

Abstract
Background
Commutable reference materials (RMs) are suitable for end-users for evaluating the metrological traceability of values obtained using routine measurement systems. We assessed the performance of 6 routine measurement systems with validated secondary RMs.
Methods
We tested the homogeneity, stability, and commutability of 5 minimally processed human serum pools according to the standard guidelines. The serum pools were assigned values as per the reference procedure of the United States Centers for Disease Control and were used to evaluate the trueness of results from 6 commercial measurement systems based on enzymatic methods: 3 glucose oxidase (GOD) and 3 hexokinase (HK) methods.
Results
The prepared RMs were validated to be sufficiently homogenous, stable, and commutable with the patient samples. Method bias varied for different systems: GOD01, -0.17 to 2.88%; GOD02, 1.66 to 4.58%; GOD03, -0.17 to 3.14%; HK01, -3.48 to -0.85%; HK02, -3.83 to -0.11%, and HK03, -1.82 to -0.27%.
Conclusions
We observed that the prepared serum glucose RMs were qualified for trueness assessment. Most of the measurement systems met the minimal quality specifications.
Keywords: Glucose, Reference material, Commercial system, Bias
INTRODUCTION
Determination of serum glucose level is extremely important for the screening, diagnosis, and monitoring of diabetes mellitus. It is recommended that the concentration of glucose be measured in an accredited laboratory to ensure accuracy [1]. The commonly used systems for glucose measurement are usually based on enzymatic methods, including glucose oxidase (GOD)-peroxidase (POD) method, GOD-oxygen electrode method, GOD-dry chemistry method, and hexokinase (HK) glucose-6-phosphate dehydrogenase (G6PD) method. Different methods and instruments lead to variations in the results from different laboratories [2-4]. It is important that the assays be standardized and harmonized.
The International Organization of Standardization (ISO) 17511 standard describes the manner of establishing a reference system for standardization of measurements in clinical laboratories. The reference material (RM) is a key component of such a reference system. Through an intermediate trueness transfer with the RM, commercial methods with validated calibrators may produce values for patient samples that are traceable to the reference method. However, some commercial systems for enzyme measurement continue producing non-traceable values because of a lack of validated calibrations [5, 6]. Hence, the traceability of glucose measurements ascertained by manufacturers may be questioned by the end-users in routine laboratories. The primary RMs for glucose measurement with the highest metrological level are available at the American National Institute of Standards and Technology (NIST). High costs and difficult transportation limit the widespread use of these NIST RMs for trueness assessment. The aim of this study was to prepare secondary RMs for glucose measurement by using commutable frozen human serum pools and to evaluate the traceability of glucose measurements by routine systems using the prepared RMs.
METHODS
1. Preparation and characteristic of the RMs
Collection and preparation of the RMs were performed with the permission of the Clinical Research Ethics Committee of the Peking University First Hospital. Leftover sera collected from apparently healthy people who had come to the hospital for a physical examination were used in the preparation. Hemolytic, icteric, and lipemic samples were excluded from the study. To obtain a serum pool with a low glucose concentration (about 3.0 mmol/L), whole blood samples were kept at 4℃ for 48 hr before serum-clot separation. Glucose powder (product no. L7626; Sigma, St. Louis, MO, USA) was spiked into the pool to produce 4 more levels of RMs. Concentrations of the 5 RMs were in the linear measurement range for the assay method. The materials were sterile-filtered before transferring them into freezing vials for storage at -70℃ as performed in a previous study [7]. During the dispensing procedure, the environmental moisture content was maintained between 50-70%, and the vials filled with sera were sealed quickly to avoid evaporation.
The homogeneity of the materials was assessed by evaluating vial-to-vial variation. We randomly selected 15 vials from each level. Analysis of each vial was performed in triplicate by using the Beckman DxC800 analyzer (Beckman Coulter Inc., Brea, CA, USA). The data were evaluated by using one-way analysis of variance. Stability of the glucose concentration in the materials was evaluated at the room temperature, 4℃, -20℃, and -70℃ [8]. The materials were analyzed in triplicate at various time intervals. Commutability of the reference materials was determined by measuring glucose concentration in the patient specimens using 6 routine commercial systems (Table 1) and the results were compared with those obtained by the reference procedure. We collected 40 patient sera with glucose concentration in the range of 1.9 to 22.0 mmol/L at our laboratory. They were aliquoted and stored at -20℃ until use. Regression analysis was performed to establish the relationship between the results for the patient samples obtained by the routine measurement procedures and by the reference method. Two-tailed 95% prediction interval of the regression line was calculated. Results for the RMs were compared with those for the patient samples. The RMs were considered commutable if their results were within the prediction interval [9, 10].
Table 1.
Relative bias for glucose measurement using 6 commercial systems

Relative bias: The difference (in%) between the mean value of the same systems in 3 labortories and the target value of the RM; *the bias (bias>3.4%) exceeded the minimal quality specifications.
Abbreviations: HK, hexokinase; GOD, glucose oxidase; POD, peroxidase; G6PD, glucose-6-phosphate dehydrogenase; ID-MS, isotope dilution-mass spectrometry; RM, reference material.
2. Value assignment for RMs
Traceable values were assigned to the RMs by using the reference method recommended by the United States Centers for Disease Control (CDC) [11]. These measurements were perform ed by the laboratory of the Peking University First Hospital, which had achieved good results in the International Federation of Clinical Chemistry and Laboratory Medicine external quality assessment scheme for reference laboratories in laboratory medicine in 2008 [12]. However, we observed a maximum bias of -2.5% when the NIST Standard Reference Material (SRM) 965a materials were measured. Therefore, we recalibrated the reference method with the NIST SRM965a material (4 levels) instead of the glucose aqueous solution. One new vial of the RMs was tested twice every day for 3 consecutive days. Then, the data were screened for the outlying values with the Grubbs test [13]. The mean value was considered the certified value. The uncertainty of the certified value was estimated by addition of the values for characterization, homogeneity, long stability, and stability during transport [14]. The RMs were transported on dry ice so that the uncertainty of their stability during transport could be negligible. The reported uncertainty was based on the combined uncertainty multiplied by the coverage factor of K=2, corresponding to a confidence interval of 95%.
3. Traceability survey
Traceability survey for glucose measurement was performed for 6 commercial systems in 3 laboratories (Table 1). The systems were well maintained by the manufacturer's engineer prior to the survey. Each RM was assayed in triplicates strictly as per the instructions of the manufacturer. Mean values from the replicates were used for calculation. The routine procedures and the reference method were compared by performing linear regression analysis according to the non-parametric Passing and Bablok method [15].
RESULTS
1. Properties of the RMs
We obtained 700 vials for RMs of every level. No significant vial-to-vial variation was detected by the analysis of variance (P > 0.05). Therefore, the materials were considered sufficiently homogeneous. The materials were stable at least for 3 days at room temperature, for 14 days at 4℃, and for 28 days at -20℃, when their concentration did not change beyond 1%. The RMs were stored at -70℃ for 1 yr, and their concentration changes were only between -1.3% and 1% (Fig. 1). The results for all the materials were within the prediction interval of the regression line between each commercial system and the reference procedure (Fig. 2); hence, the materials were concluded to be commutable.
Fig. 1.

The stability observation of the RMs for storage at -70℃.
Abbreviation: RM, reference material.
Fig. 2.

Commutability assessment of the RMs for the reference method and the commercial system by using the regression line (continuous line) and 95% prediction interval (dashed line). Black squares represent the RMs and gray circles represent the 40 patient samples.
Abbreviations: GOD, glucose oxidase; HK, hexokinase.
2. Assigned values
Among the measurements with the reference method, no outlying individual result was detected. The uncertainties of the SRM-965a materials and the linear calibration were taken into account. The glucose values and the expanded uncertainties assigned to the RMs were as follows: 3.13±0.14 mmol/L for RM1, 6.03±0.13 mmol/L for RM2, 9.34±0.16 mmol/L for RM3, 13.72±0.17 mmol/L for RM4, and 18.78±0.20 mmol/L for RM5
3. Traceability of the results from the commercial systems
A small variation (CV<3%) was observed in the results of the same assay system from 3 laboratories. Table 1 summarizes the method bias for each system: GOD01, -0.17 to 2.88%; GOD02, 1.66 to 4.58%; GOD03, -0.17 to 3.14%; HK01, -3.48 to -0.85%; HK02, -3.83 to -0.11%; and HK03, -1.82 to -0.27%. Most of the systems met the minimal quality specifications (bias<3.3%), and only the HK03 system met the desirable specification (bias<2.2%) as per the biological variability [16]. The method biases versus the target values and their uncertainties are shown in Fig. 3. Considering the uncertainties, the systems GOD01 and GOD03 showed a small positive bias. The GOD02 system showed an obviously positive bias when the RM from the higher level was measured. The HK01 and HK02 systems showed a small negative bias for the middle-level RM. The HK03 system performed well, with results mostly within the range of the uncertainties.
Fig. 3.

Mean values±2 SDs of the results from 3 laboratories with 6 commercial systems. The gray area represents the assigned value and its expanded uncertainty for the reference material.
Regression analysis (Table 2) showed that the results of all the commercial systems were strongly correlated with those of the reference method (r≥0.9998). The slope value of the regression line for the GOD02 system (1.0483) showed the highest positive bias from the value of 1. Among the other systems, slope values for the GOD01 and GOD03 systems were higher than those for the other 3 systems, but they were all close to 1 (0.981 to 1.032). All the intercept values were close to 0 (-1.05 to -0.123).
Table 2.
Regression analysis between the United States Centers for Disease Control reference procedures (X-axis) and the 6 commercial systems (Y-axis)
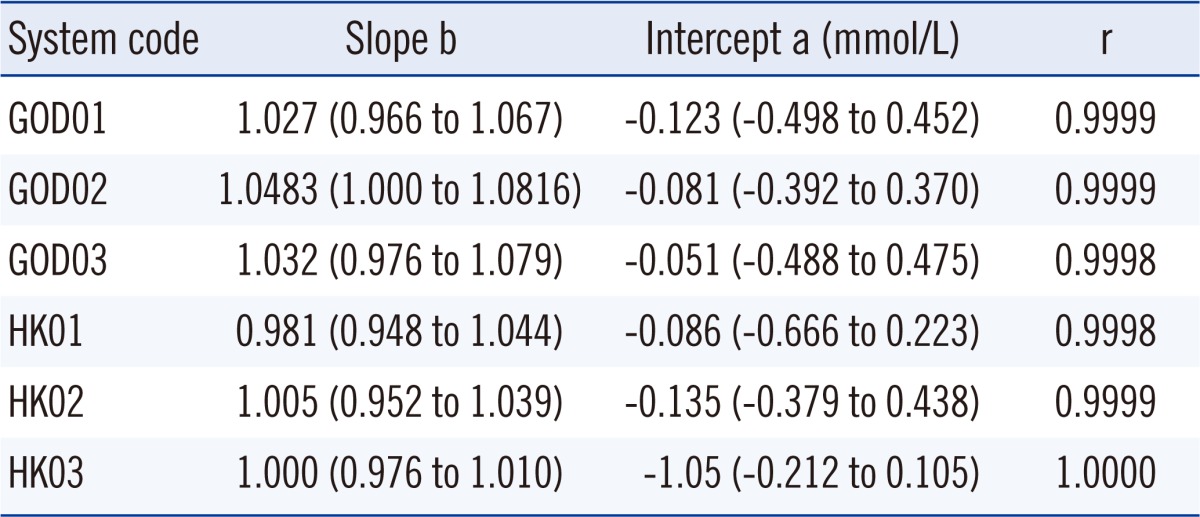
The values in the parentheses are of 95% confidence interval.
Abbreviations: GOD, glucose oxidase; HK, hexokinase.
DISCUSSION
Currently, serum glucose is determined using enzyme assays from various commercially available kits. However, a thorough evaluation of their accuracy is required. In this study, 5 frozen human serum pools were prepared and validated as secondary RMs to demonstrate the traceability of glucose measurements using routine assay systems. There are 2 reference methods for glucose measurement recommended by the Joint Committee for Traceability in Laboratory Medicine. One is the isotope dilution mass spectrometry method and another is the CDC HK-G6PD reference method. The HK method, which is less expensive and time consuming, was chosen to assign values to our RMs. In this study, the 5 RMs were minimally processed to keep the matrix as close to the fresh serum as possible [7]. They were observed to be homogenous, stable, and perfectly commutable with the fresh patient samples.
The uncertainties of the RMs in our study were slightly higher than those of NIST SRM965a. The certified concentrations of NIST SRM965a and their uncertainties in mmol/L were as follows: 1.918±0.020 for level 1; 4.357±0.048 for level 2; 6.777±0.073 for level 3; and 16.24±0.19 for level 4. The uncertainties of the RMs with a concentration less than 16 mmol/L were about 2 to 3 times higher than those of the SRM965a, and the uncertainty of RM5 was similar to that of SRM 965a level 4, the reason for which is that the calibration uncertainties were considered in the uncertainty calculation. The uncertainty of the calibration attributed a lot to the total uncertainties, especially in the low-concentration levels, which included 3 things: uncertainty of the SRM965a, uncertainty of the calibration equation, and uncertainty of value assignment.
In our study, most of the commercial measurement systems showed a good agreement with the reference method. The accuracy of glucose measurements seems to be associated more with the methodology than with the instrument, which was not observed in another study [17]. Routine HK methods showed a higher accuracy than GOD methods, which is in line with a report from Korea [18]. The biases investigated in China were higher than those in Korea, which maybe attributable to the differences in the number of laboratories and composition of the assay system.
Among the tested systems, the HK03 system showed the best performance with the smallest bias, which was similar to the results of a previous study [17]. The GOD03 system using dry chemistry method showed a small positive bias, but the bias was within the allowable bias range. The apparent difference between dry and wet chemistry systems [19] was not observed in our investigation because the RMs that we prepared were commutable. The HK01 and HK02 systems exceeded the allowable bias in the measurements of low-level RM. The allowable bias is determined on the basis of biological variability, an excess of which is considered clinically significant and would compromise the interpretation of results for diagnostic or monitoring decisions [20, 21]. Results of the regression analysis led to the same conclusion for these systems.
The GOD02 and HK02 systems were from the same manufacturer. The GOD02 system showed apparent positive bias, whereas the HK02 system showed a good performance. These divergent results may be attributed to the same value of the calibrator in the 2 methods, but the commutability of the calibrator is uncertain [22, 23]. Harmonization of routine methods regardless of the manufacturer and methodology is important, and hence, commutable calibrators for traceability are critical to ensure this goal.
Acknowledgement
Our study was supported by the National 863 Plan Projects (2006AA020909) and Capital Foundation of Medical Development of China. The authors gratefully acknowledge the co-operation of the manufacturers-Beckman, Dade, Roche, and Ortho.
Footnotes
No potential conflicts of interest relevant to this article were reported.
References
- 1.American Diabetes Association. Standards of medical care in diabetes--2010. Diabetes Care. 2010;33(Suppl 1):S11–S61. doi: 10.2337/dc10-S011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Genter PM, Ipp E. Accuracy of plasma glucose measurements in the hypoglycemic range. Diabetes Care. 1994;17:595–598. doi: 10.2337/diacare.17.6.595. [DOI] [PubMed] [Google Scholar]
- 3.Thienpont LM, Stöckl D, Kratochvíla J, Friedecký B, Budina M. Pilot external quality assessment survey for post-market vigilance of in vitro diagnostic medical devices and investigation of trueness of participants' results. Clin Chem Lab Med. 2003;41:183–186. doi: 10.1515/CCLM.2003.030. [DOI] [PubMed] [Google Scholar]
- 4.Gambino R. Glucose: a simple molecule that is not simple to quantify. Clin Chem. 2007;53:2040–2041. doi: 10.1373/clinchem.2007.094466. [DOI] [PubMed] [Google Scholar]
- 5.Jansen R, Schumann G, Baadenhuijsen H, Franck P, Franzini C, Kruse R, et al. Trueness verification and traceability assessment of results from commercial systems for measurement of six enzyme activities in serum: an international study in the EC4 framework of the Calibration 2000 project. Clin Chim Acta. 2006;368:160–167. doi: 10.1016/j.cca.2005.12.033. [DOI] [PubMed] [Google Scholar]
- 6.Xia C, Tong Q, Wang Q, Tang Z, Qi L, Chi S, et al. Application of five frozen human-pooled serum samples assigned by the International Federation of Clinical Chemistry and Laboratory Medicine reference procedure in a traceability investigation of gamma-glutamyltransferase catalytic concentration measurements in China. Ann Clin Biochem. 2010;47:189–194. doi: 10.1258/acb.2009.009210. [DOI] [PubMed] [Google Scholar]
- 7.Henriksen GM, Pedersen MM, Norgaard I, Blom M, Blou L, Blaabjerg O, et al. Minimally processed fresh frozen human reference sera: preparation, testing, and application to international external quality assurance. Scand J Clin Lab Invest. 2004;64:293–308. doi: 10.1080/00365510410006612. [DOI] [PubMed] [Google Scholar]
- 8.Linsinger T, Pauwels J, van der Veen A, Schimmel H, Lamberty A. Homogeneity and stability of reference materials. Accred Qual Assur. 2001;6:20–25. [Google Scholar]
- 9.Clinical and Laboratory Standards Institute (CLSI) Characterization and qualification of commutable reference materials for laboratory medicine. Approved guideline, C53-A. Wayne, PA: Clinical and Laboratory Standards Institute; 2010. [Google Scholar]
- 10.Infusino I, Braga F, Valente C, Panteghini M. Commutability of the ERM-DA470 reference material for two assays measuring serum albumin using immunochemical principles. Clin Chem Lab Med. 2011;49:1383–1384. doi: 10.1515/CCLM.2011.619. [DOI] [PubMed] [Google Scholar]
- 11.Neese J, Duncan P, Bayse D, Robinson M, Cooper T, Stewart C. Development and evaluation of a hexokinase/glucose-6-phosphate dehydrogenase procedure for use as a national glucose reference method. Atlanta: Center for Disease Control; 1976. [Google Scholar]
- 12.RELA-IFCC External Quality assessment scheme for Reference Laboratories in Laboratory Medicine. [Updated in 2011]. http://www.dgkl-rfb.de:81/index.shtml. [DOI] [PubMed]
- 13.Snedecor G, Cochran W. Statistical methods. 8th ed. Ames: Iowa State University Press; 1989. pp. 278–280. [Google Scholar]
- 14.Pauwels J, van der Veen A, Lamberty A, Schimmel H. Evaluation of uncertatinty of reference materials. Accred Qual Assur. 2000;5:95–99. [Google Scholar]
- 15.Passing H, Bablok W. A new biometrical procedure for testing the equality of measurements from two different analytical methods. Application of linear regression procedures for method comparison studies in clinical chemistry, Part I. J Clin Chem Clin Biochem. 1983;21:709–720. doi: 10.1515/cclm.1983.21.11.709. [DOI] [PubMed] [Google Scholar]
- 16.Fraser C. Biological Variation: From Principles to Practice. Washington, DC: AACC Press; 2001. [Google Scholar]
- 17.Miller WG, Myers GL, Ashwood ER, Killeen AA, Wang E, Ehlers GW, et al. State of the art in trueness and interlaboratory harmonization for 10 analytes in general clinical chemistry. Arch Pathol Lab Med. 2008;132:838–846. doi: 10.5858/2008-132-838-SOTAIT. [DOI] [PubMed] [Google Scholar]
- 18.Lee W, Chung HJ, Hannestad U, Kim S, Chun S, Park JY, et al. Trueness assessment of Korean nation-wide glucose proficiency testing. Clin Chem Lab Med. 2011;49:1061–1064. doi: 10.1515/CCLM.2011.169. [DOI] [PubMed] [Google Scholar]
- 19.Pedersen MM, Ornemark U, Rustad P, Steensland H, Loikkanen M, Olafsdottir E, et al. The Nordic Trueness Project 2002: use of reference measurement procedure values in a general clinical chemistry survey. Scand J Clin Lab Invest. 2004;64:309–320. doi: 10.1080/00365510410002805. [DOI] [PubMed] [Google Scholar]
- 20.Ricós C, Alvarez V, Cava F, García-Lario JV, Hernández A, Jiménez CV, et al. Current databases on biological variation: pros, cons and progress. Scand J Clin Lab Invest. 1999;59:491–500. doi: 10.1080/00365519950185229. [DOI] [PubMed] [Google Scholar]
- 21.Fraser CG, Hyltoft Petersen P, Libeer JC, Ricos C. Proposals for setting generally applicable quality goals solely based on biology. Ann Clin Biochem. 1997;34:8–12. doi: 10.1177/000456329703400103. [DOI] [PubMed] [Google Scholar]
- 22.Brion E, Lessinger JM, Gould N, Leyendecker J, Ferard G. Evaluation of commutability of control materials. Clin Chem Lab Med. 2002;40:625–630. doi: 10.1515/CCLM.2002.108. [DOI] [PubMed] [Google Scholar]
- 23.Gubern G, Canalias F, Gella FJ. Determination of alpha-amylase activity: methods comparison and commutability study of several control materials. Clin Chem. 1995;41:435–438. [PubMed] [Google Scholar]