were screened for sleep-related disorders common in older people, including sleep-disordered breathing (sleep apnea), using the Berlin Sleep Apnea Questionnaire,26 and restless legs syndrome (RLS, an unpleasant urge to move the legs when at rest while awake, generally in the evening), using a four-item RLS scale.27 The Berlin scale results in a dichotomous score of high versus low risk for sleep-disordered breathing. The RLS scale was converted into a dichotomous variable indicating the presence or absence of RLS symptoms.
To obtain an objective measure of sleep, participants wore a wrist actigraph (Octagonal Sleep Watch-L, Ambulatory Monitoring, Inc, AMI, Ardsley, NY) on their dominant arm (unless paralyzed or otherwise unable to use the dominant arm) for 3 consecutive days and nights. Raw actigraphy data (1-minute epoch length) was reviewed visually to eliminate technical (i.e., device failure) and situational (i.e., device was removed) artifact before scoring sleep using a validated algorithm within commercially available software (Action4 software, AMI). Here variables from automatic sleep scoring are reported using time above threshold (TAT; default algorithms), based on prior literature28–30 and data comparing actigraphy with standardized observations of sleep–wake from prior work. Participants were asked to record their bedtime and rise times each day the actigraph was worn to determine nighttime and daytime periods for scoring and analysis.
Functional Status, Quality of Life, and Depression Measures
Functional status was measured according to self-report using the Personal Self-Maintenance scale.31 Scores were calculated for activities of daily living (ADLs, score range 0–7) and instrumental activities of daily living (IADLs, score range 0–8). Questions about ADLs ask participants about whether they need assistance for eating, dressing, grooming, bathing, transferring in and out of bed, mobility, and continence. Questions about IADLs ask participants about whether they need assistance using the telephone, getting to places out of walking distance, shopping, preparing meals, doing housework, doing laundry, taking care of their medicines, and managing money.
The Medical Outcomes Study 12-item Short-form Health Survey (SF-12),32,33 was used as a measure of health-related quality of life. The SF-12 consists of two subscales: the physical component summary score and the mental component summary score (scores for each subscale range from 0–100; higher scores indicate better functioning).
The five-item version of the Geriatric Depression Scale34 (GDS-5; range 0–5; scores ≥2 suggest depression) was administered to assess symptoms of depression.
Other Demographic and Clinical Measures
Basic demographic information was recorded for all participants, including age, sex, ethnicity, and length of stay in the ALF. Cognitive functioning was measured using the Mini-Mental State Examination (MMSE; a 20-item measure of general cognitive functioning assessing five cognitive domains; score range 0–30; score o24 suggests cognitive impairment).35 Medical comorbidity was assessed in two ways. First, a self-report questionnaire36 modeled after the Charlson Comorbidity Index37 was used (16-item comorbidity questionnaire, range 0–32, higher scores indicating greater comorbidity). Because the Charlson index does not include some conditions that are common in older adults (e.g., hypertension), a method employed in other studies as a proxy for medical burden was also used, the total number of medications taken.38,39
To obtain medication data, participants were asked to record all medications they took during the days and nights that the actigraph was worn. For participants who received their medications from ALF staff (n = 22), medication data were abstracted from the facilities’ medication log(s). Medications taken in the evening or night with known sedating properties (including sedative-hypnotics, sedating antide-pressants, sedating antipsychotics, and other sedating agents) were identified for each participant as medications probably used for sleep.
Procedures
After enrollment, each participant completed a baseline assessment. This assessment included 3 days and nights of wrist actigraphy and a battery of self-report questionnaires (described above). Follow-up assessments were conducted 3 and 6 months from the date of enrollment. The follow-up assessments included all components of the baseline assessment. Trained research personnel collected all data in the ALF.
Data Analysis
Actigraphy variables were averaged over the 3 days and nights of recording. Nighttime was defined as the period between reported bedtime and reported rise time for each recorded night. Conversely, daytime was defined as the period between reported rise time and reported bedtime for each recorded day. Key actigraphy variables used in analyses were nighttime hours asleep, nighttime percent sleep (hours asleep/hours between bedtime and rise time), nighttime number of awakenings, and daytime hours and percent sleep (hours asleep/hours between rise time and bedtime). Key self-reported sleep variables included the PSQI total score and the dichotomous scores on the Berlin sleep apnea questionnaire (0 = low risk, 1 = high risk) and the RLS symptom questionnaire (0 = no RLS, 1 = RLS).
Data were analyzed using SPSS 16.0 (SPSS, Inc., Chicago, IL). Using univariate analyses (Pearson correlations and t-tests), relationships between the actigraphically estimated and self-reported sleep measures (listed above); participant characteristics (age, sex, ethnicity, comorbidity index, use of sleep medications); and measures of functional status (ADL, IADL), quality of life (SF-12 physical and mental component summary scores), and depression (GDS-5) were tested for. The sleep and descriptive variables with the strongest relationships (using P<.10 as the cutoff) were then entered into regression models predicting functional status, quality of life, and depression to determine whether sleep variables remained significant independent predictors of these outcomes when accounting for the effects other significant variables. All variables with bivariate associations (based on P<.10) with the outcome were included in regression models unless two independent variables were highly correlated (correlation coefficient >0.70) or represented overlapping measures (PSQI total and subscale scores, total medications and Charlson comorbidity index). In such cases, the variable with the strongest association with the outcome of interest was retained and the other excluded. Those with high collinearity (reflected as tolerance <0.10) were investigated further and excluded if regression coefficients changed dramatically when other independent variables were removed from the model. All remaining variables were included in the final regression models.
To assess whether baseline sleep was related to functional status, quality of life, and depression over the 6-month follow-up period, the baseline regression models were repeated using the follow-up values as independent variables and adding in the baseline value of the variable of interest as a dependent variable (i.e., baseline scores were included as predictors of follow-up scores). This allowed the relationship between baseline sleep and outcomes of interest to be evaluated, controlling for the effect of baseline levels of that outcome. Again, models were evaluated for collinearity (described above). For all statistical testing, P<.05 was used as the criterion for statistical significance.
RESULTS
Baseline Characteristics of Study Sample
One hundred twenty-one participants were enrolled in the study from the 18 participating ALFs (Table 1). Seventyfour percent of participants had resided in the ALF for 2 years or less. Mean scores on the ADL and IADL scales indicated dependency in approximately one ADL and three IADLs, indicating mild to moderate functional impairment. Dependency was reported most commonly for preparing meals (95%), shopping (56.2%), continence (51.2%), housekeeping (39.7%), taking medications (33.1%), and laundry (32.2%). Nineteen percent (n = 23) of participants scored in the cognitively impaired range on the MMSE (o24), and 30% (n = 36) scored above the cutoff for depression on the GDS-5 (≥2). Participant flow, deaths, and other losses to follow-up over the course of the study are shown in Figure 1.
Table 1.
Characteristics of Assisted Living Facility Residents at Baseline (N = 121)
| Characteristic | Value |
|---|---|
| Age, mean ± SD | 85.3 ± 6.5 |
| Female, n (%) | 87 (86) |
| Non-Hispanic white, n (%) | 106 (88) |
| Years of residence in the assisted living facility, mean ± SD | 2.6 ± 2.9 |
| Charlson Comorbidity Index, mean ± SD (range 0–32) | 1.4 ± 1.6 |
| Number of medications taken, mean ± SD* | |
| Routine medications | 6.3 ± 3.0 |
| As-needed medications | 0.4 ± 0.8 |
| Activities of daily living scale score, mean ± SD (range 0–7) | 6.3 ± 0.7 |
| Instrumental activities of daily living scale score, mean ± SD (range 0–8) |
5.3 ± 1.5 |
| Mini-Mental State Examination score, mean SD (range 0–30) |
26.4 ± 3.1 |
| 5-item Geriatric Depression Scale score, mean ± SD (range 0–5) |
1.1 ± 1.2 |
| Medical Outcomes Study 12-item Short-Form Health Survey score, mean ± SD (range 0–100) |
|
| Physical Component Summary | 38.1 ± 12.1 |
| Mental Component Summary | 52.9 ± 11.7 |
Total number of routine and as-needed medications taken during the 3-day actigraphy recording period. Medication data were not available for four participants.
SD = standard deviation.
Figure 1.
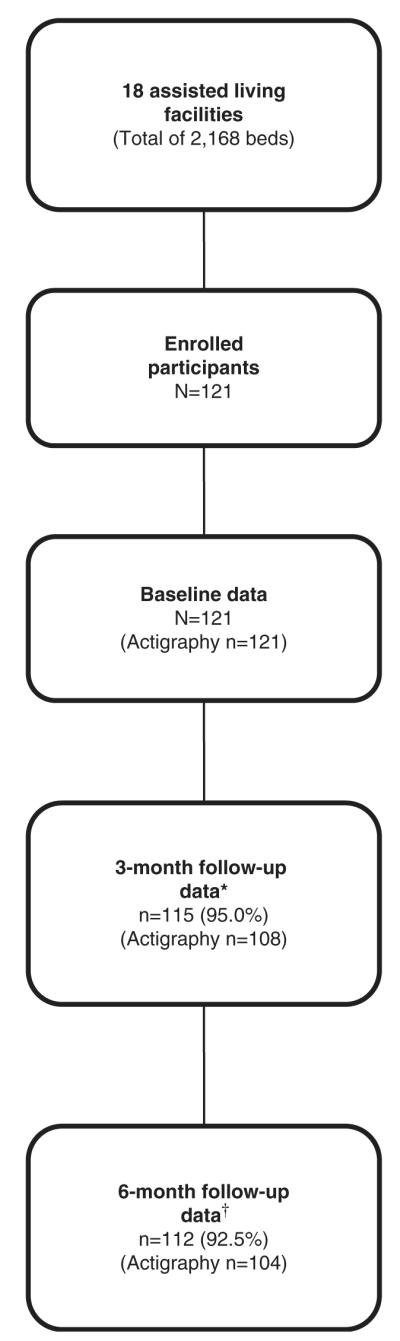
Participant flow through the study. 3-month follow-up data not available from two participants who could not be reached, two who were too ill to complete the assessments, one who withdrew from the study, and one who died. w6-month follow-up data not available from two participants who refused to complete the assessment, three who withdrew from the study, and four who died.
Self-Reported Sleep Quality
Descriptive information about self-reported and actigraphically measured sleep are shown in Table 2. Fifty-eight (65%) participants had a total PSQI score greater than 5, reflecting significant sleep disturbance. On the PSQI, the most commonly reported factors contributing to trouble sleeping included waking up in the middle of the night or early morning (60.3%) and the inability to fall asleep within 30 minutes (59.5%). Aside from these difficulties, the most commonly reported factors contributing to trouble sleeping over the previous month were getting up to use the bathroom (73.6%), noise (33.3%), and pain (32.2%). Based on review of medication logs, 36% (n = 44) of participants took sedating medications in the evening or night (presumably for sleep), most commonly benzodiazepines (n = 15, 12%). Participants also used nonbenzodiazepine hypnotic agents (n = 10, 8%), antidepressants (n = 10, 8%), antihistamines (n = 6, 5%), anticonvulsants (n = 6, 5%), and other sedating medications (n = 6, 5%).
Table 2.
Sleep Measures in Assisted Living Facility Residents (N=121)
| Variable | Value |
|---|---|
| Participant self-reported measures | |
| Pittsburgh Sleep Quality Index score, mean ± SD | |
| Total (range 0–21) | 8.0 ± 4.3 |
| Perceived Sleep Quality subscale (range 0–9) | 3.3 ± 2.4 |
| Sleep Efficiency subscale (range 0–6) | 2.2 ± 2.1 |
| Daily Disturbance subscale (range 0–6) | 2.7 ± 1.0 |
| Restless legs syndrome, n (%) | 14 (12) |
| High-risk score on the Berlin Sleep Apnea scale, n (%) | 39 (32) |
| Taking sedating medications at night, n (%)* | 44 (36) |
| Wrist actigraphy, mean ± SD† | |
| Nighttime total sleep time, hours | 6.3 ± 1.6 |
| Nighttime sleep percent (hours asleep/hours from bedtime to rise time) |
77 ± 17 |
| Nighttime number of awakenings | 11.4 ± 5.0 |
| Daytime total sleep time, hours | 1.5 ± 1.1 |
| Daytime sleep percent (hours asleep/hours from rise time to bedtime) |
10 ± 8 |
Medication data unavailable for four participants.
Nighttime defined as the interval from reported bedtime to reported rise time; daytime defined as the interval from reported rise time to reported bedtime.
SD = standard deviation.
Baseline Sleep Disturbance, Functional Status, Quality of Life, and Depression
Significant bivariate associations between sleep measures (Table 2), participant characteristics (Table 1), and baseline functional status, quality of life, and depression are shown in Table 3. Subjective and objective measures of sleep were significantly correlated with functional status, quality of life, and depression measures in bivariate analyses.
Table 3.
Relationships (P<.10) Between Descriptive and Sleep Variables and Measures of Functional Status, Health-Related Quality of Life, and Depression at Base-line in Assisted Living Facility Residents (N=121)
| Baseline Measure | r/t* | P-Value |
|---|---|---|
| SF-12 Physical Component Summary score | ||
| Charlson Comorbidity Index | −0.160 | .08 |
| Total number of medications taken | −0.287 | .002 |
| Berlin Sleep Apnea scale, high-risk scores | t=3.14 | .002 |
| PSQI total score | −0.186 | .04 |
| PSQI daily disturbance subscale score | −0.376 | <.001 |
| Actigraphy: daytime sleep percent† | −0.172 | .06 |
| SF-12 Mental Component Summary Score | ||
| Restless Legs Syndrome scale, positive responses | t=2.65 | .02 |
| PSQI score | −0.228 | .01 |
| PSQI daily disturbance subscale score | −0.267 | .003 |
| Actigraphy: number of nighttime awakenings‡ | −0.316 | <.001 |
| Activities of daily living scale, total score | ||
| MMSE score | 0.161 | .08 |
| PSQI daily disturbance subscale score | −0.173 | .06 |
| Actigraphy: nighttime total sleep time‡ | 0.191 | .04 |
| Actigraphy: percentage nighttime sleep‡ | 0.271 | .003 |
| Instrumental activities of daily living scale, total score | ||
| Sex | T= −2.10 | .04 |
| Race or ethnicity (non-Hispanic white/all others) | T = −2.49 | .08 |
| MMSE score | 0.362 | <.001 |
| Actigraphy: nighttime total sleep time‡ | 0.176 | .05 |
| Actigraphy: nighttime percent sleep‡ | 0.291 | .001 |
| Actigraphy: nighttime number of awakenings‡ | − 0.248 | .006 |
| 5-item Geriatric Depression Scale total score | ||
| Sex | t=1.87 | .06 |
| Charlson Comorbidity Index | 0.174 | .06 |
| Berlin Sleep Apnea scale, high risk score | T = −2.25 | .03 |
| PSQI total score | 0.268 | .003 |
| PSQI sleep efficiency subscale score | 0.175 | .06 |
| PSQI perceived sleep quality subscale score | 0.195 | .03 |
| PSQI daily disturbance subscale score | 0.279 | .002 |
| Actigraphy: number of nighttime awakenings‡ | 0.208 | .02 |
Pearson correlations (r) used for continuous variables; t-tests used for categorical variables.
Daytime defined as the interval from reported rise time to reported bedtime;
Nighttime defined as the interval from reported bedtime to reported rise time.
PSQI = Pittsburgh Sleep Quality Index; MMSE = Mini-Mental State Examination.
Baseline variables that were significantly correlated with each outcome variable (SF-12 mental and physical components, ADLs, IADLs, and GDS-5; Table 3) were considered for inclusion in regression models using the procedure described above to develop the most-appropriate model for each outcome. In these multivariable regression models, several baseline sleep variables were associated with these outcomes. At baseline, high risk for RLS (t = −2.58; P =.01) and more nighttime awakenings (t = −2.96; P =.004) were associated with worse baseline quality of life based on the SF-12 mental component score (model-adjusted coefficient of determination (R2) = 0.17, P<.001). High sleep apnea risk (t =2.25; P =.03), greater daily dysfunction based on the PSQI (t = −3.47; P =.001), and more medications taken (t = −2.25; P =.026) were associated with worse baseline quality of life based on the SF-12 physical component score (modeladjusted R2 = 0.21, P<.001). Lower nighttime percentage sleep (t = 2.65, P =.009) was associated with worse base-ine ADL scores (model-adjusted R2 = 0.09, P =.004), and higher MMSE scores (t = 3.47, P =.001) were associated with better baseline IADL scores (model-adjusted R2 = 0.20, P<.001). More sleep disturbance based on PSQI total score (t = 2.49, P =.01) was associated with more baseline depressive symptoms (model-adjusted R2 = 0.13, P =.001). No other predictors were significant in these models.
Baseline Sleep Disturbance and Functional Status, Quality of Life, and Depression at 3- and 6-Month Follow-Up
Using the regression models described above, baseline sleep measures and patient characteristics were examined as predictors of 3- and 6-month outcomes. As expected, baseline levels of each outcome measure were strong predictors of that same measure at 3- and 6-month follow-up. Table 4 summarizes the regression models for each outcome at each time point. In addition, higher PSQI daily dysfunction predicted poorer quality of life based on SF-12 mental component scores at 6 months but not at 3 months. Lower percentage nighttime sleep predicted lower ADL functioning at 3 and 6 months, worse self-reported sleep quality, more nighttime awakenings (according to actigraphy), and high sleep apnea risk predicted more depressive symptoms at 3 months, and worse self-reported sleep quality and more nighttime awakenings (according to actigraphy) predicted more depressive symptoms at 6 months. Female sex and more comorbidities at baseline were also significant predictors of depression at 3 months. Sleep measures did not predict SF-12 physical component scores at 3 (model-adjusted R2 = 0.43, P<.001) or 6 (model-adjusted R2 = 0.42, P<.001) months or IADL functioning at 3 (model-adjusted R2 = 0.56, P<.001) or 6 (model-adjusted R2 = 0.46, P<.001) months.
Table 4.
Regression Models Predicting Health-Related Quality of Life (Medical Outcomes Study 12-Item Short-Form Survey (SF-12) Mental and Physical Component Scores), Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) Scores, and Depression (5-Item Geriatric Depression Scale (GDS-5) Score) at 3- and 6-Month Follow-Up
| 3-Month Follow-Up |
6-Month Follow-Up |
|||||
|---|---|---|---|---|---|---|
| B (SE) | t | P-Value | B (SE) | T | P-Value | |
| Outcome Variable: | ||||||
| SF-12 Mental Component score | ||||||
| Baseline Predictor | ||||||
| PSQI Daily Dysfunction subscale | −1.01 (1.02) | −0.99 | .32 | −2.21 (1.04) | −2.12 | .04 |
| Number of nighttime awakenings* | −0.29 (0.20) | −1.43 | .16 | 0.13 (0.21) | 0.64 | .52 |
| Restless legs syndrome score | −0.05 (1.00) | −0.05 | .96 | −0.58 (1.01) | −0.57 | .57 |
| SF-12 Mental Component score | 0.52 (0.10) | 5.40 | <.001 | 0.54 (0.10) | 5.54 | <.001 |
| Outcome Variable: | ||||||
| ADL score | ||||||
| Baseline Predictor: | ||||||
| PSQI Daily Dysfunction Subscale | −0.04 (0.07) | −0.55 | .58 | −0.19 (0.09) | −2.15 | .03 |
| Percent nighttime sleep* | 0.01(0.004) | 2.56 | .01 | 0.01(0.01) | 2.50 | .01 |
| Mini-Mental State Examination score | 0.02 (0.02) | −0.84 | .23 | 0.04 (0.03) | 1.39 | .17 |
| ADL score (baseline) | 0.63 (0.11) | 6.01 | <.001 | 0.56 (0.12) | 4.55 | <.001 |
| Outcome Variable: | ||||||
| GDS-5 score | ||||||
| Baseline Predictor: | ||||||
| PSQI total score | 0.06 (0.02) | 2.96 | .004 | 0.07 (0.02) | 3.13 | .002 |
| Nighttime number of awakenings* | 0.06 (0.02) | 3.26 | .002 | 0.07 (0.02) | 3.51 | .001 |
| Berlin questionnaire | −0.41 (0.20) | −2.09 | .04 | −0.21 (0.21) | −1.00 | .32 |
| Sex | 0.43 (0.20) | 2.15 | .03 | 0.14 (0.22) | 0.62 | .54 |
| Charlson Comorbidity Index | 0.14 (0.06) | 2.36 | .02 | 0.09 (0.07) | 1.37 | .17 |
| GDS-5 score | 0.41 (.08) | 5.02 | <.001 | 0.56 (0.09) | 6.34 | <.001 |
Actigraphy variables based on mean over 3-days of recording.
Statistics for each regression model:
SF-12 Mental Component score 3-month adjusted coefficient of determination (R2) = 0.29, P<.001; degrees of freedom (df) = 4,105; 6-month adjusted R2 = 0.30, P<.001; df = 4,102.
ADL score 3-month adjusted R2 = 0.36, P<.001; df = 4,106; 6-month adjusted R2 = 0.27, P<.001; df = 4,105.
GDS-5 score 3-month adjusted R2 = 0.34, P<.001; df = 6,105; 6-month adjusted R2 = 0.43, P<.001; df = 6,104.
SE = standard error; PSQI = Pittsburgh Sleep Quality Index.
DISCUSSION
This prospective study of sleep in residents of ALFs in the Los Angeles area found that sleep disturbance, based on self-report and objective wrist actigraphy, was common; nearly two-thirds of participants reported symptoms of clinically significant sleep disturbance based on a total PSQI score greater than 5. This rate of sleep disturbance is higher than expected based on epidemiological studies of sleep in community-dwelling older adults.9 Not surprisingly, participants specifically noted difficulty falling asleep and staying asleep, as well as getting up to use the bathroom, noise and pain as factors that commonly affected their sleep. This probably reflects high rates of nocturia and chronic conditions that cause pain, in addition to noises that are common in instutional settings at night. Although noise resulting from the institutional environment (e.g., caregiving staff) appears to play an important role in the disruption of sleep in older persons in nursing homes,25 in the ALF, residents reported noises that are likely to disrupt sleep in a home setting such as traffic and neighbors. Although it is unclear from this study whether these residents suffered from poor sleep before transition to the ALF or whether sleep problems developed after that transition, some participants noted that the transition to the ALF facility coincided with the onset of their sleep-related problems.
Approximately one-third of participants used a sedating medication in the evening, most commonly benzodiazepines. These rates are consistent with community-based studies, which show rates of hypnotic use ranging form 12% in a biracial community-dwelling cohort40 to 46% in adults aged 80 and older.41 Use of these medications (as a group) was not associated with subjective or objective measures of sleep, quality of life, functional status, or depression in the current study. There was not an adequate number of participants on any particular class of sedating medications to test for a unique effect of medication class. Given the possible risks of benzodiazepine medications in older adults,42 use of these agents at night to help with sleep should be considered cautiously in ALF residents. Non-pharmacological intervention studies have not been performed to address sleep problems in ALF residents, so it is not clear whether these treatments can be adapted effectively for use in ALF settings. Future studies will need to explore the best methods for addressing sleep problems in ALF residents and to evaluate the effect of pharmacological and nonpharmacological interventions on sleep in terms of their effect on important outcomes, including depression, quality of life, and functional independence.
At baseline, sleep variables were related to multiple clinical measures in bivariate analyses. Poor self-reported sleep quality and poor objectively measured sleep were as-sociated with poorer quality of life, lower functional status, and higher levels of depression. When regression models to account for clinical and sleep measures simultaneously were developed and tested, it was found that sleep variables remained signifcant in most cases. In addition, some sleep measures predicted qualtiy of life, functional status, and depression at 3- and 6-month follow-up. The overall pattern of results suggests that daily dysfunction (as measured according to the PSQI) and poor quality nighttime sleep (measured using wrist actigraphy) were associated with lower quality of life at baseline. With the exception of PSQI daily disfunction predicting lower SF-12 mental component scores at 6 months, these relationships did not persist over time. RLS symptoms were related to baseline quality of life but did not predict quality-of-life scores at 3- and 6-month follow-up. Nonetheless, RLS and sleep apnea should be further explored in studies using objective monitoring of sleep disorders to ascertain the true prevalence and severity of these conditions.
Poor-quality nighttime sleep at baseline, based on low nightime sleep percent (according to actigraphy) was related to lower functioning (greater dependency in ADLs) at baseline and at 3- and 6-month follow-up. Daily dysfunction (based on PSQI) at baseline was associated with functional status only at 6 months. Sleep measures were not related to IADL functioning at baseline or follow-up in regression models. As in prior research, participants with worse cognitive functioning had greater IADL dependencies.43
An important finding from this study was that poor self-reported sleep quality (based on PSQI total score) at baseline was associated with more depressive symptoms at baseline and at 3- and 6-month follow-up. This finding is consistent with other studies showing that poor sleep predicts persistence of depression in older adults.44 In addition, baseline nighttime number of awakenings (based on actigraphy) was not an independent predictor of depression at baseline, although it predicted depressive symptoms at 3- and 6-month follow-up. This finding suggests that improving sleep quality has the potential to reduce future depressive symptoms.
Taken together, these findings suggest that sleep has a strong bivariate association with quality of life, functional status, and depression and that poor sleep may be a predictor of subsequent decline in functional status and increase in depression. Because functional status decline and depression are factors that can lead to nursing home placement and falls,45–47 improving sleep quality may delay these negative outcomes.
This study has several limitations, including the use of a nonrepresentative sampling method and the exclusion of individuals who were not able to self-consent. These methods resulted in underrepresentation of the more-impaired ALF residents, and the use of a presentation on sleep reserach to identify potential participants may have contributed to oversampling of those with sleep difficulties. Despite the probable oversampling of higher-functioning ALF residents and those with sleep problems, sleep measures were still associated with declining quality of life and greater depression over time, suggesting that poor sleep may be an important area for intervention in ALF residents. In addition, because polysomnographic recordings were not conducted and only self-reported measures of sleep apnea symptoms were available, the prevelance of this disorder has probably been underestimated. Future research should rely on objective measurements of sleep apnea, because the present study’s findings suggest that this may be a significant problem in ALF residents.
In conclusion, subjective and objective evidence was found that sleep disturbance was common in older people residing in ALFs. Sleep disturbance was associated with impairments in functional status and other measures of quality of life in this setting. Perhaps even more importantly, evidence was found that subjective and objective measures of sleep disturbance at baseline were associated with functional status (ADLs) and depressive symptoms at 3- and 6-month follow-up. These findings suggest that interventions targeting improvement in sleep disturbance in older people residing in ALFs may lead to maintenance of functional status and improvements in depressive symptoms over time. Although not tested in the current study, these improvements in sleep may affect other important consequences of decline in functional status, such as greater need for personal care assistance and eventual nursing home placement. Future studies should develop interventions that can be implemented within the ALF setting, with the goal of improving sleep, quality of life, functional outcomes, and depression in these older adults.
ACKNOWLEDGMENTS
The authors thank the participating facilities, the residents who took part in the study, and the research staff who made this study possible. In particular, we wish to thank Terry Vandenberg, MA, and Rebecca Saia, who served as project coordinators for this study.
Funding for this project was provided to Dr. Alessi from Sepracor Inc., Marlborough, Massachusetts. This study was supported by National Institutes of Health (NIH), National Institute on Aging Grant K23 AG028452 and National Institute of Mental Health Grant T32 MH 019925-11; the University of California at Los Angeles (UCLA) Academic Senate Council on Research; the Veterans Affairs (VA) Greater Los Angeles Healthcare System, Geriatric Research, Education and Clinical Center; VA Health Services Research and Development (IIR 04-321-2); and the UCLA Cousins Center for Psychoneuroimmunology.
Sponsor’s Role: The study sponsors had no input into the design, implementation, analysis, or interpretation of this study.
Footnotes
Author Contributions: Dr. Martin: study design, analysis and interpretation of data, and preparation of the manuscript. Dr. Fiorentino, Ms. Jouldjian, and Ms. Josephson: analysis and interpretation of data and preparation of the manuscript. Dr. Alessi: study concept and design, analysis and interpretation of data, and preparation of the manuscript.
Portions of this paper were presented at the Associated Professional Sleep Societies’ Annual Meeting, June 2009, Seattle, Washington.
Conflicts of Interest: The authors have no other potential conflicts of interest to disclose.
REFERENCES
- 1.Newcomer R, Maynard R. [Accessed September 14, 2007];Residential care for the elderly: Supply, demand and quality assurance. 2002 [on-line]. Available at http://www.canhr.org/reports/2002/rcfefullreport0102.pdf.
- 2.Hawes C, Phillps CD, Rose M. High Service or High Privacy Assisted Living Facilities, their Residents and Staff: Results from a National Survey. U.S. Department of Health and Human Services; Rockville, MD: 2000. [Google Scholar]
- 3.Golant SM. Do impaired older persons with health care needs occupy U.S. assisted living facilities? An analysis of six national studies. J Gerontol B Psychol Sci Soc Sci. 2004;59B:S68–S79. doi: 10.1093/geronb/59.2.s68. [DOI] [PubMed] [Google Scholar]
- 4.Phillips CD, Munoz Y, Sherman M, et al. Effects of facility characteristics on departures from assisted living: Results from a national survey. Gerontologist. 2003;43:690–696. doi: 10.1093/geront/43.5.690. [DOI] [PubMed] [Google Scholar]
- 5.Frytak JR, Kane RA, Finch MD, et al. Outcome trajectories for assisted living and nursing facility residents in Oregon. Health Services Res. 2001;36(1 Pt 1):91–111. [PMC free article] [PubMed] [Google Scholar]
- 6.Aud MA, Rantz MJ. Admissions to skilled nursing facilities from assisted living facilities. J Nurs Care Qual. 2005;20:16–25. doi: 10.1097/00001786-200501000-00005. [DOI] [PubMed] [Google Scholar]
- 7.Barbar SI, Enright PL, Boyle P, et al. Sleep disturbances and their correlates in elderly Japanese American men residing in Hawaii. J Gerontol A Biol Sci Med Sci. 2000;55A:M406–M411. doi: 10.1093/gerona/55.7.m406. [DOI] [PubMed] [Google Scholar]
- 8.Dew MA, Hoch CC, Buysse DJ, et al. Healthy older adults’ sleep predicts allcause mortality at 4 to 19 years of follow-up. Psychosom Med. 2003;65:63–73. doi: 10.1097/01.psy.0000039756.23250.7c. [DOI] [PubMed] [Google Scholar]
- 9.Ohayon MM, Vecchierini MF. Normative sleep data, cognitive function and daily living activities in older adults in the community. Sleep. 2005;28:981–989. [PubMed] [Google Scholar]
- 10.Goldman SE, Stone KL, Ancoli-Israel S, et al. Poor sleep is associated with poorer physical performance and greater functional limitations in older women. Sleep. 2007;30:1317–1324. doi: 10.1093/sleep/30.10.1317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dam TT, Ewing S, Ancoli-Israel S, et al. Association between sleep and physical function in older men: The Osteoporotic Fractures in Men Sleep Study. J Am Geriatr Soc. 2008;56:1665–1673. doi: 10.1111/j.1532-5415.2008.01846.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gooneratne NS, Weaver TE, Cater JR, et al. Functional outcomes of excessive daytime sleepiness in older adults. J Am Geriatr Soc. 2003;51:642–649. doi: 10.1034/j.1600-0579.2003.00208.x. [DOI] [PubMed] [Google Scholar]
- 13.Rao V, Spiro JR, Samus QM, et al. Sleep disturbances in the elderly residing in assisted living: Findings from the Maryland Assisted Living Study. Int J Ger Psych. 2005;20:956–966. doi: 10.1002/gps.1380. [DOI] [PubMed] [Google Scholar]
- 14.Martin JL, Alam T, Harker JO, et al. Sleep patterns in assisted living facilities: A comparison to home-dwelling elders. J Gerontol A Med Sci Soc Sci. 2008;163A:1407–1409. doi: 10.1093/gerona/63.12.1407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bliwise DL, King AC, Harris RB. Habitual sleep durations and health in a 50–65 year old population. J Clin Epidemiol. 1994;47:35–41. doi: 10.1016/0895-4356(94)90031-0. [DOI] [PubMed] [Google Scholar]
- 16.Prinz PN, Vitiello MV, Raskind MA, et al. Geriatrics: Sleep disorders and aging. N Engl J Med. 1990;323:520–526. doi: 10.1056/NEJM199008233230805. [DOI] [PubMed] [Google Scholar]
- 17.Bliwise DL. Review: Sleep in normal aging and dementia. Sleep. 1993;16:40–81. doi: 10.1093/sleep/16.1.40. [DOI] [PubMed] [Google Scholar]
- 18.Schmitt FA, Phillips BA, Cook YR, et al. Self report of sleep symptoms in older adults: Correlates of daytime sleepiness and health. Sleep. 1996;19:59–64. [PubMed] [Google Scholar]
- 19.Gislason T, Reynisdottir H, Kristbjarnarson H, et al. Sleep habits and sleep disturbances among the elderlyFan epidemiological survey. J Intern Med. 1993;234:31. doi: 10.1111/j.1365-2796.1993.tb00701.x. [DOI] [PubMed] [Google Scholar]
- 20.Ancoli-Israel S, Cooke JR. Prevalence and comorbidity of insomnia and effect on functioning in elderly populations. J Am Geriatr Soc. 2005;53(Suppl.):S264–S271. doi: 10.1111/j.1532-5415.2005.53392.x. [DOI] [PubMed] [Google Scholar]
- 21.Unruh ML, Redline S, An MW, et al. Subjective and objective sleep quality and aging in the Sleep Heart Health Study. J Am Geriatr Soc. 2008;56:1218–1227. doi: 10.1111/j.1532-5415.2008.01755.x. [DOI] [PubMed] [Google Scholar]
- 22.Buysse DJ, Reynolds CFI, Monk TH, et al. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- 23.Cole JC, Motivala SJ, Buysse DJ, et al. Validation of a 3-factor scoring model for the Pittsburgh Sleep Quality Index in older adults. Sleep. 2006;29:112–116. doi: 10.1093/sleep/29.1.112. [DOI] [PubMed] [Google Scholar]
- 24.Schnelle JF, Ouslander JG, Simmons SF, et al. The nighttime environment, incontinence care, and sleep disruption in nursing homes. J Am Geriatr Soc. 1993;41:910–914. doi: 10.1111/j.1532-5415.1993.tb06754.x. [DOI] [PubMed] [Google Scholar]
- 25.Ersser S, Wiles A, Taylor H, et al. The sleep of older people in hospital and nursing homes. J Clin Nurs. 1999;8:360–368. doi: 10.1046/j.1365-2702.1999.00267.x. [DOI] [PubMed] [Google Scholar]
- 26.Netzer NC, Stoohs RA, Netzer CM, et al. Using the Berlin questionnaire to identify patients at risk for the sleep apnea syndrome. Ann Intern Med. 1999;131:485–491. doi: 10.7326/0003-4819-131-7-199910050-00002. [DOI] [PubMed] [Google Scholar]
- 27.Allen RP, Picchietti D, Hening WA, et al. Restless legs syndrome: Diagnostic criteria, special considerations and epidemiology. A report from the Restless Legs Syndrome Diagnosis and Epidemiology Workshop at the National Institutes of Health. Sleep Med. 2003;4:101–119. doi: 10.1016/s1389-9457(03)00010-8. [DOI] [PubMed] [Google Scholar]
- 28.Blackwell T, Redline S, Ancoli-Israel S, et al. Comparison of sleep parameters from actigraphy and polysomnography in older women: The SOF Study. Sleep. 2008;31:283–291. doi: 10.1093/sleep/31.2.283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Blackwell T, Ancoli-Israel S, Gehrman PR, et al. Actigraphy scoring reliability in the study of osteoporotic fractures. Sleep. 2005;28:1599–1605. doi: 10.1093/sleep/28.12.1599. [DOI] [PubMed] [Google Scholar]
- 30.Bliwise DL, Bevier WC, Bliwise NG, et al. Systemic 24-hour behavior observations of sleep and wakefulness in a skilled-care nursing facility. Psychol Aging. 1990;15:16–24. doi: 10.1037//0882-7974.5.1.16. [DOI] [PubMed] [Google Scholar]
- 31.Lawton MP, Brody EM. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179–186. [PubMed] [Google Scholar]
- 32.Ware JE, Kosinski M, Keller SD. A 12-item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34:220–233. doi: 10.1097/00005650-199603000-00003. [DOI] [PubMed] [Google Scholar]
- 33.Jenkinson C, Layte R, Jenkinson D, et al. A shorter form health survey: Can the SF-12 replicate results from the SF-36 in longitudinal studies? J Public Health Med. 1997;29:179–186. doi: 10.1093/oxfordjournals.pubmed.a024606. [DOI] [PubMed] [Google Scholar]
- 34.Hoyl MT, Alessi CA, Harker JO, et al. Development and testing of a five-item version of the geriatric depression scale. J Am Geriatr Soc. 1999;47:873–878. doi: 10.1111/j.1532-5415.1999.tb03848.x. [DOI] [PubMed] [Google Scholar]
- 35.Folstein MF, Folstein SE, McHugh PR. Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–198. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- 36.Katz JN, Chang LC, Sangha O, et al. Can comorbidity be measured by questionnaire rather than medical record review? Med Care. 1996;34:73–84. doi: 10.1097/00005650-199601000-00006. [DOI] [PubMed] [Google Scholar]
- 37.Chaudhry S, Jin L, Meltzer D. Use of a self-repot-generated Charlson comorbidity index for predicting mortality. Med Care. 2005;43:607–615. doi: 10.1097/01.mlr.0000163658.65008.ec. [DOI] [PubMed] [Google Scholar]
- 38.Feldman HI, Strom BL. Utilisation of drugs for diabetes mellitus. Drug Safety. 1991;6:220–229. doi: 10.2165/00002018-199106030-00006. [DOI] [PubMed] [Google Scholar]
- 39.Whitty PM, Eccles MP, Steen IN, et al. Number of non-diabetic drugs: A simple comorbidity indicator for diabetes? Pharm World Sci. 2001;23:145–147. doi: 10.1023/a:1011895532488. [DOI] [PubMed] [Google Scholar]
- 40.Blazer D, Hybels C, Simonsick E, et al. Sedative, hypnotic, and antianxiety medication use in an aging cohort over ten years: A racial comparison. J Am Geriatr Soc. 2000;48:1073–1079. doi: 10.1111/j.1532-5415.2000.tb04782.x. [DOI] [PubMed] [Google Scholar]
- 41.Giron MS, Forsell Y, Bernsten C, et al. Sleep problems in a very old population: Drug use and clinical correlates. J Gerontol A Biol Sci Med Sci. 2002;57A:M236–M240. doi: 10.1093/gerona/57.4.m236. [DOI] [PubMed] [Google Scholar]
- 42.Cumming RG, Couteur DG Le. Benzodiazepines and risk of hip fractures in older people: A review of the evidence. CNS Drugs. 2003;17:825–837. doi: 10.2165/00023210-200317110-00004. [DOI] [PubMed] [Google Scholar]
- 43.Pereira FS, Yassuda MS, Oliveira AM, et al. Executive dysfunction correlates with impaired functional status in older adults with varying degrees of cognitive impairment. Int Psychoger. 2008;20:1104–1115. doi: 10.1017/S1041610208007631. [DOI] [PubMed] [Google Scholar]
- 44.Pigeon WR, Hegel M, Unutzer J, et al. Is insomnia a perpetuating factor for late-life depression in the IMPACT cohort? Sleep. 2008;31:481–488. doi: 10.1093/sleep/31.4.481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Givens JL, Santf TB, Marcantonio ER. Functional recovery after hip fracture: The combined effects of depressive symptoms, cognitive impairment, and delirium. J Am Geriatr Soc. 2008;56:1075–1079. doi: 10.1111/j.1532-5415.2008.01711.x. [DOI] [PubMed] [Google Scholar]
- 46.Whitson HE, Sanders L, Pieper CF, et al. Depressive symptomatology and fracture risk in community-dwelling older men and women. Aging. 2008;20:585–592. doi: 10.1007/bf03324888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Watson LC, Garrett JM, Sloane PD, et al. Depression in assisted living: Results from a four-state study. Am J Psychiatry. 2003;11:534–542. [PubMed] [Google Scholar]