

Abstract
Pleural infection is a common and increasing clinical problem in thoracic medicine, resulting in significant morbidity and mortality. In recent years there has been a marked increase in interests and publications relating to evolving interventions and management options for pleural infection and empyema. Recently published research data as well as guidelines have suggested better approaches of radiological assessment, updated management algorithms for pleural infection, intrapleural adjunct therapies and re-examined the roles of biomarkers, pleural drainage techniques, and the role of surgery. This review highlights some of the recent advances and recommendations relevant to clinical care of pleural infection.
Key words : Pleural effusion, empyema, infection, disease management
Introduction
Pleural infection (either complicated parapneumonic effusion or empyema) is an ancient problem, with the first recorded descriptions to be found in the medical texts of ancient Greece. Approximately four million people are affected by pneumonia each year, with close to half estimated to develop a parapneumonic effusion. Pleural infection is a common complication of pneumonia, reported to affect 65,000 patients per year in the USA and UK alone (1,2) at an estimated total healthcare cost approximating USD $320 million (3). Pleural infection significantly increase the morbidity and mortality associated with pulmonary infections, with a mortality rate in adults approaching 20% (4,5). This review summarizes recent advances in management of pleural infection including recommendations from the latest clinical guidelines. A detailed overview is outside the scope of this review and can be found elsewhere (6).
Rising burden of pleural infection
Regions (where pleural infection is likely to be substantially more common) are lacking. The incidence of pleural infection appears to be increasing globally, across all age ranges (7). On a recent review of national hospitalisation data in the USA by Grijalva et al., a 2 fold increase (3.04 per 100,000 in 1996 to 5.98 in 2008) in hospitalisations was reported. Overall in-hospital mortality rate was 8%, reaching 16.1% in adults ≥65 years (8). In this study pneumococcal empyema rates were stable from 1996 to 2008, but pleural infection from streptococci (non-pneumococcal) and staphylococci were rising. Staphylococcal-related empyema was associated with longer hospital stays and higher in-hospital mortality. These findings are a reflection of similar studies in the last five years noting a global increase in rates of pleural infection (9,10).
A different picture of the incidence of pneumococcal empyema has been reported by Burgos et al., suggesting an increased incidence in young adults in the post pneumococcal vaccine period (11). In an observational study of all adults hospitalized with invasive pneumococcal disease presenting with empyema, the rates of empyema in patients aged 18-50 years increased from 7.6% to 14.9%, i.e. an increase from 0.5 to 1.6 cases per 100,000 patient-years, since the introduction of pneumococcal conjugate vaccine (PCV7) in Spain in 2001. These infections appeared predominantly due to an increase of cases involving serotype 1 (43.3% of cases), a serotype not covered by PCV7. These findings highlight the changing epidemiology of pneumococcal empyema in adults, and the need for awareness by the clinician of local as well as global trends in pleural infection.
Pleural infection is more common in the paediatric and elderly populations (9,10). Reports on epidemiology of pleural infection come mainly from developed countries; data from developing.
Pathophysiology
Bacteriology
Streptococcus pneumoniae, S. pyogenes and Staphylococcus aureus are the organisms traditionally associated with pleural infection (11). Additionally the S. anginosus group (often known as S. milleri group) consisting of S. anginosus, S. constellatus and S. intermedius are part of normal human flora which become significant in the context of pleural infection, accounting for 30-50% of adult cases of community acquired empyema (11-14).
S. aureus is more commonly seen in the older, hospitalised patient with co-morbidities. It is associated with cavitation and abscess formation, with empyema present in 1-25% of adult cases. Increasing numbers of cases of empyema caused by community acquired MRSA are being reported, and such a pathogen should be considered in the appropriate setting of both community and hospital acquired empyema (15). Anaerobic bacteria however contribute significantly to pleural infection, being identified as the sole or co-pathogen in 25-76% of pediatric cases (16).
The importance of differentiating community acquired empyema from hospital acquired cases is being increasingly recognized, as the latter often has a different bacteriology. Organisms such as MRSA, Enterobacteriae and anaerobes are more prevalent in nosocomial empyema and will influence the choice of antibiotics (17). Awareness of local prevalence and antimicrobial sensitivities is essential to guide clinical decisions and antibiotic selection. Identification of the causative pathogen(s) in pleural infection can be difficult, with the microbiological diagnosis remaining elusive in 40% of cases in one study despite standard pleural fluid culture (18).
Diagnosis
Clinical presentation
A high index of suspicion is required for the diagnosis of pleural infection.
Patients may present with the finding of a pleural effusion on chest X-ray in the setting of pneumonia, with failure to clinically improve as expected. Patients may also present with fever, chest pain, cough, purulent sputum and dyspnoea. The absence of pleuritic pain does not exclude pleural infection (1).
When faced with patients with a parapneumonic effusion, no specific clinical features accurately predict the need for pleural drainage. Sampling of an effusion is often required to assess whether the pleural space is infected (19).
Imaging
Chest X-rays have long been the initial radiologic investigation for the assessment of pulmonary pathology including the presence of pleural space infections. The chest X-ray will usually show a small to moderate effusion with or without parenchymal infiltrates. The effusions may be bilateral, the larger usually on the side primarily affected by pneumonia. In the setting of complex effusions, loculations and air fluid levels may be apparent (19). Prior to the greater use of thoracic ultrasound and CT, lateral decubitus X-rays were used in the assessment of pleural collection, with Light demonstrating that effusions less than 1cm would resolve with antibiotic therapy alone and not require further intervention (1). Current guidelines recommend the sampling of parapneumonic effusions with a thickness ≥10 mm (20). However parapneumonic effusions are often loculated and assessment of thickness on chest X-ray is therefore problematic and is not a clinically reliable guide. A recent study of 61 patients with pneumonia and parapneumonic effusion showed that CXR, taken as anteroposterior, posteroanterior, or lateral, all missed more than 10% of parapneumonic effusions. Hence alternatives, such as ultrasound or CT, particularly in the setting of lower lobe consolidation (21) are now considered the mainstay imaging modalities for parapneumonic effusions.
Pleural ultrasound
The last decade has seen a significant trend worldwide to employ pleural ultrasound at the bedside to assess for the presence of pleural effusions, especially in the context of pleural infection. Pleural ultrasound is fast, safe and effective in confirming the presence of pleural fluid, and in localising the optimal site for diagnostic and therapeutic intervention in real time (22). Use of real-time pleural ultrasound by trained operators has been shown to improve the safety of sampling effusions, with reported reductions in iatrogenic pneumothoraces compared to un-guided thoracenteses (in two studies) from 10.3% and 18% to 4.9% and 3% respectively (23,24). Its role in risk reduction has been stressed in a recent meta-analysis and reviews of pleural procedures (25,26). It has been incorporated into diagnostic algorithms in major centres in recent years (27). It is sensitive in detecting small volumes of fluid and may detect loculations not evident on CT (19). Ultrasound of the pleural space is rapidly being considered as an extension of the physical examination and a core skill in those routinely assessing pleural effusions (Figure 1).
Figure 1.
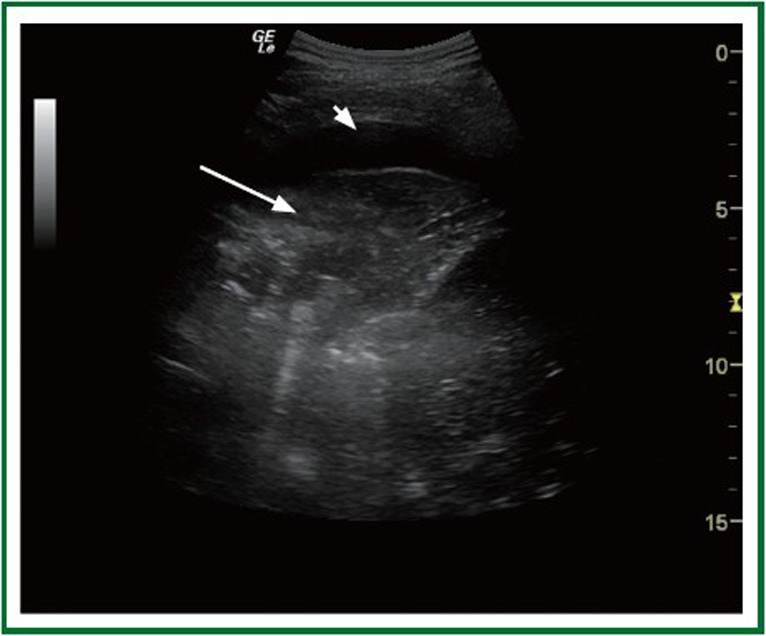
Ultrasound of a patient presenting with Right Middle Lobe pneumonia. Pleural ultrasound can differentiate the consolidated lung (in hepatization phase - white arrow) from adjacent small parapneumonic effusion (arrowhead).
CT
Pleural effusions are commonly detected on review of CTs organised for assessment of pneumonia. In terms of diagnosis and planning of intervention, contrast enhanced thoracic CT is the imaging investigation of choice, with correct timing of contrast injection allowing better definition of the pleural abnormalities as suggested by Raj et al. (28). Thoracic CT allows not only assessment of the pleura itself, but chest tube position, presence and degree of loculations, parenchymal changes, endobronchial lesions and differentiation of lung abscess from empyema (27,29).
MRI and PET
MRI is not routinely used for the assessment of the pleural space, though it has been shown to allow assessment of complex loculated effusions, and demonstrate chest wall involvement. Davies et al. also found that exudates produced higher signal than transudates on T1 and T2 weighted images, theoretically allowing differentiation of transudates and exudates (30). Use of MRI minimizes radiation from contrast media and is therefore theoretically superior to CT especially in young patients who require repeated imaging. PET cannot differentiate infection from malignancy in the setting of a pleural collection and has no clinical role in pleural infection.
Thoracentesis
Thoracentesis remains a key tool in the diagnosis and tailoring of management in pleural infection. Current guidelines advise sampling of effusions >10 mm in depth associated with pneumonia, chest trauma or thoracic surgery with features of sepsis (20). This has been questioned by Skouras et al. in a retrospective review of patients with pneumonia diagnosed with a pleural effusion on CT, with a low complication rate in patients with a pleural fluid thickness of <20 mm. These results however are preliminary and retrospective, in a small subset of patients with pneumonia, and further prospective trials are required before altering the above recommendation.
Image guidance has been shown to decrease the risk of complication including organ perforation in pleural fluid sampling. Pleural ultrasound improves accuracy of sample site selection. Simple marking of a site for pleural sampling away from the location of the actual procedure is no better than 'blind' aspiration. Patient movement in transit and lack of replication of body position from imaging to time of procedure mean that there may be significant disparity between surface site marked and the actual fluid collection. The ability of the clinician to use pleural ultrasound themselves allows visualisation of pleural anatomy and identification of barriers to thoracentesis such as ribs, vasculature or consolidated lung (26,31-34). The role of pleural ultrasound, together with simulation and supervision, has been reviewed elsewhere (35).
Pleural fluid biomarkers of infection
Pleural fluid pH should be assessed if pleural infection is suspected, except in the case of frank pus where chest tube drainage is indicated (20). A blood gas analyser should be used, as litmus paper is unreliable in the assessment of pleural pH (36,37). The method of sample collection is important, as confounders such as local anaesthetic or air in the chamber of the sampling syringe, or prolonged time between sample collection and processing, has been shown to artificially alter sample pH (38). These recommendations have been incorporated into recent guidelines (20). Clinicians should be aware that pleural fluid pH can occasionally vary among different locules (39). Fluid protein, glucose and lactate dehydrogenase (LDH) can also aid characterisation of pleural fluid and determine management, and together with microbiological culture, should be requested on initial samples. While protein concentration can contribute to confirming an effusion as an exudate, it does not have value in determining the need for tube drainage of an effusion versus less invasive management (40). Cytology and assessment for acid fast bacilli should be performed as clinically indicated. A predominance of polymorphonuclear cells is expected in pleural infection. Alternative etiologies should be entertained if the effusion is not neutrophil-dominant (41).
Newer biomarkers have been assessed to examine their efficacy in diagnosing pleural effusions secondary to infection, and to prognosticate on the likelihood of these effusions becoming complicated. Porcel et al. has recently examined a range of pleural fluid biomarkers in pleural infection, including tumor necrosis factor-alpha, myeloperoxidase, C-reactive protein and procalcitonin (42). None of these markers is superior to the classically accepted markers of pleural fluid pH <7.20, or pleural fluid glucose <60 mg/dL (43).
A promising advance in microbiological diagnosis was recently reported by Menzies et al. utilising a readily available bacterial culture system (the BACTEC blood culture bottle system) (44). In this prospective trial blood culture bottles were inoculated with pleural fluid in addition to standard pleural fluid culture, with an absolute increase in microbiological diagnostic yield by 21%, and a proportional increase close to 50%. In 4% of cases even where standard culture was positive, the results of culture of pleural fluid transported in blood culture bottles yielded additional organisms that led to an alteration in management.
Management
Multiple approaches exist for treating parapneumonic effusions and pleural infection, ranging from antibiotics alone to radical surgical intervention. The optimal management is determined by the answers to several core questions-should the pleural space be drained, how it should be drained, and should intrapleural adjunct therapy be used (19). The initial imaging and results of the pleural fluid sampling including the smell, appearance and pH provide the earliest information determining the need for formal chest tube insertion and drainage. Frank pus, regardless of other determinants, warrants immediate evacuation of any pleural collection. Further features include positive gram stain, positive culture and pleural fluid pH <7.20 [or glucose <3.4 mmol/L (60 mg/dL)] (20).
Observation
The American College of Chest Physicians guidelines outline four categories of pleural fluid collection in the setting of infection (44). These range from <1 cm effusions through to empyema, as determined by radiological features, pH, gram stain, culture and presence of pus. Only category 1 effusions (very low risk), described as minimal and free flowing and <1 cm, are considered safe for observation without diagnostic sampling. Category 2 (low risk) effusions (≥10 mm but <1/2 hemithorax, pH >7.2 and negative gram stain and culture) may be observed without formal drainage. Category 3 (moderate risk) effusions (large but free flowing effusions, loculated effusions, or effusions with thickened parietal pleura; or pH <7.2; or positive gram stain or culture) and 4 (empyema) should be drained urgently due to the associated risk of poor outcome. It is important to note that these recommendations can serve as a useful guide, but are based mainly on expert opinion and supported by limited quality data.
Antibiotics
All patients with suspected pleural infection should receive appropriate antibiotic cover from the time of first review. Initial antibiotic choice should be determined by local prescribing guidelines and resistance patterns, and where possible refined by available microbiological samples and culture. In cases of community acquired pleural infection with confirmed bacteriology, 50% of cases are reported to be due to penicillin-sensitive streptococci, with the remainder due to organisms that are penicillin resistant, such as staphylococci and Enterobacteriaceae. Roughly 25% of community acquired pleural infections include anaerobic bacteria. Approximately 40% of cases will be culture negative (13). As such empiric antibiotic choice should cover common community-acquired bacterial pathogens and anaerobic bacteria (45). Penicillins, penicillins with beta-lactamase inhibitors, cephalosporins, and fluoroquinolones all have good penetration of the pleural space (44-50). Metronidazole and clindamycin also penetrate well and cover anaerobic bacteria. Aminoglycosides have poor penetration, and may be less effective in the acidic environment of the pleural space during infection (51). The low prevalence of legionella and mycoplasma as causative agents of significant pleural infections means that specific antibiotic cover is not routinely indicated (17,45). In the setting of hospital-acquired pleural infection antibiotic selection should also cover MRSA and anaerobic bacteria (17). More extensive review of antibiotic choice for pleural infection is available elsewhere (17,45).
Duration of antibiotic therapy is based on a combination of clinical response, bacteriology where available and inflammatory marker (e.g., CRP, procalcitonin) response. Radiological changes can persist after clinical improvement and should not be the sole criteria for continuation of therapy, nor would that be an indication of treatment failure. The exact timing of change from intravenous to oral antibiotic therapy is not rigorously defined, with expert opinion suggesting at least 1 week of intravenous therapy followed by 1-2 weeks of oral therapy as appropriate based on clinical response (6).
Thoracentesis
The risk of complications in pleural infections is decreased by minimising the number of interventions. Initial thoracentesis should be therapeutic as well as diagnostic if possible (52). The reasoning behind this is that if fluid is drained and does not recur and it may not require further invasive treatment. Alternatives include insertion of a small bore catheter or a therapeutic thoracentesis. These three approaches have not been directly compared in prospective studies. Further management will depend on initial fluid findings and clinical progress.
Chest tube drainage
A large volume of recent literature has emphasized the need to be aware of complications of pleural procedures (25,26,35,45). Guidelines exist for insertion of chest tubes, as do safety protocols and web based simulations (53). Whenever possible, imaging guidance should be used, and adequate supervision is paramount (54).
Historically large bore tubes (>20 Fr) have been used for drainage of pleural infection with minimal evidence based support of superiority. Recent evidence from a large prospective series indicates that small bore chest tubes (≤14 Fr) are as effective, and better tolerated due to less pain (55). Failure of successful drainage with a small bore tube often results from loculations. Rather than insertion of a larger tube, consideration should be given to repeated imaging of the pleural space and insertion of additional small bore tubes to remaining sizeable locules.
Intrapleural therapy
Multiple observational studies and small randomised trials have examined the role of administration of intrapleural fibrinolytics in improving drainage of loculated pleural effusions. These studies were promising, though most were uncontrolled or had significant limitations. A large randomised control study, assessing 454 patients, examined the efficacy of streptokinase compared to saline. This study did not show a difference in length of hospitalisation or need for surgery between the groups, and sub-group analyses did not show any benefits from the intrapleural streptokinase (13). A meta-analysis in 2008 reviewing all available randomised controlled data, totalling seven studies and 761 patients, found no mortality benefit with intrapleural fibrinolytics alone (55).
The recent result from the Multicenter Intrapleural Sepsis Trial-2 was noteworthy. In this double-blind, multicenter trial, 210 patients with pleural infection were randomized to one of the four arms: intrapleural tissue plasminogen activator (tPA) alone, intrapleural DNase alone, placebo or intrapleural tPA and DNase. The primary end-point was radiographic improvement as measured by the percentage of the hemithorax occupied by pleural fluid on chest X-ray. The combination of tPA and DNase (but not the individual agents alone) resulted in improved radiological appearance (mean decrease in pleural opacity 7.9% over that from placebo), decreased surgical referral at three months [2/48 patients (4%) vs. 8/51 patients (16%)], and reduction in hospital stay of 6.7 days compared to placebo, without excessive adverse events (56). This therapy is increasingly employed by centers worldwide. Future studies need to define if the therapy is best to be administered to every pleural infection patients or be reserved for those who have failed standard medical management (Figure 2).
Figure 2.

A: This patient presented with a pneumococcal pneumonia which was complicated by pleural infection. A small bore tube was inserted but drainage was limited by extensive septations within the effusion. The patient remained febrile with elevated inflammatory markers; B: Intrapleural tPA and DNase was administered twice daily for three days with dramatic clearance of the loculated effusion. Her fever and inflammatory markers settled and was discharged on antibiotics; C: CXR at 3 months after discharge, with marked improvement of pleural opacities.
Surgery
Surgery remains an option when medical therapy is inadequate. Current guidelines suggest surgery should only be recommended in patients with a residual pleural collection and persistent sepsis despite adequate antibiotic therapy and drainage (45). While empyema has previously been regarded as a 'surgical' disease, the role for surgical intervention may be declining (57). Previous studies have been flawed by selection bias, with surgical patients with empyema being younger by almost 10 years and having less co-morbidity (9). In considering the role for surgery, it needs to be remembered that the majority of patients with pleural infection can be managed with antibiotics and chest tube drainage. Only 18% of patients in the MIST1 trial (14) failed this approach and only 11% in MIST2 (3). Using tPA and DNase, 96% of patients were successfully treated without surgery.
Two randomized clinical trials in adults comparing first line video-assisted thoracoscopic surgery (VATS) with medical treatment (chest tube drainage with/without fibrinolytics and antibiotics) have not shown a survival advantage from early surgical intervention (58,59). These trials did suggest a modest reduction in length of hospital stay (8.7 vs. 12.8 and 8.3 vs. 12.8 respectively). Both trials were small (n=19 and 70 respectively), and lacked a clear clinical criteria for surgery and decortication. As a result the Cochrane review examining this topic indicated further research to establish best practice (60). Currently no trials have compared VATS against the combination of tPA and DNAse in the treatment of pleural infection. The intermediate term complications of surgery must also be taken into consideration. Intercostal neuralgia is not uncommon, with Furrer et al. (61) reporting 44% of patients had pain at 6 months post thoracotomy, and Dajczman (62) reporting a series of patients (n=56) of which 9% required nerve blocks, daily analgesia and/or ongoing pain clinic review.
Conclusion
Pleural infections are increasing worldwide despite modern day medical care and antimicrobial therapies. A high index of suspicion for and early identification of pleural space infection is required for good clinical outcomes. Chest X-ray is the mainstay of identification of pleural effusions in the setting of infection, but pleural ultrasound plays a critical role in the assessment of and guidance of drainage in pleural infection. Emerging biomarkers together with currently available markers of inflammation may aid recognition of effusions associated with infection. However, the well established criteria utilising pleural fluid pH, LDH and glucose remain a cornerstone in the decision making process regarding drainage of the pleural space. Appropriate antibiotic therapy remains a key initial therapeutic intervention. The optimal size of chest tube for drainage of the pleural space remains controversial, and small-bore tubes should be considered as first line. In patients where standard medical therapy has failed the use of combination intrapleural tPA and DNase should be considered. The exact role of surgery remains controversial, especially in face of new and highly effective intrapleural therapies.
Footnotes
No potential conflict of interest.
References
- 1.Light RW, Girard WM, Jenkinson SG, George RB. Parapneumonic effusions. Am J Med. 1980;69:507-512 [DOI] [PubMed] [Google Scholar]
- 2.Brims FJ, Lansley SM, Waterer GW, Lee YC. Empyema thoracis: new insights into an old disease. Eur Respir Rev. 2010;19:220-228 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rahman NM, Maskell NA, West A, et al. Intrapleural use of tissue plasminogen activator and DNase in pleural infection. N Engl J Med. 2011;365:518-526 [DOI] [PubMed] [Google Scholar]
- 4.Ferguson AD, Prescott RJ, Selkon JB, Watson D, Swinburn CR. The clinical course and management of thoracic empyema. QJM. 1996;89:285-289 [DOI] [PubMed] [Google Scholar]
- 5.Davies CW, Kearney SE, Gleeson FV, Davies RJ. Predictors of outcome and long-term survival in patients with pleural infection. Am J Respir Crit Care Med. 1999;160:1682-1687 [DOI] [PubMed] [Google Scholar]
- 6.Rahman NM, Davies RJO. Effusions from infections: parapneumonic effusion and empyema. In: Light RW, Lee YCG (eds), Textbook of Pleural Diseases. 2nd ed. Hodder Arnold 2008:341–66. [Google Scholar]
- 7.Lisboa T, Waterer GW, Lee YC. Pleural infection: changing bacteriology and its implications. Respirology. 2011;16:598-603 [DOI] [PubMed] [Google Scholar]
- 8.Grijalva CG, Zhu Y, Nuorti JP, Griffin MR. Emergence of parapneumonic empyema in the USA. Thorax. 2011;66:663-668 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Finley C, Clifton J, Fitzgerald JM, Yee J. Empyema: an increasing concern in Canada. Can Respir J. 2008;15:85-89 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Farjah F, Symons RG, Krishnadasan B, Wood DE, Flum DR. Management of pleural space infections: a population-based analysis. J Thorac Cardiovasc Surg. 2007;133:346-351 [DOI] [PubMed] [Google Scholar]
- 11.Burgos J, Lujan M, Falcó V, et al. The spectrum of pneumococcal empyema in adults in the early 21st century. Clin Infect Dis. 2011;53:254-261 [DOI] [PubMed] [Google Scholar]
- 12.Septimus E. Pleural effusion and empyema. In: Mandell GL, Bennett JE RD (eds) Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. Churchill Livingstone 2009:917-24. [Google Scholar]
- 13.Ahmed RA, Marrie TJ, Huang JQ. Thoracic empyema in patients with community-acquired pneumonia. Am J Med. 2006;119:877-883 [DOI] [PubMed] [Google Scholar]
- 14.Maskell NA, Davies CW, Nunn AJ, et al. U.K. Controlled trial of intrapleural streptokinase for pleural infection. N Engl J Med. 2005;352:865-874 [DOI] [PubMed] [Google Scholar]
- 15.Lindstrom ST, Kolbe J. Community acquired parapneumonic thoracic empyema: predictors of outcome. Respirology. 1999;4:173-179 [DOI] [PubMed] [Google Scholar]
- 16.Micek ST, Dunne M, Kollef MH. Pleuropulmonary complications of Panton-Valentine leukocidin-positive community-acquired methicillin-resistant Staphylococcus aureus: importance of treatment with antimicrobials inhibiting exotoxin production. Chest. 2005;128:2732-2738 [DOI] [PubMed] [Google Scholar]
- 17.Schultz KD, Fan LL, Pinsky J, et al. The changing face of pleural empyemas in children: epidemiology and management. Pediatrics. 2004;113:1735-1740 [DOI] [PubMed] [Google Scholar]
- 18.Maskell NA, Batt S, Hedley EL, Davies CW, Gillespie SH, Davies RJ. The bacteriology of pleural infection by genetic and standard methods and its mortality significance. Am J Respir Crit Care Med. 2006;174:817-823 [DOI] [PubMed] [Google Scholar]
- 19.Rahman NM, Gleeson FV. New directions in the treatment of infected pleural effusion. Clin Radiol. 2006;61:719-722 [DOI] [PubMed] [Google Scholar]
- 20.Davies HE, Davies RJ, Davies CW, BTS Pleural Disease Guideline Group Management of pleural infection in adults: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010;65:ii41-ii53 [DOI] [PubMed] [Google Scholar]
- 21.Koenig SJ, Narasimhan M, Mayo PH. Thoracic ultrasonography for the pulmonary specialist. Chest. 2011;140:1332-1341 [DOI] [PubMed] [Google Scholar]
- 22.Barnes TW, Morgenthaler TI, Olson EJ, Hesley GK, Decker PA, Ryu JH. Sonographically guided thoracentesis and rate of pneumothorax. J Clin Ultrasound. 2005;33:442-446 [DOI] [PubMed] [Google Scholar]
- 23.Raptopoulos V, Davis LM, Lee G, Umali C, Lew R, Irwin RS. Factors affecting the development of pneumothorax associated with thoracentesis. AJR Am J Roentgenol. 1991;156:917-920 [DOI] [PubMed] [Google Scholar]
- 24.Gordon CE, Feller-Kopman D, Balk EM, Smetana GW. Pneumothorax following thoracentesis: a systematic review and meta-analysis. Arch Intern Med. 2010;170:332-339 [DOI] [PubMed] [Google Scholar]
- 25.Daniels CE, Ryu JH. Improving the safety of thoracentesis. Curr Opin Pulm Med. 2011;17:232-236 [DOI] [PubMed] [Google Scholar]
- 26.Duncan DR, Morgenthaler TI, Ryu JH, Daniels CE. Reducing iatrogenic risk in thoracentesis: establishing best practice via experiential training in a zero-risk environment. Chest. 2009;135:1315-1320 [DOI] [PubMed] [Google Scholar]
- 27.Kearney SE, Davies CW, Davies RJ, Gleeson FV. Computed tomography and ultrasound in parapneumonic effusions and empyema. Clin Radiol. 2000;55:542-547 [DOI] [PubMed] [Google Scholar]
- 28.Raj V, Kirke R, Bankart MJ, Entwisle JJ. Multidetector CT imaging of pleura: comparison of two contrast infusion protocols. Br J Radiol. 2011;84:796-799 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Stark DD, Federle MP, Goodman PC, Podrasky AE, Webb WR. Differentiating lung abscess and empyema: radiography and computed tomography. AJR Am J Roentgenol. 1983;141:163-167 [DOI] [PubMed] [Google Scholar]
- 30.Davis SD, Henschke CI, Yankelevitz DF, Cahill PT, Yi Y. MR imaging of pleural effusions. J Comput Assist Tomogr. 1990;14:192-198 [DOI] [PubMed] [Google Scholar]
- 31.Skouras V, Awdankiewicz A, Light RW. What size parapneumonic effusions should be sampled? Thorax. 2010;65:91. [DOI] [PubMed] [Google Scholar]
- 32.Diacon AH, Brutsche MH, Solèr M. Accuracy of pleural puncture sites: a prospective comparison of clinical examination with ultrasound. Chest. 2003;123:436-441 [DOI] [PubMed] [Google Scholar]
- 33.Jones PW, Moyers JP, Rogers JT, Rodriguez RM, Lee YC, Light RW. Ultrasound-guided thoracentesis: is it a safer method? Chest. 2003;123:418-423 [DOI] [PubMed] [Google Scholar]
- 34.Mayo PH, Goltz HR, Tafreshi M, Doelken P. Safety of ultrasound-guided thoracentesis in patients receiving mechanical ventilation. Chest. 2004;125:1059-1062 [DOI] [PubMed] [Google Scholar]
- 35.Wrightson JM, Fysh E, Maskell NA, Lee YC. Risk reduction in pleural procedures: sonography, simulation and supervision. Curr Opin Pulm Med. 2010;16:340-350 [DOI] [PubMed] [Google Scholar]
- 36.Cheng DS, Rodriguez RM, Rogers J, Wagster M, Starnes DL, Light RW. Comparison of pleural fluid pH values obtained using blood gas machine, pH meter, and pH indicator strip. Chest. 1998;114:1368-1372 [DOI] [PubMed] [Google Scholar]
- 37.Lesho EP, Roth BJ. Is pH paper an acceptable, low-cost alternative to the blood gas analyzer for determining pleural fluid pH? Chest. 1997;112:1291-1292 [DOI] [PubMed] [Google Scholar]
- 38.Rahman NM, Mishra EK, Davies HE, Davies RJ, Lee YC. Clinically important factors influencing the diagnostic measurement of pleural fluid pH and glucose. Am J Respir Crit Care Med. 2008;178:483-490 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Maskell NA, Gleeson FV, Darby M, Davies RJ. Diagnostically significant variations in pleural fluid pH in loculated parapneumonic effusions. Chest. 2004;126:2022-2024 [DOI] [PubMed] [Google Scholar]
- 40.Poe RH, Marin MG, Israel RH, Kallay MC. Utility of pleural fluid analysis in predicting tube thoracostomy/decortication in parapneumonic effusions. Chest. 1991;100:963-967 [DOI] [PubMed] [Google Scholar]
- 41.Light RW, Erozan YS, Ball WC., Jr Cells in pleural fluid. Their value in differential diagnosis. Arch Intern Med. 1973;132:854-860 [PubMed] [Google Scholar]
- 42.Porcel JM. Pleural fluid tests to identify complicated parapneumonic effusions. Curr Opin Pulm Med. 2010;16:357-361 [DOI] [PubMed] [Google Scholar]
- 43.Porcel JM, Vives M, Cao G, et al. Biomarkers of infection for the differential diagnosis of pleural effusions. Eur Respir J. 2009;34:1383-1389 [DOI] [PubMed] [Google Scholar]
- 44.Menzies SM, Rahman NM, Wrightson JM, et al. Blood culture bottle culture of pleural fluid in pleural infection. Thorax. 2011;66:658-662 [DOI] [PubMed] [Google Scholar]
- 45.Brixey AG, Luo Y, Skouras V, Awdankiewicz A, Light RW. The efficacy of chest radiographs in detecting parapneumonic effusions. Respirology. 2011;16:1000-1004 [DOI] [PubMed] [Google Scholar]
- 46.Colice GL, Curtis A, Deslauriers J, et al. Medical and surgical treatment of parapneumonic effusions: an evidence-based guideline. Chest. 2000;118:1158-1171 [DOI] [PubMed] [Google Scholar]
- 47.Nathwani D, Wood MJ. Penicillins. A current review of their clinical pharmacology and therapeutic use. Drugs. 1993;45:866-894 [DOI] [PubMed] [Google Scholar]
- 48.Scaglione F, Raichi M, Fraschini F. Serum protein binding and extravascular diffusion of methoxyimino cephalosporins. Time courses of free and total concentrations of cefotaxime and ceftriaxone in serum and pleural exudate. J Antimicrob Chemother. 1990;26:1-10 [DOI] [PubMed] [Google Scholar]
- 49.Taryle DA, Good JT, Jr, Morgan EJ, III, Reller LB, Sahn SA. Antibiotic concentrations in human parapneumonic effusions. J Antimicrob Chemother. 1981;7:171-177 [DOI] [PubMed] [Google Scholar]
- 50.Teixeira LR, Villarino MA. Antibiotic treatment of patients with pneumonia and pleural effusion. Curr Opin Pulm Med. 1998;4:230-234 [DOI] [PubMed] [Google Scholar]
- 51.Shohet I, Yellin A, Meyerovitch J, Rubinstein E. Pharmacokinetics and therapeutic efficacy of gentamicin in an experimental pleural empyema rabbit model. Antimicrob Agents Chemother. 1987;31:982-985 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Light RW. Pleural diseases. 5th edition. Baltimore (MD): Lippincott Williams & Wilkins; 2007. [Google Scholar]
- 53.British Thoracic Society. Guidance for the local implementation of local trust policies for the safe insertion of chest drains for pleural effusions in adults, following the NPSA Rapid Response Report. Available online: http://www.brit-thoracic.org.uk/Portals/0/Clinical%20Information/Pleural%20Disease/chestdrain-adults.pdf
- 54.Hooper CE, Lee YC, Maskell NA. Setting up a specialist pleural disease service. Respirology. 2010;15:1028-1036 [DOI] [PubMed] [Google Scholar]
- 55.Rahman NM, Maskell NA, Davies CW, et al. The relationship between chest tube size and clinical outcome in pleural infection. Chest. 2010;137:536-543 [DOI] [PubMed] [Google Scholar]
- 56.Cameron R, Davies HR. Intra-pleural fibrinolytic therapy versus conservative management in the treatment of adult parapneumonic effusions and empyema. Cochrane Database Syst Rev. 2008;2:CD002312. [DOI] [PubMed] [Google Scholar]
- 57.Davies HE, Rosenstengel A, Lee YC. The diminishing role of surgery in pleural disease. Curr Opin Pulm Med. 2011;17:247-254 [DOI] [PubMed] [Google Scholar]
- 58.Bilgin M, Akcali Y, Oguzkaya F. Benefits of early aggressive management of empyema thoracis. ANZ J Surg. 2006;76:120-122 [DOI] [PubMed] [Google Scholar]
- 59.Wait MA, Sharma S, Hohn J, Dal Nogare A. A randomized trial of empyema therapy. Chest. 1997;111:1548-1551 [DOI] [PubMed] [Google Scholar]
- 60.Cameron R, Davies HR. Intra-pleural fibrinolytic therapy versus conservative management in the treatment of parapneumonic effusions and empyema. Cochrane Database Syst Rev. 2004;2:CD002312. [DOI] [PubMed] [Google Scholar]
- 61.Furrer M, Rechsteiner R, Eigenmann V, Signer C, Althaus U, Ris HB. Thoracotomy and thoracoscopy: postoperative pulmonary function, pain and chest wall complaints. Eur J Cardiothorac Surg. 1997;12:82-87 [DOI] [PubMed] [Google Scholar]
- 62.Dajczman E, Gordon A, Kreisman H, Wolkove N. Long-term postthoracotomy pain. Chest. 1991;99:270-274 [DOI] [PubMed] [Google Scholar]