

Abstract
Background
GPs report various barriers to the use and practice of evidence-based medicine (EBM). A review of research on these barriers may help solve problems regarding the uptake of evidence in clinical outpatient practice.
Aim
To determine the barriers encountered by GPs in the practice of EBM and to come up with solutions to the barriers identified.
Design
A systematic review of the literature.
Method
The following databases were searched: MEDLINE® (PubMed®), Embase, CINAHL®, ERIC, and the Cochrane Library, until February 2011. Primary studies (all methods, all languages) that explore the barriers that GPs encounter in the practice of EBM were included.
Results
A total of 14 700 articles were identified, of which 22 fulfilled all inclusion criteria. Of the latter, nine concerned qualitative, 12 concerned quantitative, and one concerned both qualitative and quantitative research methods. The barriers described in the articles cover the categories: evidence (including the accompanying EBM steps), the GP’s preferences (experience, expertise, education), and the patient’s preferences. The particular GP setting also has important barriers to the use of EBM. Barriers found in this review, among others, include lack of time, EBM skills, and available evidence; patient-related factors; and the attitude of the GP.
Conclusion
Various barriers are encountered when using EBM in GP practice. Interventions that help GPs to overcome these barriers are needed, both within EBM education and in clinical practice.
Keywords: decision-making, evidence-based medicine, general practitioners, review
INTRODUCTION
Evidence-based medicine (EBM) is the translation of results of clinical epidemiological studies into daily practice. The definition states that EBM is the conscientious, explicit, and judicious use of current best evidence, in combination with the physician’s clinical expertise and the preferences of the patient in making decisions about the care of individual patients.1–4 A visual illustration of the process of decision-making according to EBM in general practice is depicted in Figure 1.
Figure 1.
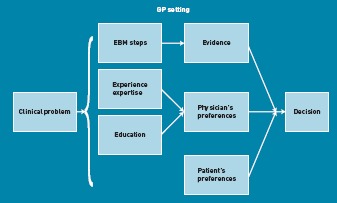
Conceptual model of evidence-based decision making in GPs, adapted from Sackett et al2 and Offringa et al.55
Integration of the above-mentioned aspects of EBM — and thereby going beyond the direct use of research knowledge without integration of GP preferences and the situation of the patient — is needed to be able to help the individual patient best.5,6 However, various review studies from other healthcare professions document the existence of barriers that hinder the practice of EBM.7,8 Consequently, improvement of medical care and the treatment of the individual patient are at stake.1 Based on the model of evidence-based decision making (Figure 1), and keeping the aspects of EBM in mind, the barriers can be related to the evidence itself, to the expertise of the GP, the GP’s and the patient’s situation, and the GP’s clinical situation. Reducing or eliminating the barriers that prevent GPs from implementing EBM in all these areas can improve evidence-based practice,9 and knowledge of these barriers can assist in enhancement of the implementation of EBM through education.
The purpose of this study was to systematically review the evidence for all the barriers encountered by GPs in the use of EBM in clinical practice.
METHOD
Eligibility criteria
Studies meeting the following criteria were included in the review:
primary studies (any language);
studies about barriers in the practice of EBM;
studies with GPs as subjects;
-
studies with either of the following outcomes:
barriers to the practice of EBM; and
barriers to the practice of more than one of the EBM steps.
Studies that had primary care physicians as subjects and in which the outcomes of GPs were not presented separately were excluded. Before definite exclusion, the study authors were contacted to obtain data for GPs only. Studies in which the application or use of specific guidelines were described were also excluded, since barriers in these latter studies are mainly related to the logistical and clinical aspects of that particular guideline or disorder. The language in which an article is written was not an exclusion criterion. If needed, relevant parts of the paper were translated. In cases where more information was needed to ascertain inclusion or exclusion, the authors of the study were contacted.
How this fits in
A significant number of barriers prevent GPs from implementing EBM. Access to and applicability of clinical evidence are major impediments to the implementation of EBM in general practice. Furthermore, despite the clear definition of EBM — combining the evidence, the GP’s preferences and expertise, and the patient’s situation — GPs still perceive the discrepancy between the situation of the patients or of themselves and the evidence as a barrier to the use of EBM. This review provides an overview of all the barriers GPs encounter in the use of EBM.
Information sources
A search for studies was carried out in MEDLINE® (PubMed®), Embase, CINAHL®, ERIC, and the Cochrane Library. The search was completed in February 2011.
The search strategy was based on the search terms from an earlier systematic review of barriers faced by resident doctors. It was developed by a clinical librarian and adapted for GPs (Box 1).8
Box 1. Search for studies
MEDLINE (PubMed) (1980 to present)
((family practitioner * OR family physician* OR “Family Practice”[Mesh] OR “Physicians, Family”[Mesh] OR “Primary Health Care”[Mesh] OR primary health care) AND (Evidence-Based Medicine [Mesh] OR evidence based medicine[Text Word] OR ebm[tiab]))
Embase (Ovid)
((General Practitioner/ OR family practitioner$.mp./ OR family physician$.mp./ OR primary health care.mp./ OR Primary Health Care) AND (evidence based medicine.mp. OR ebm.mp. OR Evidence Based Medicine/))
CINAHL and ERIC (EBSCOhost)
((evidence based medicine) OR (ebm) OR (MM “Medical Practice, Evidence-Based”) OR (MM “Professional Practice, Evidence-Based”) OR (MM “Medical Practice, Research-Based”)) AND ((MM “Family Practice”) OR (MM “Physicians, Family”) OR OR (“general practice”) OR (“General practitioner”) OR (MM “Primary health care”) OR (“Primary care”))
The Cochrane Library
((MeSH descriptor “Family Practice” explode all trees) OR (general practitioner:ti,ab) OR (family physician:ti,ab) OR (general practice:ti,ab) OR (Primary health care:ti,ab) OR (Primary care:ti,ab)) AND ((MeSH descriptor Evidence-Based Medicine explode all trees) OR (evidence NEXT based NEXT medicine):ti,ab OR ebm))
Study selection
Before reviewing, the researchers discussed the inclusion and exclusion criteria in order to improve inter-rater reliability. Two reviewers independently appraised the titles of the studies retrieved from the literature search, to assess which studies were clearly irrelevant to the present study. Studies were excluded only if both reviewers considered a title unsuitable for inclusion. The same two reviewers independently appraised the abstracts of the studies that had not been excluded. These studies were excluded if both reviewers thought it appropriate to do so. If only one reviewer thought the study should be included, a decision was made through discussion with a third reviewer.
Two reviewers independently appraised the complete texts of the studies that had been included, based on their abstracts. If only one of the reviewers thought that the study should be included, a third reviewer determined whether the article should indeed be included.
Kappa with a 95% confidence interval (CI) was calculated, to quantify the agreement between the reviewers in the various stages. The flow chart of the selection process for this review is presented in Figure 2.
Figure 2.
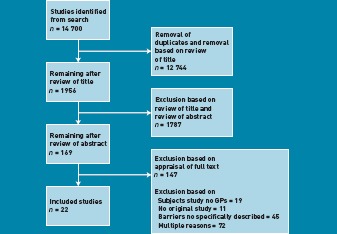
Flow chart for the selection of studies.
Quality assessment
Quality assessment was performed according to the criteria (Table 1) used in another review regarding EBM-related barriers:8
the quality of quantitative studies (except those from randomised controlled trials [RCTs]) was assessed using adapted recommendations from the STROBE (Strengthening the Reporting of OBservational studies in Epidemiology) initiative;10
the quality of qualitative studies was judged by applying adapted criteria proposed by Giacomini and Cook;11 and
the quality of RCTs was assessed using criteria recommended by the Cochrane Collaboration.12
Table 1.
Quality assessment
| Qualitative research methods | Quantitative research methods | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Year of publication | Clear objective | Selection of study participants | Methods | Data collection | Analysis of data | Clear presentation results | Specific objective/hypothesis | Inclusion participant | Definition of outcome | Description methods and measurement | Risk of recollection bias | Participants | Presentation of results |
| Sánchez López et al20 | 2010 | + | ± | ± | ± | ± | + | |||||||
| Carlsen and Norheim17 | 2008 | + | + | + | + | + | + | |||||||
| Yew and reid16 | 2008 | + | + | + | + | + | + | |||||||
| Hannes et al15 | 2005 | + | + | + | + | + | + | |||||||
| Tracy et al14 | 2003 | + | + | + | + | + | + | |||||||
| Freeman34 | 2001 | + | + | + | + | ± | + | |||||||
| Cranney et al13 | 2001 | + | + | + | + | + | + | |||||||
| Oswald and Bateman19 | 2000 | + | ± | + | ± | – | – | |||||||
| Mayer and Piterman18 | 1999 | + | + | + | + | ± | + | |||||||
| Kahveci and Meads32 | 2009 | + | ± | + | ± | n/a | ± | + | ||||||
| Barghouti et al31 | 2009 | + | ± | + | ± | n/a | ± | + | ||||||
| Trevena et al30 | 2007 | ± | ± | + | + | n/a | ± | + | ||||||
| Amin et al29 | 2006 | ± | ± | ± | ± | n/a | ± | ± | ||||||
| Upton and Upton28 | 2006 | + | + | + | + | n/a | ± | + | ||||||
| Chan and Teng21 | 2005 | + | + | + | + | n/a | + | + | ||||||
| Butzlaff et al23 | 2004 | + | ± | + | – | n/a | ± | – | ||||||
| McKenna et al27 | 2004 | + | + | + | + | n/a | ± | ± | ||||||
| Taylor et al26 | 2002 | ± | ± | + | ± | n/a | ± | ± | ||||||
| Cotton and Sullivan25 | 1999 | + | + | + | + | n/a | ± | + | ||||||
| McColl et al24 | 1998 | + | + | + | ± | n/a | + | + | ||||||
| Gupta et al22 | 1997 | + | + | + | + | n/a | + | + | ||||||
| Young and Ward33 | 2001 | + | ± | ± | - | - | - | + | ± | + | + | n/a | + | + |
Opinion of the reviewers about the quality of this item: + = positive, ± = neutral, – = negative, n/a= not applicable (cross-sectional studies).
After pilot testing of the quality-assessment form on four studies, three reviewers independently appraised the included studies on methodological quality; in the case of disagreement, they consulted a fourth reviewer. They separately discussed each item on which there was disagreement among the reviewers. Agreement between reviewers was calculated using the percentage of agreement on all items. If it remained unclear whether an article met the quality criteria, the reviewers contacted the first author of the relevant publication in order to obtain additional information. If the matter of quality remained unclear, this was indicated on the form.
Data collection
A pre-specified data-extraction form was used to extract the following data from the studies: year of publication, period of data collection, study design, validity of instruments used, characteristics of the participating GPs (country, number of responders, and types of practices), response rates (Table 2), and the main outcomes of the study (Table 3). Only outcomes that were specifically denoted as barriers described in the practice of EBM were extracted. The definition of EBM used in the various studies was also explored. Because of the variations in design and outcomes, one researcher extracted the data and then one of three other researchers reviewed the data-extraction forms to assess reliability.
Table 2.
Characteristics of the studies included in this review
| Author | Year of publication | Data collection | Study design | Instrument based on | Country | Participants, number GPs | Response rate, % |
|---|---|---|---|---|---|---|---|
| Sánchez López et al20 | 2010 | 2007 | Focus groups | Spain | 19 | 100 | |
| Carlsen and Norheim17 | 2008 | 2007 | Semi-structured group interviews | Norway | 27 | 100 | |
| Yew and Reid16 | 2008 | 2001 | Telephone interviews | Green62 | US | 10 | (10/16) = 63 |
| Hyde63 | |||||||
| Greenhalgh64 | |||||||
| Hannes et al15 | 2005 | 2002–2003 | Focus groups | Belgium | 31 | 100 | |
| Tracy et al14 | 2003 | 2002 | Semi-structured interviews | Canada | 15 | (15/23) = 65 | |
| Freeman and Sweeney34 | 2001 | Unknown | Balint style groups | UK | 19 | 100 | |
| Cranney et al13 | 2001 | Unknown | Semi-structured interviews | UK | 34 | 9/76 practices = 12 | |
| Oswald and Bateman19 | 2000 | Unknown | Interviews | UK | 6 | 100 | |
| Mayer and Piterman18 | 1999 | 1996–1997 | Focus groups | Australia | 27 | ||
| Kahveci and Meads32 | 2009 | 2006–2007 | Survey | McColl24 | Turkey | 138 | 73 |
| Barghouti et al31 | 2009 | 2007 | Survey | Al-Almaie65 | Jordan | 141 | 71 |
| Al-Ansary66 | |||||||
| McColl24 | |||||||
| Trevena et al30 | 2007 | 2003 | Telephone interviews | Degner67 | Australia | 107 | (107/155) = 69 |
| Amin et al29 | 2006 | 2004 | Survey | Fedorowicz68 | Bahrain | 81 | (81/124) = 65 |
| Upton and Upton28 | 2006 | Unknown | Survey | Upton69 | UK | 302 | 60 |
| Chan and Teng21 | 2005 | 2003 | Survey | McColl24 | Singapore | 40 | 40 |
| Butzlaff et al23 | 2004 | 2001 | Randomised controlled trial | Germany | 72 | 73 | |
| McKenna et al27 | 2004 | 2000–2001 | Survey | Funk70 | UK | 356 | 65 (overall) |
| Nylenna71 | |||||||
| Taylor et al26 | 2002 | 2000 | Survey and interviews | Australia | 89 | 86 | |
| Cotton and Sullivan25 | 1999 | 1995–1997 | Survey | UK | 228 | 74 | |
| McColl et al24 | 1998 | 1997 | Survey | UK | 302 | (302/452) = 67 | |
| Gupta et al22 | 1997 | 1993–1995 | Survey | Australia | 286 | 77 | |
| Young and Ward33 | 2001 | 1999 | Survey and interviews | McColl24 | Australia | 60 | 100 |
| Young72,73 | |||||||
Table 3.
Barriers to the use of evidence-based medicine (EBM) by GPs
| Evidence | GP's preferences | Patient's situation | Practice setting |
|---|---|---|---|
| • Translating trials into practice13,18,30 | • Knowledge of EBM15,26 | • Treatment expectations different from evidence25,31,33 | • Applicability of evidence to general practice13,14,17,18,22,24,27,30,34 |
| • Use of evidence is complicated23 | • Difficulty keeping up13,27 | • Adapting to preferences, beliefs, and demands different from evidence15,24,26,30,33 | • Lack of time:13–16,20,21,25,28–31,33 |
| • to search for evidence17,19,33 | |||
| • to access evidence19,26 | |||
| • to appraise evidence33 | |||
| • to apply evidence23 | |||
| • to keep up to date15–17 | |||
| • to discuss with patient33 | |||
| • per patient33 | |||
| • to reflect on practice26 | |||
| • Change of existing evidence15,19 | • Difficult to find information14,17,27 | • Reluctant to comply with treatment34 | • Lack of managerial support20,22,27 |
| • User-friendliness: need for summaries,14 also for better formats22,30 | • EBM skills14,15,19,24,30,31,33 | • GP's desire for patient's appreciation17 | • Lack of investment/incentives27,31 |
| • Lack of (qualitatively good) available evidence15,24,26,30,31,33 | • Attitude towards EBM15 | • Discussing with patient24 | • Fear of punishment or litigation:18,25 |
| • limited in treatment options and clinical freedom15,18,23,25 | • ‘convincing and pressure to meet | • EBM is a threat24,31 | |
| • expectations’17,26 | |||
| • lack of interest/motivation32 | • ‘selling evidence to patients’17 | ||
| • ‘EBM not helpful’16 | |||
| • ‘EBM will not benefit practice’27 | |||
| • in older people (less effort applying)13 | |||
| • lack of ownership/commitment13 | |||
| • Contradictions in evidence15,17,18,26,27,30 | • Lack of training20,25,32 | • Not accepting uncertainty of evidence18 | • Money needed:15,16,27,30,33 |
| • direction in training13,15,27 | • for access to internet and resources26 | ||
| • EBM carries no financial gain27,31 | |||
| • Too much available evidence24,31 | • Personal and professional experiences different from evidence34 | • Confidence in GP reduced by guidelines25 | • Rural location26 |
| • Lack of resources14,15,26 | • Fear of side effects17 or harm19 | • Relationship between GP and patient34 | • Morale24 |
| • Available sources not helpful16 | • Harmonising guidance19,30 | • Experiences of the patient different from evidence34 | |
| • Access (computers, internet, journals, databases, or libraries)14,16,21,23–31 | • Practicalities of real life13,24 | • Toleration of uncertainties18 | |
| • Lack of trust in origin17,18 and in independence of evidence sources15 or information spread by other organisations (not evidence based)15 | • Lack of confidence19,30 | • Clinical symptoms, disease14 | |
| • Level of evidence22 | • Familiarity with new role15,26 | • Psychosocial context18,31 | |
| • Implications of the evidence22 | • Personal and organisational inertia24 | • Influence of media15,24 | |
| • The language in which evidence is written20 | • Culture29 | • Information retrieval by patient20 | |
| • Lack of help in interpretation by experts/specialists13,14,20 | • Influence of belief of peers19,24–26,31 | • Words of GP and presentation of information used by GP34 | |
RESULTS
Study selection
The literature search led to identification of 14 700 studies (Figure 2). After screening for doubles and applying inclusion criteria to titles and abstracts, 169 articles remained for full-text assessment. During title screening, the agreement between the two reviewers was good: kappa was 0.73 (95% CI = 0.71 to 0.74). During abstract screening and full-text inclusion, the agreement between the two reviewers was fair, with a kappa of 0.34 (95% CI = 0.27 to 0.41) and good with a kappa of 0.71 (95% CI = 0.56 to 0.85), respectively. Twenty-two articles that satisfied all inclusion criteria were included in the review.13–34
Study characteristics
Of the 22 studies that were included, nine concerned qualitative,13–20,24 12 concerned quantitative,21–32,34 and one concerned both qualitative and quantitative research methods.33 One RCT was included in the review, but the barriers regarding EBM that were described in this study — and respectively included in this article — were described for the intervention group (specific access to literature) only.23 The characteristics of the studies are shown in Table 2.
Quality assessment (Table 1)
After individual judgement, the reviewers agreed on 76% of all quality criteria that were scored. Of the qualitative studies, five scored positively on all aspects (resembling a low risk of bias within these studies),13–17 while one study, which combined qualitative and quantitative methods, scored negatively on most quality aspects of the qualitative part of the study, and is therefore suspected of having a high risk of bias.33 The quality of the quantitative studies was good: two studies had a positive score on all the items,21,22 while the others had up to six items that were not adequate. Only one study had two items assessed as negative.23
Synthesis of results
Because of the expected heterogeneity between study designs and presentation of outcomes, no attempt was made to pool the quantitative data. Based on the current definition of EBM, the barriers were categorised into the following areas: evidence, the GP’s preferences and expertise, the patient’s situation, and the GP setting. Categories were created according to Figure 1, in an attempt to position the extracted barriers more systematically. When barriers could be placed in more than one category, the choice was based on whether the barrier was more common (then it was placed in the category evidence or practice) or more individualistic (then it was placed into the category GP). To enhance understanding of the chosen categories, the categories are described in more detail next.
Evidence
The five-step model emphasises the search for evidence with respect to EBM: ask, access, appraise, apply, and audit.1 In practice, these five steps are used when facing a new clinical question, and are used less explicitly when managing patients with more common clinical problems, for which the physician already knows most evidence. Particularly in primary care, aggregated evidence such as guidelines or systematic reviews are the sources most referred to.35 However, a rational analysis of all evidence has to take place.36
The GP’s preferences and expertise
In order to change their practice, GPs require both a positive attitude towards EBM37 and adequate knowledge and skills regarding the five steps of EBM.1 However, the GP’s clinical expertise and previous experiences are also important sources of information for clinical decision-making. The GP’s level of clinical experience or expertise therefore plays a role in clinical decision-making and influences the way in which problems are solved: more intuitively or rationally.38 GPs rely on so-called mindlines, which are ‘collectively reinforced, internalised, tacit guidelines’ that can be modified when integrating external information.39
The patient’s situation
The situation of the patient can be described in terms of both the clinical situation of the patient, and the patient’s personal preferences. A patient’s preference is defined as ‘the desirability of a health-related outcome, process or treatment choice’.4 Besides the research evidence and the contributions of the GP’s experience, patient preferences also need to be included in the process of decision-making.40 Patients expect to participate in the decision-making process,41 and contemporary patient-centred medicine has made the experience of patients and their role in clinical decision-making more prominent.
GP setting
There could well be barriers that apply to the GP setting, partly owing to the fact that primary care is considered different from the purely disease-centred secondary care where EBM was developed.42 Consultations in general practice are more complex than consultations in some specialties,43 and the patients in primary care also differ significantly from patients in secondary care regarding variation in disorders and disease stages.
Results of the studies
Definition of evidence-based medicine
Six of the included studies14,21,26,29,31,33 give a definition of EBM based on the definition of either Sackett et al2 or Haynes et al.44 Studies that did not explicitly give a definition of EBM are studies about the implementation of evidence,13,17,22,25 or ones that give a more exploratory description about how evidence or EBM should be used.15,16,18,20,23,24,27,28,30,32,34 In all the studies, barriers related to one or more of the components of the conceptual model of EBM (evidence, the GP’s preferences, the patient’s preferences, the GP setting) were found. These barriers are summarised in Table 3.
Barriers related to evidence
Most of the 22 articles describe barriers that are related to the evidence itself.14–18,20–34 Some say that general practice lacks sound evidence,14,24,26,30,31,33 especially for the many problems faced by GPs.15 In one study sample, 34% of the surveyed GPs felt that there is a lack of evidence.24 Other studies found that the available evidence is perceived to be of inadequate quality.15,30 On the other hand, too much available evidence is also experienced as a problem.24,31 Furthermore, GPs say that the available evidence is contradictory,15,26,27,30 not up to date, and liable to time delays.15 Time delays mainly appear between the publication of research and eventual adjustment of practice.15
Access is the barrier most mentioned.14,15,21–31 It can be subdivided into lacking resources, no access to evidence, and computer- or internet-related problems,14–16,21,23–31 and therefore mainly entails technical difficulties.23 The accessibility of literature written in English is described as a problem for non-English GPs,20 as is the understanding of the English in which articles are written and the lack of evidence published in the GP’s own language.32 One study states that logistical problems such as access make GPs less enthusiastic about using EBM.34
There are many evidence resources, but only a small number are considered independent.15 GPs doubt the reliability of evidence,17 that is, whether a guideline is truly based on evidence,22 especially when evidence has been derived from certain sources that are biased by, for instance, industry (such as the pharmaceutical industry),20,32 commercial or consumer organisations, or the mass media.15
Barriers related to the GP’s preferences and expertise
In a quantitative study, 72% of the GPs reported encountering barriers to the application of EBM.30 The GP’s attitude influences the application of EBM: GPs are generally not positive about the usefulness of EBM.16,27 This is caused by the idea that EBM requires them to work strictly according to the guidelines.15,18,23,25 Furthermore, earlier personal experiences in life or in clinical practice influence the use of evidence;26,34 for instance, deaths in the personal or practice environment due to strokes related to arrhythmias led to a more controlled anticoagulation treatment.34 The opinion of colleagues about EBM is considered important in the use of EBM,24,25,31 primarily because the attitude of these colleagues influences the practice of EBM.31
Lack of knowledge and skills also influences GPs’ use of EBM:15–17,24,30,31,33 55.6% feel that training in EBM is required,25 and that there is a lack of such training.13,20,25,27,32 A lack of skills in searching and in accessing resources is a barrier:27,30,33 not knowing where to search,26,30 and difficulty in finding evidence (or finding it quickly),14,17,26 are among the barriers mentioned by GPs. Lack of appraisal skills,24,30,31,33 and of confidence in using those skills,19 are barriers related to critical revision of the evidence. Also, GPs find it hard to assess applicability.19,23
Barriers related to the patient’s preferences
Patient-related barriers limit the use of EBM by GPs.17,18,20,24–26,30,31,33,34 Patients’ preferences, expectations, and beliefs have a major influence on EBM use, according to GPs.26,30,31,33,34 When the evidence-based preferences of the GP and the wishes of the patient do not match, the GP may feel a barrier to convincing the patient,17–26 because GPs feel pressured to fulfil patients’ wishes.15,17,24,26,34 This results from the fact that patients have strong ideas about what they want from their GP.15
As concluded in a qualitative study, the quality of the relationship with a patient is considered a barrier to using evidence.34 Especially when GPs know their patients well, they find it hard to translate the evidence to their patients because they feel that deviating from guidelines based on experience or patient preferences is not evidence-based behaviour.34
Barriers related to the general practice setting
There are several barriers relating to the general practice setting.13–18,21,23–25,27–31
A main barrier is the applicability of evidence in general practice.13,14,17–19,27,30,31,34 The difference between primary care patients and the patients in the research population of secondary care is mentioned as a reason for this,17,24,27,34 which relates to the fact that research from clinical trials cannot be generalised to patients in general practice.18 As a result, GPs fear possible harm or side effects.17,19 Overall, GPs feel a lack of commitment to and ownership of the use of evidence,13 because the psychosocial context (treating patients rather than diseases) of general practice34 can make evidence irrelevant.18
The barrier relating to the busy workload in general practice is expressed in the time that is available to GPs.14,20,25 Time for using the concept of EBM is described in many studies as a barrier.15–17,19–21,23–25,28–31,33 A shortage of time during consultations does not allow GPs to search for,17 or access,19,26 evidence, and they do not have time to reflect on their clinical practice.26 Time to search for and appraise articles is specifically mentioned in a qualitative study as an important barrier:33 GPs in this study consider time a more important barrier than lack of skills.33 GPs state that they have trouble keeping up to date;13,15,17 this applies especially to GPs who practise alone.13
Furthermore, a lack of managerial or institutional support is mentioned as a barrier.20,27 A lack of investment by health authorities is particularly described in two survey studies.24,31 Some GPs consider EBM not to be cost effective for themselves as practitioners,31 and feel they require additional financial resources for the facilities needed when using EBM.26,30,33,34 To them, seeing patients is more cost effective than spending time in the field of EBM,27 since, in their opinion, time per patient increases when EBM is used.33 For GPs, there is no financial gain in using EBM,24,31 because time spent on EBM is not paid for.15
DISCUSSION
Summary
Consistent with the definition of EBM, all three components of EBM (and not only evidence) should be used in GPs’ decision-making.1 The majority of GPs consider EBM as a positive concept.24 However, over the years, many studies have revealed that barriers limit the use of EBM.7,8,45,46 The present review confirms that GPs also experience barriers that limit incorporation of the three aspects of EBM (evidence, the GP’s preferences, and patient preferences) and barriers related to the specific clinical setting of their work.
EBM in general practice
This review shows that time-related barriers can occur in each aspect of EBM and therefore affect the entire concept of EBM. It generally takes about 2 hours to thoroughly walk through all the steps of EBM when discussing a new clinical question.36 Doctors, however, generate about 45 questions every week and spend a maximum of 2–3 minutes to answer one question.47 Fortunately, not all questions are new and a significant amount of evidence has been summarised in guidelines, syntheses, and synopses, reducing the amount of time needed to answer a question.40 However, assessing evidence does still require time, and GPs need to overcome their lack of time — the main barrier found in this review — in order to be able to apply EBM.28
Barriers in the use of evidence-based medicine by GPs
The main barriers found in this review are similar to those found in other research articles about barriers experienced by GP trainees,8 doctors from other disciplines,45,46 or nurses.7 Considering primary care in particular, most research is performed in secondary care,47 and consequently there is a lack of evidence that is suitable for application in the clinical setting of general practice.30 Some GPs say they do not trust available evidence.48 This is not necessarily a bad thing, since guidelines are not meant to be unquestioningly accepted,49 although some trust is required to not dismiss all evidence as useless. So, although awareness of uncertainties in research is important, to understand the proper applicability,24 it should not lead to dismissal of all evidence, a concept called ‘clever nihilism’. Clever nihilism, a cynical attitude towards EBM, has been shown to occur in EBM learners when maturing from EBM-naïve to mature stages, and could have a major impact on the preparedness of GPs to learn the skills necessary and apply EBM in daily practice.50
The relatively uncommon finding of this review is that GPs feel a need for incentives for working in an evidence-based manner,27 because the infrastructure that is needed for EBM requires financial input,36 and practising EBM requires time that is not reimbursed.27,33 Therefore, incentives may help in maintaining enthusiasm.51
Strengths and limitations
The quality of the studies (Table 1) is adequate, although certainly not optimal, so the results and conclusions drawn from this review are derived from studies of moderate quality, and should be interpreted as such. In qualitative studies, this mainly entails lack of a description of how analyses were performed. In quantitative studies, more information about the selection and characteristics of the participants could have been given. A limit to this review is the inclusion of studies that were carried out using self-reported outcomes or self-composed and/or not validated questionnaires. The barriers expressed during these sessions and on these questionnaires may be biased by hesitation to express socially undesirable opinions or practices. This would, however, have resulted in an underestimation of the barriers mentioned, only reinforcing the need to address these barriers. Other surveys were based on widely-used instruments such as the questionnaire from McColl et al,24 which enhances the validity and comparability of results. The quality of research studies needs explicit consideration for future studies.
This review study has some limitations. The inclusion criteria involve the inclusion of studies describing barriers that are experienced when using more than one of the EBM steps. It was decided to include studies that address more than one EBM step, because the researchers were not interested in all the detailed barriers that limit the use of specific steps, but wanted to describe barriers limiting the use of the entire concept of EBM. The same goes for barriers using one specific guideline. These kind of detailed barriers are usually more related to the specific content of that guideline or disease than to the concept of EBM itself.
Another limitation is that articles that discuss barriers regarding the use of one guideline or one illness were excluded. This was done to avoid the inclusion of barriers that are related to practical or logistical aspects of that particular guideline or illness, in clinical practice. When looking at the studies that were excluded based on this exclusion criterion, it was found that the excluded studies mainly discuss barriers that are related to the use of medication (such as side effects and non-compliance),52 to working with guidelines (such as blending in with routine practice and particular skills in the practice of the physician),53 or to care planning (such as clinical factors and additional tasks).54 Some of the excluded studies describe barriers to the implementation of a guideline that are consistent with the barriers mentioned in this study, although their main focus is not on barriers that are experienced regarding the use of guidelines in general. Although some studies do describe general barriers regarding the use of EBM in practice, the barriers mentioned in these studies are not different from the barriers found with this review.
Only digital databases were searched; no other sources (such as abstract books or conference handouts) were considered. Searching these resources could have led to the identification of additional studies. The topic of this review, however, requires a thorough description of the questions asked and the answers given, which were expected not to be present in abstracts.
A very broad search was performed, as ‘evidence’ and ‘evidence-based medicine’ are commonly used as keywords. As a consequence, over 14 000 articles have been reviewed. An advantage of this broad search is that all possible articles were reviewed and therefore probably none were missed. The disadvantage is that working through the articles was very time consuming and, since the process started with a review of only the titles, an unjustified exclusion of articles could have occurred. A more specific search would, however, have led to relevant papers being overlooked.55 Using two or three reviewers for each stage has probably reduced the risk of missing relevant papers. However, when looking at the inter-rater agreement (kappa) of the abstract review, agreement is only fair (0.34). When taking a closer look at the cause of this poor kappa, it was found that the reason lies within the doubt about whether or not to include: some abstracts are hard to review and therefore were indicated by some reviewers with a question mark. In calculating kappa, all abstracts that were indicated with a question mark and that were seen by a third reviewer, were considered to show ‘disagreement between reviewers’, although the main cause was uncertainty, not disagreement.
Since, to the authors’ knowledge, no valid measure is available to assess the quality of observational studies, these studies were assessed using the recommendation of the STROBE initiative, as was done in earlier similar studies.10 As the STROBE statement was intended as a checklist when submitting a paper to a journal and not for reviewing the quality of papers, the validity of this checklist, although intuitively acceptable, has not been formally tested and could be debated.
The barriers were organised into categories. These categories were chosen according to the model of EBM (Figure 1) and the barriers were placed under the categories. However, some overlay may exist due to the fact that the categories are broad and some barriers are related to more components of the EBM model. Although the grouping of barriers with categories was sometimes discussed, this does not influence the overall outcomes of this review.
The articles that were found date from 1997 onwards. The large range in years of publication of studies included in this review could well have highlighted barriers that are now outdated. However, similar barriers were found in both the early and the later articles, indicating that most barriers still need to be eliminated (Table 3).
A final limitation is that the included articles are derived from various countries with their various healthcare settings. In the UK, for example, guidelines are important in answering clinical questions.56 Furthermore, movements within healthcare systems, such as current implementation of pay-for-performance, influence evidence-based decision making.57 Except for barriers in access that more isolated practices experience, no studies were found on differences in barriers that are experienced by GPs in the use of EBM in practice, or changes in outcomes over time. Barriers are not described for the individual GP in particular, although barriers may vary from GP to GP.
Implications for practice and research
Although some say that training in EBM should focus on improving the skills that are needed to find and use research information,30,58 others say that training GPs in EBM should focus on what is required by the learners.59 Only providing knowledge and skills does not lead to success, since the integration and, consequently, the behaviour of GPs has to be improved.60 Respecting the outcomes of this review, the best educational method is integrating learning with clinical practice within the context of decision-making.61 Either way, teaching the skills needed for each EBM step is required in order to be able to use EBM, and these skills are needed in order to provide evidence-based care.1
Further research in the area of EBM should focus on eliminating barriers to the use of EBM and on educational solutions and interventions for both formal education and practice. Adapting training to the needs of GPs would reduce the barriers found in this study. Although a lot still has to be accomplished at the level of knowledge and skills, the focus should also be on teaching GPs how, in clinical practice, to combine evidence, their own experience and preferences, and their patient’s preferences, and thereby overcome the barriers to the practice of EBM. Lastly, barriers towards the practice of EBM by GPs should be addressed at more levels than only the GPs themselves, as barriers related to factors other than the GP also limit their use of EBM. For instance, the influence of the media is stated as an important barrier when discussing evidence-based options with patients, and attention should be paid to the trustworthiness of the messages media broadcast.
Acknowledgments
We would like to thank Ms F van Etten, clinical librarian at the Academic Medical Center, for helping us with the development of the search strategy of our review.
Funding
Department of General Practice of the Academic Medical Center-University of Amsterdam.
Ethical approval
Approval was not required for this study.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
REFERENCES
- 1.Dawes M, Summerskill W, Glasziou P, et al. Second International Conference of Evidence-Based Health Care Teachers and Developers. Sicily statement on evidence-based practice. BMC Med Educ. 2005;5(1):1. doi: 10.1186/1472-6920-5-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sackett DL, Rosenberg WM, Gray JA, et al. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312(7023):71–72. doi: 10.1136/bmj.312.7023.71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Haynes RB, Devereaux PJ, Guyatt GH. Physicians’ and patients’ choices in evidence based practice. BMJ. 2002;324(7350):1350. doi: 10.1136/bmj.324.7350.1350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Krahn M, Naglie G. The next step in guideline development: incorporating patient preferences. JAMA. 2008;300(4):436–438. doi: 10.1001/jama.300.4.436. [DOI] [PubMed] [Google Scholar]
- 5.Tonelli MR. Integrating evidence into clinical practice: an alternative to evidence-based approaches. J Eval Clin Pract. 2006;12(3):248–256. doi: 10.1111/j.1365-2753.2004.00551.x. [DOI] [PubMed] [Google Scholar]
- 6.Tonelli MR. Integrating clinical research into clinical decision making. Ann Ist Super Sanita. 2011;47(1):26–30. doi: 10.4415/ANN_11_01_07. [DOI] [PubMed] [Google Scholar]
- 7.Solomons NM, Spross JA. Evidence-based practice barriers and facilitators from a continuous quality improvement perspective: an integrative review. J Nurs Manag. 2011;19(1):109–120. doi: 10.1111/j.1365-2834.2010.01144.x. [DOI] [PubMed] [Google Scholar]
- 8.Van Dijk N, Hooft L, Wieringa-de Waard M. What are the barriers to residents’ practising evidence-based medicine? A systematic review. Acad Med. 2010;85(7):1163–1170. doi: 10.1097/ACM.0b013e3181d4152f. [DOI] [PubMed] [Google Scholar]
- 9.Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet. 2003;362(9391):1225–1230. doi: 10.1016/S0140-6736(03)14546-1. [DOI] [PubMed] [Google Scholar]
- 10.Vandenbroucke JP, Von Elm E, Altman DG, et al. Iniciativa STROBE. [Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration] PloS Med. 2007;4(10):e297. doi: 10.1371/journal.pmed.0040297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Giacomini MK, Cook DJ. Users’ guides to the medical literature: XXIII. Qualitative research in health care A. Are the results of the study valid? Evidence-Based Medicine Working Group. JAMA. 2000;284(3):357–362. doi: 10.1001/jama.284.3.357. [DOI] [PubMed] [Google Scholar]
- 12.Dutch Cochrane Centre. Formulier II. Voor het beoordelen van een randomised controlled trial (RCT) [Form II. For the assessment of a randomized controlled trial]. http://dcc.cochrane.org/sites/dcc.cochrane.org/files/uploads/RCT.pdf (accessed 28 May 2012)
- 13.Cranney M, Warren E, Barton S, et al. Why do GPs not implement evidence-based guidelines? A descriptive study. Fam Pract. 2001;18(4):359–363. doi: 10.1093/fampra/18.4.359. [DOI] [PubMed] [Google Scholar]
- 14.Tracy CS, Dantas GC, Upshur RE. Evidence-based medicine in primary care: qualitative study of family physicians. BMC Fam Pract. 2003;4:6. doi: 10.1186/1471-2296-4-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hannes K, Leys M, Vermeire E, et al. Implementing evidence-based medicine in general practice: a focus group based study. BMC Fam Pract. 2005;6:37. doi: 10.1186/1471-2296-6-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Yew KS, Reid A. Teaching evidence-based medicine skills: an exploratory study of residency graduates’ practice habits. Fam Med. 2008;40(1):24–31. [PubMed] [Google Scholar]
- 17.Carlsen B, Norheim OF. ‘What lies beneath it all?’ — an interview study of GPs’ attitudes to the use of guidelines. BMC Health Serv Res. 2008;8:218. doi: 10.1186/1472-6963-8-218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mayer J, Piterman L. The attitudes of Australian GPs to evidence-based medicine: a focus group study. Fam Pract. 1999;16(6):627–632. doi: 10.1093/fampra/16.6.627. [DOI] [PubMed] [Google Scholar]
- 19.Oswald N, Bateman H. Treating individuals according to evidence: why do primary care practitioners do what they do? J Eval Clin Pract. 2000;6(2):139–148. doi: 10.1046/j.1365-2753.2000.00243.x. [DOI] [PubMed] [Google Scholar]
- 20.Sánchez López MC, de Torres MM, Sánchez Sánchez JA, et al. Qué pensamos los médicos de familia sobre la medicina basada en la evidencia? Un estudio con grupos focales. [What do general practitioners think about evidenced-based medicine? A study with focus groups] Aten Primaria. 2010;42(10):507–513. doi: 10.1016/j.aprim.2009.09.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chan GC, Teng CL. Primary care doctors’ perceptions towards evidence-based medicine in Melaka State: a questionnaire study. Med J Malaysia. 2005;60(2):130–133. [PubMed] [Google Scholar]
- 22.Gupta L, Ward JE, Hayward RS. Clinical practice guidelines in general practice: a national survey of recall, attitudes and impact. Med J Aust. 1997;166(2):69–72. doi: 10.5694/j.1326-5377.1997.tb138723.x. [DOI] [PubMed] [Google Scholar]
- 23.Butzlaff M, Vollmar HC, Floer B, et al. Learning with computerized guidelines in general practice? A randomized controlled trial. Fam Pract. 2004;21(2):183–188. doi: 10.1093/fampra/cmh214. [DOI] [PubMed] [Google Scholar]
- 24.McColl A, Smith H, White P, Field J. General practitioners’ perceptions of the route to evidence based medicine: a questionnaire survey. BMJ. 1998;316(7128):361–365. doi: 10.1136/bmj.316.7128.361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Cotton P, Sullivan F. Perceptions of guidelines in primary and secondary care: implications for implementation. J Integrated Care. 1999;3:79–83. [Google Scholar]
- 26.Taylor J, Wilkinson D, Blue IA, Dollard JT. Evidence-based rural general practice: barriers and solutions in South Australia. Rural Remote Health. 2002;2(1):116. [PubMed] [Google Scholar]
- 27.McKenna HP, Ashton S, Keeney S. Barriers to evidence-based practice in primary care. J Adv Nurs. 2004;45(2):178–189. doi: 10.1046/j.1365-2648.2003.02879.x. [DOI] [PubMed] [Google Scholar]
- 28.Upton D, Upton P. Knowledge and use of evidence-based practice of GPs and hospital doctors. J Eval Clin Pract. 2006;12(3):376–384. doi: 10.1111/j.1365-2753.2006.00602.x. [DOI] [PubMed] [Google Scholar]
- 29.Amin FA, Fedorowicz Z, Montgomery AJ. A study of knowledge and attitudes towards the use of evidence-based medicine among primary health care physicians in Bahrain. Saudi Med J. 2006;27(9):1394–1396. [PubMed] [Google Scholar]
- 30.Trevena LJ, Irwig L, Isaacs A, Barratt A. GPs want tailored, user friendly evidence summaries — a cross sectional study in New South Wales. Aust Fam Physician. 2007;36(12):1065–1069. [PubMed] [Google Scholar]
- 31.Barghouti F, Halaseh L, Said T, et al. Evidence-based medicine among Jordanian family physicians: awareness, attitude, and knowledge. Can Fam Physician. 2009;55(7):e6–13. [PMC free article] [PubMed] [Google Scholar]
- 32.Kahveci R, Meads C. Is primary care evidence-based in Turkey? A cross-sectional survey of 375 primary care physicians. J Evid Based Med. 2009;2(4):242–251. doi: 10.1111/j.1756-5391.2009.01050.x. [DOI] [PubMed] [Google Scholar]
- 33.Young JM, Ward JE. Evidence-based medicine in general practice: beliefs and barriers among Australian GPs. J Eval Clin Pract. 2001;7(2):201–210. doi: 10.1046/j.1365-2753.2001.00294.x. [DOI] [PubMed] [Google Scholar]
- 34.Freeman AC, Sweeney K. Why general practitioners do not implement evidence: qualitative study. BMJ. 2001;323(7321):1100–1102. doi: 10.1136/bmj.323.7321.1100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Haynes RB. Of studies, syntheses, synopses, summaries, and systems: the ‘5S’ evolution of information services for evidence-based health care decisions. ACP J Club. 2006;145(3):A8. [PubMed] [Google Scholar]
- 36.Rosenberg W, Donald A. Evidence based medicine: an approach to clinical problem-solving. BMJ. 1995;310(6987):1122–1126. doi: 10.1136/bmj.310.6987.1122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Robinson G, Gould M. What are the attitudes of general practitioners towards research? Br J Gen Pract. 2000;50(454):390–392. [PMC free article] [PubMed] [Google Scholar]
- 38.Greenhalgh T. Intuition and evidence — uneasy bedfellows? Br J Gen Pract. 2002;52(478):395–400. [PMC free article] [PubMed] [Google Scholar]
- 39.Gabbay J, le May A. Evidence based guidelines or collectively constructed ‘mindlines?’ Ethnographic study of knowledge management in primary care. BMJ. 2004;329(7473):1013. doi: 10.1136/bmj.329.7473.1013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Haynes RB, Devereaux PJ, Guyatt GH. Clinical expertise in the era of evidence-based medicine and patient choice. Vox Sang. 2002;83(suppl 1):383–386. [PubMed] [Google Scholar]
- 41.Rohrbacher R, Marx P, Schaufler T, Schneider H. Patient-based medicine: aligning patients’ perspectives on disease and treatment with evidence-based medicine criteria. J Publ Health. 2009;17(3):167–176. [Google Scholar]
- 42.Reeve J. Protecting generalism: moving on from evidence-based medicine? Br J Gen Pract. 2010;60(576):521–523. doi: 10.3399/bjgp10X514792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Katerndahl D, Wood R, Jaén CR. Family medicine outpatient encounters are more complex than those of cardiology and psychiatry. J Am Board Fam Med. 2011;24(1):6–15. doi: 10.3122/jabfm.2011.01.100057. [DOI] [PubMed] [Google Scholar]
- 44.Haynes RB, Devereaux PJ, Gyuatt GH. Physicians’and patients’ choices in evidence based practice. BMJ. 2002;324(7350):1350. doi: 10.1136/bmj.324.7350.1350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Knops AM, Vermeulen H, Legemate DA, Ubbink DT. Attitudes, awareness, and barriers regarding evidence-based surgery among surgeons and surgical nurses. World J Surg. 2009;33(7):1348–1355. doi: 10.1007/s00268-009-0020-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Mittal R, Perakath B. Evidence-based surgery: knowledge, attitudes, and perceived barriers among surgical trainees. J Surg Educ. 2010;67(5):278–282. doi: 10.1016/j.jsurg.2010.06.012. [DOI] [PubMed] [Google Scholar]
- 47.Jacobson LD, Edwards AG, Granier SK, Butler CC. Evidence-based medicine and general practice. Br J Gen Pract. 1997;47(420):449–452. [PMC free article] [PubMed] [Google Scholar]
- 48.Grol R. Has guideline development gone astray? Yes. BMJ. 2010;340:c306. doi: 10.1136/bmj.c306. [DOI] [PubMed] [Google Scholar]
- 49.Gibbons RJ, Antman EM, Smith SC. Has guideline development gone astray? No. BMJ. 2010;340:c343. doi: 10.1136/bmj.c343. [DOI] [PubMed] [Google Scholar]
- 50.Meserve C, Kalet A, Hanley K, et al. Clever nihilism: do cynics learn in an evidence based medicine course? Med Educ Online. 2005;10:4. doi: 10.3402/meo.v10i.4372. [DOI] [PubMed] [Google Scholar]
- 51.Wyatt JC, Sullivan F. Keeping up: learning in the workplace. BMJ. 2005;331(7525):1129–1132. doi: 10.1136/bmj.331.7525.1129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Hickling JA, Nazareth I, Rogers S. The barriers to effective management of heart failure in general practice. Br J Gen Pract. 2001;51(469):615–618. [PMC free article] [PubMed] [Google Scholar]
- 53.van der Weijden T, Grol RPTM, Schouten BJ, Knottnerus JA. Barriers to working according to cholesterol guidelines. Eur J Public Health. 1998;8(2):113–118. [Google Scholar]
- 54.Jiwa M, Freeman J, Fisher C, et al. Factors that impact on the application of guidelines in general practice: a review of medical records and structured investigation of clinical incidents in hypertension. Qual Prim Care. 2005;13(4):213–220. [Google Scholar]
- 55.Offringa M, Assendelft WJJ, Scholten RJPM. [Introduction to evidence-based medicine. Clinical treatment based on evidence.] 3rd edn. Houten: Bohn Stafleu van Loghum; 2010. Inleiding in evidence-based medicine. Klinisch handelen gebaseerd op bewijsmateriaal. [Google Scholar]
- 56.Davies K. Evidence-based medicine: is the evidence out there for primary care clinicians? Health Info Libr J. 2011;28(4):285–293. doi: 10.1111/j.1471-1842.2011.00954.x. [DOI] [PubMed] [Google Scholar]
- 57.Rosenthal MB, Frank RG, Li Z, et al. Experience with pay-for-performance. From concept to practice. JAMA. 2005;294(14):1788–1793. doi: 10.1001/jama.294.14.1788. [DOI] [PubMed] [Google Scholar]
- 58.Glasziou P, Burls A, Gilbert R. Evidence based medicine and the medical curriculum. BMJ. 2008;337:a1253. doi: 10.1136/bmj.a1253. [DOI] [PubMed] [Google Scholar]
- 59.Straus SE, Green ML, Bell DS, et al. Society of General Internal Medicine Evidence-Based Medicine Task Force. Evaluating the teaching of evidence based medicine: conceptual framework. BMJ. 2004;329(7473):1029–1032. doi: 10.1136/bmj.329.7473.1029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Coomarasamy A, Khan KS. A systematic review of postgraduate teaching in evidence-based medicine and critical appraisal. Med Teach. 2003;25(1):77–81. doi: 10.1080/0142159021000061468. [DOI] [PubMed] [Google Scholar]
- 61.Khan KS, Coomarasamy A. A hierarchy of effective teaching and learning to acquire competence in evidence-based medicine. BMC Med Educ. 2006;6:59. doi: 10.1186/1472-6920-6-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Green ML. Graduate medical education training in clinical epidemiology, critical appraisal, and evidence-based medicine: a critical review of curricula. Acad Med. 1999;74(6):686–694. doi: 10.1097/00001888-199906000-00017. [DOI] [PubMed] [Google Scholar]
- 63.Hyde C, Parkes J, Deeks J, Milne R. Systematic review of the effectiveness of teaching critical appraisal. Oxford: UK National R&D Programme: Evaluating Methods to Promote the Implementation of R&D; 2000. [Google Scholar]
- 64.Greenhalgh T, Macfarlane F. Towards a competency grid for evidence-based practice. J Eval Clin Pract. 1997;3(2):161–165. doi: 10.1046/j.1365-2753.1997.00082.x. [DOI] [PubMed] [Google Scholar]
- 65.Al-Almaie SM, AL-Baghli N. Barriers facing physicians practicing evidence- based medicine in Saudi Arabia. J Contin Educ Health Prof. 2004;24(3):163–170. doi: 10.1002/chp.1340240307. [DOI] [PubMed] [Google Scholar]
- 66.Al-Ansary LA, Khoja TA. The place of evidence-based medicine among primary health care physicians in Riyadh region, Saudi Arabia. Fam Pract. 2002;19(5):537–542. doi: 10.1093/fampra/19.5.537. [DOI] [PubMed] [Google Scholar]
- 67.Degner LF, Sloan JA, Venkatesh P. The control preferences scale. Can J Nurs Res. 1997;29:21–43. [PubMed] [Google Scholar]
- 68.Fedorowicz Z, Almas K, Keenan JV. Perceptions and attitudes towards the use of evidence-based dentistry (EBD) among final year students and interns at King Saud University, College of Dentistry in Riyadh, Saudi Arabia. Braz J Oral Sci. 2004;3:470–474. [Google Scholar]
- 69.Upton D, Lewis BK. Evidence based practice: a questionnaire to assess knowledge, attitudes and practice. British Journal of Therapy and Rehabilitation. 1998;5:647–650. [Google Scholar]
- 70.Funk SG, Champagne MT, Wiese AR, Tornquist ET. Barriers to using research finding in practice: the clinicians perspective. Appl Nurs Res. 1991;4:90–95. doi: 10.1016/s0897-1897(05)80062-x. [DOI] [PubMed] [Google Scholar]
- 71.Nylenna M, Gjerløw Aasland O. Physicians’ internet activities and their perceived coping with the medical information. Medscape General Medicine. 2000;2(1) [PubMed] [Google Scholar]
- 72.Young JM, Ward JE. General practitioners’ use of evidence databases. Med J Aust. 1999;170:56–58. [PubMed] [Google Scholar]
- 73.Young JM, Ward JE. Strategies to improve cancer screening in general practice: are guidelines the answer? Fam Pract. 1999;16:66–70. doi: 10.1093/fampra/16.1.66. [DOI] [PubMed] [Google Scholar]