

Abstract
PURPOSE
To compare the changes in the occlusal vertical dimension, activity of masseter muscles and biting force after insertion of immediate denture constructed with conventional, tooth-supported and Implant-supported immediate mandibular complete denture.
MATERIALS AND METHODS
Patients were selected and treatment was carried out with all the three different concepts i.e, immediate denture constructed with conventional (Group A), tooth-supported (Group B) and Implant-supported (Group C) immediate mandibular complete dentures. Parameters of evaluation and comparison were occlusal vertical dimension measured by radiograph (at three different time intervals), Masseter muscle electromyographic (EMG) measurement by EMG analysis (at three different positions of jaws) and bite force measured by force transducer (at two different time intervals). The obtained data were statistically analyzed by using ANOVA-F test at 5% level of significance. If the F test was significant, Least Significant Difference test was performed to test further significant differences between variables.
RESULTS
Comparison between mean differences in occlusal vertical dimension for tested groups showed that it was only statistically significant at 1 year after immediate dentures insertion. Comparison between mean differences in wavelet packet coefficients of the electromyographic signals of masseter muscles for tested groups was not significant at rest position, but significant at initial contact position and maximum voluntary clench position. Comparison between mean differences in maximum biting force for tested groups was not statistically significant at 5% level of significance.
CONCLUSION
Immediate complete overdentures whether tooth or implant supported prosthesis is recommended than totally mucosal supported prosthesis.
Keywords: Immediate denture, Implant-supported denture, Electromyography, Bite force
INTRODUCTION
Edentulous patients with complete dentures are generally satisfied but up to 30% of the patients have complaints.1 They suffer from a variety of problems with their dentures, especially with regard to the lower denture, such as insufficient stability, retention and pain during mastication.With time, the resulting pain and difficulty may increase during oral functions to an extent that proper nutritional intake and the patients' ability to communicate with ease and confidence are jeopardized. Psychosocial problems are the result of diminished attractive facial appearance, difficulties with speech and avoidance of social contacts.2
Immediate dentures are dental prostheses constructed for insertion immediately following the extraction of the natural teeth and the attendant surgical procedures. Reviewing through the literatures3-6 has indicated that immediate denture service has several advantages as the natural facial expression and appearance is maintained because the facial muscles are maintained in their correct position and the patient never appears edentulous. Facial height is retained as the facial muscles will function at their natural length, neutral zone is maintained because the artificial teeth are arranged in a similar manner to their natural predecessors. Mastication is easy or even better than after a period of edentulousness without dentures and minimal speech impairment as there is minimal loss of masticatory efficiency because patient is not without teeth anytime. Other advantages of immediate dentures are that the occlusal vertical dimension can be accurately determined and that the remaining natural teeth aid in recording centric relation. The immediate insertion of dentures may also control hemorrhage, aid tissue healing, and contribute to the patient's comfort following surgery. However, rapid resorption of the alveolar ridge which often occurs following tooth extraction is considered as a disadvantage in immediate denture service.
For many years, traditional complete denture designs have been modified to gain additional support and stability from a few retained and suitably prepared natural teeth. Mericske-Stern et al.7 attested to the effectiveness of such tooth-supported complete dentures or overdentures as alternative to complete dentures. Roots maintained under the denture base preserves the alveolar ridge, provide sensory feedback and improve the stability of the dentures.
Recently, Morais et al.8 reported that overdenture treatment with the use of implants has become popular for edentulous elderly patients who are maladaptive to complete dentures. Although the biologic basis of implants installed in the bone is different from roots surrounded by a periodontal membrane, but the prosthetic concept is similar. Tactile sensation for implant is reduced because of the absence of periodontal receptors. However, oral function with overdentures supported by roots or implants is comparable and does not seem to depend on the presence of a periodontal membrane. They are a preferable alternative to treatment with conventional complete denture, the main advantages are decreased resorption of the residual ridges; psychological benefits for the patients and maintenance of masticatory efficiency.9
Reviewing of the literature had demonstrated a higher tendency for success when overdentures are supported by implants than by roots. This is particularly true for mandibular overdentures whereas for maxillary implants, more frequent failures are observed with low bone quality and short implants.7 Dental implants present several advantages over questionable teeth. From a restorative perspective, dental implants are made of materials with known physical properties that can provide standardized structural durability as abutments, also dental implants are not subjected to caries and may be used successfully even in caries-prone individuals.10
According to the previously cited merits with immediate denture, the question remained unanswered to what extent, provision of tooth and implant-supported mandibular overdentures would beneficially aid to edentulous patient in maintaining his or her masticatory force and occlusal vertical dimension rather than rendering him or her completely edentulous. This question warranted us to plan this study to evaluate to what extent immediate tooth and implant-supported overdentures would aid beneficially to preserve occlusal vertical dimension, biting force and maintain masticatory muscle activity. Parameters of evaluation and comparison were occlusal vertical dimension changes measured by radiograph, masseter muscle electromyographic changes measured by EMG analysis and maximum bite force changes measured by force transducer.
MATERIALS AND METHODS
Fifteen patients were selected from the out patient clinic, Faculty of Dentistry, Mansoura University. Their age were ranging from 45 to 55 years, with the mean age of 53 years. Patients were selected according to the following criteria; no signs and symptoms of TMJ dysfunction, no systemic disease which may affect the muscles, ligaments or bone, no history of prosthesis wearing and Angle's class I maxillo-mandibular relation. They had at least second premolars on each side acting as a bilateral occlusal vertical stoppers, sufficient to maintain vertical dimension of occlusion. Remaining teeth were present with unfavorable conditions needed to be subsequently extracted. All patients had approved to participate in this study and strongly motivated to retain their remaining canines.
The fabrication of immediate mandibular dentures was started by construction of a transitional distal extension acrylic partial dentures for lower jaws and complete dentures for upper jaws. Surgical preparation of the remaining natural teeth was done and all were extracted leaving the mandibular anteriors and a bilateral centric occlusal stopper on both jaws (second premolars). After a healing period, the impression procedures for construction of a maxillary complete denture opposing to a transitional mandibular bilateral distal extension acrylic removable partial denture were done in a conventional way.
Jaw relation records were judged by the contact of the remaining natural teeth which indicated occlusal vertical dimension and casts were mounted on the semi-adjustable articulator according to it. Shape, shade and form of the extracted and the remaining natural teeth were used as a guide to select the acrylic denture teeth. For freeing of occlusion, posterior teeth with thirty degrees of cuspal incline were used for maxillary denture and cuspless teeth were used for mandibular denture. Anterior teeth arrangement with zero overbite and two millimeter overjet was done. Selection and setting of posterior teeth were done according to procedure described by Passamonti et al.11 with main objective to reduce occlusal interference. Trial dentures were tested in the patient's mouth. The remaining natural premolars were trimmed off from the casts and replaced with the acrylic to complete the arrangement of the posterior teeth. A simple circlet stainless steel wrought wire clasp was adapted on each retained mandibular canines for gingivally approaching undercuts. Acrylic partial denture was planned on the remaining anterior teeth. Steps for denture completion were done including flasking, acrylic resin packing and curing, deflasking, finishing and polishing.
Prior to delievery of denture, laboratory remount was done to eliminate minor occlusal error resulting from acrylic resin processing. The remaining premolars were extracted with a minimal trauma. Bony spicules and sharp edges were carefully removed. Insertion of the dentures was done while the patients were under local anesthesia. The dentures were tested to ensure that, there were no sharp ridges or acrylic pearls on the impression surface of the denture. After appropriate infection control, the lower removable partial denture was placed in the mouth and assessed so that no overextensions were present along the periphery of the denture. Gentle pressure was applied on the occlusal surfaces of the lower premolar teeth to ensure that no stability problems were evident at this stage. Similarly, the upper denture was inserted and tested.
Occlusal relationships were confirmed and initial spot grinding was done to remove any occlusal prematurities. Patients were instructed about denture hygiene, mucosal tissue rest and denture manipulation. They were motivated for maintenance of good oral hygiene. Period of 45 days was permitted for patient adaptation to their prosthesis and any prosthesis correction and adjustment needed were done.
Grouping of the selected patients according to the study design was done and the patients were randomly classified into three equal groups as follows:
Group A: 5 patients who will be receiving conventional acrylic immediate complete mandibular denture (mucosal-supported).
Group B: 5 patients who will be receiving acrylic immediate complete mandibular denture supported by reduced root canal treated canines (tooth-supported).
Group C: 5 patients who will be receiving acrylic immediate complete mandibular denture supported by osseointegrated fixtures in the canines region (implant-supported).
In Group A, addition of the anterior teeth to the mandibular partial dentures was done in the conventional way, stored in a germicidal solution and inserted just after extraction of the lower anteriors. The patient was instructed to take care and not to remove the denture during the first 48 hours. Following that evaluation of the denture and the supporting tissues was done. Any ulceration from denture pressure or overextension of the base was relieved. The patients were instructed to clean the denture several times a day and utilize warm saline rinses and keep the denture in at night for five days.
In Group B, the procedures were followed according to Schwartz and Morrow.12 The mandibular canines were prepared on the cast to approximate the preparation that will be done intra orally and the remaining teeth were trimmed away in the usual manner. Abutment area in the finished denture fitting surface was relieved using a suitable acrylic finishing stone. Before surgical procedure, the retained mandibular canines were root canal treated, shortened to a level 2 - 3 mm in a dome shape and sealed occlusally with amalgam filling. Adaptation of the mandibular overdenture to the patient abutment was done after complete healing of the surgical site and suture removal. Caries protective varnish (Fluor Protector, Ivoclar Vivadent, Lichtenstein, Germany) was applied for two minutes weekly, for two weeks. For complete protection from caries, construction of a casted dome shaped dowel coping were done and inserted above the prepared mandibular canines abutment after two weeks. Readaptation of the mandibular overdenture was done.
In Group C, extraction of mandibular canines and immediate placement of an implant in the extraction site was discussed with each patient as an alternative for total extraction of their teeth and insertion of conventional denture. The implant surgical procedure in this study was followed according to Palmer et al.13 The surgical protocol for immediate dental implant placement into fresh extraction socket with two part dental implant system was followed according to el Charkawi's14 procedure as follows; atraumatic extraction of the canines was achieved with extraction forceps and every effort was made to preserve labial cortical plate, avoiding gingival laceration and canine fracture.
Uncoated titanium screw shaped implant (Impladrill Titanium Dental Implant System, Basel, Swiss) 3.8×13 mm were used for placement in extracted canine sites. After completion of the surgical procedures, the removable partial denture was seated in its place and tested for adequate relief above the implant sites. Once the surgical sutures were removed, intra oral adaptation and close fitness of the mandibular partial denture above the implant sites was achieved using a cold cure soft liner. Following this patients were seen frequently in the first 3 months, the proper oral hygiene was followed-up for all the patients.
The implant suprastructure used was modified to resemble dome shape, which provided abutment denture point of contact that permited mandibular overdenture free movement. After insertion of the abutments, extraction of the remaining incisors and insertion of the mandibular complete overdenture was done and post insertion care was taken. After the surgical sutures were removed, adaptation of the mandibular overdenture to the patient abutment with tooth shade autopolymerizing acrylic resin was done.
For determination of changes in occlusal vertical dimension for patients in all groups; lateral cephalometric radiographs were taken to detect occlusal vertical dimensional changes. Radiographic exposures were made at four occasions:
Before dental extraction with only bilateral upper and lower second premolars maintaining centric occlusion, vertical and horizontal relation.
Two weeks after transitional removable partial denture insertion (Time 1).
Two weeks after complete immediate mandibular denture insertion (Time 2).
One year after immediate denture insertion (Time 3).
Tracings of lateral cephalometric radiographs were done and the reference points, lines and measurements used for determination of occlusal vertical dimension were made according to the procedure described by Lambadakis and Karkazis.15 Reference lines marked were palatal plane, anterior cranial base, mandibular plane and d (line). d line was considered as a measure of vertical dimension of occlusion (Fig. 1). Comparison between mean variance of occlusal vertical dimension between observation times was statistically analyzed at 5% level of significance.
Fig. 1.
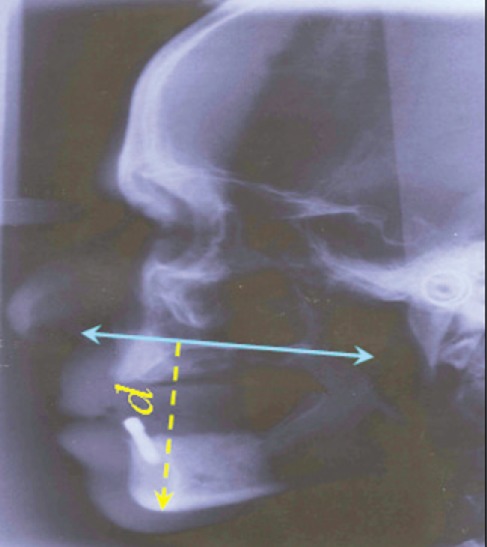
Lateral cephalometric x-ray with drawing of d line, as a reference measure for vertical dimension of occlusion.
Masseter muscle electromyographic activity measurements were recorded and processed digitally in the Medical Electronics Laboratory, Faculty of Engineering, Mansoura University using the BIOPAK system (MP100 WS BIOPAC Systems, BIOPAC Systems Inc., Santa Barbara, USA) connected to an electromyographic nodule. BIOPAK electromyographic device with a band pass of 25 to 1500 Hz = 3 dB and noise level < 0.05 Mv were used to record the EMG from the bilateral masseter muscles for 30 seconds. The surface electromyographic activities were made while the patient was sitting upright on a chair, head unsupported relaxed and looking straight. Bipolar surface electrodes were used for masseter muscle activity recording after scrubbing the superficial skin with alcoholic ether. The electrodes were circular with a diameter of 10 mm and a fixed inter electrode distance of about 10 mm was maintained to avoid pick-up of non specific facial muscle activity. To position the electrodes in the proper location according to Saifuddin et al.,16 one line was drawn from the inferior border of the tragus of the ear to the angle of the mouth. The masseter muscle width was measured by palpation and half of the width of the muscle was marked with an ink spot on that line. Electrodes were placed on both sides of the line around the ink spot and parallel to the main direction of the masseter muscle fibers. A common ground electrode was attached to the forehead of the patient. The electromyographic activity of the masseter muscle was recorded bilaterally during rest position (RP), initial contact position (IC) and maximum voluntary clench (MVC) after one year from immediate denture insertion.
EMG data were recorded with a sampling frequency 2 KHz for a time interval of 10 seconds. The recorded data were stored for further analysis. The EMG recorded data were transmitted to a personal computer and processed using MATLAB 7.0.1 (Release 14SP1, The MathWorks, Inc., Natick, USA) computer program. Wavelet packet coefficients values were computed for the masseter muscles (Right & Left) during RP, IC and MVC for each patient of the three groups and statistically analyzed by using ANOVA-F test at 5% level of significant. If the F test was significant, Least Significant Difference (LSD) test was performed to test further significant differences between the variables.
Bite force strength of each patient was measured using bite force transducer. Force transducers employed beam deflection and this deflection was sensed by a strain gauge which converts forces into measurable electrical signals. Bite force transducer consisted of force transducer and bite fork. Force transducer was composed of elastic load-bearing element for load application, strain gauge, for induced strain recording in terms of millivoltage and elastic load-bearing element. The elastic load-bearing element was constructed according to concept developed originally by Slagter et al.17 and van Kampen et al.,18 but with some modifications to suite this study as follows: casted dumbbell shaped bearing element with chrome cobalt was constructed as compared to hollow one to prevent the permanent deformation. Hard stainless steel coil was incorporated to the inner site of elastic element and a side cut with 2 mm space was made along one ring of the dumbbell to make it more flexible without permanent deformation during loading (Fig. 2).
Fig. 2.
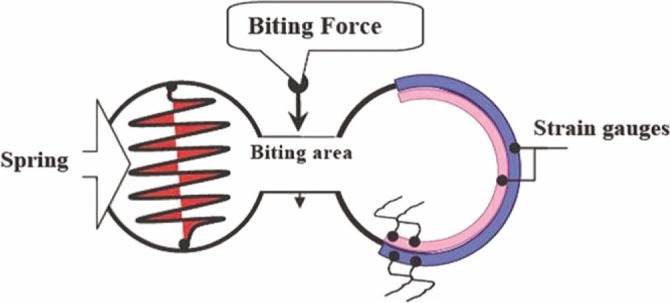
Cross section diagram of the elastic load bearing element and mounted strain gauges.
Strain gauge was used for recording strain induced on the elastic bearing element in term of millivoltage. The Kyowa (Strain gauge, Kyowa Electronic Instruments Com. Ltd. Tokyo, Japan) type strain gauge was used with the following criteria; Gauge 2.13 ± 105%, Resistance 119.6 ± 0.3, Length 10 mm, Thermal output µЄ/℃ ± 1.8 and Gauge cement Ep-IЄ. Strain gauge attachment to the elastic bearing element was done. The force transducer unit was attached to a side of specially constructed bite fork. The other side of the fork was attached to a polyethylene elastic tube, for the stabilization of the dentures during maximum biting force measurement. The mouth pieces (force transducer and stabilizing unit) were covered with an elastic rubber fingers which were changed for every patient, every time the measurement was done.
Measurement of voltage changes in the circuit with mV was done using Radioshack Digital Multimeter with a computer program 22-812 Meter View version 1.0 compatible with Windows XP. The differences between unloaded force transducer record and maximum loaded force transducer record were calculated as mV value of the maximum biting force. A simple method of calibration of bite force transducer was used according to Prombonas et al.19 to assort it by different applied load. Calibration was done in the Agriculture Engineering Laboratory, Faculty of Agriculture, Mansoura University using a testing machine (FGN - 50 Digital - LCD force testing machine, Lloyd Instruments™, AMETEK, Inc., West Sussex, UK) to apply loads of 1, 2, 4, 6, 8, 10, 12, and 14 kilograms.
The transducer output was varied linearly with the force, therefore calibration was done experimentally using weights of known mass. For calibration purpose, complete maxillary and mandibular finished dentures were mounted on a simple hinge articulator to simulate the oral condition during biting. All loads were applied through a bar mounted in contact with the central point present in the upper part of the articulator during loading. The mV measurements were converted to kilogram (kg) according to the following equation: Bite Force (kg) = mV×1.074 where 1.074 = constant factor from calibration curve.
The bite force transducer was positioned between the occlusal surfaces in the first molar region. The reproducible bite position for all measurements were obtained by insertion of the pin like projection which was present in the elastic element in a hole formed at the central fossa of the occlusal surface of the first molar of the denture. Patient was encouraged to bite as hard as possible on the bite-force transducer for a few seconds. The measurements were performed three times and the highest bite force of the three efforts was selected as a valid record. The procedure was repeated with the transducer placed on the contralateral side for recording of bite force. Right (R) and left (L) maximum biting force values were summed and the main value was calculated. The measurements were done for all groups one month after prosthesis preparation and twelve months after insertion of immediate dentures for all groups.
Data were collected from all the different groups and were subjected to statistical analysis via ANOVA-F test at 5% level of significance. If the F test was significant, LSD test was performed to test further significant differences between variables.
RESULTS
Comparison between mean differences in occlusal vertical dimension for tested groups at Time 1 and Time 2 was not statistically significant while at Time 3 it was statistically significant at 5% level of significance (Table 1 and Fig. 3)
Table 1.
Comparison between the mean differences in occlusal vertical dimension changes measured in millimeter for patients with immediate mandibular complete dentures, mucosal (Group A), tooth (Group B) and implant (Group C) supported overdentures

Fig. 3.

Comparison between the mean differences in occlusal vertical dimension changes measured in mm for groups after insertion of transitional mandibular RPD (Time 1), after insertion of immediate mandibular dentures (Time 2) and after one year of immediate mandibular dentures insertion (Time 3).
The mean occlusal vertical dimension changes in Group B were -0.34 ± 0.0894 in time 1, -0.74 ± 0.2074 in time 2 and -1.38 ± 1304 in time 3, in Group C were -0.36 ± 0.1140 in time 1, -0.76 ± .2075 in time 2 and -2.00 ± 0.2646 in time 3. Comparison between mean differences in occlusal vertical dimension for tested times were statistically significant at 5% level of significance.
Comparison between mean differences for tested sides was not statistically significant difference at 5% level of significance (Table 2, Figs 4 and 5).
Table 2.
Comparison between the mean difference of wavelet packet coefficients of the electromyographic signals of masseter muscles for patients with immediate mandibular complete dentures, mucosal (Group A), tooth (Group B) and implant (Group C) supported overdentures during rest position, initial teeth contact position and maximum voluntary clench

Fig. 4.

Comparison between the mean difference of wavelet packet coefficients of the electromyographic signals of masseter muscles for patients with immediate mandibular complete dentures, mucosal (Group A), tooth (Group B) and implant (Group C) supported overdentures during rest (R), initial teeth contact (IC) and maximum voluntary clench (MVC).
Fig. 5.

Superimposed EMG signals during rest position (R), initial contact (IC) positions and maximum voluntary clench (MVC) of immediate mandibular complete denture in Group A, Group B and Group C.
Comparison between mean differences in wavelet packet coefficients of the electromyographic signals of masseter muscles for tested groups was not statistically significant at 5% level of significance during rest position while it was statistically significant at 5% level of significance during initial teeth contact position and maximum voluntary clench position.
The mean maximum biting force before insertion of immediate mandibular dentures was 10.21 ± 1.05 in Group A, 9.97 ± 0.89 in Group B and 10.02 ± 0.72 in Group C. Comparison between mean differences in maximum biting force for tested groups was not statistically significant at 5% level of significance (Table 3 and Fig. 6).
Table 3.
Comparison between the mean differences in maximum biting force measured in kg. for patients with immediate mandibular complete dentures in Group A, Group B and Group C

Fig. 6.

Comparison between the mean differences in maximum biting force measured in kg. for patients with immediate mandibular complete dentures groups, before insertion and after insertion of immediate mandibular dentures.
The mean maximum biting force after 12 months from insertion of immediate mandibular dentures was 9.56 ± 0.99 in Group A, 13.48 ± 1.85 in Group B and 17.87 ± 1.67 in Group C. Comparison between mean differences in maximum biting force for tested groups was statistically significant at 5% level of significance.
The mean maximum biting force in Group A before insertion of immediate mandibular dentures was 10.21 ± 1.05 and 9.56 ± 0.99 after 12 months from insertion of immediate mandibular dentures. Comparison between mean differences in maximum biting force for tested times was not statistically significant at 5% level of significance.
The mean maximum biting force in Group B before insertion of immediate mandibular overdentures was 9.97 ± 0.89 and 13.48 ± 1.85 after 12 months from insertion of immediate mandibular overdentures. Comparison between mean differences in maximum biting force for tested times was statistically significant at 5% level of significance.
The mean maximum biting force in Group C before insertion of immediate mandibular overdentures was 10.02 ± 0.72 and 17.87 ± 1.67 after 12 months from insertion of immediate mandibular overdentures. Comparison between mean differences in maximum biting force for tested times was statistically significant at 5% level of significance.
DISCUSSION
The loss of the remaining natural teeth is a major and irreversible procedure for the patient. The level of anxiety, with which people face the prospect of losing all their teeth and having to rely on complete denture is unlimited as recorded by Todd and Lader.20 Moreover Basker et al.5 added that irrevocable loss of all teeth can be a serious blow to a patient's morale as it signals, perhaps, that a major milestone in life has been reached and that all that senile decay.
For this study, fifteen patients were selected and the patients were borderline cases for whom a particular form of treatment with immediate overdentures or immediate complete dentures was not clearly indicated.21
Mandibular canines were retained in tooth-supported overdenture group and used as overdenture abutments, because the mandibular canines are usually amenable to endodontic treatment, have strong roots and are strategically located at the corner of the arch as discussed by Renner22 and Langer et al.23 Retaining of mandibular canines also has the main concern for alveolar bone preservation particularly in mandibular anterior segment. Canine abutments were reduced about three mm above the free gingival margin and they were reduced to dome shape to provide point of contact between denture base and abutment for freeing of mandibular denture movement that reduces the damaging effect of horizontal forces.12
Adaptation of the mandibular overdenture to the patients abutments using tooth shade autopolymerized acrylic resin was done to compensate the differences in arbitrary reduction of the canines in the cast and intra orally. This compensation enhances the role of periodontal ligament in overdenture patient.24 Adaptation of the mandibular overdenture to the patient abutments was done after complete healing. The adaptation of the overdenture to the abutments has a positive effect on the reduction of the alveolar bone in the period during which the bone reduction is the maximum and helps in preserving the residual ridge from pressure during the period of bone healing.21 Casted dome shaped dowel coping were made and inserted above the prepared mandibular canines abutment for their protection from caries and for establishing and maintaining specific abutment contours.5,12
Two implants were used to support the immediate mandibular overdenture in the present study for implant supported overdenture group. The use of implant supported overdentures with two implants placed in the mandibular canine region was an efficacious modality for providing an improved chewing function for the completely edentulous patients as found by Jemt et al.,25 Schmitt and Zarb,26 Naert et al.,27 Payne and Solomons28 and Karkazis,29 Visser et al.10 also concluded that there is no difference in clinical and radiographical state of patients treated with an overdenture on two or four implants during a 5-year evaluation period. Hemmings et al.30 added that the implant-supported overdentures presents fewer complications and maintenance requirements. Immediate implants were used in this study to prevent the loss of alveolar bone in height and width as believed by Huys.31 Dental implants are placed directly into an extraction socket site, it decreases the treatment time compared with the traditional 2-stage protocol, and sometimes cost, as mentioned by Castellon and Yukna.32
The implant type used in this study was Impladrill with apical lock osseointegrated implants. The apical lock implant design provides initial stabilization and resists torsional movement of implant as recommended by manufacturer. Implant initial stabilization is an essential need for implant bone osseointegration. The immediate implant, in the present study, replaced the mandibular canines; because the mandibular canine area is the area of choice for most over-implant mandibular overdentures33 and also the single-rooted teeth have been the most frequent sites for immediate implants.34-36
In this study, immediate dental implantation was employed in two stage surgical procedures, firstly submerging for four months, secondly re-exposure and abutment insertion. These procedures of implant submerging and re-exposure were crucial to avoid loading of the implant during the initial healing period.37,38 The implant suprastructure used in this study was modified to be dome shape to provide abutment denture point of contact that permit mandibular overdenture free movement, direct the occlusal forces along the long axes of the implant and reduced the destructive horizontal forces. Adaptation of the mandibular overdenture to the implant abutments using tooth shade autopolymerized acrylic resin was done to compensate the differences in reduction of the canine areas arbitrary in the fitting surface of the denture base and actual size of abutment suprastructure of the implant intraoral during insertion of the mandibular overdenture.
Lateral cephalometric radiograph was used for evaluation of the occlusal vertical dimension changes. This analysis have provided information on skeletal, facial proportions and visualized the changes of occlusal vertical dimension for edentulous patients.39 For determination of occlusal vertical dimension changes in centric occlusion position; reference points, lines and measurements on cephalometric radiographs were used according to procedure described by Lambadakis and Karkazis.15
Electromyography is excellent for information on diagnostic aid of muscle function and is also a reliable and a reproducible method in detecting changes in electrical muscle activity and changes in isometric muscle tension.16,40-46 Evaluation of masseter muscle activity was performed during rest, initial tooth contact from the mandibular rest position and maximum voluntary clench in centric occlusion as described by Tallgren et al.47
In this study, electromyographic recording of the masseter muscle activity was decomposed into wavelet packet coefficient values. The decomposition of the signal into the basis of wavelet functions implies the computation of the inner products between the signal and the basis functions, leading to a set of coefficients called wavelet coefficients. The signal can consequently be reconstructed as a linear combination of the basis function weighted by the wavelet coefficients. The main characteristic of wavelet packet coefficient is the time-frequency localization. It means that most of the energy of the wavelet is restricted to a finite time interval. The advantage of time-frequency localization is that contrary to the short-time Fourier transforms, a wavelet analysis varies the time-frequency aspect ratio, producing good frequency localization at low frequencies (long time windows), and good time localization at high frequencies (short time windows). This produces segmentation or tiling of the time-frequency plane that is appropriate for most physical signals. According to the above cited merits, the wavelet coefficient decomposition of electromyographic signals makes it more accurate method than power spectral analysis.48
Force transducer used in this study for bite force recording employs beam deflection and this deflection was sensed by a strain gauge, which converts forces into measurable electrical signals. Among research workers17-19,49-50 measuring bite force; a bite force transducer was the most commonly used. The elastic load-bearing element of bite force transducer was constructed according to the concept developed originally by Slagter et al.17 and van Kampen et al.,18 but with some modifications to suite this study. A hollow dumbbell shaped stainless steel bearing element was constructed with the same dimensions as developed by Slagter et al.,17 but it was noted that during its calibration, permanent deformation was induced at time of load application at 8 kg. This permanent deformation was considered as a drawback of original designed stainless steel dumbbell shaped bearing element, particularly the suspected average loading for overdenture patients exceeding 8 kg. So, casted dumbbell shaped bearing element with chrome cobalt was constructed to overcome this problem. During calibration of the bite force transducer for this study, it was noted that the recorded strains in relation to applied loads was minimal and not corresponding to the greater changes in load application, for example, when load was 6 kg, the recorded strain was 3 mV, by increasing load up to 12 kg, the induced strain was 3.25 mV. To overcome this problem and make it more suitable for recording the extremity of patients own bite loading, hard stainless steel coil was incorporated to the inner site of elastic load bearing element. Also a side cut with 2 mm space was made along one ring of the elastic load bearing element to make it more flexible without permanent deformation during loading.
For calibration purpose, complete maxillary and mandibular finished dentures were mounted on a simple hinge articulator and mounting of the bite force transducer was aimed to simulate the oral condition during biting.
Method of calibration of bite force transducer was made according to Prombonas et al.19 and to assort it by applying loads of 1, 2, 4, 6, 8, 10, 12, and 14 kilograms. For frequent bite force recording, the elastic load bearing element was designed with metal pin projection that had two mm height and one mm diameter. This pin projection housed in a pinhole formed in the central fossa of the first molar of the denture. The elastic load bearing element was positioned accurately for all frequent recall measurements. While the other method provided by van Kampen et al.18 who used the bite-force transducer covered with rubber base dental impression material to fit the profile of the subjects' teeth. Using this method, a reproducible bite position was obtained for all the five measurements during the fourteen month period, but in this study no attempt was made to follow this procedure due to distortion of rubber base impression material.
The maximum biting force measurements were taken for all groups; one month after prosthesis insertion and twelve months after insertion of immediate dentures. It was aimed to study the changes in maximum biting force in different treatment groups. The measurements were performed three times and the highest bite force of the three efforts was selected as recommended by Slagter et al.17 and van Kampen et al.18
Results of measured occlusal vertical dimension demonstrated regression for all the tested groups. The regression of the occlusal vertical dimension might be due to the continuous decrease in bone volume related to residual ridge resorption. Lambadakis and Karkazis15 found that the reduction in the occlusal vertical dimension can be attributed to continuous vertical reduction of the alveolar process. Also, according to Tallgren et al.,47 the alveolar ridge reduction and settling of the dentures on the basal seats brought about a mandibular inclination with forward-upward rotation of the mandible. This rotation leads to decrease in occlusal vertical dimension with mandibular prognathism.
The results of this study demonstrated that there was significant decrease of the occlusal vertical dimension in the complete denture group, compared with the overdenture groups (tooth and implant-supported), in the first year after extraction of the last remaining teeth and after insertion of the dentures. This result is in agreement with Van Waas et al.21 He also explained the forces on the bone near and at some distance from the remaining roots or implants are less, resulting in less bone reduction and less occlusal vertical dimension changes.
A greater decrease of occlusal vertical dimension for Group C than that for Group B can be because of the sensory feedback input of tooth which preserves alveolar bone, while the absence of such tooth sensory feedback in implant-supported overdenture group may contribute to more alveolar bone resorption. This explanation appeared logic as Sigvard et al. found that the situation with a mandibular overdenture supported by 2 bar-connected implants resembled the situation with natural anterior teeth and a removable partial denture. Maxillary changes were similar to the combination syndrome with anterior bone loss in the maxilla and posterior loss of occlusal contact. Result of this study did not show any significant electromyographic recording activity differences along the right and left masseter muscles. This result confirms the proper patient's selection as all have healthy stomatognathic system.
In addition, the results of this study had shown an interesting finding, that there was no statistically significant difference in masseter muscles electromyographic recording in the rest position between all the tested groups. This indicated that the rest position is a postural mechanism which coexist with the sensorimotor feed back mechanism during dentate life and manifest itself again when teeth are removed and clinical rest position disappear and suspecting that primitive unlearned postural reflexes of the mandible also exist. Another argument might be that the facial muscles are maintained in their correct position in immediate denture as found by Tallgren et al.47
The result of this study also showed a significantly decreased masseter muscles' electromyographic activity in tooth-supported overdenture group compared with that of conventional immediate complete denture and implant-supported overdenture groups during initial tooth contact position. This result might be due to the role of periodontal ligament as suggested by Nagasawa et al.,24 who suggested that the periodontal ligament plays an important role in the efficiency of the muscular activity during chewing in patients wearing overdenture prosthesis.
Another finding was significant differences in the electromyographic masseter muscles' activity during maximum voluntary clench in all the tested groups. Patients with implant supported overdentures seemed to exhibit a greater masseter muscles' electromyographic activity during maximum voluntary clench than mucosal and tooth supported overdentures. This can be attributed to the voluntary reflex which made jaw closing to a much greater extent.
Results of increased masseter muscle activity for implant supported overdenture group than tooth and mucosal borne prosthesis is according to van Kampen et al.,18 who observed a significant increase in masticatory function after the new overdenture was attached to the oral implants and implant-supported prostheses tend to increase masticatory muscles activity. Results of recording maximum biting force for Group A, who received immediate complete mandibular denture (totally mucosal supported) demonstrated insignificance difference in their maximum biting after one year of immediate denture insertion. This result was properly related to recent extraction and patient's inability to bite hard with new dentures. Although all sore spots had been eliminated before recording bite force; patients were still unable to bite hard. The fact that patients wearing complete dentures for one year without complaints and still experiencing the same magnitude of biting force, could be due to the changes in occlusal relationships of the dentures because of alveolar ridge resorption and settling of the dentures on the basal seat. This explanation appears to be supported by results of decreased occlusal vertical dimension for mucosal supported mandibular complete dentures.
Results of significant increase in maximum biting force for both tooth and implant supported overdenture after one year than that before immediate denture insertion can be explained as there is improved support and stability, more self confidence, assurance and satisfaction with their prosthesis. With respect for implant-supported, the same explanation for tooth supported overdenture group can be used.
The result of this study also revealed a significant increase in maximum biting force after one year for implant and tooth-supported overdenture groups compared to conventional immediate denture group. This result may be due to the good support and stability of the tooth and implant-supported overdentures in comparison to the mucosal-supported dentures.
In comparison of maximum biting force for tooth and implant supported overdentures after one year of overdenture wearing, the implant-supported overdenture group experienced greater increase in the maximum biting force than tooth-supported group. This can be explained as the patient with implant-supported prosthesis exhibited voluntary reflex which make their jaw close to a much greater extent than the patient with tooth borne prosthesis. Patient with tooth-supported prosthesis still had tactile proprioceptive reflex arising from periodontal ligament that alarm them against overload.
CONCLUSION
With increased experience comes a greater understanding of potential complications and features when applying immediate prosthetic fabrication to better insure its success. Immediate fabrication of implant overdenture prosthesis can be successful with increased clinical efficiency under specific clinical situations. The biting force of masticatory muscle is functionally dependent on maintenance of muscle health and occlusal vertical dimension.
References
- 1.van Waas MA. The influence of psychologic factors on patient satisfaction with complete dentures. J Prosthet Dent. 1990;63:545–548. doi: 10.1016/0022-3913(90)90073-l. [DOI] [PubMed] [Google Scholar]
- 2.Boerrigter EM, Geertman ME, Van Oort RP, Bouma J, Raghoebar GM, van Waas MA, van't Hof MA, Boering G, Kalk W. Patient satisfaction with implant-retained mandibular overdentures. A comparison with new complete dentures not retained by implants-a multicentre randomized clinical trial. Br J Oral Maxillofac Surg. 1995;33:282–288. doi: 10.1016/0266-4356(95)90038-1. [DOI] [PubMed] [Google Scholar]
- 3.Fenn HRB, Liddlelow KP, Gimson AP, MacCregor AR. Clinical Dental prosthetics. 3rd ed. Butterworth-Heinemann Ltd; 1989. pp. 290–304. [Google Scholar]
- 4.Winkler S. Essentials of complete denture prosthodontics. 2nd ed. Philadelphia: Ishiyaku Euro America; 1994. pp. 361–374. [Google Scholar]
- 5.Basker RM, Davenport JC, Tomlin HR. Prosthetic treatment of the edentulous patient. 4th ed. Blackwell Co; 2002. pp. 32–53. [Google Scholar]
- 6.Zarb GA, Bolender CL, Eckert SE. Prosthodontic treatment for edentulous patients: complete dentures and implant-supported prostheses. 12th ed. St. Louis: Mosby; 2004. pp. 123–159. [Google Scholar]
- 7.Mericske-Stern R, Steinlin Schaffner T, Marti P, Geering AH. Peri-implant mucosal aspects of ITI implants supporting overdentures. A five-year longitudinal study. Clin Oral Implants Res. 1994;5:9–18. doi: 10.1034/j.1600-0501.1994.050102.x. [DOI] [PubMed] [Google Scholar]
- 8.Morais JA, Heydecke G, Pawliuk J, Lund JP, Feine JS. The effects of mandibular two-implant overdentures on nutrition in elderly edentulous individuals. J Dent Res. 2003;82:53–58. doi: 10.1177/154405910308200112. [DOI] [PubMed] [Google Scholar]
- 9.Budtz-Jørgensen E. Effect of controlled oral hygiene in overdenture wearers: a 3-year study. Int J Prosthodont. 1991;4:226–231. [PubMed] [Google Scholar]
- 10.Visser A, Raghoebar GM, Meijer HJ, Batenburg RH, Vissink A. Mandibular overdentures supported by two or four endosseous implants. A 5-year prospective study. Clin Oral Implants Res. 2005;16:19–25. doi: 10.1111/j.1600-0501.2004.01085.x. [DOI] [PubMed] [Google Scholar]
- 11.Passamonti G, Kotrajarus P, Gheewalla RK, Clark RE, Maness WL. The effect of immediate dentures on maxillomandibular relations. J Prosthet Dent. 1981;45:122–126. doi: 10.1016/0022-3913(81)90326-7. [DOI] [PubMed] [Google Scholar]
- 12.Schwartz IS, Morrow RM. Overdentures. Principles and procedures. Dent Clin North Am. 1996;40:169–194. [PubMed] [Google Scholar]
- 13.Palmer R, Palmer P, Howe L. Complications and maintenance. Br Dent J. 1999;187:653–658. doi: 10.1038/sj.bdj.4800358. [DOI] [PubMed] [Google Scholar]
- 14.el Charkawi H. Immediate implant in fresh extraction socket of resected mandibular first molar: a preliminary clinical report. Implant Dent. 2001;10:272–279. doi: 10.1097/00008505-200110000-00011. [DOI] [PubMed] [Google Scholar]
- 15.Lambadakis J, Karkazis HC. Changes in the mandibular rest position after removal of remaining teeth and insertion of complete dentures. J Prosthet Dent. 1992;68:74–77. doi: 10.1016/0022-3913(92)90289-m. [DOI] [PubMed] [Google Scholar]
- 16.Saifuddin M, Miyamoto K, Ueda HM, Shikata N, Tanne K. A quantitative electromyographic analysis of masticatory muscle activity in usual daily life. Oral Dis. 2001;7:94–100. [PubMed] [Google Scholar]
- 17.Slagter AP, Bosman F, van der Glas HW, van der Bilt A. Human jaw-elevator muscle activity and food comminution in the dentate and edentulous state. Arch Oral Biol. 1993;38:195–205. doi: 10.1016/0003-9969(93)90028-k. [DOI] [PubMed] [Google Scholar]
- 18.van Kampen FM, van der Bilt A, Cune MS, Bosman F. The influence of various attachment types in mandibular implant-retained overdentures on maximum bite force and EMG. J Dent Res. 2002;81:170–173. doi: 10.1177/154405910208100305. [DOI] [PubMed] [Google Scholar]
- 19.Prombonas A, Vlissidis D, Molyvdas P. The effect of altering the vertical dimension of occlusion on biting force. J Prosthet Dent. 1994;71:139–143. doi: 10.1016/0022-3913(94)90021-3. [DOI] [PubMed] [Google Scholar]
- 20.Todd JE, Lader D. Adult Dental Health 1988: United, Kingdom. Social Survey Report SS1260. London: HMSO; 1991. [Google Scholar]
- 21.Van Waas MA, Jonkman RE, Kalk W, Van't Hof MA, Plooij J, Van Os JH. Differences two years after tooth extraction in mandibular bone reduction in patients treated with immediate overdentures or with immediate complete dentures. J Dent Res. 1993;72:1001–1004. doi: 10.1177/00220345930720060101. [DOI] [PubMed] [Google Scholar]
- 22.Renner RP. The overdenture concept. Dent Clin North Am. 1990;34:593–606. [PubMed] [Google Scholar]
- 23.Langer Y, Langer A. Root-retained overdentures: Part II-Managing trauma between edentulous ridges and opposing dentition. J Prosthet Dent. 1992;67:77–81. doi: 10.1016/0022-3913(92)90054-e. [DOI] [PubMed] [Google Scholar]
- 24.Nagasawa T, Okane H, Tsuru H. The role of the periodontal ligament in overdenture treatment. J Prosthet Dent. 1979;42:12–16. doi: 10.1016/0022-3913(79)90322-6. [DOI] [PubMed] [Google Scholar]
- 25.Jemt T, Stålblad PA. The effect of chewing movements on changing mandibular complete dentures to osseointegrated overdentures. J Prosthet Dent. 1986;55:357–361. doi: 10.1016/0022-3913(86)90120-4. [DOI] [PubMed] [Google Scholar]
- 26.Schmitt A, Zarb GA. The notion of implant-supported overdentures. J Prosthet Dent. 1998;79:60–65. doi: 10.1016/s0022-3913(98)70195-7. [DOI] [PubMed] [Google Scholar]
- 27.Naert I, De Clercq M, Theuniers G, Schepers E. Overdentures supported by osseointegrated fixtures for the edentulous mandible: a 2.5-year report. Int J Oral Maxillofac Implants. 1988;3:191–196. [PubMed] [Google Scholar]
- 28.Payne AG, Solomons YF. Mandibular implant-supported overdentures: a prospective evaluation of the burden of prosthodontic maintenance with 3 different attachment systems. Int J Prosthodont. 2000;13:246–253. [PubMed] [Google Scholar]
- 29.Karkazis HC. EMG activity of the masseter muscle in implant supported overdenture wearers during chewing of hard and soft food. J Oral Rehabil. 2002;29:986–991. doi: 10.1046/j.1365-2842.2002.00943.x. [DOI] [PubMed] [Google Scholar]
- 30.Hemmings KW, Schmitt A, Zarb GA. Complications and maintenance requirements for fixed prostheses and overdentures in the edentulous mandible: a 5-year report. Int J Oral Maxillofac Implants. 1994;9:191–196. [PubMed] [Google Scholar]
- 31.Huys LW. Replacement therapy and the immediate post-extraction dental implant. Implant Dent. 2001;10:93–102. doi: 10.1097/00008505-200104000-00004. [DOI] [PubMed] [Google Scholar]
- 32.Castellon P, Yukna RA. Immediate dental implant placement in sockets augmented with HTR synthetic bone. Implant Dent. 2004;13:42–48. doi: 10.1097/01.id.0000116451.04676.7b. [DOI] [PubMed] [Google Scholar]
- 33.Payne AG, Solomons YF. The prosthodontic maintenance requirements of mandibular mucosa- and implant-supported overdentures: a review of the literature. Int J Prosthodont. 2000;13:238–243. [PubMed] [Google Scholar]
- 34.Salama H, Salama M. The role of orthodontic extrusive remodeling in the enhancement of soft and hard tissue profiles prior to implant placement: a systematic approach to the management of extraction site defects. Int J Periodontics Restorative Dent. 1993;13:312–333. [PubMed] [Google Scholar]
- 35.Gelb DA. Immediate implant surgery: three-year retrospective evaluation of 50 consecutive cases. Int J Oral Maxillofac Implants. 1993;8:388–399. [PubMed] [Google Scholar]
- 36.Becker W, Dahlin C, Becker BE, Lekholm U, van Steenberghe D, Higuchi K, Kultje C. The use of e-PTFE barrier membranes for bone promotion around titanium implants placed into extraction sockets: a prospective multicenter study. Int J Oral Maxillofac Implants. 1994;9:31–40. [PubMed] [Google Scholar]
- 37.Brosh T, Persovski Z, Binderman I. Mechanical properties of bone-implant interface: an in vitro comparison of the parameters at placement and at 3 months. Int J Oral Maxillofac Implants. 1995;10:729–735. [PubMed] [Google Scholar]
- 38.Sahin S, Cehreli MC, Yalçin E. The influence of functional forces on the biomechanics of implant-supported prostheses-a review. J Dent. 2002;30:271–282. doi: 10.1016/s0300-5712(02)00065-9. [DOI] [PubMed] [Google Scholar]
- 39.Brzoza D, Barrera N, Contasti G, Hernández A. Predicting vertical dimension with cephalograms, for edentulous patients. Gerodontology. 2005;22:98–103. doi: 10.1111/j.1741-2358.2005.00060.x. [DOI] [PubMed] [Google Scholar]
- 40.Gervais RO, Fitzsimmons GW, Thomas NR. Masseter and temporalis electromyographic activity in asymptomatic, subclinical, and temporomandibular joint dysfunction patients. Cranio. 1989;7:52–57. doi: 10.1080/08869634.1989.11678268. [DOI] [PubMed] [Google Scholar]
- 41.Ferrario VF, Sforza C, D'Addona A, Miani A., Jr Reproducibility of electromyographic measures: a statistical analysis. J Oral Rehabil. 1991;18:513–521. doi: 10.1111/j.1365-2842.1991.tb00074.x. [DOI] [PubMed] [Google Scholar]
- 42.Visser A, McCarroll RS, Naeije M. Masticatory muscle activity in different jaw relations during submaximal clenching efforts. J Dent Res. 1992;71:372–379. doi: 10.1177/00220345920710020501. [DOI] [PubMed] [Google Scholar]
- 43.Carlson CR, Okeson JP, Falace DA, Nitz AJ, Curran SL, Anderson D. Comparison of psychologic and physiologic functioning between patients with masticatory muscle pain and matched controls. J Orofac Pain. 1993;7:15–22. [PubMed] [Google Scholar]
- 44.Carlson N, Moline D, Huber L, Jacobson J. Comparison of muscle activity between conventional and neuromuscular splints. J Prosthet Dent. 1993;70:39–43. doi: 10.1016/0022-3913(93)90035-m. [DOI] [PubMed] [Google Scholar]
- 45.Gay T, Rendell J, Majoureau A, Maloney FT. Estimating human incisal bite forces from the electromyogram/bite-force function. Arch Oral Biol. 1994;39:111–115. doi: 10.1016/0003-9969(94)90105-8. [DOI] [PubMed] [Google Scholar]
- 46.Türp JC, Schindler HJ, Pritsch M, Rong Q. Antero-posterior activity changes in the superficial masseter muscle after exposure to experimental pain. Eur J Oral Sci. 2002;110:83–91. doi: 10.1034/j.1600-0722.2002.11198.x. [DOI] [PubMed] [Google Scholar]
- 47.Tallgren A, Holden S, Lang BR, Ash MM., Jr Jaw muscle activity in complete denture wearers-a longitudinal electromyographic study. J Prosthet Dent. 1980;44:123–132. doi: 10.1016/0022-3913(80)90122-5. [DOI] [PubMed] [Google Scholar]
- 48.Daubechies I. Orthonormal bases of compactly supported wavelets. Comm Pure Appl Math. 1988;41:909–996. [Google Scholar]
- 49.Laurell L. Occlusal forces and chewing ability in dentitions with cross-arch bridges. Swed Dent J Suppl. 1985;26:160. [PubMed] [Google Scholar]
- 50.Clark GT, Carter MC, Beemsterboer PL. Analysis of electromyographic signals in human jaw closing muscles at various isometric force levels. Arch Oral Biol. 1988;33:833–837. doi: 10.1016/0003-9969(88)90108-2. [DOI] [PubMed] [Google Scholar]