

Abstract
Purpose
Exercise-induced bronchoconstriction (EIB) in patients with asthma occurs more frequently in winter than in summer. The concentration of house dust mite (HDM) allergens in beds also shows seasonal variation. This study examined the relationship between seasonal differences in the prevalence of EIB and sensitization to HDMs in patients with asthma.
Methods
The medical records of 74 young adult male patients with asthma-like symptoms who underwent bronchial challenge with methacholine, 4.5% saline and exercise, and allergen skin prick tests, were reviewed. The subjects were divided into summer (n=27), spring/fall (n=26) and winter (n=21) groups according to the season during which they underwent testing.
Results
The positive responses to exercise differed according to season (48.1% in summer, 73.1% in spring/fall, and 90.5% in winter; P<0.01). In addition, the prevalence of positive responses to HDM (70.4%, 88.5%, and 95.2%, respectively; P<0.05) and pollen skin tests (37.0%, 19.2%, and 0%, respectively; P<0.01) also showed significant seasonal differences. Severe responses to 4.5% saline showed a similar trend, although it was not statistically significant (44.4%, 50.0%, and 71.4%, respectively; P=0.07). Skin test reactivity to HDMs was significantly related to maximal fall in forced expiratory volume in one second (FEV1) following exercise (r=0.302, P<0.01) and the index of airway hyperresponsiveness (AHR) to 4.5% saline (r=-0.232, P<0.05), but not methacholine (r=-0.125, P>0.05).
Conclusions
Positive skin test reactions to HDMs and EIB occurred in winter, spring/fall, and summer in decreasing order of frequency. Seasonal variation in the prevalence of EIB may be related to seasonal variation in sensitization to HDMs, accompanied by differences in indirect, but not direct, AHR.
Keywords: Asthma, bronchoconstriction, exercise, house dust mite, season
INTRODUCTION
Exercise is a common stimulus for asthma symptoms in asthmatic patients. The prevalence of exercise-induced asthma (EIA) in asthmatic patients has been reported to be 40%-90%.1 This wide variation may result from many factors, including the severity of the underlying airway hyperresponsiveness (AHR) in enrolled patients and environmental factors such as cold air. Our previous studies have shown that the maximal fall in forced expiratory volume in one second (FEV1) after exercise (exercise-induced bronchoconstriction, EIB) is significantly related to methacholine-AHR2,3 and 4.5% hypertonic saline-AHR,2 and that the prevalence of EIA in patients with perennial asthma is significantly related to temperature and humidity (prevalence of 50.0% in summer, 86.4% in spring/fall, and 84.0% in winter).4
More than 80% of asthma cases occur through Th2 immune reactions after exposure to allergens such as house dust mites (HDMs) in subjects with allergic diathesis.5 The HDMs Dermatophagoides farinae (D. farinae) and D. pteronyssinus are the most common allergens,6 and sensitization to HDMs is significantly related to AHR.7 Sears et al.8 reported that the relative risk for AHR is 4.45 times higher in children sensitized to HDMs. Pollen allergy is more significantly related to allergic rhinitis than to asthma.9 In our previous study, we also found that the relative risk for moderate or severe methacholine-AHR was 1.21 times higher in subjects sensitized to D. farinae and 0.72 times higher in subjects sensitized to hazel pollen than in non-sensitized subjects.6
Concentrations of indoor HDMs and pollen show seasonal variation,10,11 while the incidence of AHR varies seasonally depending on the concentration of HDMs.10 The prevalence of EIA may therefore also differ between seasons not only under the direct influence of temperature and humidity, but also under the indirect influence of concentrations of allergens, which change in association with changes in temperature and humidity. Although it has been demonstrated that EIA is aggravated during pollen seasons in patients with pollen allergy,12,13 no study, as far as we know, has examined whether EIA is aggravated seasonally when sensitization to HDMs is increased in patients with asthma. Thus, this study was conducted to examine the relationship between seasonal differences in the prevalence of EIA and sensitization to HDMs in asthmatics.
MATERIALS AND METHODS
Subjects
Young male subjects with asthma-like symptoms aged 18-30 years who visited the Department of Allergy, Chonnam National University Hospital in order to obtain a medical certificate that granted them exemption from military service between January 2004 and February 2009 were enrolled into this study. From their charts, we retrospectively collected information about patient age, height, duration of asthma, and the results of skin prick tests, and bronchial challenge with methacholine, 4.5% hypertonic saline, or exercise. Subjects who underwent all of the three aforementioned bronchial challenge tests were included in the study. The subjects were divided into summer (June to September, n=27), spring/fall (March to May/October to November, n=26) and winter (December to February, n=21) groups according to the seasons during which they underwent the tests.
Bronchial challenge tests
Bronchial challenge tests were performed according to our protocol. Exercise challenges were performed first, 4.5% hypertonic saline tests on the next day, and methacholine-AHR tests at least 4 hours after the hypertonic saline tests. The following medications were withdrawn before the tests: anti-histamines (from at least 48 hours before the tests), theophylline (24 hours), long-acting β2 agonists (24 hours), ipratropium (12 hours), and short-acting β2 agonists (8 hours). Pulmonary function tests were conducted using a Spiro-Analyzer ST-250 computerized spirometer (Fukuda Sangyo, Tokyo, Japan). The representative values for spirometry were selected from the "best spirogram"-the one for which the sum of forced vital capacity (FVC) and FEV1 was largest among the three or more acceptable spirograms-according to the method proposed by the Intermountain Thoracic Society.14 Regression equations provided by Crapo et al.15 were used for reference spirometric values.
Exercise challenges
Exercise challenges were performed using the free running method described in a previous study.4 Exercise intensity was increased during the first 2-3 minutes until the heart rate (HR) reached 85% of the maximal rate (220 minus the subject age), and this HR was maintained for up to 6 minutes after the start of the exercise. FEV1 was measured before exercise and 1, 3, 5, 7, 10, 15, 20, 30, 45, and 60 minutes after exercise (three times per time point). The highest value at each time point was regarded to be representative. EIB was calculated using the following equation: EIB=(pre-exercise FEV1 value - post-exercise lowest FEV1 value)/pre-exercise FEV1 value×100. EIA was defined as an EIB of ≥15%. By modifying the EIA severity assessment method of Lazo-Velásquez et al.,16 which uses peak expiratory flow, we rated EIB on a 4-point scale:<15%, 0 points (normal); 15%-25%, 1 point (mild); 25%-50%, 2 points (moderate); and ≥50%, 3 points (severe).
Hypertonic saline challenge tests
Hypertonic saline challenge tests were performed according to the method proposed by Iredale et al.17 The subjects inhaled 4.5% hypertonic saline aerosols generated using an Ultra-neb 200 ultrasonic nebulizer (DeVilbiss Co, Somerset, PA; output 0.15 mL/min) through a mouthpiece with the nose clipped, for inhalation periods that doubled successively in length (0.5, 1, 2, 4, and 8 minutes). FEV1 was measured 30 and 90 seconds after each inhalation period. The test proceeded to the next step within 3 minutes of the end of the previous inhalation period. If FEV1 decreased by <10%, the inhalation time was doubled; if FEV1 decreased by 10%-15%, the inhalation time was maintained; if FEV1 decreased by ≥15% or the maximal volume of saline was inhaled, inhalation was stopped. A dose-response curve was constructed by plotting % decrease in FEV1 against the logarithm of the cumulative volume of aerosol delivered (in mL) for each inhalation period. The provocative dose of hypertonic saline that induced a 15% fall of FEV1 (PD15) was calculated by linearly interpolating from the log-dose-response curve. For subjects who did not respond to the maximal saline dose, the provocation dose was assigned a value by doubling the maximal dose inhaled. By modifying the method of Anderson and Brannan,18 we defined a positive response to the test as a PD15 value of ≤20 mL (instead of maximal dose), and rated the degree of airway responsiveness to hypertonic saline on a 4-point scale: >20 mL, 0 points (normal); 6-20 mL, 1 point (mild); 2-6 mL, 2 points (moderate); and <2 mL, 3 points (severe).
Methacholine provocation tests
Methacholine-AHR tests were performed using the tidal breathing method standardized by Cockcroft.19 Fresh methacholine solutions with concentrations of 0.075, 0.15, 0.31, 1.25, 2.5, 5.0, 10, and 25 mg/mL were prepared every morning of the study. Aerosols generated using a DeVilbiss 646 jet nebulizer (DeVilbiss Co; output 0.13 mL/min) were inhaled by tidal breathing for 2 minutes at 5-minute intervals. When the FEV1 value decreased by ≥20% as compared with the post-saline control value, methacholine inhalation was stopped. The concentration that reduced the FEV1 value by 20% (PC20, mg/mL) was obtained by linear interpolation from the log dose-response curve. If FEV1 did not decrease by ≥20% at a concentration of 25 mg/mL, the PC20 value was regarded to be 50 mg/mL. The method of Woolcock and Jenkins20 for classifying the severity of methacholine-AHR was modified with reference to the classification by Cockcroft,21 and severity was rated on a 4-point scale: PC20>16 mg/mL, 0 points (normal); 2-16 mL, 1 point (mild); 0.2-2 mL, 2 points (moderate); and <0.2 mL, 3 points (severe).
Skin prick tests
Skin pick tests were performed with eight common allergens, including HDMs (D. farinae and D. pteronyssinus), cat, dog, mold (Aspergillus fumigatus), tree pollen (hazel), grass pollen (timothy), and weed pollen (ragweed). A histamine solution (1 mg/mL) was used as a positive control and normal saline as a negative control. Wheal and flare sizes were measured 15 minutes after the application of test allergens. The largest and smallest diameters of wheals at right angles to each other were summed and divided by 2. Skin test positivity was assessed by calculating the ratio of the size of the wheal induced by the allergen to the size of the wheal induced by histamine solution. Size ratios were classified as follows: 25%-50%, 1+; 50%-99%, 2+; 100%-199%, 3+; and ≥200%, 4+. The atopy score was defined as the sum of the degrees of positivity (maximum, 32).22 Reactions with scores of ≥3+ were deemed to indicate clinically significant allergy.23
Statistical analysis
Data are presented as the mean±standard error. Statistical analyses were performed using SPSS for Windows version 18.0 (SPSS Inc., Chicago, IL, USA). Statistical comparisons were made using the chi-square test for trends, the Kruskal-Wallis test, the Mann-Whitney U test, and logistic regression. Correlations between variables were assessed using Spearman rank correlation coefficients. A P value of <0.05 was considered statistically significant.
RESULTS
There was no significant difference in age or atopy score between the different season groups (Table 1). However, the duration of asthma was significantly longer in the summer and winter groups than the spring/fall group, and the proportion of subjects with peripheral blood eosinophil counts≥5% was higher in the summer group. In addition, the rate of positive results for skin tests with HDMs progressively increased, and for tests with pollen progressively decreased, from summer and spring/fall to winter.
Table 1.
Clinical characteristics of young male patients with asthma in the summer, spring/fall, and winter groups, and bronchoprovocation test results
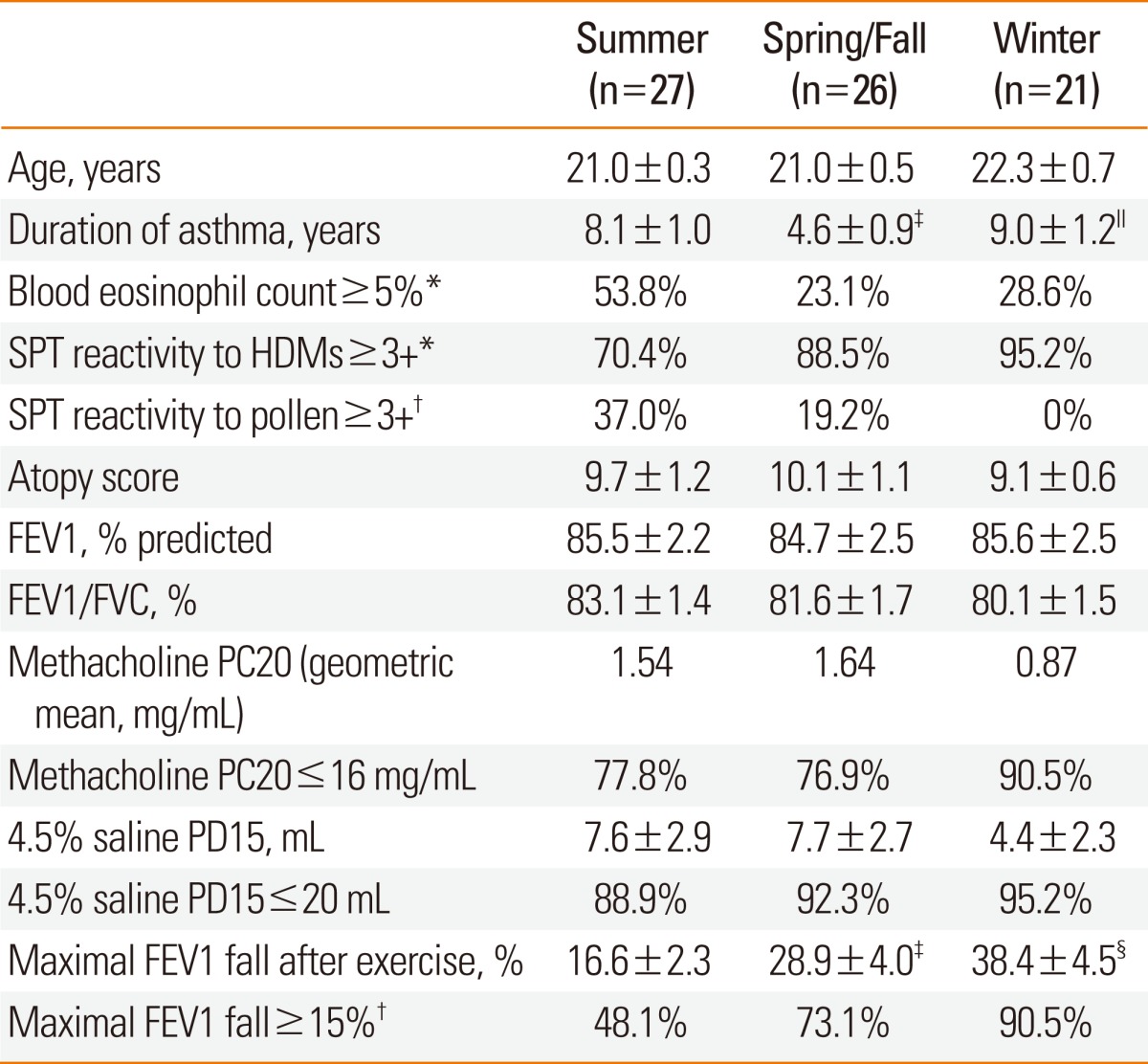
SPT reactivity ≥3+: ≥100% allergen/histamine wheal size ratio in skin prick test.
HDMs, house dust mites: D. farinae and D. pteronyssinus.
Pollen: hazel, timothy and ragweed.
Atopy score: sum of skin prick test grades for two HDMs, three types of pollen, cat, dog, and A. fumigatus.
FEV1, forced expiratory volume in one second; FVC, forced vital capacity; PC20, provocative concentration of methacholine causing a 20% fall in FEV1; PD15, cumulative provocative dose of 4.5% saline causing a 15% fall in FEV1.
*P<0.05, †P<0.01 (chi-square test); ‡P<0.05, §P<0.001 vs. summer; ∥P<0.01 vs. spring/fall.
There was no significant difference in baseline lung function or methacholine-AHR between the different seasons (Table 1). However, the prevalence of severe hypertonic saline-AHR tended to be higher during low-temperature seasons, although not significantly so (44.4% in summer, 50.0% in spring/fall and 71.4% in winter; χ2=3.3, P=0.071; Figure). Moreover, EIB was significantly larger in spring/fall and winter than in summer, and so the prevalence of EIA was lowest in summer and highest in winter (Table 1; Figure). When the severity of AHR was compared among the different measurement methods, moderate methacholine-AHR and moderate EIB were similar to severe hypertonic saline-AHR.
Figure.

Comparisons of the distribution of subjects with varying degrees of airway responsiveness to methacholine and 4.5% hypertonic saline aerosols, and exercise challenges across different seasons. Mild/moderate/severe: methacholine PC20, 2-16/0.2-2/<0.2 mg/mL; 4.5% saline-PD15, 6-20/2-6/<2 mL; % fall in FEV1 after exercise, 15-25/25-50/>50%.
EIB showed a direct correlation with skin test reactivity to HDMs and atopy score, but an inverse correlation with the FEV1/FVC ratio, methacholine-AHR, and hypertonic saline-AHR (Table 2). Methacholine-AHR and hypertonic saline-AHR were correlated with the duration of asthma, blood eosinophil count, FEV1, atopy score, and FEV1/FVC ratio. Hypertonic saline-AHR, but not methacholine-AHR, was significantly correlated with skin reactivity to HDMs.
Table 2.
Relationship between airway responses to various stimuli and other variables in asthma
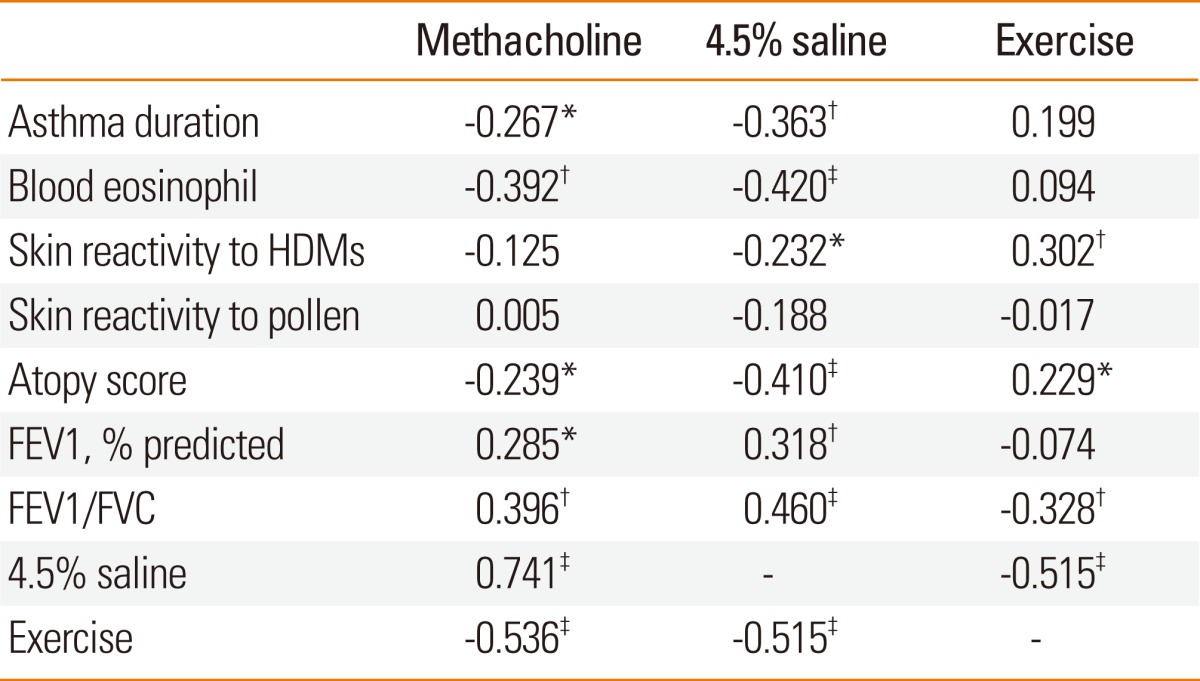
HDMs, house dust mites: D. farinae and D. pteronyssinus.
Pollen: hazel, timothy, and ragweed.
Atopy score: sum of skin prick test grades for two HDMs, three types of pollen, cat, dog, and A. fumigatus.
FEV1, forced expiratory volume in one second; FVC, forced vital capacity.
*P<0.05, †P<0.01, ‡P<0.001.
Season, duration of asthma, FEV1/FVC ratio, methacholine-AHR, and hypertonic saline-AHR showed significant relative risks for moderate or severe EIB (Table 3). The crude odds ratios (ORs) for moderate or severe EIB were 22.2 in moderate or severe methacholine-AHR and 5.8 in severe hypertonic saline-AHR. In a multivariate logistic regression analysis, the adjusted OR for moderate or severe EIB was 19.28 (95% confidence interval [CI]=3.06-121.51, P=0.002) in season and 38.40 (6.17-239.22, P=0.000) in moderate or severe methacholine-AHR.
Table 3.
Relative risk for moderate to severe exercise-induced asthma
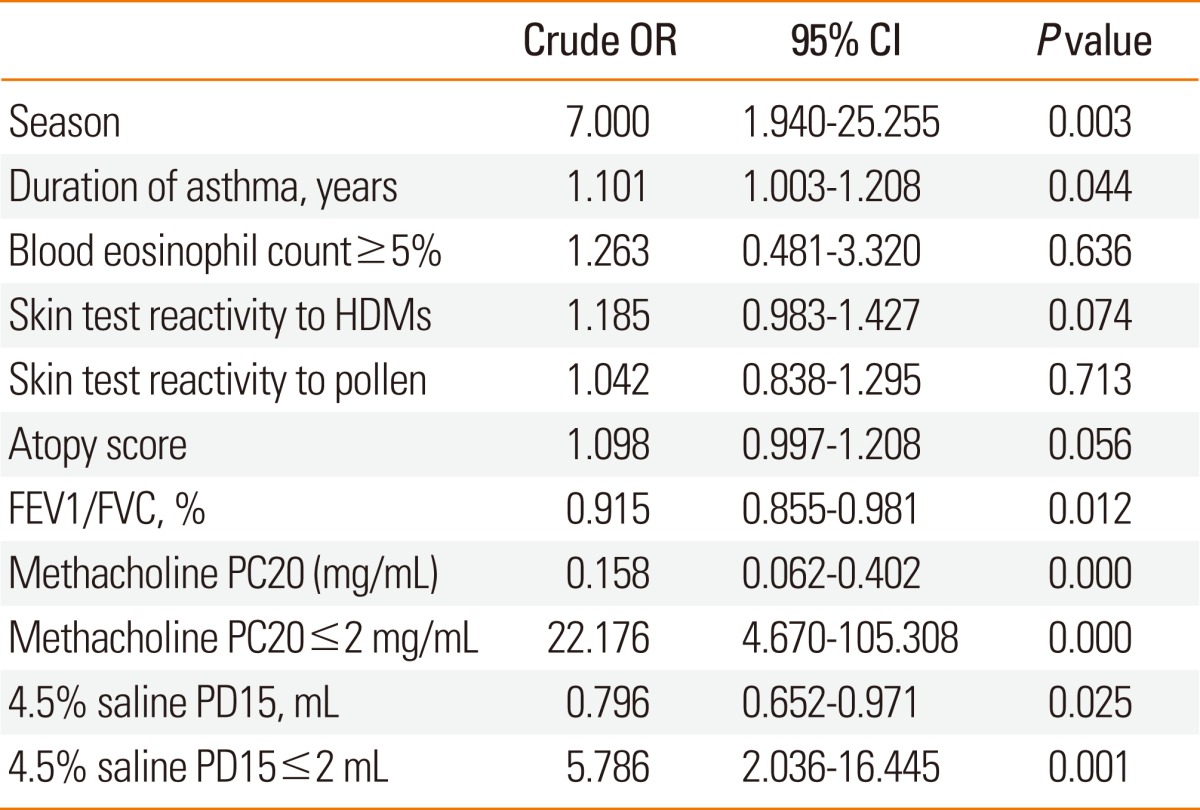
OR, odds ratio; CI, confidence interval.
HDMs, house dust mites: D. farinae and D. pteronyssinus.
Pollen: hazel, timothy, and ragweed.
Atopy score: sum of skin prick test grades for two HDMs, three types of pollen, cat, dog, and A. fumigatus.
FEV1, forced expiratory volume in one second; FVC, forced vital capacity; PC20, provocative concentration of methacholine causing a 20% fall in FEV1; PD15, cumulative provocative dose of 4.5% saline causing a 15% fall in FEV1.
DISCUSSION
In this study, the prevalence of EIA among young male patients with asthma-like symptoms was 48.1% in summer, 73.1% in spring/fall, and 90.5% in winter, suggesting significant seasonal variation. In our previous study, the prevalence of EIA was 50.0% in summer, 86.4% in spring/fall, and 84.0% in winter.4 These results may be explained by the fact that there are considerable seasonal differences in mean temperature (25.3℃ in summer, 16.1℃ in fall, 11.0℃ in spring, and 3.5℃ in winter) and humidity (74.6% in summer, 69.1% in fall, 57.7% in spring, and 66.2% in winter) in Korea.4 In the previous and present studies, exercise challenges were performed using the free running method. The test results were therefore directly affected by temperature and humidity. These results represent the actual clinical setting, as the free running was performed outdoors, and it is possible that the seasonal variation in EIA may not be easily observed when exercise challenges are performed indoors with a treadmill or a bicycle.
In addition, the results of this study indicate that the seasonal variation in EIA prevalence may also be affected by seasonal variation in the rate of sensitization to allergens and the severity of AHR. The rate of clinically significant sensitization (≥3+) to HDMs (70.4% in summer, 88.5% in spring/fall, and 95.2% in winter) and pollen (37.0%, 19.2%, and 0%, respectively) varied seasonally. Based on our findings that both the rate of sensitization to HDMs and prevalence of EIA were low in summer and high in winter, and that there was a significant correlation between the severity of EIB and skin reactivity to HDMs, it is conceivable that sensitization to HDMs may have a significant effect on the prevalence of EIA. Because sensitization to HDMs is significantly correlated with AHR,7 and because subjects sensitized to HDMs have a higher risk of AHR,6,8 AHR associated with sensitization to HDMs would easily lead to EIB. The rate of sensitization to pollen is naturally low in winter, and pollen allergy is more closely related to allergic rhinitis than to asthma,9 although EIA can be aggravated during pollen seasons in patients with asthma who are sensitized to pollen.12,13 Therefore, our patients that were sensitized to pollen seemed to show an inverse correlation with EIA, unlike those sensitized to HDMs. The relative risk of AHR was 0.72 times higher in patients sensitized to hazel pollen in our previous study.6
Methacholine-AHR and 4.5% hypertonic saline-AHR did not show statistically significant seasonal variation, as shown in our previous study.4 However, the geometric mean methacholine PC20 value tended to be lower in winter (0.87 mg/mL in winter, 1.54 mg/mL in summer, and 1.64 mg/mL in spring/fall), and hypertonic saline-AHR tended to be more severe in winter (71.4% in winter, 44.4% in summer, and 50.0% in spring/fall). Based on our findings that EIB was significantly correlated with methacholine-AHR and hypertonic saline-AHR, and that the relative risk of moderate or severe EIB was 22 times higher in patients with moderate or severe methacholine-AHR and 5.8 times higher in those with severe hypertonic saline-AHR, we conclude that seasonal variation in AHR may affect seasonal variation in the prevalence of EIA.
Although seasonal variation in methacholine-AHR was minimal, the variation in hypertonic saline-AHR showed a similar trend to that for EIA in this study. Methacholine acts directly on receptors in airway smooth muscles. Thus, methacholine-AHR can occur in patients with respiratory diseases other than asthma.24 However, exercise and hypertonic saline act through chemical mediators released by inflammatory cells or sensory nerve stimulation, and the test results obtained using these indirect stimuli are more specific for asthma.25 Moreover, since changes in the osmotic pressure of airway lining fluid is an important and common mechanism of EIA and hypertonic saline-AHR,26 the EIB and hypertonic saline-AHR results may be more closely related, and hypertonic saline-AHR may well reflect seasonal variation, similar to EIB. Asthma is an inflammatory airway disease that occurs after exposure to offending allergens, and it is associated with irreversible structural changes (airway remodeling) as a result of an aberrant repair process. While airway inflammation is associated with variable or inducible AHR that can be improved by inhaled steroids, airway remodeling induces permanent AHR that cannot be improved with medical treatment.27 Methacholine-AHR is associated with both variable AHR and permanent AHR, whereas EIA and hypertonic saline-AHR are mainly associated with variable AHR.3,27 Therefore, although hypertonic saline-AHR and EIB sensitively represent seasonal variation in sensitization to HDMs, associated airway inflammation, and variable AHR, methacholine-AHR may not properly reflect slight seasonal variation in variable AHR because of preexisting permanent AHR. These findings are consistent with the results of a previous study showing that hypertonic saline-AHR is more closely related to the number of eosinophils, interleukin (IL)-5 concentration, and the interferon-γ:IL-5 ratio in sputum than to methacholine-AHR.28 Further, these results are also consistent with a longitudinal study showing that changes in EIB over time are larger than those in methacholine-AHR.3
Despite the definition of positive hypertonic saline-AHR with a fall in FEV1 of ≥15% being restricted to ≤20 mL in this study, rather than the maximal provocation dose of saline proposed by Anderson and Brannan,18 positive reactions to hypertonic saline occurred more frequently than reactions to methacholine or exercise. In addition, severe hypertonic saline-AHR had a prevalence similar to that of moderate methacholine-AHR and moderate EIB. When the hypertonic saline-AHR test was first introduced into clinical practice, a positive reaction was defined as a fall in FEV1 of ≥20%. However, this definition has since been changed to a fall in FEV1 of ≥15% based on data from numerous healthy subjects.29 Moreover, review articles by Anderson and Gibson30 in 1997 and Anderson and Brannan18 in 2003 used PD15 to classify the severity of AHR; therefore, we used PD15 in the present study. However, considering the high rate of hypertonic saline-AHR, further studies on PD20 and more strictly defined criteria for the severity of AHR are needed to accurately interpret test results obtained using hypertonic saline.
The indoor concentration of HDMs is closely related to humidity, and the number of HDMs increases in summer and progressively decreases thereafter; however, the concentration of group 1 mite allergens is maintained until winter.31 In Korea, the concentration of Der f 1 increases in summer and is maintained until winter. Serum Der f 1-specific antibody levels are high in inhabitants with high Der f 1 levels in their bedclothes dust.32 HDM concentrations32 and HDM-specific antibody levels33 are highest in autumn. Patients sensitized to HDMs have severe methacholine-AHR.34 With increasing concentrations of Der p 1, histamine-AHR becomes more severe,10 and severe asthma attacks occur more frequently.33 However, the rate of sensitization to HDMs was highest in winter in the present study. Since we only assessed subjects with asthma who wanted to obtain a medical certificate granting them exemption from military service, it is possible that their symptoms were aggravated in the fall, but that they were not admitted to the hospital until winter due to long waiting times. For this reason, our results appeared to differ from those of previous studies. Further studies on this issue are therefore warranted. The number of peripheral blood eosinophils was previously found to be closely related to AHR.35 Similarly, our study showed that there was a significant correlation between the number of eosinophils and methacholine-AHR/hypertonic saline-AHR. However, since the sensitization rate to pollen and the number of eosinophils increased in summer, the relationship between eosinophilia and EIA that usually occurs in other seasons became insignificant in this study.
Hypertonic saline-AHR, which occurs through a similar mechanism to EIB, but was examined indoors in contrast to the free-running test for EIB, showed only a non-significant trend toward increased prevalence during low-temperature seasons, while EIB showed an apparent increase in prevalence. Thus, outdoor cold air and humidity would play roles as confounding factors in the EIB test and the actual influence of sensitization to HDMs on EIB would be limited. Further study of EIB using a treadmill or a bicycle indoors is required to exclude the effects of cold air and humidity. Other limitations of this study were the small numbers of subjects and the fact that the study group was limited to young men. Further studies are necessary to address these limitations.
In summary, EIB occurred most frequently in winter, followed by spring/fall and summer. Skin reactivity to HDMs and pollen also showed seasonal variation. Methacholine-AHR did not show significant seasonal variation, but hypertonic saline-AHR showed similar variation to EIB. The results of this study suggest that the change in hypertonic saline-AHR associated with sensitization to HDMs may be related to seasonal variation in EIB.
Footnotes
There are no financial or other issues that might lead to conflict of interest.
References
- 1.McFadden ER., Jr . Approach to the patient with exercise-induced airway narrowing. In: Adkinson NF Jr, Bochner BS, Busse WW, Holgate ST, Lemanske RF Jr, Simons FER, editors. Middleton's allergy: principles & practice. 7th ed. Philadelphia: Mosby; 2009. pp. 1385–1393. [Google Scholar]
- 2.Choi IS, Chung SW, Koh YI, Sim MK, Hong SN, Moon JS. Airway hyperresponsiveness to hypertonic saline as a predictive index of exercise-induced bronchoconstriction. Korean J Intern Med. 2005;20:284–289. doi: 10.3904/kjim.2005.20.4.284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kim CS, Choi IS, Kim SH, Woo H, Sim HJ, Han ER. A longitudinal study on the relationship between methacholine airway hyperresponsiveness and exercise-induced bronchoconstriction. Korean J Med. 2009;77:472–479. [Google Scholar]
- 4.Koh YI, Choi IS. Seasonal difference in the occurrence of exercise-induced bronchospasm in asthmatics: dependence on humidity. Respiration. 2002;69:38–45. doi: 10.1159/000049368. [DOI] [PubMed] [Google Scholar]
- 5.Holgate ST, Lemanske RF, Jr, O'Byrne PM, Kakumanu S, Busse WW. Asthma pathogenesis. In: Adkinson NF Jr, Bochner BS, Busse WW, Holgate ST, Lemanske RF Jr, Simons FER, editors. Middleton's allergy: principles & practice. 7th ed. Philadelphia: Mosby; 2009. pp. 893–919. [Google Scholar]
- 6.Han ER, Choi IS, Lee S, Cho YW. Airway hyperresponsiveness-related aeroallergens in suspected asthma. Korean J Asthma Allergy Clin Immunol. 2007;27:105–110. [Google Scholar]
- 7.Choi IS, Koh YI, Koh JS, Lee MG. Sensitivity of the skin prick test and specificity of the serum-specific IgE test for airway responsiveness to house dust mites in asthma. J Asthma. 2005;42:197–202. [PubMed] [Google Scholar]
- 8.Sears MR, Herbison GP, Holdaway MD, Hewitt CJ, Flannery EM, Silva PA. The relative risks of sensitivity to grass pollen, house dust mite and cat dander in the development of childhood asthma. Clin Exp Allergy. 1989;19:419–424. doi: 10.1111/j.1365-2222.1989.tb02408.x. [DOI] [PubMed] [Google Scholar]
- 9.Gergen PJ, Turkeltaub PC. The association of individual allergen reactivity with respiratory disease in a national sample: data from the second National Health and Nutrition Examination Survey, 1976-80 (NHANES II) J Allergy Clin Immunol. 1992;90:579–588. doi: 10.1016/0091-6749(92)90130-t. [DOI] [PubMed] [Google Scholar]
- 10.van der Heide S, De Monchy JG, De Vries K, Dubois AE, Kauffman HF. Seasonal differences in airway hyperresponsiveness in asthmatic patients: relationship with allergen exposure and sensitization to house dust mites. Clin Exp Allergy. 1997;27:627–633. doi: 10.1046/j.1365-2222.1997.d01-554.x. [DOI] [PubMed] [Google Scholar]
- 11.Crisafulli D, Almqvist C, Marks G, Tovey E. Seasonal trends in house dust mite allergen in children's beds over a 7-year period. Allergy. 2007;62:1394–1400. doi: 10.1111/j.1398-9995.2007.01533.x. [DOI] [PubMed] [Google Scholar]
- 12.Henriksen JM. Exercise-induced bronchoconstriction. Seasonal variation in children with asthma and in those with rhinitis. Allergy. 1986;41:499–506. doi: 10.1111/j.1398-9995.1986.tb00335.x. [DOI] [PubMed] [Google Scholar]
- 13.Karjalainen J, Lindqvist A, Laitinen LA. Seasonal variability of exercise-induced asthma especially outdoors. Effect of birch pollen allergy. Clin Exp Allergy. 1989;19:273–278. doi: 10.1111/j.1365-2222.1989.tb02383.x. [DOI] [PubMed] [Google Scholar]
- 14.Morris AH, Kanner RE, Crapo RO, Gardner RM. Clinical pulmonary function testing. a manual of uniform laboratory procedures. 2nd ed. Salt Lake City, UT: Intermountain Thoracic Society; 1984. [Google Scholar]
- 15.Crapo RO, Morris AH, Gardner RM. Reference spirometric values using techniques and equipment that meet ATS recommendations. Am Rev Respir Dis. 1981;123:659–664. doi: 10.1164/arrd.1981.123.6.659. [DOI] [PubMed] [Google Scholar]
- 16.Lazo-Velásquez JC, Lozada AR, Cruz HM. Evaluation of severity of bronchial asthma through an exercise bronchial challenge. Pediatr Pulmonol. 2005;40:457–463. doi: 10.1002/ppul.20275. [DOI] [PubMed] [Google Scholar]
- 17.Iredale MJ, Wanklyn SA, Phillips IP, Krausz T, Ind PW. Non-invasive assessment of bronchial inflammation in asthma: no correlation between eosinophilia of induced sputum and bronchial responsiveness to inhaled hypertonic saline. Clin Exp Allergy. 1994;24:940–945. doi: 10.1111/j.1365-2222.1994.tb02725.x. [DOI] [PubMed] [Google Scholar]
- 18.Anderson SD, Brannan JD. Methods for "indirect" challenge tests including exercise, eucapnic voluntary hyperpnea, and hypertonic aerosols. Clin Rev Allergy Immunol. 2003;24:27–54. doi: 10.1385/CRIAI:24:1:27. [DOI] [PubMed] [Google Scholar]
- 19.Cockcroft DW. Measurement of airway responsiveness to inhaled histamine or methacholine: method of continuous aerosol generation and tidal breathing inhalation. In: Hargreave FE, Woolcock AJ, editors. Airway responsiveness: measurement and interpretation - proceedings from a workshop held at Mont Ste. Marie, Quebec, June 15-17, 1983- Mississauga, ON: Astra Pharmaceuticals Canada Ltd; 1985. pp. 22–28. [Google Scholar]
- 20.Woolcock AJ, Jenkins CR. Assessment of bronchial responsiveness as a guide to prognosis and therapy in asthma. Med Clin North Am. 1990;74:753–765. doi: 10.1016/s0025-7125(16)30550-8. [DOI] [PubMed] [Google Scholar]
- 21.Cockcroft DW. Airway responsiveness. In: Barnes PJ, Grunstein MM, Leff AR, Woolcock AJ, editors. Asthma. Philadelphia: Lippincott-Raven Publishers; 1997. pp. 1253–1266. [Google Scholar]
- 22.Crockcroft DW, Murdock KY, Berscheid BA. Relationship between atopy and bronchial responsiveness to histamine in a random population. Ann Allergy. 1984;53:26–29. [PubMed] [Google Scholar]
- 23.Adinoff AD, Rosloniec DM, McCall LL, Nelson HS. Immediate skin test reactivity to Food and Drug Administration-approved standardized extracts. J Allergy Clin Immunol. 1990;86:766–774. doi: 10.1016/s0091-6749(05)80181-2. [DOI] [PubMed] [Google Scholar]
- 24.O'Byrne PM. Airway hyperresponsiveness. In: Middleton E Jr, Reed CE, Ellis EF, Adkinson NF Jr, Yunginger JW, Busse WW, editors. Allergy: principles & practice. 5th ed. Toronto, ON: Mosby; 1998. pp. 859–866. [Google Scholar]
- 25.Van Schoor J, Joos GF, Pauwels RA. Indirect bronchial hyperresponsiveness in asthma: mechanisms, pharmacology and implications for clinical research. Eur Respir J. 2000;16:514–533. doi: 10.1034/j.1399-3003.2000.016003514.x. [DOI] [PubMed] [Google Scholar]
- 26.Godfrey S. Exdercise-induced asthma. In: Barnes PJ, Grunstein MM, Leff AR, Woolcock AJ, editors. Asthma. Philadelphia: Lippincott-Raven Publishers; 1997. pp. 1105–1119. [Google Scholar]
- 27.Cockcroft DW, Davis BE. Mechanisms of airway hyperresponsiveness. J Allergy Clin Immunol. 2006;118:551–559. doi: 10.1016/j.jaci.2006.07.012. [DOI] [PubMed] [Google Scholar]
- 28.Choi IS, Hong SN, Lee YK, Koh YI, Jang AS, Lee HC. Asthmatic airway inflammation is more closely related to airway hyperresponsiveness to hypertonic saline than to methacholine. Korean J Intern Med. 2003;18:83–88. doi: 10.3904/kjim.2003.18.2.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Anderson SD. Indirect challenge tests: Airway hyperresponsiveness in asthma: its measurement and clinical significance. Chest. 2010;138:25S–30S. doi: 10.1378/chest.10-0116. [DOI] [PubMed] [Google Scholar]
- 30.Anderson SD, Gibson P. Use of aerosols of hypertonic saline and distilled water (fog) In: Barnes PJ, Grunstein MM, Leff AR, Woolcock AJ, editors. Asthma. Philadelphia: Lippincott-Raven Publishers; 1997. pp. 1135–1149. [Google Scholar]
- 31.Platts-Mills TA, Hayden ML, Chapman MD, Wilkins SR. Seasonal variation in dust mite and grass-pollen allergens in dust from the houses of patients with asthma. J Allergy Clin Immunol. 1987;79:781–791. doi: 10.1016/0091-6749(87)90211-9. [DOI] [PubMed] [Google Scholar]
- 32.Kim JH, Choi SY, Lee IY, Lee YW, Yong TS, Kim CW, Song YS, Park JW, Kim YS, Park JW, Hong CS. Seasonal variation of house dust mite and its influence on the inhabitant health. Korean J Asthma Allergy Clin Immunol. 2006;26:27–34. [Google Scholar]
- 33.Kim E, Kim MJ, Lee JS, Yoon JS. Association between autumnal exacerbation and Dermatophagoides pteronyssinus specific IgE in childhood asthma. Pediatr Allergy Respir Dis. 2007;17:242–248. [Google Scholar]
- 34.Riccioni G, Di Stefano F, De Benedictis M, Verna N, Cavallucci E, Paolini F, Di Sciascio MB, Della Vecchia R, Schiavone C, Boscolo P, Conti P, Di Gioacchino M. Seasonal variability of non-specific bronchial responsiveness in asthmatic patients with allergy to house dust mites. Allergy Asthma Proc. 2001;22:5–9. doi: 10.2500/108854101778249221. [DOI] [PubMed] [Google Scholar]
- 35.Koh YI, Choi IS. Blood eosinophil counts for the prediction of the severity of exercise-induced bronchospasm in asthma. Respir Med. 2002;96:120–125. doi: 10.1053/rmed.2001.1238. [DOI] [PubMed] [Google Scholar]