

A 71-year-old woman presented with symptoms of dyspnea, cough, and fever. Chest radiography revealed interstitial infiltrates, which confirmed the diagnosis of pneumonia. In addition, a low-density mass adjacent to the right side of the heart was identified (Fig. 1). Chest computed tomography and transthoracic echocardiography indicated the presence of a mass of water-density opacity that was compressing the right atrium (Fig. 2). Cardiovascular magnetic resonance suggested a pericardial cyst, which usually presents as a homogeneous mass located in the right anterior cardiophrenic angle, with high signal intensity on T2-weighted images and low-to-intermediate signal intensity on T1-weighted images. Furthermore, there was no gadolinium enhancement, which confirmed the avascular and likely benign nature of the mass1 (Fig. 3). Because of the large size of the mass and its effect on the heart, the patient underwent video-assisted thoracoscopic excision of the mass, which was located in the right cardiophrenic angle, adjacent to the right atrium (Fig. 4A). Histologic examination confirmed that the mass was a pericardial cyst (Fig. 4B).
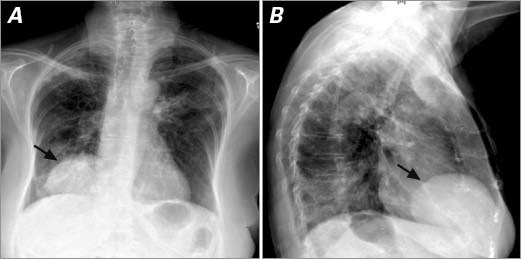
Fig. 1 Chest radiography. A) Posteroanterior and B) lateral views show a mass (arrow) in the right cardiophrenic angle. Patches of infiltrates are seen in both lung fields.
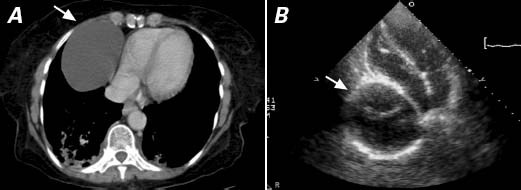
Fig. 2 A) Chest computed tomography (cross-section) and B) transthoracic echocardiography (apical 4-chamber view) show a large, unilocular, thin-walled structure (arrow) of water-density opacity, located lateral to the right atrium and compressing both the right atrium and the inferior vena cava.
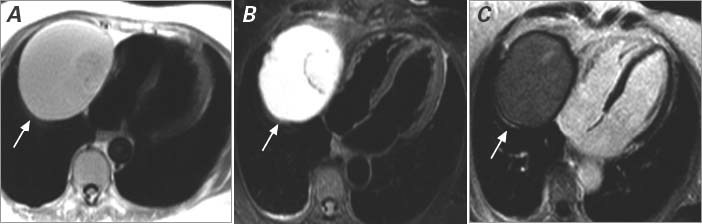
Fig. 3 Cardiovascular magnetic resonance shows a large, well-defined extracardiac mass (arrow) in the right cardiophrenic space, with partial compression of the right atrium and bowing of the interatrial septum to the left. A) A T1-weighted image and B) a T2-weighted image show a large mass that is hyperintense to the myocardium, indicative of significant water content. C) After administration of gadolinium, there was no enhancement of the mass, which suggested its avascular nature.
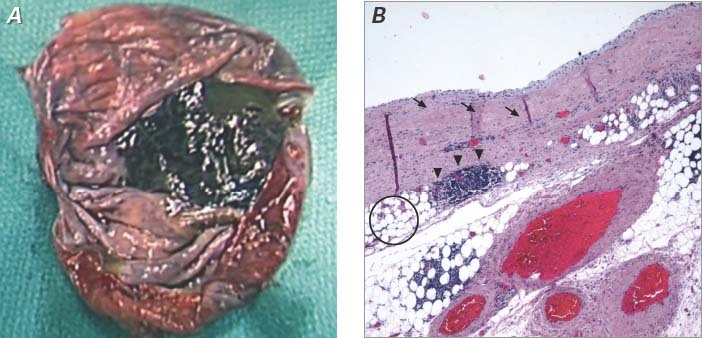
Fig. 4 Pathology specimen. A) Macroscopic view shows an oval-round cystic lesion (8 cm at largest diameter) filled with clear, watery fluid. B) Microscopic view shows that the cystic wall is composed of hypocellular fibroconnective tissue (arrows) with scattered lymphoid aggregates (arrowheads) and a substantial number of fat cells (circle). No malignant features are seen (H & E, orig. ×40).
Comment
Pericardial cysts affect 1 person in 100,000.2 Although they can occur anywhere in the mediastinum, they are typically found in the right cardiophrenic angle.1 Seventy-five percent of pericardial cysts have no associated symptoms and are incidental findings.2 Symptoms, if present, are usually due to compression of adjacent organs and include atypical chest pain, dyspnea, and persistent cough.2 Pericardial cysts can cause cardiac tamponade, obstruction of the right main stem bronchus, and sudden death.2,3 Treatment options include surgical resection or percutaneous aspiration of the cyst. However, when a typical, asymptomatic pericardial cyst is identified, it should be monitored by follow-up imaging, at 6- to 12-month intervals, until stability is established or the benign nature of the lesion is confirmed. Thereafter, in the absence of new symptoms, less frequent imaging seems reasonable, although there are not enough data on the outcomes of this uncommon condition.
Footnotes
Address for reprints: Su Min Chang, MD, The Methodist DeBakey Heart & Vascular Center, 6550 Fannin St., Suite 1901, Houston, TX 77030
E-mail: SMChang@tmhs.org
References
- 1.Wang ZJ, Reddy GP, Gotway MB, Yeh BM, Hetts SW, Higgins CB. CT and MR imaging of pericardial disease. Radiographics 2003;23 Spec No:S167–80. [DOI] [PubMed]
- 2.Patel J, Park C, Michaels J, Rosen S, Kort S. Pericardial cyst: case reports and a literature review. Echocardiography 2004; 21(3):269–72. [DOI] [PubMed]
- 3.Borges AC, Gellert K, Dietel M, Baumann G, Witt C. Acute right-sided heart failure due to hemorrhage into a pericardial cyst. Ann Thorac Surg 1997;63(3):845–7. [DOI] [PubMed]