

Abstract
The powerful positive results of implementing teamwork are not always achieved. It has been suggested that attempts to implement theories regarding teamwork do not always lead to those theories being put into practice, and as a result positive outcomes are not always found. The participation of employees in the development and implementation of an intervention may help to ensure that changes take place. In this longitudinal study (N = 583) of teamwork implementation in Denmark we examined the links between pre-intervention working conditions and well-being, levels of participation in planning and implementation, employees’ reports of changes in procedures, and intervention outcomes. Pre-intervention levels of autonomy and job satisfaction predicted the degree of employee participation in the planning and implementation of the intervention. Pre-intervention well-being and social support were linked directly to the degree to which employees reported changes in existing work practices concerning teamwork. In addition, participation and changes in work procedures were significantly associated with post-intervention autonomy, social support and well-being. The results indicate that employee participation in intervention processes is crucial in what appears to be an important association with perceived changes in procedures and, therefore, in intervention outcomes.
Keywords: teamwork, participation, intervention, theories-in-use, process evaluation, organizational change
Introduction
Teamwork has been linked to a number of positive outcomes in organizations. Employees working in teams have been found to report higher job satisfaction and well-being and lower levels of absenteeism than those not working in teams (Rasmussen & Jeppesen, 2006). The implementation of teamwork in healthcare settings has also been shown to improve important objective outcomes such as patient mortality rates (Michie & West, 2004). However, in a review of the research literature, Bambra, Egan, Thomas, Petticrew, and Whitehead (2007) reported that team intervention effects have been inconsistent. They suggested that this could be because of the faulty development and implementation of some teamwork interventions. In this study we examine the importance of implementation processes in a team implementation intervention.
Some of the positive effects suggested by teamwork research include increases in social support as employees engage in joint decision-making and problem solving (Parker & Williams, 2001; Rasmussen & Jeppesen, 2006). Team member autonomy may also increase as the team manager's role becomes that of a coach and a facilitator (Day, Gronn, & Salas, 2006) where team members take over managerial tasks (Rasmussen & Jeppesen, 2006; van Mierlo, Rutte, Kompier, & Dooreward, 2005). There is some evidence that the significant changes in existing procedures (e.g. new problem-solving processes) that occur when employees are re-organized into teams are the active ingredients of teamwork interventions (Parker & Williams, 2001). It appears likely that these active ingredients bring about the positive working conditions reported by those working in teams which, in turn, are often associated with good job satisfaction and well-being (Rasmussen & Jeppesen, 2006; van Mierlo et al., 2005).
In this study we examined two neglected aspects of the teamwork intervention process in order to understand better the mediating mechanisms underpinning effective teamwork implementation. First, we examined directly employees’ reports of whether changes in existing work procedures were implemented. This is in contrast to much previous research in which the assumption is often that teamworking is being implemented according to plan. We did this to test whether employees targeted during the intervention perceived that changes in procedures concerning teamwork had taken place (Argyris, 2004), and whether the reporting of these changes was related to intervention outcomes. Second, we examined the role of employee participation in the intervention processes. Participation is generally recommended and widely used in intervention research (Kompier, Geurts, Grundemann, Vink, & Smulders, 1998) but to our knowledge no studies have included quantitative data on employees’ perceptions of participation in the change process and tested whether such perceptions were linked to the degree to which interventions were being implemented. In this study we tested whether employees’ participation in the planning and implementation of a teamwork intervention was linked to their reports of changes in work procedures, which in turn mediated intervention outcomes. Hurrell (2005) has suggested that intervention outcomes may also be directly linked to the psychological impact of participatory problem-solving processes. Therefore, we also tested the direct relationships between employees’ perceptions of participation and intervention outcomes.
Changes in procedures as active ingredients of teamwork
Argyris (1995) argued that espoused theories (the attitudes, values, policies and practices that are verbalized) need to become theories-in-use (the attitudes, values, policies and practices that are enacted) for interventions to be effective. Significant, noticeable and sustainable changes in existing values and practices, in order to successfully implement organizational change, are what Argyris (2004) labelled double-loop organizational learning. Argyris (2004) stated that “double-loop learning and effective implementation are tightly linked” (p. 44).
Research has shown that such changes are required for teamwork implementation to be an effective intervention. Parker and Williams (2001) showed in a review that effective teamwork was driven by changes in structures and procedures that led to significant changes in work design, i.e. employees within the team becoming more dependent on each other and gaining more autonomy as a group. When employees become jointly responsible for completing a task they must interact in a different way by supporting each other more when completing the task (van Mierlo et al., 2005). Teamwork theories-in-use result in individual team members having more opportunities to make decisions about how to complete work tasks and plan their work: as more responsibilities are transferred to the group, higher levels of individual and team autonomy can be expected (van Mierlo et al., 2005).
Exposure to procedures that support employees in making decisions and supporting each other in completing the team's tasks has been linked to increased affective well-being and job satisfaction (van Mierlo et al., 2005). Such findings are consistent with the predictions of established theories of work stress such as the demands-control-support model (Karasek & Theorell, 1990). It has been argued that these positive effects can only be expected if employees experience teamwork theories-in-use that have implications for perceived working conditions (Argyris, 1995). No previous study of teamwork implementation has included a direct test of whether the teamwork intervention has become a theory-in-use rather than an espoused theory. In this study we used a direct measure of perceived changes in work procedures as an indicator of theories-in-use. We defined these changes as the degree to which employees had openly discussed previous work procedures and decided which procedures to keep and which to change, and whether actual working procedures had changed and unconstructive work procedures been abandoned as a result of the team implementation intervention. We predicted that the reporting of theories-in-use would be related to post-intervention social support and autonomy.
Hypothesis 1. The extent to which participants report changes in work procedures brought about by the intervention will be positively related to post-intervention measures of intervention impact i.e. perceived social support and autonomy and job satisfaction and affective well-being.
Linking employee participation and changes in procedures
In this study we defined participation as employees’ active involvement in planning and implementing a teamwork intervention (Hurrell, 2005). This participatory approach to implementing teamwork meant that employees were involved in: (1) making decisions about the team in which they wished to work; (2) planning how they wished to work together in teams; (3) planning the implementation of teams (the speed with which they took on additional areas of responsibility); (4) defining initiatives to support team implementation, such as additional training; and (5) evaluating the results by reflecting on the implementation in teams.
Participants’ job expertise and knowledge of the organizational context have been identified as being an important supplement to the expertise of managers and intervention experts during intervention planning and implementation activities (Kompier et al., 1998). It has been argued that employee participation has increased the likelihood of changes in procedures being appropriate and useful (Rosskam, 2009), of them being integrated well into existing organizational structures (Tsutsumi, Nagami, Yoshikawa, Nogi, & Kawakami, 2009), and of them being sustained as theories-in-use (Daltuva, King, Williams, & Robins, 2009). It has also been suggested that the participatory process increases employees’ perceived ownership of change, thus helping to ensure implementation (Rosskam, 2009). Double-loop organizational learning is often evident in change processes that draw upon employee expertise, and appears to be associated with increased dialogue between key stakeholders in the change process and a critical analysis of change options (Rosskam, 2009).
There is also some direct evidence of the effects of participation on employee exposure to interventions. Lines (2004) found that participation was negatively related to resistance to change, and positively related to employees’ reports of achievement of intervention goals and organizational commitment. Nielsen, Randall, and Albertsen (2007) showed that employee influence over the content of an intervention was linked to uptake of intervention activities. However, the links between participants’ reports of participation in intervention processes and their reports of changes in working procedures (theories-in-use) have not been examined in previous research. Therefore, we tested whether participation in intervention planning and implementation increased the likelihood of employees reporting changes in existing procedures (i.e. evidence of teamworking theories-in-use).
Hypothesis 2. Employee participation in the intervention design and implementation process (measured at Time 2) will be positively associated with the reporting of changes in work procedures at Time 2.
Mechanisms linking participation and intervention outcomes
The activities involved in participatory organizational interventions often include a collaborative problem-solving dialogue (Rosskam, 2009). This dialogue has often been designed to make those involved feel more supported by colleagues (Mikkelsen, 2005). In a participatory environment, it has been argued that employees and managers act as co-learners in an empowerment process (Mikkelsen, 2005). The active collective learning that employees experience during participatory change has been found to result in strengthened working relationships with co-workers (Landsbergis & Vivona-Vaughan, 1995). Direct increases in perceived autonomy and empowerment have also been observed when employees are involved in decisions about intervention processes (Rosskam, 2009). The mechanisms described in the job demands-control model (Karasek & Theorell, 1990) indicate that in a high control-high demands condition participants are more likely to experience active jobs characterized by learning and personal growth and as a consequence improved well-being.
The significant changes in working conditions observed during participatory change processes have been linked to improvements in employee well-being and satisfaction (Landsbergis & Vivona-Vaughan, 1995; Rosskam, 2009). Bond and Bunce (2001) found that changes in job control in a participatory intervention were linked to improvements in employees’ mental health. Any additional social support stimulated by the participatory process may also buffer the impact of working conditions on employee well-being (Karasek, 2004). Control and influence in the change process has also been identified as a possible additional buffer of the impact of change-related stressors on employee well-being (Landsbergis & Vivona-Vaughan, 1995).
It has also been suggested that there can be a direct link between participation and well-being (Hurrell, 2005). In a study of hospital downsizing, Sverke, Hellgreen, Näswall, Göransson, and Öhrming (2008) found that participation in decision-making concerning downsizing was directly and positively associated with job satisfaction and directly and negatively associated with emotional exhaustion. Johnson, Brems, Mills, Neal, and Houlihan (2006) found that providing input to and exerting control over organizational changes minimized the negative effects of difficult changes at work. The activities involved in participatory processes may also directly increase employee self-esteem, with consequent increases in well-being (Mikkelsen, 2005; Rosskam, 2009).
To date no studies of participation have included direct tests of whether a measure of participation in the change process (the supposed working mechanism in participatory designs) predicts intervention outcomes. To begin to address this gap in the research literature we tested whether employees’ influence over how a teamwork intervention was planned and implemented was linked to their perceptions of autonomy over decisions in their job and levels of support at work. We then tested whether participation was directly linked to employee well-being and satisfaction or whether its impact was mediated through its links with the working conditions of autonomy and social support.
Hypothesis 3. Participation in the intervention design and implementation process (as reported post-intervention, at Time 2) will be positively related to autonomy, social support, affective well-being, and Time 2 job satisfaction.
The pre-intervention context as a predictor of employees’ experiences of interventions
It has been argued that a threshold level of maturity is needed in order for organizations to engage successfully in participatory approaches to change (Nielsen, Fredslund, Christensen, & Albertsen, 2006). Workplaces characterized by good job design and employee health may provide the conditions that allow employees the time and resources to become involved in participative interventions (Taris et al., 2003). Various problems with pre-intervention working conditions have been shown to limit participation in intervention activities and the extent to which employees were exposed to the changes in existing procedures associated with the intervention (Nielsen & Randall, 2009; Randall, Cox, & Griffiths, 2007). Evidence for this effect has also been found in studies of teamwork where poor implementation has been observed in settings characterized by poor pre-intervention levels of interpersonal relations (including team conflict), low coordination of work tasks and a lack of individual autonomy (Sims & Salas, 2007).
Several established theories can be used to make predictions about the links between the pre-intervention context and employees’ subsequent experiences of participatory interventions. The application of the job demands-resources model (Bakker & Demerouti, 2007) would suggest that workers use the pre-intervention job resources to create good working conditions during intervention processes. Conservation of Resources (COR) theory (Hobfoll, 1989, 2002) would suggest that employees try to obtain, retain and increase resources during interventions, but it is those who already have a certain level of resources who try the hardest to increase these resources, thus establishing a positive gain spiral (Bakker & Demerouti, 2007). The application of the resources framework suggests that employees experiencing high pre-intervention resources will also be those most likely to involve themselves in the teamwork intervention by working proactively to gain additional resources.
Pre-intervention social support may play a particularly important role in determining employees’ exposure to organizational interventions. For example, Seaverson, Grossmeier, Miller, and Anderson (2009) found that management and coworker support predicted uptake in workplace health promotion programmes. Social exchange theory suggests that employees who feel well-supported by their colleagues are likely to engage in extra-role behaviours and to reciprocate supportive actions by accepting new tasks, or more responsibilities (Cole, Schaninger, & Harris, 2002). Employees experiencing high levels of support themselves have been found to interact more with their colleagues in order to support them in decision-making and in planning and implementing intervention activities (Taris et al., 2003). Therefore, we hypothesize that employees experiencing high levels of support are more likely to engage in implementing teamwork structures as they see this as an opportunity to gain additional social support through the increased interaction associated with teamwork. Further, a supportive pre-intervention climate may mean that employees are more receptive to the prospect of working together more closely and to changes in the leader's role (a precursor to changes in procedures).
Pre-intervention levels of autonomy could also be linked to employees’ exposure to teamwork. High levels of autonomy have been found to be linked to engagement in decision-making about how teams will function during and after teamwork interventions (De Dreu & West, 2001). Guth and Macmillan (1986) argued that employees resist change when they fear they do not have the competencies needed to work effectively when working practices change: employees who already have experience of high levels of autonomy may be more likely to welcome a change such as teamwork that requires collaborative and reflexive work practices. This may also mean that these employees shape the teamwork intervention to fit their needs, i.e. as an opportunity to increase their levels of autonomy (van Mierlo et al., 2005) and to gain additional resources (Hobfoll, 1989). Therefore, we suggest that employees who have high autonomy pre-intervention are those most likely to engage in team decision-making and adapt to changed procedures concerning how work is allocated and conducted; the higher the pre-intervention levels of autonomy the more changes in procedures will be reported post-intervention.
It is also plausible that pre-intervention levels of overall job satisfaction and employee well-being are linked to subsequent intervention experiences. Overall levels of job satisfaction have been associated with increased effort and engagement (Taris & Schreurs, 2009). This may translate into increased uptake of intervention activities and greater willingness to engage in changed procedures that are seen to enhance the positive aspects of work. An important aspect of affective well-being is a high level of arousal and energy (van Horn, Taris, Schaufeli, & Schreurs, 2004). In their review, Lyubomirsky, King, and Diener (2005) concluded that individuals high in affective well-being experienced higher levels of social support and autonomy, were more proactive and creative, and engaged in more activities and problem solving than their counterparts with lower levels of affective well-being. We propose that employees with good well-being possess the resources to engage in teamwork activities and to invest their energy in changing procedures.
Hypothesis 4. Pre-existing levels of social support, autonomy, job satisfaction and wellbeing (Time 1) will be positively related to the degree to which employees report changes in work procedures at Time 2 (18 months after the implementation of teamworking). Furthermore, the effects of pre-intervention conditions on changes in procedures will be both direct and partially mediated through participation.
Method
Design
This study was conducted in a local government organization in the Danish elder care sector. The stimuli for the teamwork intervention were difficulties maintaining and recruiting staff and high absence levels. A senior management decision had been made that all of the local government's elder care centres would implement teamwork in an attempt to tackle these problems. The participants in this study were drawn from two of the elder care centres out of 17. All elder care centres were invited to participate by the internal team implementation consultant and two volunteered. Analyses showed the two centres did not differ from the remaining centres in terms of employee autonomy and affective well-being. (Full details of these analyses are available from the authors.)
The stated objectives of the intervention were to implement teams with some degree of self-management and to create a climate that fostered open discussions and joint decision-making that would improve employee well-being and job satisfaction. A team was defined as a group of people who have a joint task to solve and share a joint responsibility for solving the tasks; within the team there are defined roles, and team members depend on each other to solve the task. This definition is consistent with scientific definitions (e.g. Cohen & Bailey, 1997).
Prior to team implementation, employees were working in large groups. They would be allocated clients depending on their working schedule in a large geographical area. As a result employees had little local knowledge of their clients’ needs and had little opportunity for discussing solutions to problems concerning specific clients. As part of the intervention, teams were formed such that a group of employees were jointly responsible for a group of clients. Teams would receive tasks from clients and the team manager and then team members were jointly responsible for allocating tasks among themselves and deciding how they should be carried out. Other managerial tasks were also transferred to team members, e.g. rota planning and direct client contact. Regular team meetings were introduced to support this joint decision-making and problem solving. An elder care centre manager, who had previous experience with implementing teamwork, worked as a full-time consultant to develop and implement a strategy for implementing teams. The manager of every elder care centre participated in meetings where they were told about teamwork in an effort to secure their involvement and participation. The team consultant also held meetings where managers and their employees were told about the advantages and the challenges of implementing and working in teams. Further, the personnel magazine carried regular updates about the team implementation process.
Questionnaires were distributed immediately prior to the implementation of teams (Time 1) and again 18 months later (Time 2). The questionnaires included demographic questions, and measures of social support, autonomy, job satisfaction and affective well-being. At T2, in addition to the T1, measures information was also gathered on participation in the intervention process and changes in working procedures and practices (Randall, Nielsen, & Tvedt, 2009).
The ethical conduct of the study was ensured by using the guidance provided by the British Psychological Society's Code of Ethics and Conduct (2006) and the study was approved by the Danish Data Protection Agency and its regulations for data storage and protection were followed. Before completing the questionnaire, participants received information about the study and it was made clear that participation was voluntary and that their individual data would remain confidential. They returned their completed questionnaires directly by mail to the research group and confidentiality was maintained by using numbers to identify participants.
Participants
In total, 583 employees in 31 teams participated in the study. In each elder care centre about half of the employees (51% of the sample) provided care to elder people who are still in their own home (homecare) and the remainder worked in residential elder care homes. At Time 1, questionnaires were distributed to 551 staff and 447 questionnaires were returned, yielding a response rate of 81%. At Time 2 the questionnaire was distributed to 521 staff and 274 returned the questionnaire (response rate 54%). Inspection of organizational records showed that this sample was representative of the total available study population at both Time 1 and Time 2. Specific information on the demographic composition of the samples is available upon request.
Results of t-tests revealed that there were no significant differences between the two centres on measures of demographics and study variables (t-values ranged between −1.89 and .86, p >.05), but that homecare staff had been employed for a significantly shorter period than staff employed at the elder care residential homes (t (310) = −2.50, p <.05), reported higher job satisfaction (t (324) = 3.07, p <.01), higher autonomy (t (375) = 3.16, p <.01), and higher social support (t (320) = 2.60, p <.05), all at Time 1. No other significant differences were found in terms of age, gender and well-being or for Time 2 measures (t-values ranging from −1.91 to 1.18, p > .05). Analyses testing for systematic dropout from Time 1 to Time 2 revealed no significant differences between those who only responded at Time 1 to those who responded both times in terms of gender, tenure, baseline social support and autonomy. Higher levels of job satisfaction (t (335) = −2.00, p <.05) and affective well-being (t(366) = −4.08, p <.001) were reported among those who responded both times (when compared to those who did not). The sample that responded both times was also significantly older (t (342) = −2.30, p <.05). Whether a participant had responded both times or only at Time 2 was not correlated to intervention outcomes; therefore we did not control for these variables in our subsequent analyses. Group/team sizes varied from two to 35. The mean group size was 15 at Time 1 and mean team size was 12 at Time 2. At Time 2, the very large groups had been divided into smaller groups to develop interdependency between members of these smaller teams. Thus one manager who previously had one large group of 30–35 members could have up to three teams with 10–12 members in each (e.g. two day-shift teams and a night-shift team). Team response rates ranged from 55% to 100%.
Outcome measures
Autonomy (four items)
This scale measured the extent to which employees had autonomy over whom they worked with, the amount of work they had to do or their decision-making authority (Kristensen, Hannerz, Høgh, & Borg, 2005). An example of an item was “Do you have a large degree of influence on decisions concerning your work?” Responses to these items were given on a five-point scale ranging from 1 (always) to 5 (never/hardly ever). Cronbach's α at Time 1 was .73, and .74 at Time 2.
Social support (two items)
This measured the degree to which employees felt supported by colleagues (Kristensen, Hannerz, Høgh, & Borg, 2005). An example of an item was: “I receive help and support from my colleagues”. Responses to these items were given on a five-point scale ranging from 1 (to a very large extent) to 5 (to a very small extent). Inter-item correlations were .73, at Time 1 and .70 at Time 2.
Job satisfaction (five items)
This scale was an overall measure of job satisfaction (Kristensen, Hannerz, Høgh, & Borg, 2005). An example of an item was: “How satisfied are you with your job as a whole, everything taken into consideration?” The response categories were very satisfied to highly dissatisfied on a four-point Likert scale. Cronbach's α was .82 at Time 1 and Time 2.
Affective well-being (five items)
This scale measured the degree to which employees had been in a positive state of mind over the past two weeks, e.g. happy and vivacious (Bech, Olsen, Kjoller, & Rasmussen, 2003). An example of an item was: “Have you over the past two weeks felt active and energetic?” Ratings were provided on as five-point scale from 1 (all the time) to 5 (not at all). Cronbach's α at Time 1 was .87, and .85 at Time 2.
Intervention process measures
Measures were also taken of employee participation in the change process and their self-reported changes in work procedures associated with the implementation of teams (Randall et al., 2009).
Employee participation (three items)
Employees were asked to comment upon their involvement in the design and implementation of the intervention. The items were: “I was involved in the design of the implementation of teams at the team level,” “I was involved in the design of the implementation of teams at the organizational level,” and “Management has made a great effort to involve employees in the change process”. Responses to these items were given on a five-point from 1 (strongly agree) to 5 (highly disagree). Cronbach's α = .77.
Changes in procedures (four items)
Employees were asked to report on changes in procedures (i.e. reports of the shift changing from working in groups to functioning as teams). The items were: “I have changed routines and procedures after the implementation of teams,” “Through the implementation of teams we finally get to straighten up some bad methods/procedures, that we had acquired,” “In this change we openly discuss which traditions or procedures we wish to change and which we wish to keep,” and “The implementation of teams has made it easier to tackle the changes in the organization”. Responses to these items were given on a five-point scale ranging from 1 (strongly agree) to 5 (highly disagree). Cronbach's α = .75.
To enhance clarity in the interpretation and meaning of the results, scores on each scale were transformed so they ranged from 0–100 with 100 representing a high positive/healthy score on the construct. For scales with five response categories, responses were transformed such that 1 = 0, 2 = 25, 3 = 50, 4 = 75, 5 = 100. This transformation had no impact on the relationship between variables and thus does not influence the covariance matrix on which the analyses are based.
Data analysis
Our data were collected from teams, and therefore we considered using multi-level analysis to analyze the data, however, ANOVA and ICC(1) analyses indicated that multi-level analyses were not appropriate (Hox, 2002). Full details of these analyses are available upon request.
We computed standardized effect sizes (ESs) of the changes as Cohen's d, that is, the mean difference for all outcomes measures for each group from Time 1 (T1) to Time 2 (T2), divided by the average standard deviation from the two measures of each group separately (Dunlop, Cortina, Vaslow, & Burke, 1996). The ES thus reflects the degree of change in terms of standard deviation.
We tested our hypotheses in a pathway structural equation model (SEM) using pairwise deletion (LISREL 8.8, Jöreskog & Sörbom, 1999). The maximum likelihood method of parameter estimation was used with the covariance matrix as input. All scales were significantly correlated: this provided some initial justification for testing the mediating mechanisms using SEM.
To test Hypothesis 1 we included paths from reports of perceptions of changes in procedures T2 to social support, autonomy, well-being, and job satisfaction at T2. To test Hypothesis 2 we specified a path from employee participation reported at T2 to changes in procedures reported at T2. To test Hypothesis 3 we included paths from participation in intervention activities to social support, autonomy, affective wellbeing and job satisfaction at T2. To test the paths in Hypothesis 4 we included paths between T1 social support, autonomy, job satisfaction and well-being, and both participation and changes in procedures at T2. In addition, because many studies have shown that working conditions are associated with job satisfaction and affective well-being (e.g. de Lange, Taris, Kompier, Houtman, & Bongers, 2004) we also included paths from autonomy and social support (both at T2) to job satisfaction and affective well-being (also at T2).
As our hypotheses 1 and 3 were tested cross-sectionally we controlled for pre-intervention levels of the study variables by including paths from affective well-being T1 to affective well-being T2, from job satisfaction at T1 to job satisfaction at T2, and from social support at T1 to social support at T2, and from autonomy at T1 to autonomy at T2. Parameter estimates were used to detect non-significant paths that could be deleted. The acceptable levels of fit used to assess the adequacy of each model were according to the recommendations made by Anderson and Gerbing (1988). NNFI (non-normed fit index), AGFI (adjusted goodness of fit index), CFI (comparative fit index) should be above .90 and RMSEA (root-mean-square error of approximation) should be below .08 for a good fit and below .05 for an excellent fit of the model to the data.
Results
Table 1 shows the scales, means, standard deviations and intercorrelations of all variables in this study. Simple t-tests between T1 and T2 were used to identify any significant intervention effects across the sample as a whole. These revealed that autonomy (t(400) = −4.46, p <.001, ES = .45), and affective well-being (t (403) = −1.35, p <. 05, ES = .13) improved significantly whereas job satisfaction (t(352) = 2.15, p <.05, ES = .23) decreased significantly. No significant change was observed for social support (t(321) = 1.12, p >.05, ES = .06). These results showed that without considering within-intervention group variability in reports of participation and of theories-in-use it would have been reasonable to conclude that the intervention had mixed and modest effects. This would have made the impact of the intervention extremely difficult to interpret and left open the possibility that teamwork had either remained largely an espoused theory in this intervention process or a theory-in-use with disappointing outcomes.
Table 1.
Means, standard deviations and correlations.
| Scale | M (T1) | SD (T1) | M (T2) | SD (T2) | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Participation | 41.36 | 21.31 | .41** | .18* | .20** | .19* | .20** | |||
| 2. Changes in procedures | 45.92 | 16.92 | .10 | .20** | 23** | .22** | ||||
| 3. Social support | 76.71 | 19.98 | 75.43 | 19.36 | .43** | .20** | .22** | .15** | ||
| 4. Autonomy | 48.34 | 19.30 | 52.64 | 19.22 | 19** | .59** | .22** | .18** | ||
| 5. Job satisfaction | 66.76 | 16.17 | 64.91 | 15.68 | .35** | .15** | .38** | .36** | ||
| 6. Affective well-being | 66.47 | 17.21 | 67.63 | 15.76 | 23** | .21** | .33** | .52** |
Notes: Ns range from 129 to 400. Correlations below the diagonal are from Time 1 and above the diagonal from Time 2. Correlations on the diagonal are between Time 1 and Time 2. Changes in procedures and participation were only measured at Time 2.
p < .05;
p < .01.
Testing the study hypotheses
The hypothesized model presented an acceptable fit to the data. RMSEA was .06; NNFI (.92), CFI (.98) and AGFI (.94) indicated a good fit to the data, all above the level of .90. χ2 (12) = 40.97.
The final model is presented in Figure 1. Hypothesis 1 was partially supported: changes in procedures reported at T2 were positively related to autonomy at T2 (β = 12, p <.01), well-being T2 (β = .09, p <.05) and job satisfaction T2 (β = .14, p <.01). Testing Hypothesis 1 revealed that changes in procedures were significantly associated with post-teamwork implementation levels of autonomy, affective wellbeing, and job satisfaction. While participation at T2 was positively associated with social support at T2 (β = .09, p <.01), the paths from participation T2 to autonomy, well-being, and job satisfaction were non-significant. Hypothesis 2 was supported: having participated in the planning and implementation of teamwork predicted the degree to which employees experienced changes had been introduced at follow-up (β = .39, p <.001). Hypothesis 3 was only partially supported. Participation in the planning and implementation of change was linked to post-intervention social support. We found no significant relationships between the measure of participation and post-intervention autonomy, job satisfaction, and well-being.
Figure 1.
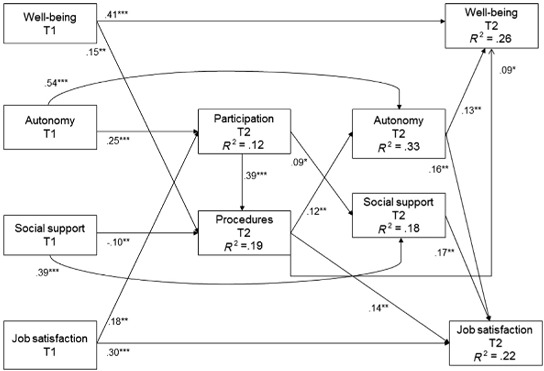
Model of the mediating role of participation and changes in procedures, with maximum likelihood estimates (standardized).
Note: * <.05, **p <.01, ***p <.001. Only significant paths are reported in this figure.
Hypothesis 4 was also partially supported. Autonomy and job satisfaction at T1 significantly predicted participation at T2 (β = .25, p <.001, β = .18, p <.01, respectively). Affective well-being and social support at T1 did not significantly predict participation at T2. Well-being levels prior to the interventions predicted changes in procedures at T2 (ß = .15, p <.01), however, this was not the case for autonomy and job satisfaction. Contrary to our expectations, the higher the level of social support that employees reported having before team implementation the fewer changes in procedures they reported having introduced (β = −10, p <.01). Finally, autonomy at T2 significantly predicted affective well-being and job satisfaction (T2) (β = .13, p <.01, β = .16, p < .01, respectively) but social support at T2 was only found to be related to job satisfaction at T2 (β = .17, p < .01), No significant relationship was found between social support (T2) and affective well-being (T2). In summary, we found that social support, autonomy and job satisfaction at baseline level predicted the degree to which employees reported changes in procedures and this was fully mediated by the degree to which employees reported that they had participated in the planning and implementation of teamwork (Hypothesis 4). Sobel's test (1982) for the mediated link between autonomy, participation and changes in procedures was significant, z = 4.67, p <.001, and the z value for the pathway between job satisfaction, participation and changes in procedures was also significant, z = 2.92, p <.001.
Discussion
In this study we presented the results of a natural intervention study implementing teams in the elder care sector. The main contribution of this paper is that it includes separate direct tests of how (1) the active participation of employees in the planning and implementation of teamwork; and (2) direct measures of perceived changes in procedures (i.e. theories-in-use) are significantly linked to intervention outcomes.
The results of testing our first hypothesis lend support to the argument that in order to be successful, participatory organizational changes must involve espoused theories becoming theories-in-use (Argyris, 1995, 2004). In intervention research, the degree to which planned changes have actually been implemented has not always been examined before conclusions have been reached about intervention effectiveness (Nielsen et al., 2006). When such data have been collected, links have been found between intervention outcomes and active participation in intervention activities (Nielsen et al., 2007). Our results indicate that measures should be included to confirm that changes have actually taken place and that such measures should capture perceptions of theories-in-use (the active ingredients) associated with the intervention.
In our study the changes in procedures associated with team implementation only explained variance in autonomy, affective well-being and job satisfaction but no significant relationship was found between changes in procedures and post-intervention social support. This result is in contrast to previous research that suggests introducing teamwork may increase social support (Rasmussen & Jeppesen, 2006). This finding may be specific to our sample, as employees already worked in groups prior to team implementation: the emphasis in the intervention was on transferring responsibilities to employees that had formerly been the responsibility of the supervisor.
Our findings led us to accept Hypothesis 2: this supports the notion that involving employees in change processes is important to ensure commitment to change and learning, thus bringing about a transition from espoused theory to theory-in-use. Our results are in line with those of Nielsen et al. (2007), who found that participation was linked to an uptake in intervention activities. Our results also indicated that both of the two mechanisms identified by Hurrell (2005) – i.e. participation would be directly linked to intervention outcomes as well as to changes in existing work procedures – were active in our study: participation in planning and implementing teamwork also showed a small direct link to post-intervention social support.
Our results do not support the part of Hypothesis 3 suggesting that the participatory approach brings about autonomy because employees are able to have their views heard and shape the design and implementation of changes. Our results showed that it was the measure of changes in procedures (i.e. evidence of double-loop learning) that was significantly related to autonomy. These results suggest that in the absence of theories-in-use (changes in procedures), participatory change processes do not necessarily bring about increases in autonomy. More research is needed to test the external validity of this finding.
The link between participation and job satisfaction found by Sverke et al. (2008) was not replicated in our study. One reason for this may be that Sverke and colleagues only examined participation in decision-making. In contrast our measure also included questions about whether employees had been actively involved in implementing change, which may have a different relationship with job satisfaction. Another explanation may be that job satisfaction lacks sensitivity as an outcome variable because it can be affected by many factors in the work context itself and not just the participatory nature of the intervention (Bond & Bunce, 2001). However, consistent with the work of Johnson et al. (2006), we did find a direct link between participation and affective well-being.
The partial support for Hypothesis 4 is consistent with Taris et al. (2003) who suggested that those in well-designed jobs may be more likely to get involved in the change process. Interestingly, we found no relationship between baseline levels of affective well-being and participation. It may be that affective individual-level wellbeing has little effect on the readiness of organizational systems and structures for participation in change. Our results suggest that it is primarily work-related features that encourage employees to participate in change processes: if employees feel little supported, do not feel that their opinions are valued at work and in general are dissatisfied with their work they may not feel responsible for, or feel encouraged to, engage in planning and implementing interventions.
On the other hand, our results indicated that baseline levels of affective wellbeing and social support significantly predicted whether employees’ reported actual changes had been made in procedures as a result of team implementation (also Hypothesis 4). This relationship was positive for affective well-being (i.e. those employees who reported a high level of affective well-being reported more changes in the way work had been carried out) and negative for social support (the more social support employees reported being at baseline the fewer changes they reported). A possible explanation may be that employees who reported a high level of affective well-being had higher levels of energy and thus made challenge appraisals rather than threat appraisals (Lazarus & Folkman, 1992) when presented with the opportunity for change. With regards to social support it is possible that a ceiling effect (Nielsen et al., 2006) was operating (see Table 1): that is, baseline social support was so high that it would be difficult to improve social support levels. Our results suggest that those who already felt supported by their colleagues may have felt little encouragement to change their existing working procedures. This result is inconsistent with COR theory, which suggests that individuals try to increase resources (Hobfoll, 1989). These complex patterns in our results indicate that much more work needs to be done in order to understand how pre-intervention working conditions and affective well-being influence intervention processes.
Finally, our results confirmed the important role that may be played by working conditions in determining intervention outcomes. Social support and autonomy post-intervention were significantly associated with job satisfaction and affective well-being post-intervention. These results are in accordance with previous studies suggesting that intermediate working conditions may be the explanation for why we see changes in employee health and well-being (Bond & Bunce, 2001; Nielsen et al., 2007).
Turning to a more general methodological issue, our results confirm the importance of integrating process measures when evaluating the effects of organizational interventions. By using SEM analysis including measures of intervention processes we found that within-group variability in participation and exposure to actual changes in procedures were linked to variability in intervention outcomes. In this study we tested mediation in order to test the validity of a hypothesized sequence of events; however, it is also possible that intervention processes act as moderators such that stronger effects would be found when employees participated in the process. Future studies should examine the moderating effects of implementation processes on intervention outcomes.
Implications for research and practice
Previous teamwork intervention research has often been based upon the assumption that the outcome of team implementation will usually be positive for both the organization and employees but has not included sufficient measures of the complex processes by which organizational change is brought about (Egan et al., 2009). Our study provides an example of how the internal validity of intervention research may be increased (Campbell & Stanley, 1963) by measuring the extent of double-loop learning. By including a test of whether the team intervention actually brought about perceptions of changes in procedures we were able to show the relationship between this working mechanism in the change process and intervention outcomes. In field studies it is often challenging to secure suitable control groups (Nielsen et al., 2006; Nielsen, Taris, & Cox, 2010). Including tests of whether changes have taken place may increase the internal validity of studies where it is only possible to track changes in an intervention group. Future research should focus on how this test can be used to link interventions to intervention outcomes using quasi-experimental designs that also include a control group.
In this study we used self-report measures of participation and changes in procedures. Subjective appraisals, however, play a crucial role in dominant theories (e.g. stress theory (Lazarus & Folkman, 1992); theory of planned behaviour (Ajzen, 1991) and mental models (Johnson-Laird, 2003)) and studies have found that individuals’ appraisal plays an important role in determining their health and wellbeing (Daniels, Boocock, Glover, Hartley, & Holland, 2009). Nevertheless, it may be worthwhile employing a mixed methods approach to include other sources of data about participation and changes in procedures (e.g. by using organizational material and observational studies). A longitudinal observational study may reveal verifiable evidence of changes in employee behaviour associated with theories-in-use. Interview methods may reveal more details about the various mechanisms through which participation impacts on outcome measures. In the present study this may have helped us to explain why participation was linked to social support but not autonomy as we had predicted. Future studies should examine the link between self-reported participation and observations of participation as suggested above.
The importance of measuring participation intervention activities directly is indicated by Hurrell (2005) who distinguished between two types of participatory interventions: psychosocial action research interventions (where employees work jointly with outside experts to define problems and develop intervention strategies to improve health and well-being) and job redesign interventions. While the former most often include a smaller number of employees participating in health circles, problem solving or steering groups (Nielsen, Randall, Holten, & Rial González, 2010), the latter involves all employees being affected by changes in job design. Hurrell (2005) concluded that interventions of the former type rarely bring about positive effects. It may be that the former results in only those individuals directly involved in the intervention acquiring learning, and thus the intended organizational learning does not materialize. Landsbergis and Vivona-Vaughan (1995) found evidence for this effect: most of the employees directly involved in planning and implementing intervention activities felt that the project had been moderately or very effective whereas most of the remaining intervention group felt the intervention had been only slightly or ineffective. Taken together with our results, this research highlights the importance of using measures of participation in an intervention to monitor the implementation process and ensure that the expertise of employees is used in order to increase the success of the intervention.
The evaluation of these change processes often uses qualitative methods, e.g. semi-structured interviews (Nielsen, Taris & Cox, 2010). Such an approach to evaluation requires many resources in terms of both the competencies of, and time used by, those conducting the evaluation (and therefore most such evaluations often require external help). It can also be very resource-intensive to allow managers and employees time to participate in interviews. Using a quantitative measure of change processes means that enhanced evaluation can be integrated in existing risk assessments and attitude surveys to provide an insight into how the intervention is progressing. It also provides data that can be used to identify and deal with the faulty implementation of interventions.
Strengths and limitations
The main strengths of this study are its relatively large sample size along with the integration of process evaluation (i.e. evaluation of participation and of the changes in procedures) into the outcome evaluation (Semmer, 2006). Controlling for pre-test levels on study variables helped to rule out many of the threats to internal validity (Cook & Campbell, 1979). There are, however, several limitations that should be considered when interpreting the results. First, we had no non-intervention group. This was not possible as the changes were implemented organization-wide. This is common in intervention situations (Nielsen et al., 2010b), partly because organizations seek to give as many employees as possible the chance to benefit from the intervention (Randall et al., 2007). However, the absence of a non-intervention group was not crucial to the testing of the study hypotheses. The use of process evaluation allowed us to capitalize upon variability in the intervention experience with greater rigour than is usually possible when there is no pre-determined control group.
Second, drop-out analyses indicated that employees who responded both times experienced higher job satisfaction and affective well-being. A healthy worker effect may have influenced our findings in that only healthy workers responded to the questionnaire both times. Less healthy employees may have left the organizations due to the potential increased demands associated with teamwork. This possibility should be tested in future intervention studies.
Third, this study was conducted in an elder care setting. This setting means that teamwork mostly occurred in terms of planning the job and helping each other (e.g. with problematic clients such as those with special physical or psychological needs). It is possible that our results cannot be transferred to other settings such as manufacturing (the setting for a great deal of teamwork research). Other team implementation research has focused on similar outcomes (Bambra et al., 2007) and we tentatively suggest that factors such as participation and changes in procedures may be universally important when conducting organizational interventions. Naturally these factors should be directly studied in other settings. Some of our specific results may be less generalizable, for example, the ceiling effects found for social support may not be generalizable across occupational groups. In other teamwork interventions where the shift is from individual working to teamworking, a certain level of pre-intervention social interaction between individual employees may be necessary to trigger engagement in the intervention. Future research should replicate our findings in studies where employees have not previously worked in groups.
Fourth, common method and common source bias may pose a threat to our results (Podsakoff, MacKenzie, Lee, & Podsakoff, 2003). We used several methods to minimize any impact of these biases. First, we ensured respondent confidentiality. Second, we counterbalanced questionnaire items such that it was not clear to the respondents which items belonged to which scales. Finally, we attempted to use questionnaire items that were clear, simple and specific to each of the constructs being measured. To help ensure that this was achieved, the questionnaire was piloted by a steering group of employee representatives and managers before distributing it at the elder care centres.
Finally, due to financial and organizational restrictions we were only able to include one follow-up. As a result, process issues and intervention outcomes were measured simultaneously; for obvious reasons it was not possible to measure process before it took place and we are therefore unable to draw any conclusions on causality. It is possible that those employees who have been heavily involved in the planning and implementation of the intervention are reluctant to admit that the intervention has no effect and therefore score higher on changes in procedures and outcomes or reversely, that employees who are disappointed in the lack of impact of the intervention downplay their own involvement in the intervention process. We do, however, believe this study adds to the existing knowledge on intervention implementation in that to the best of our knowledge no previous research has tested, quantitatively measured and analyzed participation in intervention planning and implementation or in employees’ perceived changes in procedures (that is, tested the working mechanisms of an intervention). Future research should include at least three measurement points to measure process measures independently of intervention outcomes. However, one of these would need to be carried out very close in time to the outcome evaluation in order to allow employees to comment on their experience of the whole of the intervention.
Conclusions
This study offers new knowledge in three areas. First, it provides direct evidence of the validity of the mechanisms that link employee involvement in the planning and implementation of organizational change interventions to intervention outcomes. We found that employee participation, while important, needs to be accompanied by perceptions of actual changes in daily work practices if important outcomes such as increases in autonomy and job satisfaction are to occur. Our results also highlight the importance of testing how social support, autonomy, job satisfaction and well-being may be differently affected by different aspects of the change process. Second, it appears that the pre-intervention situation (organizational maturity) influences employees’ experiences of the intervention process (both the degree to which they participate, and also their reports that actual changes have been implemented). Finally, we used two quantitative measures of participation in the intervention process and changes in procedures: these were found to explain some of the variance in post-intervention working conditions, job satisfaction and affective well-being. Using quantitative process evaluation may offer a cost-effective solution to manage and monitor intervention processes and may be integrated in existing risk assessments and attitude surveys.
Acknowledgements
This research was funded by the National Work Environment Research Fund, grant 16-2004-09. The authors would like to thank data manager, Isabella Gomes Carneiro, for preparing data for analysis.
References
- Ajzen I. The theory of planned behavior. Organizational Behavior and Human Decision Processes. 1991;50:179–211. [Google Scholar]
- Anderson J.C., Gerbing D.W. Structural equation modelling in practice: A review and recommended two-step approach. Psychological Bulletin. 1988;103:411–423. [Google Scholar]
- Argyris C. Action science and organizational learning. Journal of Managerial Psychology. 1995;10:20–26. [Google Scholar]
- Argyris C. Double-loop learning and implementable validity. In: Tsoukas H., Mylonopoulos N., editors. Organizations as knowledge systems: Knowledge, learning and dynamic capabilities. Basingstoke: Palgrave Macmillan; 2004. pp. 29–45. [Google Scholar]
- Bakker A.B., Demerouti E. The job demands-resources model: State of the art. Journal of Managerial Psychology. 2007;22:309–328. [Google Scholar]
- Bambra C., Egan M., Thomas S., Petticrew M., Whitehead M. The psychosocial and health effects of workplace reorganisation. 2. A systemic review of task restructuring interventions. Journal of Epidemiology & Community Health. 2007;61:1028–1037. doi: 10.1136/jech.2006.054999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bech P., Olsen L.R., Kjoller M., Rasmussen N.K. Measuring well-being rather than the absence of distress symptoms: A comparison of the SF-36 Mental Health subscale and the WHO-five Well-being Scale. International Journal of Methods in Psychiatric Research. 2003;12:85–91. doi: 10.1002/mpr.145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bond F., Bunce D. Job control mediates change in a work reorganization intervention for stress reduction. Journal of Occupational Health Psychology. 2001;6:290–302. [PubMed] [Google Scholar]
- British Psychological Society. Code of ethics and conduct. Leicester: British Psychological Society; 2006. [Google Scholar]
- Campbell D.T., Stanley J.C. Experimental and quasi-experimental design for research. Skokie, IL: Rand McNally; 1963. [Google Scholar]
- Cohen S., Bailey D. What makes teams work: Group effectiveness research from the shop floor to the executive suite. Journal of Management. 1997;23:239–290. [Google Scholar]
- Cole M.S., Schaninger W.S., Harris S.G. The workplace social exchange network: A multilevel, conceptual examination. Group & Organization Management. 2002;27:142–167. [Google Scholar]
- Cook T.R., Campbell D.T. Quasi-experimentation: Design and analysis issues for the field settings. Chicago, IL: Rand McNally; 1979. [Google Scholar]
- Daltuva J.A., King K.R., Williams M.K., Robins T.G. Building a strong foundation for occupational health and safety: Action research in the workplace. American Journal of Industrial Medicine. 2009;52:614–624. doi: 10.1002/ajim.20711. [DOI] [PubMed] [Google Scholar]
- Daniels K., Boocock G., Glover J., Hartley R., Holland J. An experience sampling study of learning, affect, and the demands control support model. Journal of Applied Psychology. 2009;94:1003–1017. doi: 10.1037/a0015517. [DOI] [PubMed] [Google Scholar]
- Day D.V., Gronn P., Salas E. Leadership in team-based organizations: On the threshold of a new era. The Leadership Quarterly. 2006;17:211–216. [Google Scholar]
- De Dreu C.K.W., West M.A. Minority dissent and team innovation. The importance of participation in decision making. Journal of Applied Psychology. 2001;86:1191–1201. doi: 10.1037/0021-9010.86.6.1191. [DOI] [PubMed] [Google Scholar]
- de Lange A.H., Taris T.W., Kompier M.A.J., Houtman I.L.D., Bongers P.M. The relationships between work characteristics and mental health. Examining normal, reversed and reciprocal relationships in a 4-wave study. Work & Stress. 2004;18:149–166. [Google Scholar]
- Dunlop W.P., Cortina J.M., Vaslow J.B., Burke M.J. Meta-analysis of experiments with matched groups or repeated measures design. Psychological Methods. 1996;1:170–177. [Google Scholar]
- Egan M., Bambra C., Petticrew M., Whitehead M. Reviewing evidence on complex social interventions: appraising implementation in systemic reviews of the health effects of organisational-level workplace interventions. Journal of Epidemiology & Community Health. 2009;63:4–11. doi: 10.1136/jech.2007.071233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guth W.D., Macmillan I.C. Strategy implementation versus middle manager self-interest. Strategic Management Journal. 1986;7:313–327. [Google Scholar]
- Hobfoll S.E. Conservation of resources: A new attempt at conceptualizing stress. American Psychologist. 1989;44:513–524. doi: 10.1037//0003-066x.44.3.513. [DOI] [PubMed] [Google Scholar]
- Hox J.J. Multilevel analysis: Techniques and applications. Mahwah, NJ: Erlbaum; 2002. [Google Scholar]
- Hurrell J. Organizational stress intervention. In: Barling J., Kelloway E.K., Frone M.R., editors. Handbook of work stress. Thousand Oaks, CA: Sage; 2005. pp. 623–645. [Google Scholar]
- Johnson M.E., Brems C., Mills M.E., Neal D.B., Houlihan J.L. Moderating effects of control on the relationship between stress and change. Administration and Policy in Mental Health Services Research. 2006;33:499–503. doi: 10.1007/s10488-005-0002-6. [DOI] [PubMed] [Google Scholar]
- Johnson-Laird P.N. Mental models and reasoning. In: Leighton J.P., Sternberg R.J., editors. The nature of reasoning. Cambridge: Cambridge University Press; 2003. pp. 169–204. [Google Scholar]
- Jöreskog K.G., Sörbom D. LISREL 8.3: Structural equation modelling with the SIMPLIS command language. London: Lawrence Erlbaum; 1999. [Google Scholar]
- Karasek R.A. An analysis of 19 international case studies of stress prevention through work reorganization using the demand/control model. Bulletin of Science, Technology & Society. 2004;24:446–456. [Google Scholar]
- Karasek R.A., Theorell T. Healthy work: Stress, productivity and the reconstruction of working life. New York, NY: Basic Books; 1990. [Google Scholar]
- Kompier M., Geurts S., Grundemann R., Vink P., Smulders P. Cases in stress prevention: The success of a participative and stepwise approach. Stress Medicine. 1998;14:155–168. [Google Scholar]
- Kristensen T., Hannerz H., Høgh A., Borg V. The Copenhagen Psychosocial questionnaire (COPSOQ) A tool for the assessment and improvement of the psychosocial work environment. Scandinavian Journal of Work and Environmental Health. 2005;31:438–449. doi: 10.5271/sjweh.948. [DOI] [PubMed] [Google Scholar]
- Landsbergis P., Vivona-Vaughan E. Evaluation of an occupational stress intervention in a public agency. Journal of Organizational Behavior. 1995;16:29–48. [Google Scholar]
- Lazarus R., Folkman S. Stress, appraisal and coping. New York, NY: Springer Publications; 1992. [Google Scholar]
- Lines R. Influence of participation in strategy change: Resistance, organizational commitment and change goal achievement. Journal of Change Management. 2004;4:193–215. [Google Scholar]
- Lyubormirsky S., King L., Diener E. The benefits of frequent positive affect: Does happiness lead to success? Psychological Bulletin. 2005;131:803–855. doi: 10.1037/0033-2909.131.6.803. [DOI] [PubMed] [Google Scholar]
- Michie S., West M.A. Managing people and performance: An evidence based framework applied to health service organizations. International Journal of Management Reviews. 2004;5/6:91–111. [Google Scholar]
- Mikkelsen A. Methodological challenges in the study of organizational interventions in flexible organizations. In: Fuglseth A.M., Kleppe I.A., editors. Anthology for Kjell Grønhaug in celebration of his 70th birthday. Bergen, Norway: Fagbokforlaget; 2005. pp. 151–178. [Google Scholar]
- Nielsen K., Fredslund H., Christensen K.B., Albertsen K. Success or failure? Interpreting and understanding the impact of interventions in four similar worksites. Work & Stress. 2006;20:272–287. [Google Scholar]
- Nielsen K., Randall R. Managers’ active support when implementing teams: The impact on employee well-being. Applied Psychology: Health and Well-being. 2009;1:374–390. [Google Scholar]
- Nielsen K., Randall R., Albertsen K. Participants’ appraisals of process issues and the effects of stress management interventions. Journal of Organizational Behavior. 2007;28:793–810. [Google Scholar]
- Nielsen K., Randall R., Holten A.L., Rial González E. Conducting organizational-level occupational health interventions: What works? Work & Stress. 2010;24:234–259. [Google Scholar]
- Nielsen K., Taris T.W., Cox T. The future of organizational interventions: Addressing the challenges of today's organizations. Work & Stress. 2010;24:219–233. [Google Scholar]
- Parker S., Williams H. Effective teamworking: Reducing the psychosocial risks. Norwich: HSE Books; 2001. [Google Scholar]
- Podsakoff P.M., MacKenzie S.B., Lee J.Y., Podsakoff N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. Journal of Applied Psychology. 2003;88:879–903. doi: 10.1037/0021-9010.88.5.879. [DOI] [PubMed] [Google Scholar]
- Randall R., Cox T., Griffiths A. Participants’ accounts of a stress management intervention. Human Relations. 2007;60:1181–1209. [Google Scholar]
- Randall R., Nielsen K., Tvedt S.D. The development of scales to measure participants’ appraisals of organizational-level stress management interventions. Work & Stress. 2009;23:1–23. [Google Scholar]
- Rasmussen T.H., Jeppesen H.J. Teamwork and associated psychological factors: A review. Work & Stress. 2006;20:105–128. [Google Scholar]
- Rosskam E. Using participatory action research methodology to improve worker health. In: Schnall P., Dobson M., Rosskam E., editors. Unhealthy work: Causes, consequences, cures. New York, NY: Baywood Publishing Company; 2009. pp. 211–229. [Google Scholar]
- Seaverson E.L.D., Grossmeier J., Miller T.M., Anderson D.R. The role of incentive design, incentive value, communications strategy, and worksite culture on health risk assessment participation. Quantitative Research: Financial Analysis. 2009;23:343–352. doi: 10.4278/ajhp.08041134. [DOI] [PubMed] [Google Scholar]
- Semmer N.K. Job stress interventions and the organization of work. Scandinavian Journal of Work and Environmental Health. 2006;32:515–527. doi: 10.5271/sjweh.1056. [DOI] [PubMed] [Google Scholar]
- Sims D.E., Salas E. When teams fail in organizations. What creates teamwork breakdowns? In: Langan-Fox J., Cooper C.L., Klimoski R.J., editors. Research companion to the dysfunctional workplace. Northhampton, MA: Edward Elgar; 2007. pp. 302–318. [Google Scholar]
- Sobel M.E. Direct and indirect effects in linear structural equation models. In: Long J.S., editor. Common problems/proper solutions. Beverly Hills, CA: Sage; 1982. pp. 46–64. [Google Scholar]
- Sverke M., Hellgren J., Näswall K., Göransson S., Öhrming J. Employee participation in organizational change: Investigating the effects of proactive vs. reactive implementation of downsizing in Swedish hospitals. Zeitschrift für Personalforschung. 2008;22:111–129. [Google Scholar]
- Taris T.W., Kompier M., Geurts S., Schreurs P., Schaufeli P., De Boer E., Sepmeijer K., Wattez C. Stress management interventions in the Dutch domiciliary care sector: Findings from 81 organisations. International Journal of Stress Management. 2003;10:297–325. [Google Scholar]
- Taris T.W., Schreurs P.J.G. Well-being and organizational performance: An organizational-level test of the happy-productive worker hypothesis. Work & Stress. 2009;23:120–136. [Google Scholar]
- Tsutsumi A., Nagami M., Yoshikawa T., Nogi K., Kawakami N. Participatory intervention for workplace improvements on mental health and job performance among blue-collar workers: A cluster randomized controlled trial. Journal of Occupational and Environmental Medicine. 2009;51:554–563. doi: 10.1097/JOM.0b013e3181a24d28. [DOI] [PubMed] [Google Scholar]
- van Horn J.E., Taris T.W., Schaufeli W.B., Schreurs P.C. The structure of occupational well-being: A study among Dutch teachers. Journal of Occupational and Organizational Psychology. 2004;77:365–375. [Google Scholar]
- van Mierlo H., Rutte C., Kompier M., Dooreward H. Self-managing teamwork and psychological well-being: Review of a multilevel research domain. Group & Organization Management. 2005;30:211–235. [Google Scholar]