

Executive Summary
In July 2010, the Medical Advisory Secretariat (MAS) began work on a Chronic Obstructive Pulmonary Disease (COPD) evidentiary framework, an evidence-based review of the literature surrounding treatment strategies for patients with COPD. This project emerged from a request by the Health System Strategy Division of the Ministry of Health and Long-Term Care that MAS provide them with an evidentiary platform on the effectiveness and cost-effectiveness of COPD interventions.
After an initial review of health technology assessments and systematic reviews of COPD literature, and consultation with experts, MAS identified the following topics for analysis: vaccinations (influenza and pneumococcal), smoking cessation, multidisciplinary care, pulmonary rehabilitation, long-term oxygen therapy, noninvasive positive pressure ventilation for acute and chronic respiratory failure, hospital-at-home for acute exacerbations of COPD, and telehealth (including telemonitoring and telephone support). Evidence-based analyses were prepared for each of these topics. For each technology, an economic analysis was also completed where appropriate. In addition, a review of the qualitative literature on patient, caregiver, and provider perspectives on living and dying with COPD was conducted, as were reviews of the qualitative literature on each of the technologies included in these analyses.
The Chronic Obstructive Pulmonary Disease Mega-Analysis series is made up of the following reports, which can be publicly accessed at the MAS website at: http://www.hqontario.ca/en/mas/mas_ohtas_mn.html.
Chronic Obstructive Pulmonary Disease (COPD) Evidentiary Framework
Influenza and Pneumococcal Vaccinations for Patients With Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Smoking Cessation for Patients With Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Community-Based Multidisciplinary Care for Patients With Stable Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Pulmonary Rehabilitation for Patients With Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Long-term Oxygen Therapy for Patients With Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Noninvasive Positive Pressure Ventilation for Acute Respiratory Failure Patients With Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Noninvasive Positive Pressure Ventilation for Chronic Respiratory Failure Patients With Stable Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Hospital-at-Home Programs for Patients With Acute Exacerbations of Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Home Telehealth for Patients With Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Cost-Effectiveness of Interventions for Chronic Obstructive Pulmonary Disease Using an Ontario Policy Model
Experiences of Living and Dying With COPD: A Systematic Review and Synthesis of the Qualitative Empirical Literature
For more information on the qualitative review, please contact Mita Giacomini at: http://fhs.mcmaster.ca/ceb/faculty_member_giacomini.htm.
For more information on the economic analysis, please visit the PATH website: http://www.path-hta.ca/About-Us/Contact-Us.aspx.
The Toronto Health Economics and Technology Assessment (THETA) collaborative has produced an associated report on patient preference for mechanical ventilation. For more information, please visit the THETA website: http://theta.utoronto.ca/static/contact.
Objective
The objective of this health technology assessment was to determine the effectiveness and cost-effectiveness of noninvasive ventilation for stable chronic obstructive pulmonary disease (COPD).
Clinical Need: Condition and Target Population
Noninvasive ventilation is used for COPD patients with chronic respiratory failure. Chronic respiratory failure in COPD patients may be due to the inability of the pulmonary system to coordinate ventilation, leading to adverse arterial levels of oxygen and carbon dioxide. Noninvasive ventilation in stable COPD patients has the potential to improve quality of life, prolong survival, and improve gas exchange and sleep quality in patients who are symptomatic after optimal therapy, have hypercapnia or nocturnal hypoventilation and mild hypercapnia, and are frequently hospitalized.
Technology
Noninvasive positive pressure ventilation (NPPV) is any form of positive ventilatory support without the use of an endotracheal tube. For stable COPD, the standard of care when using noninvasive ventilation is bilevel positive airway pressure (BiPAP). Bilevel positive airway pressure involves both inspiratory and expiratory pressure, high during inspiration and lower during expiration. It acts as a pressure support to accentuate a patient’s inspiratory efforts. The gradient between pressures maintains alveolar ventilation and helps to reduce carbon dioxide levels. Outpatients typically use BiPAP at night. Additional advantages of using BiPAP include resting of respiratory muscles, decreased work of breathing, and control of obstructive hypopnea.
Research Question
What is the effectiveness and cost-effectiveness of noninvasive ventilation, compared with no ventilation while receiving usual care, for stable COPD patients?
Research Methods
Literature Search
Search Strategy
A literature search was performed on December 3, 2010, using OVID MEDLINE, OVID MEDLINE In-Process and Other Non-Indexed Citations, OVID EMBASE, EBSCO Cumulative Index to Nursing & Allied Health Literature (CINAHL), the Wiley Cochrane Library, and the Centre for Reviews and Dissemination database for studies published from January 1, 2004 to December 3, 2010. Abstracts were reviewed by a single reviewer and, for those studies meeting the eligibility criteria, full-text articles were obtained. Reference lists were also examined for any additional relevant studies not identified through the search. When the reviewer was unsure of the eligibility of articles, a second clinical epidemiologist and then a group of epidemiologists reviewed these until consensus was reached.
Inclusion Criteria
full-text English language articles,
studies published between January 1, 2004 and December 3, 2010,
journal articles that report on the effectiveness or cost-effectiveness of noninvasive ventilation,
clearly described study design and methods, and
health technology assessments, systematic reviews, meta-analyses, randomized controlled trials (RCTs).
Exclusion Criteria
non-English papers
animal or in vitro studies
case reports, case series, or case-case studies
cross-over RCTs
studies on noninvasive negative pressure ventilation (e.g., iron lung)
studies that combine ventilation therapy with other regimens (e.g., daytime NPPV plus exercise or pulmonary rehabilitation)
studies on heliox with NPPV
studies on pulmonary rehabilitation with NPPV
Outcomes of Interest
mortality/survival
hospitalizations/readmissions
length of stay in hospital
forced expiratory volume
arterial partial pressure of oxygen
arterial partial pressure of carbon dioxide
dyspnea
exercise tolerance
health-related quality of life
Note: arterial pressure of oxygen and carbon dioxide are surrogate outcomes.
Statistical Methods
A meta-analysis and an analysis of individual studies were performed using Review Manager Version 5. For continuous data, a mean difference was calculated, and for dichotomous data, a relative risk ratio was calculated for RCTs. For continuous variables with mean baseline and mean follow-up data, a change value was calculated as the difference between the 2 mean values.
Quality of Evidence
The quality of each included study was assessed taking into consideration allocation concealment, randomization, blinding, power/sample size, withdrawals/dropouts, and intention-to-treat analyses.
The quality of the body of evidence was assessed as high, moderate, low, or very low according to the GRADE Working Group criteria. The following definitions of quality were used in grading the quality of the evidence:
| High | Further research is very unlikely to change confidence in the estimate of effect. |
| Moderate | Further research is likely to have an important impact on confidence in the estimate of effect and may change the estimate. |
| Low | Further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change the estimate. |
| Very Low | Any estimate of effect is very uncertain |
Summary of Findings
Conclusions
The following conclusions refer to stable, severe COPD patients receiving usual care.
Short-Term Studies
Based on low quality of evidence, there is a beneficial effect of NPPV compared with no ventilation on oxygen gas exchange, carbon dioxide gas exchange, and exercise tolerance measured using the 6 Minute Walking Test.
Based on very low quality of evidence, there is no effect of NPPV therapy on lung function measured as forced expiratory volume in 1 second (Type II error not excluded).
Long-Term Studies
Based on moderate quality of evidence, there is no effect of NPPV therapy for the outcomes of mortality, lung function measured as forced expiratory volume in 1 second, and exercise tolerance measured using the 6 Minute Walking Test.
Based on low quality of evidence, there is no effect of NPPV therapy for the outcomes of oxygen gas exchange and carbon dioxide gas exchange (Type II error not excluded).
Qualitative Assessment
Based on low quality of evidence, there is a beneficial effect of NPPV compared with no ventilation for dyspnea based on reduced Borg score or Medical Research Council dyspnea score.
Based on moderate quality of evidence, there is no effect of NPPV therapy for hospitalizations.
Health-related quality of life could not be evaluated.
Background
In July 2010, the Medical Advisory Secretariat (MAS) began work on a Chronic Obstructive Pulmonary Disease (COPD) evidentiary framework, an evidence-based review of the literature surrounding treatment strategies for patients with COPD. This project emerged from a request by the Health System Strategy Division of the Ministry of Health and Long-Term Care that MAS provide them with an evidentiary platform on the effectiveness and cost-effectiveness of COPD interventions.
After an initial review of health technology assessments and systematic reviews of COPD literature, and consultation with experts, MAS identified the following topics for analysis: vaccinations (influenza and pneumococcal), smoking cessation, multidisciplinary care, pulmonary rehabilitation, long-term oxygen therapy, noninvasive positive pressure ventilation for acute and chronic respiratory failure, hospital-at-home for acute exacerbations of COPD, and telehealth (including telemonitoring and telephone support). Evidence-based analyses were prepared for each of these topics. For each technology, an economic analysis was also completed where appropriate. In addition, a review of the qualitative literature on patient, caregiver, and provider perspectives on living and dying with COPD was conducted, as were reviews of the qualitative literature on each of the technologies included in these analyses.
The Chronic Obstructive Pulmonary Disease Mega-Analysis series is made up of the following reports, which can be publicly accessed at the MAS website at: http://www.hqontario.ca/en/mas/mas_ohtas_mn.html.
Chronic Obstructive Pulmonary Disease (COPD) Evidentiary Framework
Influenza and Pneumococcal Vaccinations for Patients With Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Smoking Cessation for Patients With Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Community-Based Multidisciplinary Care for Patients With Stable Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Pulmonary Rehabilitation for Patients With Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Long-term Oxygen Therapy for Patients With Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Noninvasive Positive Pressure Ventilation for Acute Respiratory Failure Patients With Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Noninvasive Positive Pressure Ventilation for Chronic Respiratory Failure Patients With Stable Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Hospital-at-Home Programs for Patients With Acute Exacerbations of Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Home Telehealth for Patients With Chronic Obstructive Pulmonary Disease (COPD): An Evidence-Based Analysis
Cost-Effectiveness of Interventions for Chronic Obstructive Pulmonary Disease Using an Ontario Policy Model
Experiences of Living and Dying With COPD: A Systematic Review and Synthesis of the Qualitative Empirical Literature
For more information on the qualitative review, please contact Mita Giacomini at: http://fhs.mcmaster.ca/ceb/faculty_member_giacomini.htm.
For more information on the economic analysis, please visit the PATH website: http://www.path-hta.ca/About-Us/Contact-Us.aspx.
The Toronto Health Economics and Technology Assessment (THETA) collaborative has produced an associated report on patient preference for mechanical ventilation. For more information, please visit the THETA website: http://theta.utoronto.ca/static/contact.
Objective of Analysis
The objective of this health technology assessment was to determine the effectiveness and cost-effectiveness of noninvasive ventilation (NIV) for stable chronic obstructive pulmonary disease (COPD).
Clinical Need and Target Population
Ventilation Therapy in Chronic Obstructive Pulmonary Disease
Noninvasive ventilation in stable COPD patients has the potential to improve quality of life, prolong survival, and improve gas exchange and sleep quality in patients who are symptomatic after optimal therapy, have arterial carbon dioxide levels greater than 55 mm Hg, or nocturnal hypoventilation and arterial carbon dioxide levels between 50 and 54 mm Hg, and are frequently hospitalized. One of the goals of long-term ventilation at home is to persistently reduce hypercapnia. The mechanism of action of NIV is not clear but may include respiratory muscle rest, restoration of chemosensitivity, improved compliance of the chest wall and lungs, improved sleep quality, and reduced respiratory system load. (1)
Noninvasive Positive Pressure Ventilation
Mechanical ventilation is used for COPD patients with chronic respiratory failure. Respiratory failure is found only in very severe stage 4 COPD, where the arterial pressure of oxygen is less than 60 mm Hg, with or without forced expiratory volume in 1 second (FEV1) less than 30% predicted (i.e., FEV1 < 50% with PaO2 < 60 mm Hg is also a criterion for stage 4 COPD). Therefore, respiratory failure in the absence of severe decreased lung function is a criterion for very severe COPD. Respiratory failure may lead to secondary effects on the heart, known as cor pulmonale or right heart failure. Patients at this stage are typically considered to have end-organ dysfunction related to COPD. (2) In type 1 respiratory failure, the arterial level of carbon dioxide is normal or low but the patient is in a state of hypoxemia. In type 2 respiratory failure, high levels of carbon dioxide (> 45 mm Hg) and low levels of oxygen (< 60 mm Hg) occur. In terms of pathophysiology of the respiratory system, type 1 respiratory failure may be due to failure of the lungs to provide adequate gas exchange, and type 2 respiratory failure may be due to the inability of the pulmonary system to coordinate ventilation. The clinical sign of chronic respiratory failure is shallow breathing. Respiratory failure can occur as acute, chronic, or acute-on-chronic failure. Acute-on-chronic respiratory failure occurs when there is acute deterioration of the pre-existing state of chronic respiratory failure. (3)
Ontario Context
In Ontario, ventilatory devices and positive airway pressure systems are covered under Respiratory Products of the Assistive Devices Program. There are no specific guidelines for their use; however, applicants must be assessed by a medical professional. (4) The Ventilator Equipment Pool (VEP) loans invasive (mechanical ventilators) and noninvasive positive airway (bilevel devices) systems to eligible individuals. The VEP, a Transfer Payment Agency of the Assistive Devices Program that operates out of the Kingston General Hospital, is a recycling pool that loans these devices until they are no longer required, at which time they are returned to VEP for recycling and reuse. Funding assistance is also provided for supplies when devices are used through VEP. (Personal communication, November 7, 2011) According to the VEP database, 263 patients were registered with a primary or secondary diagnosis of chronic bronchitis, emphysema, bronchiectasis, and chronic airway obstruction between 2005 and 2010. This may be an underestimate because diagnoses such as respiratory failure/respiratory insufficiency or hypoventilation are not captured in the VEP. (Personal communication, expert, February 2, 2011)
Technology
Noninvasive positive pressure ventilation (NPPV) is any form of positive ventilatory support without the use of an endotracheal tube. For stable COPD, the standard of care when using NIV is bilevel positive airway pressure (BiPAP). Bilevel positive airway pressure involves both inspiratory and expiratory positive airway pressures, high pressure during inspiration and lower pressure during expiration. This acts as a pressure support to accentuate a patient’s inspiratory efforts. The gradient between these pressures maintains alveolar ventilation and helps to reduce arterial carbon dioxide levels. Additional advantages may include resting of respiratory muscles, decreased respiratory system load (work of breathing), control of obstructive hypopnea, and improved quality of sleep. It is typically used at night in outpatients. Other indications for use include obstructive sleep apnea with continuous positive airway pressure (CPAP) intolerance, obstructive sleep apnea with central sleep apnea, restrictive thoracic disorders, and obesity-hypoventilation syndrome with coexisting obstructive sleep apnea and residual hypoventilation despite CPAP.
Continuous positive airway pressure technology is not indicated for COPD; it simply acts to splint the airway open. Bilevel positive airway pressure applies a constant level of positive pressure during spontaneous breathing. When the BiPAP technology is set at 2 cm H2O for inspiratory and expiratory settings, the BiPAP system capabilities for COPD patients is equivalent to CPAP technology; in other words, there is no ventilation support for COPD patients at these settings due to the lack of a pressure gradient. (5) (Personal communication, clinical expert, March 3, 2011)
Evidence-Based Analysis
Research Question
What is the effectiveness and cost-effectiveness of NIV, compared with no ventilation while receiving usual care, for stable COPD patients?
Research Methods
Literature Search
Search Strategy
A literature search was performed on December 3, 2010, using OVID MEDLINE, OVID MEDLINE In-Process and Other Non-Indexed Citations, OVID EMBASE, EBSCO Cumulative Index to Nursing & Allied Health Literature (CINAHL), the Wiley Cochrane Library, and the Centre for Reviews and Dissemination database, for studies published from January 1, 2004 to December 3, 2010. Abstracts were reviewed by a single reviewer and, for those studies meeting the eligibility criteria, full-text articles were obtained. Reference lists were also examined for any additional relevant studies not identified through the search. When the reviewer was unsure of the eligibility of articles, a second clinical epidemiologist and then a group of epidemiologists reviewed these until consensus was reached.
Inclusion Criteria
full-text English language articles
studies published between January 1, 2004 and December 3, 2010
journal articles that report on the effectiveness or cost-effectiveness
study design and methods must be clearly described
health technology assessments, systematic reviews, meta-analyses, randomized controlled trials (RCTs)
Exclusion Criteria
non-English papers
animal or in vitro studies
case reports, case series, or case-case studies
cross-over RCTs
studies using noninvasive negative pressure ventilation (e.g., iron lung)
studies that combine ventilation therapy with other regimens (e.g., daytime NPPV plus exercise or pulmonary rehabilitation)
studies on heliox with NPPV
studies on pulmonary rehabilitation with NPPV
Outcomes of Interest
mortality/survival
hospitalizations
length of stay in hospital
forced expiratory volume (FEV1)
arterial partial pressure of oxygen (PaO2)
arterial partial pressure of carbon dioxide (PaCO2)
dyspnea
exercise tolerance
health-related quality of life (HRQOL)
Note: arterial pressure of oxygen and carbon dioxide are surrogate outcomes.
Statistical Analysis
A meta-analysis and an analysis of individual studies were performed using Review Manager Version 5. (6) For continuous data a mean difference was calculated, and for dichotomous data a relative risk ratio was calculated for RCTs. For continuous variables with mean baseline and mean follow-up data, a change value was calculated as the difference between the 2 mean values (e.g., follow-up minus baseline). A standard deviation that accounts for the baseline standard deviation and follow-up standard deviation was calculated from 3 parameters: baseline standard deviation, follow-up standard deviation, and a correlation coefficient. The correlation coefficient represents the strength of the relationship between the 2 standard deviations. A correlation coefficient of 0.5 was used for this analysis. Graphical display of the forest plots was also examined. A P value of less than 0.05 was considered statistically significant. P values in the text have been rounded to 3 decimal places.
Quality of Evidence
The quality of each included study was assessed taking into consideration the following 7 study design characteristics:
adequate allocation concealment,
randomization (study must include a description of the randomization procedure used and must be a proper method),
power/sample size (adequate sample size based on a priori calculations, underpowered studies were identified, when possible, using post hoc sample size power calculations),
blinding (if double blinding is not possible, a single blind study with unbiased assessment of outcome was considered adequate for this criterion),
< 20% withdrawals/dropouts,
intention-to-treat (ITT) analysis conducted and done properly (withdrawals/dropouts considered in analysis), and
other criteria as appropriate for the particular research question and study design.
The quality of the body of evidence was assessed as high, moderate, low, or very low according to the GRADE Working Group criteria (7) as presented below.
Quality refers to the criteria such as the adequacy of allocation concealment, blinding, and follow-up.
Consistency refers to the similarity of estimates of effect across studies. If there are important and unexplained inconsistencies in the results, our confidence in the estimate of effect for that outcome decreases. Differences in the direction of effect, the magnitude of the difference in effect, and the significance of the differences guide the decision about whether important inconsistency exists.
Directness refers to the extent to which the interventions and outcome measures are similar to those of interest.
As stated by the GRADE Working Group, (8) the following definitions of quality were used in grading the quality of the evidence:
| High | Further research is very unlikely to change confidence in the estimate of effect. |
| Moderate | Further research is likely to have an important impact on confidence in the estimate of effect and may change the estimate. |
| Low | Further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change the estimate. |
| Very Low | Any estimate of effect is very uncertain. |
Results of Evidence-Based Analysis
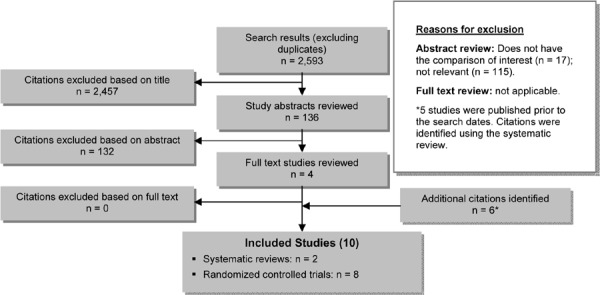
The database search yielded 2,593 studies published between January 1, 2004 and December 3, 2010, of which 3 studies and 1 systematic review met the inclusion criteria (Table 1). An additional 5 citations were identified using the systematic review. (9) An additional citation was identified from review of reference lists. Overall, there were 10 eligible studies.
Table 1: Body of Evidence Examined According to Study Design*.
| Study Design | Number of Eligible Studies† |
|---|---|
| RCT Studies | |
| Systematic review of RCTs | 2 |
| Large RCT† | - |
| Small RCT | 8 |
| Observational Studies | |
| Systematic review of non-RCTs with contemporaneous controls | - |
| Non-RCT with contemporaneous controls | - |
| Systematic review of non-RCTs with historical controls | - |
| Non-RCT with historical controls | - |
| Database, registry, or cross-sectional study | - |
| Case series | - |
| Retrospective review, modelling | - |
| Studies presented at an international conference or other sources of grey literature | - |
| Expert opinion | - |
| Total | 10 |
Abbreviation: RCT, randomized controlled trial.
Some citations identified were prior to the literature search dates.
Large RCT ≥ 150 subjects.
Figure 1: Citation Flow Chart.
For each included study, the study design was identified and is summarized below in Table 1, which is a modified version of the hierarchy of study design by Goodman. (10)
Systematic Reviews
A Cochrane systematic review and meta-analysis was performed to determine the effect of nocturnal NPPV using a nasal mask for at least 5 hours nightly for at least 3 consecutive weeks in patients with COPD. The relevant measured outcomes were blood gases, exercise tolerance, dyspnea, and HRQOL. The Cochrane analysis included 4 studies (years 1991−2000), 2 of which were cross-over designs and 2 of which were parallel RCT designs. The authors of the included studies reported that there were a high number of dropouts as a result of patients not tolerating the nose mask, getting infections, or no longer meeting the inclusion criteria of the individual studies. No effect of ventilation was shown for FEV1, forced vital capacity, PaO2, PaCO2, and the 6 Minute Walking Test (6MWT test) in standard Cochrane analyses examining the mean difference of change values. There was no effect for these outcome measures when examined among the subset of parallel studies (significant results were shown for outcome measures that were not relevant for this analysis, e.g., maximum inspiratory pressure). The risk of bias scored low for all included studies. The results of the studies may have been affected by low inspiratory pressures, the extent of nocturnal hypoventilation (with studies of COPD patients with more severe hypercapnia showing the greatest improvement in daytime hypercapnia), and differences in training techniques. All studies used nocturnal BiPAP. The small sample size (< 10 subjects) may have also been a limiting factor. (11)
A systematic review and meta-analysis was performed to determine the effectiveness of bilevel NPPV in chronic respiratory failure in severe, stable COPD patients. The relevant outcome measures examined were gas exchange, lung function, dyspnea, exercise tolerance, morbidity, and HRQOL. (The outcome measures not relevant here are not discussed.) Eligible studies were categorized as RCTs and non-RCTs, with no restrictions on how bilevel NPPV was used or length of follow-up. The search strategy included the years 2001 to 2003. The majority of studies rated high on methodological quality. For RCTs, ventilation did not affect PaO2, PaCO2, FEV1 (data not shown), 6MWT (data not shown), mortality (data not shown), and morbidity (e.g., hospital and intensive care unit admissions), with data not meta-analyzed for morbidity due to different units of measurement (data not shown). A beneficial effect of ventilation was shown for dyspnea, although the data for dyspnea were not meta-analyzed due to different measurement scales, and HRQOL measured using St. George’s Respiratory Questionnaire (SGRQ) in a single study, which was also not meta-analyzed. Only follow-up data were analyzed. A majority of studies included in the systematic review were also eligible for this report. (9)
The parallel design RCTs included in the Cochrane Review (11) were also included in the more recent systematic review (9) discussed above.
Randomized Controlled Trials
There were 5 parallel RCTs (12-16) identified from the most recent systematic review (9) and 3 parallel RCTs (17-19) identified from the literature search. Appendix 3 (Tables A3 to A8) summarizes the studies and their characteristics. The terms NPPV and NIV are used interchangeably. No studies refer to the iron lung.
A multicentre parallel RCT conducted in Australia across 4 university hospitals compared nocturnal NIV plus long-term oxygen therapy (LTOT) to LTOT alone. Patients were included if they were aged less than 80 years; had severe COPD (FEV1 < 50%) and stable hypercapnia (PaCO2 > 46 mm Hg); had used LTOT for at least 3 months; and were not currently smoking. Patients were excluded if they had severe comorbidities (e.g., malignancy, left ventricular heart failure, unstable angina) that could affect the completion of the study; severe psychiatric disorder that affected use of the technology; body mass index (BMI) greater than 40 kg/m2; and sleep apnea (> 20 episodes of apnea + hypopnea per hour of sleep). Patients with sleep apnea or obesity may have previously required the intervention and thus could no longer be randomized to a non-treatment group. Additionally, excluding individuals with sleep apnea or obesity helped to produce a more homogeneous COPD study population. The generalizability of the study results is high with respect to other populations with similarly severe COPD. The outcome measures of interest examined included mortality, hospitalizations, gas exchange, lung function, and HRQOL. Arterial blood gases were taken on room air. Follow-up was up to 5 years. A central study coordinator generated a random sequence of treatment assignments, stratified by centre and distributed in blocks of 10 sealed opaque envelopes to centres. Patients assigned to NIV were educated and familiarized with the equipment. Data were presented in a useable form for mortality only. Data on hospitalizations were given as the number of days in hospital per days on trial; data on PaCO2 and FEV1 were given, but without standard deviations; data on PaO2 were missing; and data on HRQOL based on SGRQ were not provided but only described in the text. (Additional information on Short Form-36 health survey was provided but not included in this analysis since it is not one of the outcome measures.) (19)
A parallel RCT that included patients from university specialists’ clinics in Canada compared nocturnal NIV to sham therapy. Willing patients aged 40 years or more who had a history of smoking were included in the trial if they had a clinical diagnosis of COPD (FEV1 < 70%). Patients were excluded if they had other medical conditions that could affect survival, cognitive impairment that could affect consent, left ventricular heart failure, and apnea-hypopnea (index ≥ 20 on a home-based sleep apnea test). The outcome measures of interest examined included gas exchange, lung function, and exercise-tolerance. Arterial blood gases were taken on room air. Randomization occurred at a central site. Personnel blinded to each patient’s type of treatment assessed and interpreted the outcome measures. All patients received standard medical therapy and NIV training. Sham therapy was CPAP set at 4 cm H2O. Data were presented in a useable form for the 6MWT only. There was some description of the results for PaCO2 and A parallel laboratory-based RCT that included patients from an outpatient clinic in Chile compared active diurnal NIV to sham therapy. Patients were included in the trial if they had stable COPD with hypercapnia (PaCO2 ≥ 50 mm Hg) and hypoxemia (< 60 mm Hg). They were excluded if they experienced either airway improvement or clinical exacerbation upon bronchodilation and had obstructive sleep apnea and comorbidities including left ventricular failure, peripheral vascular occlusive disease, and orthopedic disorder. Patients were nonsmokers and were using LTOT. Outcome measures of interest examined included gas exchange, lung function, dyspnea, and exercise tolerance. Arterial blood gases were taken while resting. Patients were randomly allocated to the study or the control using a table of random numbers and sealed envelopes. The treating physicians and personnel supervising the dyspnea and exercise tolerance tests were blinded to the type of treatment. Sham therapy was CPAP set at 2 cm H2O. Ventilation was provided under direct supervision. Data were provided in a suitable format for PaO2, PaCO2, FEV1, 6MWT, and Borg score. (17)
A multicentre parallel RCT conducted in Italy and France compared NIV plus LTOT to LTOT alone. Patients aged less than 76 years diagnosed with severe, stable COPD (FEV1 < 1.5 L) were included in the trial if they experienced chronic ventilatory failure (PaCO2 > 50 mm Hg); had used LTOT for at least 6 months; had an Medical Research Council (MRC) dyspnea score of 2 or higher; and had hypoxemia (PaO2 < 60 mm Hg). Excluded were smokers who experienced airway improvement upon bronchodilation; had sleep apnea (apnea-hypopnea index > 10 episodes per hour during polysomnography); were being treated with systemic steroids; had concomitant chronic systemic diseases (e.g., chronic heart failure, diabetes) and infections, neoplasms, other chronic respiratory disease (including fibrothorax, bronchiectasis, and cystic fibrosis); and were previously using NIV or LTOT. All outcome measures of interest were examined. All patients received standard medical treatment. Arterial blood gases were taken while resting and on oxygen. A centralized randomization procedure was used. Outcome measurements were performed by personnel blinded to treatment and not involved in the study. Data were provided in a suitable format for mortality, FEV1, and 6MWT. Results shown in graph form only for PaO2, PaCO2, dyspnea, and SGRQ were difficult to extrapolate (i.e., small scale). Data provided for hospitalizations used number of patients per year as the unit of analysis, which was not suitable for the meta-analysis. (16)
Another parallel laboratory-based RCT that was conducted in Chile included patients from an outpatient clinic and compared active diurnal NIV to sham therapy. Stable COPD patients who were nonsmoking and using LTOT were included in the trial if they had hypercapnia (PaCO2 ≥ 50 mm Hg) and hypoxemia (< 60 mm Hg). Patients were excluded if their airways improved upon bronchodilation; they experienced a clinical exacerbation; they were obese (BMI ≥ 30 kg/m2); they had a history of asthma and of obstructive sleep apnea; and they had comorbidities including left ventricular failure and bronchiectasis. Outcome measures of interest examined included gas exchange and lung function. Arterial blood gases were taken while resting. Patients were randomly allocated using a table of random numbers. Outcome measures were determined by trained nurses unaware of the purpose of the study. Sham therapy was CPAP set at 2 cm H2O. Ventilation was supervised. Data were provided in a suitable format for PaO2, PaCO2, and FEV1. (14)
A parallel RCT conducted in the Canary Islands compared nocturnal NIV to usual care. Stable patients with severe COPD (FEV1 < 45%) from 2 pulmonary clinics were included in the trial if they were aged 45 to 75 years and had a smoking history (> 20 pack-years). They were excluded if bronchodilation improved their airways; they refused to stop smoking; and they had sleep apnea (> 10 apnea-hypopnea episodes per hour), other etiologies of chronic airway obstruction (e.g., bronchiectasis, cystic fibrosis), and comorbidities (e.g., left ventricular failure). Outcome measures of interest included mortality, hospitalizations, gas exchange, lung function, and dyspnea. Patients were receiving supplemental oxygen.
Arterial blood gases were taken at rest. Patients were randomized by an independent office using a table of random numbers. Data were provided in a suitable format for mortality, PaO2, PaCO2, and FEV1. Data without standard deviations were extrapolated from the graph for hospitalizations, and point estimates without standard deviations were provided for dyspnea measures. As a result, these data could not be meta-analyzed. (13)
A parallel RCT used a United States pulmonary function laboratory database of patients seen during routine clinical assessments. This trial compared nocturnal NIV to sham therapy. Included in the trial were clinically nonobese (BMI < 30 kg/m2) stable patients aged less than 80 years with severe COPD (FEV1 < 40%) and hypercapnia (PaCO2 > 45 mm Hg). Excluded were patients who were being treated with sedatives or hypnotic medications; had had lung transplantation; were currently using nocturnal ventilation or CPAP; and had major illnesses that would preclude completion of the clinical trial. Outcome measures of interest included lung function and exercise tolerance. Supplemental oxygen was used according to prior physician prescription. Patients were randomized. Sham therapy was provided using the same equipment as used for the intervention group (e.g., BiPAP), without the use of an inspiratory setting and at the lowest expiratory setting. Data were in a suitable format for 6MWT, though FEV1 data were in litres and therefore not analyzed. (15)
A parallel RCT conducted using the medical records of a pulmonary function laboratory compared NIV to sham therapy. Patients were included in the trial if they had stable, severe COPD (FEV1 < 50%). They were excluded if they had congestive heart failure, asthma, lung cancer, thoracic cage abnormalities, prior thoracic surgery, restrictive pulmonary disease, obstructive sleep apnea, and degenerative joint disease. Also excluded were those who had had an exacerbation within the preceding 6 weeks. Outcome measures of interest included gas exchange, dyspnea, and exercise tolerance. Arterial blood gases were taken at rest while patients were breathing air or home oxygen. Patients were randomized. Sham therapy was provided using the same equipment as used by the intervention group (e.g., BiPAP) with inspiratory and expiratory pressures set at the minimum of 2 cm H2O. None of the data were available in a suitable format for meta-analysis. (12)
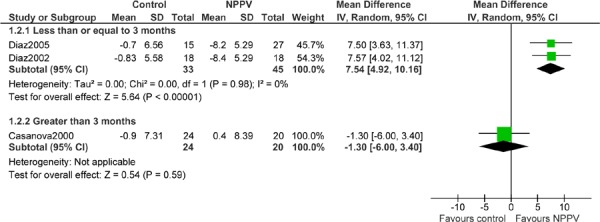
Meta-Analysis
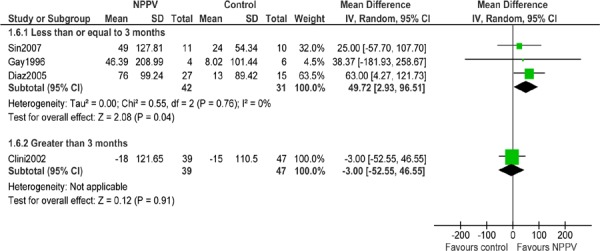
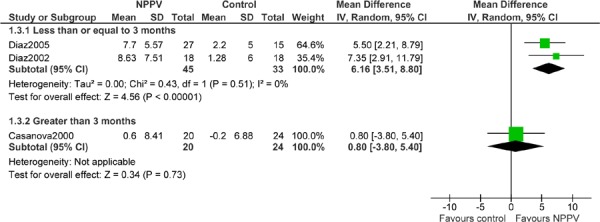
An analysis was performed to address the following research question: What is the effectiveness of noninvasive ventilation compared with no ventilation, while receiving usual care, for stable COPD patients? The potential outcomes examined were mortality, hospitalizations, FEV1, PaO2, PaCO2, dyspnea, exercise tolerance, and HRQOL. The gas exchange measures were considered surrogate outcomes. From among the 8 eligible studies, suitable data were found for mortality, FEV1, PaO2, PaCO2, and 6MWT. The outcome measures of hospitalizations, dyspnea, and HRQOL were analyzed qualitatively. The authors were contacted for their data but these were not received or, in one instance, the data were received in a format that was still unsuitable for analysis. For FEV1, PaO2, PaCO2, and 6MWT, the results shown (Figures 2 to 6) are for change values that make use of the maximum amount of data (e.g., compared with analysis on follow-up data only). Change was calculated as the difference between the mean baseline value and the mean follow-up value. Due to the different lengths of follow-up and the possibility of clinical heterogeneity, where possible, data were examined in subgroups based on the length of follow-up as less than or equal to 3 months (i.e., short-term), 4 to 11 months, or greater than or equal to 12 months (i.e., long-term). (Personal communication, clinical expert, March 8, 2011) The estimates for FEV1, PaO2, PaCO2, and 6MWT were interpreted as the change over time (≤ 3 months vs. > 3 months) for a given factor. The interpretation of the results differs based on the direction of change and the outcome measure. A positive change over time is favourable for FEV1, PaO2, and 6MWT, suggesting an increase in respiratory capacity; a negative change over time is favourable for PaCO2, suggesting a decrease in an adverse respiratory factor. For mortality, the presentation of the analysis defines a beneficial effect of NPPV compared with no ventilation (i.e., the control) as an increased risk for the group of no ventilation (i.e., relative risk > 1).
Figure 2: Mortality (Number of Events) – All Studies With Follow-up Greater Than 3 Months*,†, ‡.
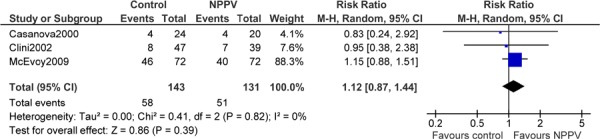
Figure 6: Six Minute Walking Test (Metres)*,†,‡.
Abbreviations: CI, confidence intervals; hrs, hours; IPAP, inspiratory positive airway pressure; IV, inverse variance; NPPV, noninvasive positive pressure ventilation; SD, standard deviation.
For consistency, a beneficial effect of NPPV is shown on the right-hand side of the zero line of the forest plots, and a negative effect on the left-hand side.
Figure 3: Forced Expiratory Volume in 1 Second (% Predicted)*,†,‡,

Abbreviations: CI, confidence interval; hrs, hours; IPAP, inspiratory positive airway pressure; IV, inverse variance; NPPV, noninvasive positive pressure ventilation; SD, standard deviation.
Figure 4: Arterial Pressure of Oxygen (mm Hg)*,†,‡.
Abbreviations: CI, confidence interval; hrs, hours; IPAP, inspiratory positive airway pressure; IV, inverse variance; NPPV, noninvasive positive pressure ventilation; SD, standard deviation.
Figure 5: Arterial Pressure of Carbon Dioxide (mm Hg)*,†,‡.
Abbreviations: CI, confidence interval; hrs, hours; IPAP, inspiratory positive airway pressure; IV, inverse variance; NPPV, noninvasive positive pressure ventilation; SD, standard deviation.
Results of Meta-Analysis
The results of the analyses are shown in Figures 2 to 6. Noninvasive positive pressure ventilation had a short-term beneficial effect on PaO2 (mean difference [MD], 6.16; 95% CI, 3.51-8.80 mm Hg; P < 0.001); PaCO2 (MD, 7.54; 95% CI, 4.92-10.16 mm Hg; P < 0.001); and 6MWT (MD, 49.72; 95% CI, 2.93−96.51 m; P = 0.04). The result for the 6MWT was statistically significant and clinically relevant (minimally clinically important difference: 25−54 m). (20-22) Although the results for PaO2 and PaCO2were statistically significant, the point estimate did not meet the minimum for clinical relevance, a change of at least 10 mm Hg. (Personal communication, clinical expert, April 14, 2011) However the gas exchange measures are considered surrogate outcomes. Noninvasive positive pressure ventilation had no effect on FEV1 in the short term.
Noninvasive positive pressure ventilation did not have any long-term effect on mortality, FEV1, PaO2, PaCO2, or 6MWT.
Qualitative Assessment
Some studies examined the outcomes of interest but did not have data suitable for a meta-analysis. In that case, or if there was only one study that had data suitable for meta-analysis for a given outcome, these were assessed qualitatively in aggregate by outcome, as shown below.
Hospitalizations
Two studies had information on hospitalizations. These showed no overall effect of NPPV on hospitalizations. McEvoy et al (19) found no difference between NPPV and usual care based on days in hospital and days on trial (rate ratio, 0.96; 95% CI, 0.90−1.02; P = 0.16). Casanova et al (13) found no differences in the number of hospital admissions between the NPPV group and usual care at the 12-month follow-up (both ~ 20%); however, there was an apparent difference between the groups at 3 months (treatment group [TR]: ~ 5% vs. control [CT]: ~ 15%), although the statistical significance for both were not reported. The 2 studies had different lengths of follow-up (5 years vs. 3 and 12 months), and characterized hospitalizations differently, which precluded a meta-analysis.
Dyspnea
Four studies had information on dyspnea. Overall, there was a beneficial effect of NPPV therapy on dyspnea as indicated by a reduction in Borg score or MRC dyspnea score for the NPPV group compared with the control group. Diaz et al (17) found an increased reduction in Borg score between baseline and follow-up at 3 weeks in the NPPV group compared with the no ventilation group when assessed during walking (TR: −1.5 vs. CT: −0.1; P < 0.001). Clini et al (16) found that MRC dyspnea score decreased in the NPPV group compared with usual care at the 2-year follow-up, indicating improved dyspnea (P = 0.01). This information was reported in graph format only. Casanova et al (13) found no difference between the NPPV group and usual care in the mean MRC dyspnea score at the 6-month follow-up (TR: 2 vs. CT: 2). In the same study, the NPPV group showed a statistically significant higher level of dyspnea when measured on the Borg scale (TR: 5 vs. CT: 4; P = 0.03). However, no standard deviations were provided. In Renston et al (12) the NPPV group showed a decreased modified Borg score in arbitrary units (data in graph format) and a decreased MRC dyspnea score at 5 days of follow-up compared with no ventilation (TR: 2.6, standard deviation [SD]: 0.5 vs. CT: 3.3, SD: 0.4; P not given), suggesting improved dyspnea for the NPPV group. Dyspnea tests were administered with participants at rest in all the studies except Diaz et al. (17) The 2 short-term studies with 5 days (12) and 3 weeks (17) of follow-up characterized their outcome measures differently, which precluded a meta-analysis. For the 2 long-term studies with 6 months (13) and 2 years (16) of follow-up, there were insufficient data to perform a meta-analysis.
The 2007 systematic review (9) examined dyspnea, and additional data were available. Review of these found there was information from one study on MRC dyspnea scores (16) that could be combined with data presented in the original paper of another study. (12) However, since the data for these studies were for 2 years (long-term) and 5 days (short-term) of follow-up, respectively, a meta-analysis was not performed.
Health-Related Quality of Life
Although 2 studies included HRQOL among their outcome measures, the data were not substantial enough to form a conclusion. McEvoy et al (19) found no difference between NPPV and usual care groups; however, they did not show the data for this outcome measure. Clini et al (16) found improved scores at the 2-year follow-up; however, there was no significant difference between the NPPV and usual care groups (P not given). Data were presented in a graph.
The results of the studies are summarized in Appendix 3, Tables A3 to A5. The consistency of the qualitative assessment of the evidence is summarized in Appendix 3, Table A7.
Summary of the Literature Review
The results of this evidence-based analysis show short-term beneficial effects of NPPV on oxygen and carbon dioxide levels and on exercise tolerance. There was no short-term beneficial effect of NPPV on FEV1. However, because the primary sample size calculation was not for FEV1, type II error cannot be excluded. There were no long-term beneficial effects of NPPV on mortality, FEV1, oxygen levels, carbon dioxide levels, and exercise tolerance. The qualitative assessment indicated a beneficial effect of NPPV on breathlessness but no effect on hospitalizations. The data on HRQOL were not substantial enough to form a conclusion.
From the 8 studies included, 5 used nocturnal NPPV (13;15;16;18;19) and 3 used diurnal NPPV therapy. (12;14;17) Of the 3 studies that used diurnal NPPV therapy, 2 were predominately based in pulmonary laboratories where NPPV use was closely supervised. (14;17) The studies that used nocturnal NPPV were not directly observed. Increased quality assurance would be expected in a laboratory environment. (Personal communication, clinical expert, March 23, 2011) All studies included no ventilation as the comparator, with 3 studies using CPAP (14;17;18) and 2 studies using BiPAP without a pressure gradient. (12;15) These “sham therapy” types of studies were designed to minimize a placebo effect for the patient and to ensure personnel were blinded to treatment. However, the CPAP equipment differs from the BiPAP equipment, as do the settings for use: the BiPAP equipment cycles audibly between high inspiratory and low expiratory settings, which are likely to be noticed. Some studies indicated in their methods that the personnel performing the outcome assessment were blinded to the allocation of treatment or the research question. (14;16-18) The 2 studies that used BiPAP equipment as the comparator (12;15) (though at low settings) likely achieved a higher level of patient and personnel blinding. (Personal communication, clinical expert, March 18, 2011) Sham therapy was generally given with usual care. Thus, these types of studies are comparable to the non-sham-based studies that examined long-term oxygen use and usual care as the comparator, since in these studies what was compared was NPPV therapy to no ventilation therapy while receiving usual care.
The studies included in this evidence-based analysis addressed the limitations of previous systematic reviews. Patients had severe to very severe COPD with hypercapnia and thus the greatest potential to benefit from NPPV therapy. Patients also underwent NPPV training prior to study initiation. However, low inspiratory levels may have been a limiting factor (< 15 cm H2O). When there was a trend for a beneficial effect of NPPV on PaO2 and PaCO2, the 2 studies that contributed to the estimate were distinct in that they were pulmonary laboratory-based studies with NPPV in use for 3 hours per day, 5 days a week at an IPAP of 18 cm H2O. (14;17) This suggests that proper use, as can be expected in a pulmonary laboratory–based setting, and high IPAP values are necessary in order to see the benefit of NPPV therapy. (23) Studies that used nocturnal NPPV may not have been adequately designed. (13;15;16;18;19) The study design concerns may be less relevant when examining the 6MWT. The heterogeneity in study design, as well as measurement and characterization of hospitalizations, dyspnea, and HRQOL, precluded a meta-analysis; however, there was some consistency in the results for dyspnea suggesting a beneficial effect of NPPV.
The evidence for the outcomes that could be meta-analyzed (mortality, PaO2, PaCO2, FEV1, 6MWT) was graded as very low to moderate quality of evidence. The evidence for the outcome of hospitalizations, which was not meta-analyzed, was graded as of moderate quality, and the evidence for the outcome of dyspnea, which was also not meta-analyzed, was graded as low quality. There was a lack of substantial data to grade the outcome of HRQOL. Grade quality of evidence for all outcomes is shown in Appendix 2.
Given the grade quality of evidence, the generalizability of the study results is high with respect to other severe to very severe COPD populations. For a majority of studies, individuals with sleep apnea were excluded as they may require the intervention and would not be able to be randomized to a non-treatment group. Additionally, the exclusion of individuals with sleep apnea or obesity helped to produce a more homogeneous COPD study population. Disease conditions that may affect the completion of the study (e.g., severe comorbidity), or the ability to use the technology (e.g., psychiatric conditions) were also excluded.
The characteristics of the studies identified in the literature review are shown in Appendix 3, Tables A3 to A8.
Economic Analysis
The results of the economic analysis are summarized in issue 12 of the COPD series entitled Cost-Effectiveness of Interventions for Chronic Obstructive Pulmonary Disease Using an Ontario Policy Model. This report can be accessed at: www.hqontario.ca/en/mas/tech/pdfs/2012/rev_COPD_Economic_March.pdf.
The results from the systematic review of the clinical evidence for NPPV for chronic respiratory failure in stable COPD patients were not included in the economic model because it was not shown to be clinically effective.
Conclusions
The following conclusions refer to stable, severe COPD patients receiving usual care.
Short-Term Studies
Based on low quality of evidence, there is a beneficial effect of NPPV compared with no ventilation on oxygen gas exchange, carbon dioxide gas exchange, and exercise tolerance measured using the 6MWT.
Based on very low quality of evidence, there is no effect of NPPV therapy on lung function measured as FEV1 (Type II error not excluded).
Long-Term Studies
Based on moderate quality of evidence, there is no effect of NPPV therapy for the outcomes of mortality, lung function measured as FEV1, and exercise tolerance measured using the 6MWT.
Based on low quality of evidence, there is no effect of NPPV therapy for the outcomes of oxygen gas exchange and carbon dioxide gas exchange (Type II error not excluded).
Qualitative Assessment
Based on low quality of evidence, there is a beneficial effect of NPPV compared with no ventilation for dyspnea based on reduced Borg score or MRC dyspnea score.
Based on moderate quality of evidence, there is no effect of NPPV therapy for hospitalizations.
HRQOL could not be evaluated.
Existing Guidelines for Noninvasive Positive Pressure Ventilation
An overview of existing guidelines for NPPV were identified from one journal article by Hill et al. (24) For Ontario, the Ministry of Health and Long-Term Care website was reviewed for existing guidelines. (4) The following guidelines are arranged according to the source of the guidelines: Consensus Conference Guidelines, (24) Centers for Medicare and Medicaid Services Guidelines, (24) and the Ministry of Health and Long-Term Care Guidelines. (4)
Consensus Conference Guidelines
For severe, stable COPD:
symptomatic after optimal therapy
sleep apnea excluded
PaCO2 ≥ 55 mm Hg or
PaCO2 50-54 mm Hg and evidence of nocturnal hypoventilation based on nocturnal oximetry showing sustained desaturation to < 89% for ≥ 5 min on oxygen use
repeated hospitalizations
Centers for Medicare and Medicaid Services Guidelines
For severe, stable COPD:
PaCO2 ≥ 52 mm Hg and
evidence of nocturnal hypoventilation based on nocturnal oximetry showing sustained desaturation to < 89% for ≥ 5 min on oxygen use
sleep apnea excluded
Ministry of Health and Long-Term Care Guidelines
no specific criteria
assessment by medical professional (i.e., a doctor who works at a sleep clinic registered with the Assistive Devices Program)
Glossary
- 6 Minute Walking Test (6MWT)
A measure of exercise capacity which measures the distance that a patient can quickly walk on a flat, hard surface in a period of 6 minutes. A widely used outcome measure in respiratory rehabilitation of patients with COPD.
- Acute exacerbations of chronic obstructive pulmonary disease (AECOPD)
A change in baseline symptoms that is beyond day-to-day variation, particularly increased breathlessness, cough, and/or sputum, which has an abrupt onset.
- Admission avoidance hospital-at-home program
Treatment program for patients experiencing acute exacerbations of COPD which allows patients to receive treatment in their home and avoid admission to hospital. After patients are assessed in the emergency department for an acute exacerbation, they are prescribed the necessary medications and additional care needed (e.g., oxygen therapy) and then sent home where they receive regular visits from a medical professional until the exacerbation has resolved.
- Ambulatory oxygen therapy
Provision of oxygen therapy during exercise and activities of daily living for individuals who demonstrate exertional desaturation.
- Bilevel positive airway pressure (BiPAP)
A continuous positive airway pressure mode used during noninvasive positive pressure ventilation (see definition below) that delivers preset levels of inspiratory and expiratory positive airway pressure. The pressure is higher when inhaling and falls when exhaling, making it easier to breathe.
- Cost-effectiveness acceptability curve (CEAC)
A method for summarizing uncertainty in estimates of cost-effectiveness.
- Cor pulmonale
Right heart failure, as a result of the effects of respiratory failure on the heart.
- Dyspnea
Difficulty breathing or breathlessness.
- Early discharge hospital-at-home program
Treatment program for patients experiencing acute exacerbations of COPD which allows patients to receive treatment in their home and decrease their length of stay in hospital. After being assessed in the emergency department for acute exacerbations, patients are admitted to the hospital where they receive the initial phase of their treatment. These patients are discharged early into a hospital-at-home program where they receive regular visits from a medical professional until the exacerbation has resolved.
- Forced expiratory volume in 1 second (FEV1)
A measure of lung function used for COPD severity staging; the amount of air that can be forcibly exhaled from the lungs in the first second of a forced exhalation.
- Forced vital capacity (FVC)
The amount of air that can be forcibly exhaled from the lungs after taking the deepest breath possible.
- Fraction of inspired oxygen (FiO2)
The percentage of oxygen participating in gas exchange.
- Hypercapnia
Occurs when there is too much carbon dioxide in the blood (arterial blood carbon dioxide > 45 to 60 mm Hg).
- Hypopnea
Slow or shallow breathing.
- Hypoxemia
Low arterial blood oxygen levels while breathing air at rest. May be severe (PaO2≤ 55 mm Hg), moderate (56 mm Hg ≤ PaO2 < 65 mm Hg), or mild-to-moderate (66 mm Hg < PaO2 ≤ 74 mm Hg).1
- Incremental cost-effectiveness ratio (ICER)
Ratio of the change in costs of a therapeutic intervention to the change in effects of the intervention compared to the alternative (often usual care).
- Intention-to-treat analysis (ITT)
An analysis based on the initial treatment the participant was assigned to, not on the treatment eventually administered.
- Invasive mechanical ventilation (IMV)
Mechanical ventilation via an artificial airway (endotracheal tube or tracheostomy tube).
- Long-term oxygen therapy (LTOT)
Continuous oxygen use for about 15 hours per day. Use is typically restricted to patients fulfilling specific criteria.
- Multidisciplinary care
Defined as care provided by a team (compared to a single provider). Typically involves professionals from a range of disciplines working together to deliver comprehensive care that addresses as many of the patient’s health care and psychosocial needs as possible.
- Nicotine replacement therapy (NRT)
The administration of nicotine to the body by means other than tobacco, usually as part of smoking cessation.
- Noninvasive positive pressure ventilation (NPPV)
Noninvasive method of delivering ventilator support (without the use of an endotracheal tube) using positive pressure. Provides ventilatory support through a facial or nasal mask and reduces inspiratory work.
- Partial pressure of carbon dioxide (PaCO2)
The pressure of carbon dioxide dissolved in arterial blood. This measures how well carbon dioxide is able to move out of the body.
- Partial pressure of oxygen (PaO2)
The pressure of oxygen dissolved in arterial blood. This measures how well oxygen is able to move from the airspace of the lungs into the blood.
- Palliative oxygen therapy
Use of oxygen for mildly hypoxemic or nonhypoxemic individuals to relieve symptoms of breathlessness. Used short term. This therapy is “palliative” in that treatment is not curative of the underlying disease.
- Pulmonary rehabilitation
Multidisciplinary program of care for patients with chronic respiratory impairment that is individually tailored and designed to optimize physical and social performance and autonomy. Exercise training is the cornerstone of pulmonary rehabilitation programs.
- Pulse oximetry
A noninvasive sensor, which is attached to the finger, toe, or ear to detect oxygen saturation of arterial blood.
- Quality-adjusted life-years (QALYs)
A measure of disease burden that includes both the quantity and the quality of the life lived that is used to help assess the value for money of a medical intervention.
- Respiratory failure
Respiratory failure occurs when the respiratory system cannot oxygenate the blood and/or remove carbon dioxide from the blood. It can be either acute (acute respiratory failure, ARF) or chronic, and is classified as either hypoxemic (type I) or hypercapnic (type II) respiratory failure. Acute hypercapnic respiratory failure frequently occurs in COPD patients experiencing acute exacerbations of COPD.
- Short-burst oxygen therapy
Short-duration, intermittent, supplemental oxygen administered either before or after exercise to relieve breathlessness with exercise.
- Sleep apnea
Interruption of breathing during sleep due to obstruction of the airway or alterations in the brain. Associated with excessive daytime sleepiness.
- Smoking cessation
The process of discontinuing the practice of inhaling a smoked substance.
- Spirometry
The gold standard test for diagnosing COPD. Patients breathe into a mouthpiece attached to a spirometer which measures airflow limitation.
- SpO2
Oxygen saturation of arterial blood as measured by a pulse oximeter.
- Stable COPD
The profile of COPD patients which predominates when patients are not experiencing an acute exacerbation.
- Supplemental oxygen therapy
Oxygen use during periods of exercise or exertion to relieve hypoxemia.
- Telemedicine (or telehealth)
Refers to using advanced information and communication technologies and electronic medical devices to support the delivery of clinical care, professional education, and health-related administrative services.
- Telemonitoring (or remote monitoring)
Refers to the use of medical devices to remotely collect a patient’s vital signs and/or other biologic health data and the transmission of those data to a monitoring station for interpretation by a health care provider.
- Telephone only support
Refers to disease/disorder management support provided by a health care provider to a patient who is at home via telephone or videoconferencing technology in the absence of transmission of patient biologic data.
- Ventilator-associated pneumonia (VAP)
Pneumonia that occurs in patients undergoing mechanical ventilation while in a hospital.
Acknowledgements
Medical Information Officer
Kellee Kaulback
Editorial Staff
Joanna Odrowaz
Irina Alecu
COPD Expert Advisory Panel
The role of the expert panel was to provide direction on the scope of the project and the relevant outcomes measures of effectiveness, to review the evidence-based analyses and to identify any societal or systemic issues that are relevant to intervention effectiveness. However, the statements, conclusions and views expressed in this report do not necessarily represent the views of the expert panel members.
Jeremy Grimshaw, MD, MBChB, PhD (Chair)
Senior Scientist, Ottawa Hospital Research Institute
Professor, Department of Medicine, University of Ottawa
Dina Brooks, PhD
Professor, Department of Physical Therapy, University of Toronto
Debbie Coutts, RRT, CRE
Andrea Gershon, MD, MSc, FRCP(C)
Scientist, Institute for Clinical Evaluative Sciences
Respirologist, Sunnybrook Health Sciences Centre
Assistant Professor, Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto
Mita Giacomini, BSc, MPH, MA, PhD
Professor, Department of Clinical Epidemiology & Biostatistics, McMaster University
Ron Goeree, BA, MA
Director, PATH Research Institute, St. Joseph’s Hospital (Hamilton)
Associate Professor, Department of Clinical Epidemiology & Biostatistics, McMaster University
Roger Goldstein, MBCHB, FRCP(C), FRCP(UK)
NSA Chair in Respiratory Rehabilitation Research
Director, Respiratory Services, and Senior Scientist, West Park Healthcare Centre
Professor, Medicine and Physical Therapy, University of Toronto
Alan G Kaplan, MD, CCFP(EM), FCFP
Chairperson, Family Physician Airways Group of Canada
Chairperson, Special Interest Focused Care Group in Respiratory Medicine, College of Family Physicians of Canada
Clinical Lecturer, Department of Family and Community Medicine, University of Toronto
DE O’Donnell, MD, FRCP(C)
Director, COPD Centre, Kingston General Hospital
Professor, Department of Medicine, Queen’s University
Asad Razzaque, MD
Family Physician
Holger Schünemann, MD, PhD, MSc, FRCP(C)
Michael Gent Chair in Healthcare Research
Chair, Department of Clinical Epidemiology & Biostatistics, McMaster University
Professor, Department of Clinical Epidemiology & Biostatistics and Medicine, McMaster University
Tasnim Sinuff, MD, PhD, FRCP(C)
Clinician Scientist, Sunnybrook Health Sciences Centre
Assistant Professor, Department of Medicine, University of Toronto
Laura Watling, RRT, BSc(HK)
Clinical Practice Leader/Clinical Coordinator, Respiratory Therapy, West Park Healthcare Centre
Appendices
Appendix 1: Literature Search Strategies
Search date: December 3, 2010
Databases searched: OVID MEDLINE, MEDLINE In-Process and Other Non-Indexed Citations, OVID EMBASE, Wiley Cochrane Library, Cumulative Index to Nursing & Allied Health Literature (CINAHL), Centre for Reviews and Dissemination/International Agency for Health Technology Assessment
Database(s): Ovid MEDLINE(R) 1950 to November Week 3 2010
Search Strategy:
| # | Searches | Results |
|---|---|---|
| 1 | exp Pulmonary Disease, Chronic Obstructive/ (chronic obstructive adj2 (lung* or pulmonary or airway* or airflow or respiratory) adj | 15011 |
| 2 | (disease* or disorder*)).ti,ab. | 21909 |
| 3 | (copd or coad).ti,ab. | 16795 |
| 4 | chronic airflow obstruction.ti,ab. | 493 |
| 5 | exp Emphysema/ | 7051 |
| 6 | ((chronic adj2 bronchitis) or emphysema).ti,ab. | 22960 |
| 7 | or/1-6 | 54680 |
| 8 | exp Respiration, Artificial/ | 51221 |
| 9 | ((artificial or non-invasive or noninvasive or invasive or nasal or mechanical or volume-controlled or pressure controlled or positive) adj2 (ventilat* or respiration)).ti,ab. (NIV or NPPV or NIPPV or NIAV or continous positive airway pressure or CPAP or bi-level | 29829 |
| 10 | positive pressure or ventilation support or BiPAP or endotracheal intubation or ventilat* failure).ti,ab. | 10735 |
| 11 | exp Ventilator Weaning/ | 2368 |
| 12 | limit 11 to “all adult (19 plus years)” | 1062 |
| 13 | or/8-10 | 68682 |
| 14 | 7 and 13 | 3314 |
| 15 | 12 or 14 | 4228 |
| 16 | limit 15 to (english language and humans and yr=“2004 -Current”) | 1206 |
Database(s): EMBASE 1980 to 2010 Week 47
Search Strategy:
| # | Searches | Results |
|---|---|---|
| 1 | exp chronic obstructive lung disease/ | 48840 |
| 2 | (chronic obstructive adj2 (lung* or pulmonary or airway* or airflow or respiratory) adj (disease* or disorder*)).ti,ab. | 26482 |
| 3 | (copd or coad).ti,ab. | 21755 |
| 4 | chronic airflow obstruction.ti,ab. | 551 |
| 5 | exp emphysema/ | 25753 |
| 6 | exp chronic bronchitis/ | 6600 |
| 7 | ((chronic adj2 bronchitis) or emphysema).ti,ab. | 25596 |
| 8 | or/1-7 | 89245 |
| 9 | exp artificial ventilation/ | 86836 |
| 10 | ((artificial or non-invasive or noninvasive or invasive or nasal or mechanical or volume-controlled or pressure controlled or positive) adj2 (ventilat* or respiration)).ti,ab.(NIV or NPPV or NIPPV or NIAV or continous positive airway pressure or CPAP or bi-level | 36697 |
| 11 | positive pressure or ventilation support or BiPAP or endotracheal intubation or ventilat* failure).ti,ab. | 13569 |
| 12 | (ventilat* adj2 wean*).mp. [mp=title, abstract, subject headings, heading word, drug trade 12 name, original title, device manufacturer, drug manufacturer] | 971 |
| 13 | limit 12 to (adult <18 to 64 years> or aged <65+ years>) | 357 |
| 14 | or/9-11 | 102073 |
| 15 | 8 and 14 | 6573 |
| 16 | 13 or 15 | 6871 |
| 17 | limit 16 to (human and english language and yr=“2004 -Current”) | 2094 |
CINAHL
| # | Query | Results |
|---|---|---|
| S14 | (S11 or S12) Limiters - Published Date from: 20040101-20101231; English Language |
416 |
| S13 | (S11 or S12) | 794 |
| S12 | s6 and s10 | 585 |
| S11 | (MH “Ventilator Weaning”) Limiters - Age Groups: Aged: 65+ years |
235 |
| S10 | S7 or S8 or S9 | 12790 |
| S9 | NIV or NPPV or NIPPV or NIAV or continous positive airway pressure or CPAP or bi-level positive pressure or ventilation support or BiPAP or endotracheal intubation or ventilat* failure | 1689 |
| S8 | artificial N2 ventil* or non-invasive N2 ventil* or noninvasive N2 ventil* or invasive N2 ventil* or nasal N2 ventil* or mechanical N2 ventil* or volume-controlled N2 ventil*or pressure controlled N2 ventil*or positive N2 ventil* or artificial N2 respirat* or non-invasive N2 respirat* or noninvasive N2 respirat* or invasive N2 respirat* or nasal N2 respirat* or mechanical N2 respirat* or volume-controlled N2 respirat*or pressure controlled N2 respirat*or positive N2 respirat* | 9597 |
| S7 | (MH “rdquo;Respiration, Artificial+”) | 10081 |
| S6 | S1 or S2 or S3 or S4 or S5 | 7579 |
| S5 | chronic bronchitis or emphysema | 1606 |
| S4 | (MH “Emphysema+”) | 982 |
| S3 | copd or coad | 4153 |
| S2 | (chronic obstructive and (lung* or pulmonary or airway* or airflow or respiratory) and (disease* or disorder*)) | 5747 |
| S1 | (MH “Pulmonary Disease, Chronic Obstructive+”) | 4462 |
Appendix 2: GRADE Evidence Tables
Table A1: GRADE Evidence Assessment for Outcomes of Mortality and Lung Function*.
| Quality Assessment | Summary of Findings | Importance | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of patients | Effect | Quality | ||||||||||
| No. of Studies | Design | Limitations | Inconsistency | Indirectness | Imprecision | Other Considerations | NIV | No NIV | RR (95% CI) | Absolute | ||
| Mortality | ||||||||||||
| 3 | Randomized trials | Serious†,‡,§ | No serious inconsistency | No serious indirectness | No serious imprecision | Long term only |
51/131 (38.9%) |
58/143 (40.6%) _________ 17% |
RR 0.91 (0.7 to 1.19) |
37 fewer per 1000 (from 122 fewer to 77 more)__________ 15 fewer per 1000 (from 51 fewer to 32 more) |
⊕⊕⊕O MODERATE |
|
| PaCO2 Surrogate Outcome | ||||||||||||
| 3 | Randomized trials | Serious†,§ | No serious inconsistency | Pulmonary lab in the short term | Small sample in the long term║ | Short term Long term |
45 20 |
33 24 |
- |
MD 7.54 lower (10.16 lower to 4.92 lower) MD 1.30 higher (3.40 lower to 6.00 higher) |
⊕⊕OO LOW⊕⊕OO LOW |
|
| PaO2 Surrogate Outcome | ||||||||||||
| 3 | Randomized trials | Serious†,§ | No serious inconsistency | Pulmonary lab in the short term | Small sample in the long term║ | Short term Long term |
45 20 |
33 24 |
- |
MD 6.16 higher (3.51 higher to 8.80 higher) MD 0.80 higher (3.80 lower to 5.40 higher) |
⊕⊕OO LOW⊕⊕OO LOW |
|
| FEV1 | ||||||||||||
| 3 | Randomized trials | Serious†,§ | No serious inconsistency | Pulmonary lab in the short term | Small sample in the short term║ | Short term Long term |
18 59 |
18 71 |
- |
MD 5.00 higher (1.91 lower to 11.91 higher) MD 1.05 higher (2.17 lower to 4.27 higher) |
⊕⊕OO LOW⊕⊕OO LOW |
|
| 6MWT | ||||||||||||
| 4 | Randomized trials | Serious¶.#’ | No serious inconsistency | Pulmonary lab in the short term | No serious imprecision | Short term Long term |
42 39 |
31 47 |
- |
MD 49.72 higher (2.93 higher to 96.51 higher) MD 3.00 lower (52.55 lower to 46.55 higher) |
⊕⊕OO LOW⊕⊕OO LOW |
|
Abbreviations: 6MWT, 6 Minute Walking Test; CI, confidence interval; FEV1, forced expiratory volume in 1 second; MD, mean difference; NIV, noninvasive ventilation; no., number; PaCO2, arterial pressure of carbon dioxide; PaO2, arterial pressure of oxygen; RR, relative risk.
Lack of blinding of patients and/or assessors: mortality, (13;19); PaO2, (13); PaCO2, (13); FEV1, (13).
Significant losses to follow-up in 1 study: mortality, (16).
Allocation concealment was not well described in 2 studies (mortality, (13;16); PaO2, (13;14); PaCO2, (13;14)), or 3 studies (FEV1, (13;14;16)).
Table A2: GRADE Evidence Assessment for Outcomes of Hospitalizations, Dyspnea, and SGRQ*.
| Quality Assessment | Summary of Findings | Additional Comments | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No of patients | Effect | Quality | ||||||||||
| No. of Studies | Design | Limitations | Inconsistency | Indirectness | Imprecision | Other Considerations | NIV | No NIV | Relative (95% CI) | Absolute | ||
| Hospitalizations | ||||||||||||
| 2 | Randomized trials | Serious†,‡ | No serious inconsistency | No serious indirectness | No serious imprecision | None |
0/0 (0%) |
0/0 (0%) _________ 0% |
RR 0 (0 to 0) |
0 fewer per 1000 (from 0 fewer to 0 fewer)_________ 0 fewer per 1000 (from 0 fewer to 0 fewer) |
⊕⊕⊕O MODERATE |
3 and 12 months, and 5 years of follow-up, data could not be pooled across the 2 studies with different lengths of follow-up (qualitative assessment) |
| Dyspnea | ||||||||||||
| 4 | Randomized trials | Very serious†,§,║,¶ | No serious inconsistency | No serious indirectness | No serious imprecision | None |
0/0 (0%) |
0/0 (0%) _________ 0% |
RR 0 (0 to 0) |
0 fewer per 1000 (from 0 fewer to 0 fewer)_________ 0 fewer per 1000 (from 0 fewer to 0 fewer) |
⊕⊕OO LOW |
5 days, 3 weeks, 6 months, and 2 years of follow-up, data could not be pooled, different characterization of outcome by follow-up (qualitative assessment) |
| SGRQ | ||||||||||||
| n/a | n/a | n/a | n/a | n/a | n/a | n/a |
__________ |
__________ |
n/a |
Insufficient data on which to base a conclusion | ||
Abbreviations: CI, confidence interval; NIV, noninvasive ventilation; No., number; RR, relative risk; SGRQ, St. George’s Respiratory Questionnaire.
Allocation concealment was not well described: hospitalizations, (13).
Allocation concealment was not well described in 3 studies (dyspnea, (12;13;16) and the process of randomization in 1 study (dyspnea, (12)).
High attrition in 1 study (dypsnea, (16)).
Unknown if randomization was achieved in 1 study (dyspnea, (12)).
Appendix 3: Summary Tables
Table A3: Summary of Study Characteristics (N = 8 Studies)*.
| Author, Year | Study Location | COPD Severity† | Study Design | Length of Follow-up | Treatment/Control (no.) | Losses to Follow-up‡ |
|---|---|---|---|---|---|---|
| McEvoy et al, 2009 (19) | University hospitals, Australia | Severe | Parallel RCT | 5 years | 72/72 | 4/4 |
| Sin et al, 2007 (18) | Specialists’ clinics, University of Alberta | Moderate | Parallel RCT | 3 months | 10/11 | 2/0 |
| Diaz et al, 2005 (17) | Universidad Catolica de Chile, Chile | Severe | Parallel RCT | 3 weeks | 27/15 | 0/0 |
| Clini et al, 2002 (16) | Respiratory units, Italy and France | Severe | Parallel RCT | 2 years | 39/47 | 8/15 |
| Diaz et al, 2002 (14) | Universidad Catolica de Chile, Chile | Severe | Parallel RCT | 3 weeks | 18/18 | 0/0 |
| Casanova et al, 2000 (13) | Pulmonary clinics, Canary Islands | Severe | Parallel RCT | 1 year | 20/24 | 5/2 |
| Gay et al, 1996 (15) | Database, United States | Severe | Parallel RCT | 3 months | 7/6 | 3/0 |
| Renston et al, 1994 (12) | Pulmonary lab records, United States | Severe | Parallel RCT | 5 days | 9/8 | n/a |
Abbreviations: COPD, chronic obstructive pulmonary disease; no., number; RCT, randomized controlled trial.
COPD severity based on study entry criteria. Final study population may differ. See Appendix 3, Table A8 for baseline values.
Losses to follow-up refer to treatment/control (no.).
Table A4: Summary of Study Design Characteristics From Studies Identified From the Literature Search (N = 3 Studies)*.
| Author, Year | Comparator | Study Population | Intervention | Results | Additional Comments |
|---|---|---|---|---|---|
| McEvoy et al, 2009 (19) | N-NIV + LTOT vs. LTOT | 144† COPD patients, < 80 yrs, severe (FEV1 < 50%), stable, hypercapnic (PaCO2 > 46 mmHg), FU: 5 yrs | N-NIV, patient triggered BiPAP, IPAP to max tolerable, EPAP of 3 cm H2O, IPAP-EPAP difference of ≥10 cm H2O | Mean age: ~68 yrs; median FU, TR: 28.5 vs.CT: 20.5 mo, no diff in LTOT use (~19 hrs);mean NIV use: 4.5 hrs/night; mean IPAP: 13cm H2O Mortality, HR: 0.63, 95% CI: 0.40-0.99, P=0.045, (TR: 40/72 (55.6%) vs. 46/72 (63.9%));no diff in hospitalization rates based on days on trial Lung function: no diff for PaO2 (DNS), PaCO2, FEV1 at 12 mo, P?HRQOL: no diff for SGRQ at 12 mo (DNS) |
LTOT for at least 3 mo, nasal or face mask, sleep apnea excluded, nonsmoking, plus usual care in both arms, close contact for FU, subgroup analysis for NIV > 4 hrs, NIV training, 8/144 R-DO (5.6%) (TR: 4/72 (5.6%) vs. CT: 4/72 (5.6%)) |
| Sin et al, 2007(18) | N-NIV vs. CPAP | 23 COPD patients, > 39 yrs, moderate (FEV1 < 70%), stable? near hypercapnic (from baseline: ~44.2 mm Hg), FU: 3 mo | N-NIV, BiPAP, IPAP to max tolerable, EPAP of 4 cm H2O | Mean age: ~65 yrs; mean NIV use? Mean IPAP: 15.5 cm H2O 6MWT at 3 mo, no diff (TR: 367 vs. CT: 311 m, P = 0.311); No suitable data for PaCO2 and FEV1 (within group comparison from baseline) |
O2 use as needed, nasal or face mask, sleep apnea excluded, smokers, std medical, close contact for FU, NIV training, 2/23 R-DO (8.7%) (TR: 2/13 (15.4%) vs. 0/10 CT (0%)) |
| Diaz et al, 2005 (17) | NIV vs. CPAP | 62 COPD patients, all ages, severe (at baseline), stable, hypercapnic (PaCO2≥ 50 mm Hg), FU: 3 wks | NIV, spontaneous mode, BiPAP, IPAP to max tolerable, EPAP of 2 cm H2O, 3 hrs/day, 5 days/wk | Mean age: ~68 yrs; use of NIV as in lab; meanIPAP: 18 cm H2O Change in PaCO2, TR: -8.2 vs. CT: -0.7 mm Hg, P< 0.0001; PaO2, TR: 7.7 vs. CT: 2.2 mm Hg, P< 0.001; FEV1, TR: 0.08 vs. CT: 0 litres, P< 0.001; 6MWT, TR: 76 vs. CT: 13 m, P< 0.0001; Borg, TR: -1.5 vs. CT: -0.1, P< 0.0001 |
LTOT use, no prior NIV use, sleep apnea excluded, current medication (e.g., bronchodilators), O2 for all controls, face mask, nonsmoking, pulmonary lab, 0 R-DO |
Abbreviations: 6MWT, 6 Minute Walking Test; BiPAP, bilevel positive airway pressure; COPD, chronic obstructive pulmonary disease; CPAP, continuous positive airway pressure; CRQ, Chronic Respiratory Questionnaire; CT, control group; diff, difference; DNS, data not shown; DO, dropout; EPAP, expiratory positive airway pressure; FEV1, forced expiratory volume in 1 second; FU, follow-up; HR, hazard ratio; HRQOL, health-related quality of life; hrs, hours; IPAP, inspiratory positive airway pressure; LTOT, long-term oxygen therapy; mm Hg, millimetres of mercury; NIV, noninvasive ventilation; N-NIV, nocturnal noninvasive ventilation; O2, supplementary oxygen; PaCO2, arterial pressure of carbon dioxide; PaO2, arterial pressure of oxygen; R-DO, dropouts from randomization; SGRQ, St. George’s Respiratory Questionnaire; TR, treatment group; wk, week.
After exclusions. Remaining numbers refer to the initial COPD study population.
Table A5: Summary of Study Design Characteristics From Eligible Studies (N = 5 Studies)*,†.
| Author, Year | Comparator | Study Population | Intervention | Results | Additional Comments |
|---|---|---|---|---|---|
| Clini et al, 2002 (16) | N-NIV + LTOT vs. LTOT | 122 COPD patients < 76 yrs, severe (FEV1<1.5 L), stable, hypercapnic (PaCO2>50 mm Hg), FU: 2 yrs | N-NIV, spontaneous/timed mode, BiPAP, IPAP to max tolerable, EPAP of 2−5 cm H2O | Mean age: ~65 yrs; mean LTOT use (~20 hrs); mean NIV use: 9 hrs/night; mean IPAP: 14 cm H2O Mortality: no diff (TR: 18 vs. CT: 17%) Lung function: no diff for FEV1 and PaO2 at 12 and 24 mo; PaCO2 diff at 12 and 24 mo (24 mo, TR: 55 vs. CT: 60 mm Hg, P= 0.002); MRC dyspnea diff at 12 and 24 mo (24 mo, TR: 2.2 vs. CT: 3, P= 0.013); no diff for 6MWT at 12 and 24 mo HRQOL: no diff for SGRQ at 12 and 24 mo |
LTOT for at least 6 mo, nasal, no prior use of NIV, sleep apnea and smokers excluded, SM (e.g., bronchodilators), close contact for FU, NIV training, 23/86 R-DO (26.7%) (TR: 8/39 (20.5%) vs. CT: 15/47 (31.9%)), PaCO2 and HRQOL on usual O2, MRF-28 available |
| Diaz et al, 2002 (14) | NIV vs. CPAP | 56 COPD patients, all ages, severe (?FEV1), stable, hypercapnic (PaCO2 >50 mm Hg), FU: 3 wks | NIV, spontaneous mode, BiPAP, IPAP to max tolerable, EPAP of 2 cm H2O, laboratory/direct supervision (outpatient), 3 hrs/day, 5 days-wk | Mean age: ~67 yrs, use of NIV as in lab; mean IPAP: 18 cm H2O Lung function at 3 wks, PaCO2, TR: 6.5 vs. CT: 7.3 kPa; PaO2, TR: 7.1 vs. 6.7 kPa; FEV1, TR: 35.8 vs. 36.7% (P? for all) |
All controls needed O2(offered to NIV but not needed), face mask, sleep apnea excluded, SM (e.g., bronchodilators), no prior use of NIV, nonsmoking, std medical, pulmonary lab, 0 R-DO |
| Casanova et al, 2000 (13) | N-NIV + SM vs. SM | 80 COPD patients, 45-75 yrs, severe (< 45%), stable, hypercapnic (from baseline: ~52 mm Hg), FU: 1 yr | N-NIV, spontaneous mode, BiPAP, IPAP of 12 cm H2O, EPAP of 4 cm H2O | Mean age: ~66 yrs; mean NIV use: 6.1hrs/day, mean IPAP: 12 cm H2O Morbidity, no sign diff at 1 yr (e.g., hospitaladmissions, ~20%) Mortality, no sign diff at 1 yr (TR: 4/20 (20%)vs. CT: 4/24 (16.7%), P?) Lung function (gases and FEV1), no sign diff at 6 mo (e.g., FEV1, TR: 30 vs. 31%) |
SM as bronchodilators, antibiotics, corticosteroids, and LTOT use, nasal, O2 as needed, sleep apnea excluded, stopped smoking, NIV training, 7/52 R-DO (13.5%) (TR: 5/26 (19.2%) vs. CT: 2/26 (7.7%)) |
| Gay et al, 1996 (15) | N-NIV vs. CPAP | 85 COPD patients,< 80 yrs, severe (FEV1< 40%), stable, hypercapnic (PaCO2 > 45 mm Hg), FU: 3 mo | N-NIV, spontaneous mode, BiPAP, IPAP: 10 cm H20, EPAP of 2 cm H2O | Mean age: ~69 yrs; NIV use: ~4.5 hrs/night, IPAP: 10 cm H2O Lung function, FEV1, TR: 0.60 vs. CT: 0.71 litres, P? data are difficult to extrapolate for PaCO2; 6MWT, TR: 309.2 vs. CT: 306.9 m, P?) |
LTOT use, nasal, NIV training, medications, 3/13 R-DO (23.1%) (TR: 3/7 (42.9%) vs. CT: 0/6) |
| Renston et al, 1994 (12) | NIV vs. CPAP | 17 COPD patients, all ages, severe (FEV1<50%), stable, hypercapnic? FU: 5 days | NIV, spontaneous mode, BiPAP, IPAP: 15-20 cm H2O, EPAP of 2 cm H2O | Mean age: ~65 yrs; NIV use: 2 hrs/day, Mean IPAP? Lung function, PaCO2, PaO2: no sign diff at FU(extrapolated from graph), Borg, TR: 0.6 vs. CT:1.3, P? (extrapolated from graph, au), 6MWT, Change, TR: 32 vs. CT: 0 m, P? (extrapolated from graph) |
Home oxygen use, nasal, sleep apnea excluded, very short duration study, 0 R-DO |
Abbreviations: 6MWT, 6 Minute Walking Test; au, arbitrary units; BiPAP, bilevel positive airway pressure; COPD, chronic obstructive pulmonary disease; CPAP, continuous positive airway pressure; CT, control group; diff, difference; EPAP, expiratory positive airway pressure; FEV1, forced expiratory volume in 1 second; FU, follow-up; HRQOL, health-related quality of life; hrs, hours; kPa, kilopascal; IPAP, inspiratory positive airway pressure; LTOT, long-term oxygen therapy; mm Hg, millimetres of mercury; mo, months; MRC, Medical Research Council; MRF-28, Maugeri Foundation Respiratory Failure Questionnaire; NIV, noninvasive ventilation; N-NIV, nocturnal noninvasive ventilation; O2, supplementary oxygen; PaCO2, arterial pressure of carbon dioxide; PaO2, arterial pressure of oxygen; R-DO, dropouts from those randomized (early dropouts excluded from denominator); SGRQ, St. George’s Respiratory Questionnaire; SM, standard medical; TR, treatment group; yrs, years.
Source: Kolodziej et al, 2007 (9)
Table A6: Study Design Strengths and Limitations*.
| Study Design Strengths and Limitations† | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study, Year | COPD Study Population | Adequate Sample Size‡ | Exclusions Detailed | Randomization Achieved | Blinding§ | Adequately Measured Compliance | All-Cause Mortality | Survival Analysis | Intent-to-Treat Analysis | Minimal Attrition║ |
| McEvoy et al, 2009 (19) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Sin et al, 2007 (18) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
| Diaz et al, 2005 (17) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓¶ | ✓ | |||
| Clini et al, 2002 (16) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Diaz et al, 2002 (14) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓¶ | ✓ | ||
| Casanova et al, 2000 (13) | ✓ | ✓ | ✓ | ✓# | ✓ | ✓ | ✓ | ✓ | ||
| Gay et al, 1996 (15) | ✓ | ✓ | ✓** | ? | ||||||
| Renston et al, 1994 (12) | ✓ | ✓ | ✓** | ✓ | ✓¶ | ✓ | ||||
Abbreviations: BiPAP, bilevel positive airway pressure; COPD, chronic obstructive pulmonary disease; ✓, study design strengths; ? compliance of NIV use was determined but not reported.
Allocation concealment was not adequate for Clini (2002), Diaz (2002), Sin (2007), Casanova (2000), Gay (1996), and Renston (1994) and the process of generating randomized schedules was not adequate for Sin (2007), Gay (1996) and Renston (1994).
Lack of sample size based on reported sample size calculation for primary association of interest.
Personnel performing outcome assessment were blinded to allocation of treatment or research question. Placebo effect for the patient cannot be ruled out.
Minimal attrition based on examination of total and per arm losses to follow-up/dropouts, with less than 20% attrition deemed to be adequate.
For a short length of follow-up, with zero dropouts.
Slight differences for age only.
Blinding based on use of sham-BiPAP.
Table A7: Summary of the Results from the Qualitative Assessment*.
| Outcome Measures | Assessment | |
|---|---|---|
| 1) Dyspnea | ||
| 4 Studies | ||
| Diaz et al, 2005 (17) | + | |
| Clini et al, 2002 (16) | + | |
| Casanova et al, 2000 (13) | -/= | |
| Renston et al, 1994 (12) | + | |
| 2) Hospitalizations | ||
| 2 Studies | ||
| McEvoy et al, 2009 (19). | = | |
| Casanova et al, 2000 (13) | = | |
| 3) Health-Related Quality of Life | ||
| 2 Studies | ||
| McEvoy et al, 2009 (19). | = | |
| Clini et al, 2002 (16) | = | |
indicates evidence that showed no difference between technologies;
indicates evidence favouring the technology;
indicates evidence favouring the control.
Table A8: Summary of Key Study Characteristics*.
| Summary of Key Study Characteristics† | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study, Year | FEV1 Total Baseline‡ (% pred) | FEV1 TR Baseline‡ (% pred) | FEV1 CT Baseline‡ (% pred) | PaO2 Total Baseline§ (mm Hg) | PaO2 TR Baseline§ (mm Hg) | PaO2 CT Baseline§ (mm Hg) | PaCO2 Total Baseline║ (mm Hg) | PaCO2 TR Baseline║ (mm Hg) | PaCO2 CT Baseline║ (mm Hg) | Mean (SD) FU or Range (years) |
| McEvoy et al, 2009 (19) | 24.1 | 25 | 23.1 | 53.7 | 54.8 | 52.5 | 53.5 | 52.6 | 54.4 | 2.0¶ |
| Sin et al, 2007 (18) | 31.2 | 37.6 | 24.8 | 60 | 59.3 | 60.7 | 44.2 | 45.2 | 43.1 | ? |
| Diaz et al, 2005 (17) | 32.5 | 30 | 35 | 46.6 | 45.3 | 47.9 | 56.6 | 56.5 | 56.7 | n/a |
| Clini et al, 2002 (16) | 29 | 27 | 31 | 49.9 | 50.3 | 49.5 | 54.8 | 54 | 55.5 | ? |
| Diaz et al, 2002 (14) | 0.8# | 0.7# | 0.8# | 47.2 | 45.2 | 49.2 | 56 | 56.8 | 55.2 | n/a |
| Casanova et al, 2000 (13) | 0.9# | 0.8# | 0.9# | 56.6 | 55.7 | 57.5 | 52.0 | 50.7 | 53.2 | ? |
| Gay et al, 1996 (15) | 0.7# | 0.6# | 0.7# | 62.1 | 66.4 | 57.8 | 51.6 | 54.7 | 48.5 | ? |
| Renston et al, 1994 (12) | 34.5 | 32 | 37 | 65 | 65** | 65** | 48.5 | 50** | 47** | n/a |
Abbreviations: COPD, chronic obstructive pulmonary disease; CT, control group; FEV1, forced expiratory volume in 1 second; FU, follow-up; mm Hg, millimetres of mercury; n/a, not applicable; PaCO2, arterial pressure of carbon dioxide; PaO2, arterial pressure of oxygen; pred, predicted; SD, standard deviation; TR, treatment group; ? indicates data not provided.
Data were reported as means and standard deviations unless otherwise indicated; total was either taken from the original paper or calculated as the mean from the two arms of the trial; total refers to the study population as a whole including the treatment group and control group.
COPD Stage: Mild, FEV1 ≥ 80% predicted; Moderate, FEV1 < 80% and FEV1 ≥ 50% predicted; Severe, FEV1 < 50% and FEV1 ≥ 30% predicted; Very Severe, FEV1 < 30%.
Hypoxemia: Severe, < 55 mm Hg; Mild-Moderate, ~ 56-65 mm Hg.
Hypercapnia: > 45-60 mm Hg.
Median, average of both arms.
FEV1 in litres. Severe COPD defined as FEV1 < 1.5 litres.
Extrapolated from graph.
Suggested Citation
This report should be cited as follows:
COPD Working Group. Noninvasive positive pressure ventilation for chronic respiratory failure patients with stable chronic obstructive pulmonary disease (COPD): an evidence-based analysis. Ont Health Technol Assess Ser [Internet]. 2012 Mar; 12(9): 1−51. Available from: www.hqontario.ca/en/mas/tech/pdfs/2012/rev_COPD_Ventilation_Chronic_March.pdf
Indexing
The Ontario Health Technology Assessment Series is currently indexed in Excerpta Medica/EMBASE and the Center for Reviews and Dissemination database.
Permission Requests
All inquiries regarding permission to reproduce any content in the Ontario Health Technology Assessment Series should be directed to: MASinfo@hqontario.ca.
How to Obtain Issues in the Ontario Health Technology Assessment Series
All reports in the Ontario Health Technology Assessment Series are freely available in PDF format at the following URL: http://www.hqontario.ca/en/mas/mas_ohtas_mn.html.
Conflict of Interest Statement
All analyses in the Ontario Health Technology Assessment Series are impartial and subject to a systematic evidence-based assessment process. There are no competing interests or conflicts of interest to declare.
Peer Review
All analyses in the Ontario Health Technology Assessment Series are subject to external expert peer review. Additionally, the public consultation process is also available to individuals wishing to comment on an analysis prior to finalization. For more information, please visit: http://www.hqontario.ca/en/mas/ohtac_public_engage_overview.html.
Health Quality Ontario
130 Bloor Street West, 10th Floor
Toronto, Ontario
M5S 1N5
Tel: 416-323-6868
Toll Free: 1-866-623-6868
Fax: 416-323-9261
Email: MASinfo@hqontario.ca
ISSN 1915-7398 (online)
ISBN 978-1-4435-7015-2 (PDF)
© Queen’s Printer for Ontario, 2012
About the Medical Advisory Secretariat
Effective April 5, 2011, the Medical Advisory Secretariat (MAS) became a part of Health Quality Ontario (HQO), an independent body funded by the Ministry of Health and Long-Term Care. The mandate of MAS is to provide evidence-based recommendations on the coordinated uptake of health services and health technologies in Ontario to the Ministry of Health and Long-Term Care and to the health care system. This mandate helps to ensure that residents of Ontario have access to the best available and most appropriate health services and technologies to improve patient outcomes.
To fulfill its mandate, MAS conducts systematic reviews of evidence and consults with experts in the health care services community. The resulting evidence-based analyses are reviewed by the Ontario Health Technology Advisory Committee—to which MAS also provides a secretariat function—and published in the Ontario Health Technology Assessment Series.
About the Ontario Health Technology Assessment Series
To conduct its comprehensive analyses, MAS systematically reviews the available scientific literature, making every effort to consider all relevant national and international research; collaborates with partners across relevant government branches; consults with clinical and other external experts and developers of new health technologies; and solicits any necessary supplemental information.
In addition, the Secretariat collects and analyzes information about how a new technology fits within current practice and existing treatment alternatives. Details about the technology’s diffusion into current health care practices add an important dimension to the review of the provision and delivery of the health technology in Ontario. Information concerning the health benefits; economic and human resources; and ethical, regulatory, social and legal issues relating to the technology assist decision-makers in making timely and relevant decisions to optimize patient outcomes.
The public consultation process is available to individuals wishing to comment on an analysis prior to publication. For more information, please visit: http://www.hqontario.ca/en/mas/ohtac_public_engage_overview.html.
Disclaimer
This evidence-based analysis was prepared by MAS for the Ontario Health Technology Advisory Committee and developed from analysis, interpretation, and comparison of scientific research and/or technology assessments conducted by other organizations. It also incorporates, when available, Ontario data and information provided by experts and applicants to MAS to inform the analysis. While every effort has been made to reflect all scientific research available, this document may not fully do so. Additionally, other relevant scientific findings may have been reported since completion of the review. This evidence-based analysis is current to the date of the literature review specified in the methods section. This analysis may be superseded by an updated publication on the same topic. Please check the MAS website for a list of all evidence-based analyses: http://www.hqontario.ca/en/mas/mas_ohtas_mn.html.
List of Tables
| Table 1: Body of Evidence Examined According to Study Design* |
| Table A1: GRADE Evidence Assessment for Outcomes of Mortality and Lung Function* |
| Table A2: GRADE Evidence Assessment for Outcomes of Hospitalizations, Dyspnea, and SGRQ* |
| Table A3: Summary of Study Characteristics (N = 8 Studies)* |
| Table A4: Summary of Study Design Characteristics From Studies Identified From the Literature Search (N = 3 Studies)* |
| Table A5: Summary of Study Design Characteristics From Eligible Studies (N = 5 Studies)*,† |
| Table A6: Study Design Strengths and Limitations* |
| Table A7: Summary of the Results from the Qualitative Assessment* |
| Table A8: Summary of Key Study Characteristics* |
List of Figures
| Figure 1: Citation Flow Chart |
| Figure 2: Mortality (Number of Events) – All Studies With Follow-up Greater Than 3 Months*,†,‡ |
| Figure 3: Forced Expiratory Volume in 1 Second (% Predicted)*,†,‡ |
| Figure 4: Arterial Pressure of Oxygen (mm Hg)*,†,‡ |
| Figure 5: Arterial Pressure of Carbon Dioxide (mm Hg)*,†,‡ |
| Figure 6: Six Minute Walking Test (Metres)*,†,‡ |
List of Abbreviations
- 6MWT
6 Minute Walking Test
- BiPAP
Bilevel positive airway pressure
- BMI
Body mass index
- CI
Confidence interval
- COPD
Chronic obstructive pulmonary disease
- CPAP
Continuous positive airway pressure
- CT
Control group
- FEV1
Forced expiratory volume in 1 second
- HRQOL
Health-related quality of life
- IPAP
Inspiratory positive airway pressure
- kPa
kilopascal (1 kPa = 7.5 mm Hg)
- LTOT
Long-term oxygen therapy
- MAS
Medical Advisory Secretariat
- MRC
Medical Research Council
- NIV
Noninvasive ventilation
- NPPV
Noninvasive positive pressure ventilation
- PaCO2
Arterial partial pressure of carbon dioxide
- PaO2
Arterial partial pressure of oxygen
- RCT
Randomized controlled trial
- RR
Relative risk
- SD
Standard deviation
- SGRQ
St. George’s Respiratory Questionnaire
- TR
Treatment group, referring to NPPV
- VEP
Ventilator Equipment Pool
Footnotes
The mild-to-moderate classification was created for the purposes of the report.
References
- 1.Diaz-Lobato S, Alises SM, Rodriguez EP. Current status of noninvasive ventilation in stable COPD patients. Int J Chron Obstruct Pulmon Dis. 2006;1(2):129–35. doi: 10.2147/copd.2006.1.2.129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gold PM. The 2007 GOLD Guidelines: a comprehensive care framework. Respir Care. 2009;54(8):1040–9. [PubMed] [Google Scholar]
- 3.Budweiser S, Jorres RA, Pfeifer M. Treatment of respiratory failure in COPD. Int J Chron Obstruct Pulmon Dis. 2008;3(4):605–18. doi: 10.2147/copd.s3814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ministry of Health and Long-Term Care. Assistive Devices Program: Respiratory Products [Internet] [[cited: 2011 Jan 6]];Ontario: Queen's Printer of Ontario. 2004 Jun 1; Available from: http://www.health.gov.on.ca/english/public/pub/adp/resp.html .
- 5.Theerakittikul T, Ricaurte B, Aboussouan LS. Noninvasive positive pressure ventilation for stable outpatients: CPAP and beyond. Cleve Clin J Med. 2010;77(10):705–14. doi: 10.3949/ccjm.77a.10060. [DOI] [PubMed] [Google Scholar]
- 6.Review Manager (RevMan) [Computer program]. Version 5.1. Copenhagen (DK) The Nordic Cochrane Centre, The Cochrane Collaboration. 2011 [Google Scholar]
- 7.Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, et al. Grading quality of evidence and strength of recommendations. BMJ. 2004;328(7454) doi: 10.1136/bmj.328.7454.1490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Guyatt GH, Oxman AD, Schunemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. J Clin Epidemiol. 2011;64(4):380–2. doi: 10.1016/j.jclinepi.2010.09.011. [DOI] [PubMed] [Google Scholar]
- 9.Kolodziej MA, Jensen L, Rowe B, Sin D. Systematic review of noninvasive positive pressure ventilation in severe stable COPD. Eur Respir J. 2007;30(2):293–306. doi: 10.1183/09031936.00145106. [DOI] [PubMed] [Google Scholar]
- 10.Goodman C. Literature searching and evidence interpretation for assessing health care practices. Stockholm, Sweden: Swedish Council on Technology Assessment in Health Care. 1996 doi: 10.1017/s0266462300008321. SBU Report No. 119E. [DOI] [PubMed] [Google Scholar]
- 11.Wijkstra PPJ, Lacasse Y, Guyatt GH, Goldstein R, Struik F. Nocturnal non-invasive positive pressure ventilation for stable chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews 2002, Issue 2. doi: 10.1002/14651858.CD002878. Art. No.: CD002878. DOI: 10.1002/14651858.CD002878. [DOI] [PubMed] [Google Scholar]
- 12.Renston JP, DiMarco AF, Supinski GS. Respiratory muscle rest using nasal BiPAP ventilation in patients with stable severe COPD. Chest. 1994;105(4):1053–60. doi: 10.1378/chest.105.4.1053. [DOI] [PubMed] [Google Scholar]
- 13.Casanova C, Celli BR, Tost L, Soriano E, Abreu J, Velasco V, et al. Long-term controlled trial of nocturnal nasal positive pressure ventilation in patients with severe COPD. Chest. 2000;118(6):1582–90. doi: 10.1378/chest.118.6.1582. [DOI] [PubMed] [Google Scholar]
- 14.Diaz O, Begin P, Torrealba B, Jover E, Lisboa C. Effects of noninvasive ventilation on lung hyperinflation in stable hypercapnic COPD. Eur Respir J. 2002;20(6):1490–8. doi: 10.1183/09031936.02.00034402. [DOI] [PubMed] [Google Scholar]
- 15.Gay PC, Hubmayr RD, Stroetz RW. Efficacy of nocturnal nasal ventilation in stable, severe chronic obstructive pulmonary disease during a 3-month controlled trial. Mayo Clin Proc. 1996;71(6):533–42. doi: 10.4065/71.6.533. [DOI] [PubMed] [Google Scholar]
- 16.Clini E, Sturani C, Rossi A, Viaggi S, Corrado A, Donner CF, et al. The Italian multicentre study on noninvasive ventilation in chronic obstructive pulmonary disease patients. Eur Respir J. 2002;20(3):529–38. doi: 10.1183/09031936.02.02162001. [DOI] [PubMed] [Google Scholar]
- 17.Diaz O, Begin P, Andresen M, Prieto ME, Castillo C, Jorquera J, et al. Physiological and clinical effects of diurnal noninvasive ventilation in hypercapnic COPD. Eur Respir J. 2005;26(6):1016–23. doi: 10.1183/09031936.05.00033905. [DOI] [PubMed] [Google Scholar]
- 18.Sin DD, Wong E, Mayers I, Lien DC, Feeny D, Cheung H, et al. Effects of nocturnal noninvasive mechanical ventilation on heart rate variability of patients with advanced COPD. Chest. 2007;131(1):156–63. doi: 10.1378/chest.06-1423. [DOI] [PubMed] [Google Scholar]
- 19.McEvoy RD, Pierce RJ, Hillman D, Esterman A, Ellis EE, Catcheside PG, et al. Nocturnal non-invasive nasal ventilation in stable hypercapnic COPD: a randomised controlled trial. Thorax. 2009;64(7):561–6. doi: 10.1136/thx.2008.108274. [DOI] [PubMed] [Google Scholar]
- 20.Redelmeier DA, Bayoumi AM, Goldstein RS, Guyatt GH. Interpreting small differences in functional status: the Six Minute Walk test in chronic lung disease patients. Am J Respir Crit Care Med. 1997;155(4):1278–82. doi: 10.1164/ajrccm.155.4.9105067. [DOI] [PubMed] [Google Scholar]
- 21.Holland AE, Hill CJ, Rasekaba T, Lee A, Naughton MT, McDonald CF. Updating the minimal important difference for six-minute walk distance in patients with chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2010;91(2):221–5. doi: 10.1016/j.apmr.2009.10.017. [DOI] [PubMed] [Google Scholar]
- 22.Puhan MA, Mador MJ, Held U, Goldstein R, Guyatt GH, Schunemann HJ. Interpretation of treatment changes in 6-minute walk distance in patients with COPD. Eur Respir J. 2008;32(3):637–43. doi: 10.1183/09031936.00140507. [DOI] [PubMed] [Google Scholar]
- 23.Budweiser S, Jorres RA, Pfeifer M. Noninvasive home ventilation for chronic obstructive pulmonary disease: indications, utility and outcome. Curr Opin Pulm Med. 2008;14(2):128–34. doi: 10.1097/MCP.0b013e3282f379fc. [DOI] [PubMed] [Google Scholar]
- 24.Hill NS. Noninvasive ventilation for chronic obstructive pulmonary disease. Respir Care. 2004;49(1):72–87. [PubMed] [Google Scholar]