

Abstract
Context
Home-visiting programs have been offered for more than sixty years to at-risk families of newborns and infants. But despite decades of experience with program delivery, more than sixty published controlled trials, and more than thirty published literature reviews, there is still uncertainty surrounding the performance of these programs. Our particular interest was the performance of home visiting in reducing child maltreatment.
Methods
We developed a program logic framework to assist in understanding the neonate/infant home-visiting literature, identified through a systematic literature review. We tested whether success could be explained by the logic model using descriptive synthesis and statistical analysis.
Findings
Having a stated objective of reducing child maltreatment—a theory or mechanism of change underpinning the home-visiting program consistent with the target population and their needs and program components that can deliver against the nominated theory of change—considerably increased the chance of success. We found that only seven of fifty-three programs demonstrated such consistency, all of which had a statistically significant positive outcome, whereas of the fifteen that had no match, none was successful. Programs with a partial match had an intermediate success rate. The relationship between program success and full, partial or no match was statistically significant.
Conclusions
Employing a theory-driven approach provides a new way of understanding the disparate performance of neonate/infant home-visiting programs. Employing a similar theory-driven approach could also prove useful in the review of other programs that embody a diverse set of characteristics and may apply to diverse populations and settings. A program logic framework provides a rigorous approach to deriving policy-relevant meaning from effectiveness evidence of complex programs. For neonate/infant home-visiting programs, it means that in developing these programs, attention to consistency of objectives, theory of change, target population, and program components is critical.
Keywords: Policy-relevant evidence synthesis, complex interventions, infant home visiting
Background
Home-visiting programs have been offered for more than sixty years, with the aim of creating a safe and nurturing environment for newborns and infants and preventing child abuse and neglect. Home-visiting programs involve the use of a professional (such as a nurse or social worker) or a trained paraprofessional or layperson to make regular visits in the home of a mother (or family) commencing prenatally or soon after the birth of a baby. Home visits are provided for anything from a few months to two or more years, with more visits (e.g., weekly) closer to the birth and fewer (e.g., monthly) as the child grows. The general aim is to improve outcomes for mothers and babies.
The Nurse Family Partnership (NFP) developed by Olds (Olds et al. 1986, 1997) is perhaps the best-known home-visiting program. Home-visiting programs are now implemented widely, covering many thousands of families across the United States (Barth 1991; Bugental and Schwartz 2009; Duggan et al. 2004; Gessner 2008; Hardy and Streett 1989; Lutzker and Rice 1984; Schuler et al. 2000), the United Kingdom (Barlow et al. 2007; Wiggins et al. 2005), Canada (Infante-Rivard et al. 1989; Larson 1980; Steel O’Connor et al. 2003), Australia (Armstrong et al. 1999; Kemp et al. 2008), and elsewhere, including Syria (Bashour et al. 2008), New Zealand (Fergusson et al. 2005), Norway (Kaaresen et al. 2006) and Japan (Cheng et al. 2007).
Home-visiting programs have a number of possible objectives, including the health of the baby (e.g., immunization, breast-feeding), safety (e.g. general risks, maltreatment), school readiness, and positive parenting (e.g. infant mother bonding and responding to cues). The focus of this article is home visiting for the prevention of child maltreatment. Child maltreatment—defined as any act of commission or omission by a parent or caregiver that results in harm, or the threat of harm, to a child—is widespread and of global concern (WHO 2006). As reported by Gilbert and colleagues (Gilbert et al. 2009a, 2009b), population surveys in countries in the Organization for Economic Cooperation and Development put rates of child physical abuse at 4 to 16 percent and neglect at 1.4 to 15.4 percent.
In Australia, rates of child physical and/or sexual abuse are estimated at 15.5 percent, based on the national mental health and well-being survey (ABS 2008; Reeve and van Gool 2010). Furthermore, rates of child maltreatment notifications in Australia nearly trebled between 2000/2001 and 2008/2009, from 115,471 to 339,454 (Productivity Commission 2011), placing considerable pressure on child protection services and calls for investment in preventive services.
Child maltreatment has well-documented adverse outcomes across many domains, contemporaneous with the abuse and extending many years into the future. It is associated with poor mental and physical health, high rates of suicide, poor physical health, low educational outcomes, high involvement in crime, incarceration, substance abuse, behavioral problems, homelessness, welfare dependency, and unemployment (Dube et al. 2003; Eckersley 1988; Evans, Hawton, and Rodham 2005; Gilbert et al. 2009b; Peden et al. 2008; Pinheiro 2006; Reeve and van Gool 2010; Thornberry et al. 2010; WHO 2010).
Home visiting in the prenatal and early childhood period is an identified strategy for reducing child abuse and neglect. But despite decades of experience with the delivery of home-visiting programs and more than sixty published controlled trials and numerous literature reviews, the performance of home visiting is still reported as equivocal. In this article, we review the literature using a theory-driven framework in an attempt to bring greater clarity to understanding the disparate evidence base.
Existing Evidence Base
Using a standard search strategy (described later), we identified fifteen systematic literature reviews (including two meta-analyses) with a focus on home visiting as an intervention to prevent child maltreatment or risk factors for maltreatment. The number of programs covered in the reviews varied from two to sixty, reflecting distinct inclusion and exclusion criteria (see table 1).
TABLE 1.
Key Conclusions of Fifteen Reviews of Neonate/Infant Home-Visiting Studies
| Review and Number of Primary Studies | Focus of Review | Conclusions |
|---|---|---|
| Bilukha et al. 2005; 25 studies | To assess the effectiveness of home-visitation programs in preventing violence. | “Study findings are inconsistent.”…“The evidence is insufficient to determine the effectiveness of early home interventions in preventing violence by visited children or visited parents or in preventing intimate partner violence” (p. 17). |
| Doggett, Burrett, and Osborn 2005; 6 studies | Effect of pre- and/or postnatal home visits for women with a drug or alcohol problem. | “This review failed to find evidence that home visits reduced the risk of continuing drug or alcohol use” (p. 18). |
| Drummond, Weir, and Kysela 2002; 14 articles on 9 programs. | Focuses on program components, practices, outcomes and quality to understand considerable variation across studies. | “Progress in evaluation of home visitation has been made, but much remains to be clarified” (p. 157). |
| Gonzalez and MacMillan 2008; 3 home visiting studies | Restricted to controlled trials of very stringent methodological criteria. | “The development of future programs needs to be theoretically driven” (p. 284). |
| Guterman 1999; 19 studies | Examines outcomes linked with differing screening and enrolment strategies. | “Population-based enrolment strategies appear favourable to screening-based ones in early home visitation programs seeking to prevent physical child abuse and neglect” (p. 863). |
| Hahn et al. 2003; 21 studies and 26 intervention arms | Effectiveness of early childhood home visiting in preventing violence. | “The Task Force found insufficient evidence to determine the effectiveness of early childhood home visitation in preventing violence by visited children and between adults” (p. 7). |
| Howard and Brooks-Gunn 2009; 9 RCTs | Early intervention–families recruited prenatally or around birth, stated aim to improve parenting and prevent child abuse and neglect. | “A review of the literature reveals a mixed picture regarding the efficacy of home-visiting programs” (p. 17). |
| Kearney, York, and Deatrick 2000; 20 random or quasi-RCTs | The characteristics of nurse-delivered home visiting in the U.S. and Canada that improve maternal health, parenting skills, maternal-child interaction, child health and development, and use of well child health care. | “In nurse-delivered home visiting interventions to young families and preterm and full-term infants, maternal well-being and life course development, maternal-infant interaction, and parenting often improved, but child development gains mainly were limited to preterm infants” (p. 375). |
| Kendrick et al. 2000; 17 studies reporting HOME scores. | Restricted to studies reporting HOME score (that measures parenting quality and safety of home environment for raising children). | “Our review of the effectiveness of home visiting programmes suggests they are effective in increasing the quality of the home environment as measured by HOME scores” (p. 447). |
| MacMillan et al. 2009; 2 home visiting models (NFP & Early Start) | Effect on the five major subtypes of child maltreatment of two high-profile nurse-visiting programs; Nurse Family Partnership and Early Start (Fergusson et al. 2005). | “Despite the promotion of a broad range of early childhood home visiting programmes, most of these have not been shown to reduce physical abuse and neglect when assessed using RCTs” (p. 251). |
| McNaughton 2004; 13 studies | Nurse home-visiting interventions. | “Many important issues about the implementation of home-visiting programs that impact their success or failure remain unclear” (p. 217). |
| Mikton and Butchart 2009; 26 reviews of 17 home visiting programs | Synthesize recent evidence from reviews on the effectiveness of universal and selective child maltreatment prevention, evaluating methodological quality. | “Reviews suggest that early home visitation programmes are effective in reducing risk factors for child maltreatment, but whether they reduce direct measures is less clear-cut” (p. 354). |
| Roberts, Kramer, and Suissa 1996; 11 random or quasi-RCTs | Quantify the effectiveness of home visiting programs in preventing child injury and child abuse. | “The effect of home visiting on the occurrence of child abuse varied across studies in both magnitude and direction” (p. 312). |
| Shaw et al. 2006; 22 studies in their review; 8 were of home visiting for neonates or infants | Postpartum support strategies and maternal knowledge, attitudes, and | “No RCT evidence is available to endorse universal provision of postpartum support to improve parenting, maternal mental |
| skills related to parenting, maternal mental and physical health, and quality of life. | health, maternal quality of life, or maternal physical health.” … “There is some evidence that high-risk populations may benefit from postpartum support” (p. 219). | |
| Sweet and Appelbaum 2004; 60 programs | Address the broad question of whether home-visiting programs help families across a variety of child and parent/maternal outcomes. | “What exactly makes a home visiting program successful is unclear at this time.” … “Home visiting does seem to help families with young children, but the extent to which this help is worth the cost of creating and implementing programs has yet to be determined” (p. 1448). |
Most of the reviews reported on many outcomes. These might include one or more direct child maltreatment measures (child abuse reports or substantiations, out-of-home placement) plus predictors of child maltreatment (such as parenting knowledge, attitudes, or behaviors) or indirect evidence of maltreatment (such as injury hospitalizations or child health development).
All the reviews sought to assess the overall performance of home visiting, for programs “within scope,” with some also seeking to describe the characteristics predictive of success (Drummond, Weir, and Kysela 2002; Kearney, York, and Deatrick 2000; Sweet and Appelbaum 2004). The reviews generally reported mixed results across outcome measures and struggled to generate meaning from the mixed findings. As reported in table 1, the conclusion of most of the reviews, including the high quality comprehensive review by Sweet and Appelbaum (2004), was that the evidence of success was equivocal. Only the review by Kendrick and colleagues (Kendrick et al. 2000) concluded that home visiting was successful, although their review was restricted to studies reporting HOME scores (a multicomponent questionnaire measuring the nurturing potential of the home/parenting environment).
A range of reasons were offered to explain why the performance of home-visiting programs might appear inconclusive. These included possible error that was caused by the poor reliability and validity of measures (McNaughton 2004), the possibility that “certain outcome data are selectively omitted from published reports because the results fail to reach significance” (Roberts, Kramer, and Suissa 1996, 31), a follow-up period that was too short (McNaughton 2004), and possible “surveillance bias” (a higher rate of abuse notification related to contact with the home visitor). More commonly, the reviewers postulated that the considerable diversity in home-visiting programs was largely responsible for the confusion. The programs varied with respect to models of service delivery (when commenced and at what age concluded, number and length of home visits), target population (risk profile, cultural group), home visitor (qualifications, training, supervision), and program components (use of multidisciplinary team, access to specialist services such as counseling, drug and alcohol services, job placement, child care).
Several reviewers reported specific program features predictive of success, such as targeting of low-income, first time adolescent mothers (Howard and Brooks-Gunn 2009) or those “at elevated risk of maltreatment” (Bilukha et al. 2005, 22); or when the program was delivered by professional visitors (Bilukha et al. 2005; Hahn et al. 2003) or when families received a longer and/or more intensive program (Bilukha et al. 2005; Howard and Brooks-Gunn 2009). Kearney and colleagues conclude that “effective nurse home visiting included nurses with advanced education, frequent visits over a long period of time, and were focused less on building parent resources, as in the social ecology model, and more on building a relationship with the mother and providing her with coaching in maternal-infant interaction and cognitive development” (Kearney, York, and Deatrick 2000, 375). But they also report uncertainty in the determinants of success. Sweet and Appelbaum, who reviewed sixty controlled trials, conclude that “what exactly makes a home visiting program successful is unclear at this time” (Sweet and Appelbaum 2004, 1448). Yet none of the reviews consider this issue in a rigorous way.
In short, despite the expectation that the attributes of home-visiting programs will affect performance, the reviews published to date have not established the determinants of success nor have they considered this question in a rigorous way. So despite dozens of random controlled trials (RCTs) and nearly as many reviews of home-visiting programs for neonates and infants, the current state of knowledge leaves policymakers without clear evidence-based advice.
Aim of Study
The aim of our study was to gain a new understanding of the home-visiting literature for the prevention of child maltreatment by taking a program logic approach that incorporated a theory of change.
We hypothesized that the success of home-visiting programs would reflect the consistency between (1) the stated or implied theory (mechanism) of change underpinning the program, (2) the target population and their specific needs, (3) the program components/activities, and (4) the program objectives. Figure 1 depicts the overall program logic incorporating these four levels. We sought to test this proposition by analyzing all the published control studies of infant/neonate home-visiting interventions to prevent child maltreatment or known risk factors that met our inclusion criteria.
FIGURE 1.
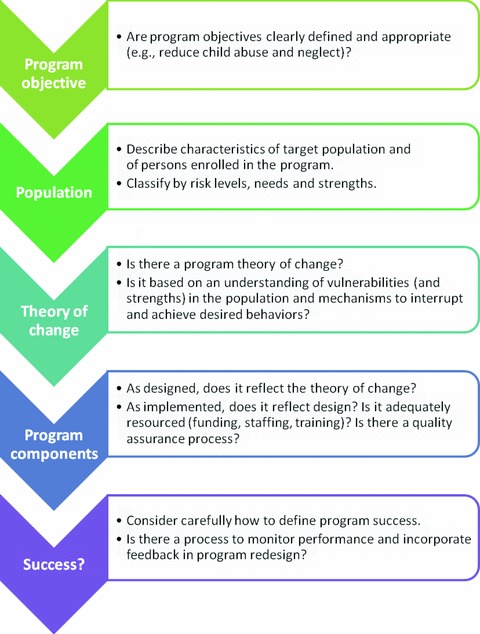
Program Logic Model for Reviewing Complex Interventions
The approach is complementary to theory-driven evaluation, in which the underlying theory and fidelity of implementation are central to explanations of program performance (Coryn et al. 2011). An overarching aim of our article is to encourage the use of program logic in the systematic review of complex interventions and to demonstrate how this may be achieved. Adopting a theory-driven approach to understanding the complex home-visiting literature has a powerful internal logic. It is also supported by evidence that behavior change programs developed according to a defined theory are more likely to be successful than those not so developed (Noar and Zimmerman 2005). Painter and colleagues (2008) estimated that only one-third of health-related behavior change studies explicitly identify an underlying theory, and that such identification affects success. In relation to infant home visiting, we postulate that greater attention to the underlying theory and the integrity of the theory with program components, target population, and objectives will provide a more coherent explanation of the observed results. For example, Gardner and colleagues used a theory-driven approach to evidence synthesis to review audit and feedback mechanisms in chronic disease management (Gardner et al. 2003) and it was found to assist in understanding program performance.
We are not aware that a program logic approach incorporating a theory of change has been applied previously to a review of the home-visiting literature in neonates and infants. Even though some of the reviews identify whether individual programs specify and use a theory (of change) in program development and implementation (McNaughton 2004) and others specify objectives for each program that may imply a theory of change (Drummond, Weir, and Kysela 2002; Howard and Brooks-Gunn 2009; Sweet and Appelbaum 2004), none formally connects these observations to the programs’ success.
In the evaluation of individual programs, it is not uncommon for a theory of change to be considered in assessing performance (e.g., Barnard et al. 1988), or for a theory-driven (program logic) approach to be adopted (Rogers et al. 2000). However, it is the use of a program logic framework for a systematic review, the approach taken here, that is unique.
Our program logic–based review, though consistent with the growing realist synthesis literature in arguing for a theory-driven approach to the review of complex interventions (Pawson et al. 2005), has some important differences. The realist synthesis approach proposes that context is paramount, such that universal conclusions are unlikely to be possible. Instead, our expectation is that by using a theory-driven approach, the importance of context—albeit central—will not preclude overarching conclusions being drawn, but that this is unlikely to be a set of universally effective program elements. That is, by using a theory-driven approach, what currently seems confusing in understanding predictors of success will become clear.
Methods
Our research had four phases:
Developing the criteria for the literature review, data extraction, and analysis for a systematic review of home visiting based on the program logic approach shown in figure 1.
Conducting a comprehensive literature search to identify all home-visiting programs meeting our inclusion criteria.
Extracting data using the established criteria including data on the programs’ performance.
Testing whether a match of the program theory, the program components, the target population, and the child maltreatment objective predicts success.
Criteria for Analyzing Home-Visiting Programs Using a Theory-Driven Approach
We developed a classification system to describe (1) the underlying theory or mechanism of change, (2) the target population, (3) the program components, (4) the program objective, (5) the definition of a program's success, and (6) the basis for classifying a match.
Theory Underpinning Home-Visiting Programs
The underlying theories of home-visiting programs to prevent child maltreatment draw on various literatures, including child development, attachment, health promotion, mental health, neuroscience, education and learning, and evolutionary biology. The discussion in this article represents a start on this complex area. It concentrates on the theories described in the child protection literature, for example drawing on the psychodynamic, sociological, social-psychological, and ecological theories (Sidebotham 2001).
We found that six reasonably distinct theoretical mechanisms (and associated theories of change) are commonly used to explain poor parenting and poor child outcomes. These were based on (modified and further developed) the state of Georgia's Child Abuse Prevention Theory of Change and Logic Model Early Childhood comprehensive systems implementation project, supported by the World Health Organization (WHO) (WHO 2011).
Lack of knowledge and skills regarding important topics like normal child development or how to look after or relate to a young infant by some mothers (and fathers) that undermines the quality of their parenting. For example, some of the early infant home-visiting programs reflect a knowledge and skills deficit model, such as the Parents as Teachers program developed in 1981 (Wagner and Clayton 1999).
Limited access to health care due to financial, cultural, logistical barriers, and/or competing priorities or chaotic life circumstances that compromises the physical health of the mother and baby (as might be seen in failure to thrive, failure to achieve baby milestones). Home visiting seeks to address this by providing direct access to the health and welfare system in the family's home (through the visitor/team) and through facilitating referral/access to other health and welfare services.
Social isolation of mothers as a predictor of child maltreatment (Runyan et al. 2002), reflecting the importance of good emotional and social support for new mothers when they are particularly vulnerable and at high risk of postpartum depression.
Disruptions to the mother-infant interaction and bonding and low maternal sensitivity affecting the ability to be a good parent, described in the attachment theory literature (Bowlby 1969/1982; Lyons-Ruth 2008). The crucial importance of early infancy (including in utero) and the mother-child relationship is emerging also from the neuroscience literature (Schore 2005).
A poor or compromised psychological state that undermines a mother's capacity to parent and poses a direct threat to the mother-infant attachment and meeting of the infant's basic physical and emotional needs. This risk can be exacerbated by drug and alcohol misuse and mental illness, especially when the mother was abused or neglected as a child (Amos, Furber, and Segal 2011). This would suggest a home-visiting program with a strong mental health capability.
Some home-visiting programs refer to an “ecological model,” which places the mother and child within the family, community, and societal context. The premise is that there are factors beyond the individual mother or child that limit the mother's capacity to parent. These factors could include a lack of employment opportunities, poor access to affordable housing, or inadequate social welfare support (Sidebotham 2001). Home-visiting programs that take an “ecological approach” may provide initiatives to support the wider economic and social context, for instance, supporting education or access to employment for the mother.
Target Population
Target populations were classified according to characteristics correlated to risk of abuse or threats to a safe and nurturing environment for the child (Runyan et al. 2002) in a way that would establish a hierarchical schema. We sought to balance complexity in the classification system with relative homogeneity within each population subgroup, resulting in five population subgroups, ranging from (1) low-risk / general population to (5) active abuse / domestic violence, with three intermediate risk levels. The specific characteristics of the five population risk levels are listed in the notes to table 2.
TABLE 2.
Match between Target Population and Program Theory
| Population Target | Matching Theorya |
|---|---|
| 1. Low risk | 1. Mothers lack parenting knowledge and skills. |
| 2. Some elevated risk | 2. Access to health care for health/developmental milestones. |
| 3. Mothers lack emotional/social support. | |
| 3. High risk | 2. Access to health care for health/developmental milestones. |
| 3. Mothers lack emotional/social support. | |
| 4. Mother-infant interaction/attachment. | |
| 4. Very high risk | 5. Poor mental health/therapeutic/psychological model. |
| 5. Current abuse | 6. Ecological model. |
Notes:aA match requires one of the theories in the matching theory column to be applied, although a higher level theory also is acceptable. More complete descriptors of theory categories are provided in the text and table 3.
Low risk: General population of families with neonates.
Some elevated risk: One of the following: mothers < 19 years old, racial minority group, low income, low socioeconomic status, unemployed, limited education, lack of social support / social isolation, single parent, unmarried, financial stress, underuse of needed community services, low self-esteem.
High risk: Mental illness, unstable housing, chaotic lifestyle, low intelligence / low IQ, difficult child, ambivalence to pregnancy (sought termination / no antenatal care), ≥ two of “some elevated risk.”
Very high risk: Criminal record, in-utero drug exposure, prenatal drug use, drug abuse, parent history of childhood abuse, suspicion of previous abuse by parent, or 3 or more combinations of level 3.
Current abuse: At least one previous incident of child abuse or neglect and/or evidence of domestic violence.
Program Components
Programs have been described in terms of their constituent components using a classification system designed to capture program diversity but limited to ten broad components (see table 3).
TABLE 3.
Match between Program Theory and Program Components
| Program Theorya | Program Components |
|---|---|
| 1. Mothers lack parenting knowledge and skills. | 1. Education, training, information* |
| 6. Problem solving/goal settingb | |
| 2. Limited access to health services pose a threat to health of mother and baby. | 5. Referral and linking to health services/advocacy* |
| 6. Problem solving/goal settingb | |
| 9. Clinical services responsive to mother/child family circumstance* | |
| 3. Social isolation: mothers lack social and emotional resources. | 2. Emotional support* |
| 5. Referral and linking to health services/advocacyb | |
| 6. Problem solving/goal settingb | |
| 4. Disruption to the mother-infant interaction and bonding or of maternal sensitivity. | 3. Modeling/mentoring* |
| 4. Counseling/therapy by mental health worker* | |
| 6. Problem solving/goal settingb | |
| 5. A compromised psychological state/poor mental health undermine the capacity to parent. | 4. Counseling (including drug and alcohol)/therapeutic support by a mental health worker (psychiatrist, psychologist, mental health nurse)* |
| 8. Case management involving mental health worker* | |
| 6. Ecological modelc: ecological factors (social, community, and family level) have a core influence on capacity of mothers to parent. | 5. Referral/link to services/advocacy* |
| 7. Provision of goods and services (food, contraception, transport, access to education, training, job placement) | |
| 9. Clinical services responsive to mother/child circumstanceb | |
| 10. Child careb |
Notes: Match: At least one core component (identified with an asterisk, *) must be present for a match.
When more than one program theory is identified, a match requires a core (identified with an asterisk, *) program component to be present for each theory.
Useful but not sufficient.
For the ecological model, the core component plus ≥ 1b must be present for a match.
Program Objective
We wanted to establish whether the reduction of child abuse and/or neglect was an explicit program objective, which was not a criterion for inclusion in our review, although reporting at least one direct or indirect child abuse outcome was.
Program Performance
We created a protocol to classify programs as “successful or not” that was designed to weigh up all the relevant outcomes that were measured, rather than to selectively report only those that were statistically significant, without reference to those that were not. Our aim was to assess whether, on balance, there was likely to be a positive and important impact for the client population. Surprisingly little attention has been paid to this task. Instead, most reviewers assess performance one outcome measure at a time, collating the evidence across all programs reporting that outcome. The general absence of prespecified protocols for defining program success leaves considerable opportunity for selective outcome reporting and interpretation. In their 2010 review of sixty-six home-visiting programs for infants, children, and adolescents, Kahn and Moore (2010) defined the program's success by the report of at least one positive outcome (intervention group statistically significantly better than control), regardless of the number of reported outcomes or the existence of negative results. This might be considered a minimum hurdle for potential classification as successful.
We adopted an approach to defining success that was based on the primacy of outcome and the number and proportion of statistically significant (p < 0.05) positive (or negative) outcomes, relative to all outcomes reported. The precise protocol adopted is described in the section “Approach to Data Extraction.”
Definition of a “Match” between Program Theory, Components, and Population
For each of these six theories, we selected those program components that were consistent with the theory, based on the postulated mechanisms of action. A match between program theory and program components was tied to the mechanism inherent in the theory. At least one “critical program component” needed to be present to yield a match with the program theory. A match between the target population and the theory was defined according to a hierarchy, starting with the simple knowledge deficit model matched with low-risk populations and advancing to a therapeutic or ecological model matched with higher-risk populations. For this purpose, the target populations were collapsed from five to three. How we defined a match between population and program theory is described in table 2 and that between theory and components in table 3.
Literature Search
We conducted a literature search to identify all published controlled studies of home visiting for neonates/infants at risk of child maltreatment, searching electronic databases using key terms for “home visiting” and “child.” Owing to the large number of published systematic reviews of home-visiting programs, we used a three-step process:
Step 1: Search for systematic reviews using search filters and pertinent databases—Cochrane, Medline, Embase, Meditext, and Social Sciences Citation Index—locating all individual home-visiting trials included in these reviews fitting our inclusion criteria.
Step 2: Search for RCTs using search filters for 2000 onward from Cochrane, Medline, Embase, PsychInfo, Meditext, and Social Sciences Index (assuming earlier studies would have been included in at least one of the several published reviews).
Step 3: Search of bibliographies, key authors, key journals (Child Abuse & Neglect, Child Maltreatment) and the gray literature via the National Child Protection Clearinghouse of Australia. The full details of our search strategy and search filters are available from the authors.
Eligibility Criteria
One of us (Opie) excluded those articles that were obviously irrelevant, based on an inspection of the abstract and title. We then obtained the full articles that appeared to meet our broad selection criteria or whose relevance could not be assessed from the abstract and title. Opie and Dalziel assessed them separately for inclusion, reading a total of 143 full text studies. Initial agreement was obtained on all but five studies, which were discussed with Segal and agreement reached on all studies.
Our inclusion criteria were the following:
A randomized controlled trial or quasi-experimental design with a control or comparison group.
Home visiting (defined as at least two home visits by someone other than a relative).
Visits commencing during pregnancy or within six months of birth for the purpose of reducing the risk of child maltreatment or related outcome.
At least one quantifiable outcome related to maltreatment or the risk of maltreatment, primarily the notification or substantiation of child abuse or neglect, out-of-home placement, cases of intentional injury, hospitalization, ED visits, Child Abuse Potential Inventory (CAPI), Conflict Tactics Scale (CTS), Home Observation for Measurement of the Environment (HOME) inventory, Family Stress Checklist (FSC), Parenting Stress Index, rapid repeat births, substance misuse, Parent-Infant Relationship Global Assessment Scale (PIRGAS), and Mother Infant Interaction Scale.
Published in the English language.
Quality Assessment
Table 1 summarizes the study design and rating of each program's potential for bias. Dalziel formally assessed each included study for bias, using criteria developed from the Cochrane Handbook (Higgins and Green 2009), the Centre for Reviews and Dissemination's guidelines (2009), and Edgeworth and Carr's criteria specific to child abuse research (2000). Each study was classified as of “good quality” (zero or one potential for bias), “adequate quality” (two potentials for bias), or “poor quality” (three or more potentials for bias). Potentials for bias were restricted to quality items most likely to compromise study results: specifically unadjusted group differences at baseline, failure to conduct intention to treat analysis, outcome assessors not blinded to group status, provision of intervention and control services by the same nurses, and nonrandom allocation to groups. The quality of the studies were considered good for fourteen (27%) programs, adequate for twenty-five (48%), and poor for thirteen (25%).
Approach to Data Extraction
We created several tables to classify the programs by the underlying theory (six options), program components (ten options), population target (1 to 5), and objective (child abuse yes or no) according to the preceding definitions. Dalziel and Opie independently double-extracted the data for program theory, program components, and child abuse objectives. When they differed, Segal helped them agree on an allocation. In every case, the data were extracted based on what actually occurred (notably the population who participated in the program and the program components as delivered).
Underpinning Program Theory
The underpinning program theory was directly obtained from the stated theory when it was described, or it was drawn from the reported program goals or intention. In other words, in the absence of an explicitly stated theory, a theory was inferred from other related information. In most cases, one of the six theories was identified as predominant and allocated to the program, but we allowed up to three to be identified.
Population Target
The population target(s) for each program were selected from the five options described in table 2, based on the characteristics of the enrolled population. For example, a program that recruited pregnant teenagers in Baltimore might be allocated to risk level 2, but if the enrolled population included 75 percent with a drug addiction, the program would be allocated to risk level 4. The allocation was made independently by Rachelle Sara Opie and Kim Dalziel, with any differences resolved through discussion with Leonie Segal. Classification to more than one population target was allowed.
Program Components
The program components were determined based on the description of the service delivery components/activities described for the intervention arm and allocated to one or more of the ten categories listed in table 3. The components as delivered, even if they differed from what was intended, were used.
Objective of Child Maltreatment Prevention
A program was classified as “yes” if any program reports stated that an objective was to prevent child maltreatment or “no” if they did not.
Overall Success of the Program/Intervention Arm
We analyzed the program results in two steps: first outcomes were classified as either (1) a direct measure of child abuse, defined to include child protection service reports, reports or substantiated cases of abuse or neglect (including domestic violence), out-of-home placement, nonaccidental injury (captured in hospital admissions or hospital emergency department visits) or Child Abuse Potential Inventory (CAPI) score; or (2) indicator or risk for child maltreatment, primarily the HOME score, rapid repeat births, substance abuse, parent-child conflict tactics scales, mother-infant interaction rating scale, family stress checklist, and/or parenting stress index (PSI).
The second task was to look for consistency in the direction of outcome (positive or negative). Subgroup analyses were not considered, only main program effects. For a program to be classified as having an overall “positive outcome” and thus designated as a “success,” the following protocol was adopted: If only one variable was reported, it had to be statistically significantly positive. If two or more variables were reported, at least one needed to be statistically significantly positive if all other variables showed, at worst, no difference. In all cases, success required the absence of any reported statistically significant negative outcomes. Indicators of or risks for child maltreatment (considered proxy outcomes) were considered only if no direct child maltreatment variables were reported. Success was then defined using the same protocol described above. This approach to defining success was designed to ensure that studies that collected many outcomes were not more likely to be identified as successful simply because of the greater likelihood of a chance positive finding. The approach also placed the greatest weight on more direct child maltreatment outcomes as the best indicator of child abuse or neglect. Although these might be considered low-risk events, in the typically higher-risk populations that receive home visiting, they are not uncommon.
Defining a Match
Once each program was allocated to a program theory (1 to 6), a set of program components (1 to 10) and population (1 to 5), as well as a child abuse objective (yes or no), the existence of a match was assigned according to the protocols defined in tables 2 and 3. The programs were then classified as one of three categories: (1) a “full match” across program theory, components, population, and yes for stated child abuse objective; (2) a “partial match,” involving a match of theory, components, and population but without a child abuse objective or a match of theory, components, and child abuse objective but only for part of the population; or (3) “no match,” a residual category. If a program offered additional components beyond those deemed a necessary minimum for the target population, this was recorded as a full match. This may affect cost-effectiveness but seemed unlikely to undermine a positive outcome.
Relationship between Match and Program Success
We hypothesized that if the program components, population, and child abuse objective matched the underlying theory, the program was more likely to be successful. If there was no match across these variables, we hypothesized that the program was less likely to be successful. We then observed whether there was a difference in rates of program success across the “three defined match categories.” We also formally tested the relationship by modeling program success against the match results.
Data Analysis
We used standard tests of statistical significance (Pearson's chi-square and Fisher’s exact) to test the relationship between program classification as successful; and having a full, partial, or no match between theory and program components and population.
Results
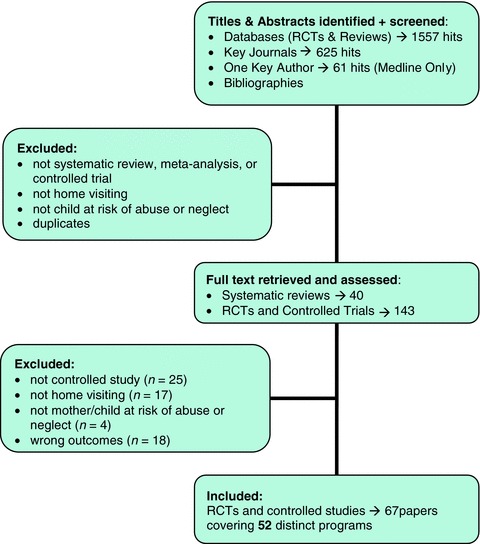
Study Selection
Our literature search yielded 2,243 articles, of which we examined 143 papers in full text (see appendix A), and identified fifty-two “distinct” home-visiting programs meeting the inclusion criteria (associated with forty-five models). Programs implemented in a unique setting and/or with different populations were treated as distinct, even if based on the one overarching model (e.g., three programs applied the Olds's Nurse Family Partnership model but in different settings and for distinct populations). References to included programs are listed in appendix B.
Program Characteristics
Study Design
Of the fifty-two included programs, fourteen were nonrandomized controlled studies; two were cohort studies; and the remaining thirty-six were randomized controlled trials. Thirty-seven programs were delivered in the United States, three in Australia, six in Canada, two in the United Kingdom, and one each in New Zealand, Syria, Japan, and Norway. The studies were published between 1969 and 2009.
Type of Home Visitor
Many programs used nurses for home visiting (n= 19), but the use of other professionals (e.g., social workers n= 15), “paraprofessionals” (n= 9) or laypersons (n= 6) for visiting was also common. A formal multidisciplinary team was used for three programs. Twenty programs used more than one discipline group on their team for the home visit or for training and/or support.
Program Intensity
There was considerable diversity in program intensity. Twenty-five home-visiting programs commenced during pregnancy, and the others began after birth. The child's age at exit from the program varied from one month up to five years. The mean number of visits ranged from two to forty-one, and the length of visit varied from twenty minutes to four hours, resulting in considerable variation in the potential (as well as actual) hours of home visiting for the family.
Population Characteristics
Seven programs exclusively targeted teenage/adolescent parents; four programs targeted high-risk families defined by the Kempe Family Stress checklist; and four programs recruited parents using illicit drugs. Many programs drew their populations from two or three risk categories. Most programs targeted persons at considerably elevated risk, including current abuse, current drug or alcohol problems, or existence of several risk characteristics (n= 23). Often, the enrolled populations exhibited higher-risk attributes than suggested by the enrollment criteria. Only two programs included the entire range of population categories (see table 4).
TABLE 4.
Key Data Extraction: Predominant Theory, Population, Stated Child Abuse Objective, Program Components, Match, Outcomes, and Success
| Matchf | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Program, Location (key reference)a | Target Populationb | Core Theoryc | Aim: Reduce Child Abuse (yes/no)d | Program Componentse | Theory and Components | Theory and Population | Full/Partial/No Match | Primary Outcomeg | Other Outcomesh | Success (yes/no)i | Potential for Biasj | |
| Very High Risk (e.g., illicit drug use)/Current Abuse Populations | ||||||||||||
| 1. | Special Families Care Project, MN (Christensen, Schommer, and Velasquez 1984) | 5 | 5 | Yes | 1, 2, 4, 5, 6 | Yes | Yes | Full | *Abuse*Neglect*Out-of-home placement /foster care | Yes | 1 | |
| 2. | Project 12-Ways, IL (Lutzker and Rice 1984) | 5 | 6 | Yes | 1, 2, 4, 5, 7 | Yes | Yes | Full | *Abuse or neglect incidents*Substantiated instance of abuse or neglect | Yes | 2 | |
| 4. | Home visiting, Perth, Australia (Bartu et al. 2006) | 4 (illicit drug use) | 2 | No | 1, 2, 5 | Yes | No | No | NA | †Drug use increased | No | 1 |
| 5. | Home visiting, Baltimore (Nair et al. 2003; Schuler et al. 2000) | 4 (drug use) | 4 | No | 1, 2, 5, 6 | No | No | No | NA | †Narcotic, alcohol, or marijuana use †Maternal responsiveness or infant warmth | No | 0 |
| 6. | Healthy Families America (HFA), Healthy Families New York (DuMont et al. 2008) | 3–5 | 4, 5, 6 | Yes | 1, 2, 3, 5 | No | Yes | No | Year 2:†Composite score serious abuse or neglect, prevalence, or frequency†Frequency of substantiated CPS reports | No | 0 | |
| 31. | Nurse Visiting, Baltimore (Black et al. 1994) | 4, 5 (prenatal illicit drug use) | 6 | Yes | 1, 2, 3, 4, 5, 6 | Yes | Yes | Full | *CAPI | *Drug free*Overall home score†PSI | Yes | 0 |
| High to very high risk target population | ||||||||||||
| 3. | Home visiting, Denver (Gray et al. 1977) | 3–5 | 4 | Yes | 1, 2, 3, 5, 9 | Yes | Part | Partial | *Hospital attendance for injuries due to abnormal parenting practices | Yes | 2 | |
| 7. | Home visiting, Queensland, Australia (Armstrong et al. 1999) | 3–5 | 4 | Yes | 1, 2, 3, 4, 5 | Yes | Part | Partial | *CAPI (baseline to 7 months)*Self-reported fewer injuries and bruises†Use of health services | *Improvement in overall PD score (PSI)*HOME (all subscales and total HOME score) | Yes | 0 |
| 8. | Child Parent Enrichment Project, Contra Costa County, CA (Barth 1991) | 3–5 (most very high risk) | 6 | Yes | 1, 2, 3, 5 | No | Yes | No | †Unsubstantiated reports†CAPI†Illness/ED visits | No | 1 | |
| 9. | Community Infant Project, Boulder, CO (Huxley and Warner 1993) | 3–5 | 3 | Yes | 1, 2, 4, 5, 8 | Yes | Part | Partial | *Emergency room use*Confirmed child abuse episode†Child abuse or neglect report | *HOME: total HOME score, + some subscores†HOME other subscales | Yes | 2 |
| 10. | Early Intervention Program, San Bernardino, CA (Koniak-Griffin et al. 2002) | 3–5 | 3 | Yes | 1, 2, 4, 5, 6, 8 | Yes | Part | Partial | *Total days hospitalization*Number of episodes of hospitalization†Total number of ED visits*Never used ED | *Next conception†Time to repeat pregnancy*Marijuana use†Alcohol and tobacco†HOME scores | Yes | 1 |
| 11. | Hawaii Healthy Start Program, HI (Duggan et al. 1999) | 3–5 | 1, 3, 4 | Yes | 1, 2, 3, 5, 6 | Yes | Part | Partial | †Frequent and severe self-reported abuse behaviors†Maternal neglect†Substantiated CPS report rates†Hospitalizations†Mother relinquish primary caregiver | †HOME: acceptance of child†PC-CTS†RRB | No | 1 |
| 12. | Healthy Families America (HFA), Healthy Families Alaska (Gessner 2008)k | 3–4 | 3, 5 | Yes | 1, 2, 3, 5, 6 | No | Yes | No | HFA versus high risk matched control†CPS referral†Substantiated neglect and abuse | No | 2 | |
| 32. | (HFA), Healthy Families Alaska (Duggan et al. 2007) RCTk | 3–4 | 3, 5 | Yes | 1, 2, 3, 5, 6 | No | Yes | No | †CPS Reports and Neglect†Hospitalization and ED visits†Birth mother relinquished her role | *Fewer extremely poor total HOME scores†Group scores for HOME subscale†Substance abuse†Total PSI scores | No | 0 |
| 13. | Home visiting, Western Australia (Quinlivan, Box, and Evans 2003) | 3–5 | 1, 2, 3 | Yes | 1, 2, 3, 5 | Yes | Part | Partial | *Neonatal adverse outcome (deaths, injury, non-voluntary foster care placement) | Yes | 0 | |
| 14. | Early Start, New Zealand (Fergusson et al. 2005) | 3–5 | 1, 3 | Yes | 1, 2, 3, 6 | Yes | Part | Partial | *Severe physical assault†Rates of agency contact for child abuse and neglect*Fewer hospital attendances for injury | *Nonpunitive parenting†Next pregnancy†Alcohol/substance use†Life stresses, family functioning | Yes | 1 |
| 15. | Family Partnership Model, two counties in the UK (Barlow et al. 2007) | 3–5 (65% mental health, 34% DV) | 3 | Yes | 1 | No | Part | No | †Hospitalization at 6 months†Child protection register or care proceedings†Children removed from home | †HOME*(MCI–CARE Index) sensitive to babies, who were more cooperative | No | 0 |
| 16a | Nurse Family Partnership (NFP) Nurse home-visiting, Denver (Olds 2002) | 2–5 (low income +/− DV) | 1, 2, 4 | No | 1, 2, 5 | Yes | Yes | Partial | *Any domestic violence | *Timing next births†Marijuana†Alcohol use†HOME score | Yes | 1 |
| 16b. | (NFP) Paraprofessional home visiting, Denver (Olds 2002) | 2–5 | 1, 2, 4 | No | 1, 2, 5 | Yes | Yes | Partial | †Any domestic violence | †Subsequent pregnancies and births†Marijuana/alcohol use†HOME score*More sensitive and responsive interaction | No | 1 |
| 17. | Parenting on Edge, GA (Mulsow and Murray 1996) | 3–4 | 6 | Yes | 1, 2 | No | Yes | No | †Incidence of abuse or neglect reports†N reports per mother | No | 2 | |
| 18. | Linkages for Prevention Project, Durham, NC (Margolis et al. 2001) | 3–4 | 6 | No | 1, 2, 5 | No | Yes | No | †Substantiated neglect†Substantiated cases of abuse†ED or hospitalized | †Drug or alcohol use*3/5 safety measures child home environment*HOME scale | No | 2 |
| 33. | Addition of intensive home visiting to (CAMP), Denver (Stevens-Simon, Nelligan, and Kelly 2001) | 4, 5 | 4 | Yes | 1, 2, 3, 4, 5 | Yes | Part | Partial | †All maltreatment, (physical abuse, neglect, abandonment) | †Repeat pregnancy rate | No | 1 |
| 34. | Home visiting, Philadelphia, (Marcenko and Spence 1994) | 3–5 (high-risk for psychosocial reasons) | 3 | Yes | 1, 2, 3, 4, 5, 6 | Yes | Part | Partial | †Placed in out-of-home care | †Home Inventory | No | 1 |
| Moderate-risk target population | ||||||||||||
| 19. | Child and Youth Program Module, Baltimore (Hardy and Streett 1989) | 2, 3 | 1 | Yes | 1, 2, 5 | Yes | Part | Partial | *Child abuse and neglect*Inpatient care*Clinic or ED visit for fall or head injury | Yes | 1 | |
| 20. | (NFP), Olds Nurse Family partnership, Memphis (Kitzman et al. 1997) | 3 | 6 | No | 1, 5, 6, 7 | Yes | Yes | Partial | First 2 years:*Injuries and ingestions†ED visits†Hospitalizations*Less hospitalization for injury and ingestionBirth to age 9:*Death | First 2 years:*Second pregnancy and subsequent live births*HOME scoresBirth to age 9:*Subsequent births*Substance use | Yes | 1 |
| 26a. | (NFP), Olds Nurse Family Partnership, pre- and postnatal, Elmira, NY (Olds et al. 1997) | 2–3 | 1, 2, 3 | Yes | 1, 2, 5 | Yes | Yes | Yes | 25 to 50 months:†New cases child abuse and neglect*Injuries and ingestions*ED visits†Hospitalizations15 years:*Child abuse and neglect substantiations | 25 to 50 months:†HOME total score15 years:†Next pregnancy and birth†Substance use | Yes | 0 |
| 26b. | (NFP) Olds Nurse Family Partnership, prenatal, Elmira, NY (Olds et al. 1997) | 2–3 | 1, 2, 3 | Yes | 1, 2, 5 | Yes | Yes | Yes | 25 to 50 months:†New child abuse and neglect cases*Injuries and ingestions*ED visits†Hospitalizations15 years:*Child abuse and neglect substantiations | 25 to 50 months:†HOME total score15 years:†Next pregnancy and births†Substance use | Yes | 0 |
| 21. | Three Generation Study, Baltimore (Black et al. 2006) | 3 | 3 | No | 1, 2, 3, 6, 7 | Yes | Yes | Partial | NA | *Extend time to second birth | Yes | 0 |
| 22. | Parent Training by CETA aide, Miami (Field et al. 1982) | 3 | 4 | No | 1, 3 | Yes | Yes | Partial | NA | *Repeat pregnancy | Yes | 1 |
| 23. | Comprehensive Child Development Program, USA (St. Pierre and Layzer 1999) | 2–3 | 6 | No | 1, 2, 4, 5, 6, 7, 8 | Yes | Yes | Partial | NA | †HOME score†PCI | No | 2 |
| 24. | Home visiting, CO (Dawson, van Doorninck, and Robinson 1989) | 2–3 | 3 | No | 1, 2, 5, 7 | Yes | Yes | Partial | †Child abuse and neglect reports†Accidents or hospitalization | †Subsequent childbearing | No | 2 |
| 25a. | Parents as Teachers (PAT) Program—Teens Combined = basic + case management, CA (Wagner and Clayton 1999) | 2–3 | 1, 6 | Yes | 1, 2, 3, 5, 7, 8 | Yes | Yes | Yes | *Opened cases of child abuse or neglect†Child abuse†Child treated for injury | †Total HOME score | Yes | 1 |
| 25b. | Parents as Teachers (PAT) Program – basic program, CA (Wagner and Clayton 1999) | 2–3 | 1 | No | 1, 2, 3, 5 | Yes | Yes | Partial | †Treated for injury†ED visits | †Total HOME score | No | 1 |
| 25c. | Parents as Teachers (PAT) Program, Teen PAT (basic teenage program), CA (Wagner and Clayton 1999) | 2–3 (teenage parents) | 1 | No | 1, 2, 3, 5 | Yes | Yes | Partial | †Opened cases of child abuse or neglect†Child abuse†Child treated for injury | †Total HOME score | No | 1 |
| 27. | Social Support and Family Health Study, London (Wiggins et al. 2004) | 2–3 | 3 | No | 1, 2 | Yes | Yes | Partial | †injuries requiring medical attention | †maternal smoking | No | 1 |
| 28. | Home visiting, Quebec, Canada (Infante-Rivard et al. 1989) | 2–3 | 1 | No | 1, 4 | Yes | Part | No | †Hospitalization | †Total HOME score‡and *HOME score components | No | 1 |
| 29a. | Postnatal home visiting, Montreal (Larson 1980) | 2, 3 | 4 | No | 1, 2, 4 | Yes | Yes | Partial | *Accident rate @ 12 months†Accident rate @ 6 and 18 months†Rate of ED visits over 18 months | †HOME | No | 2 |
| 29b. | Pre and postnatal visiting, Montreal (Larson 1980) | 2, 3 | 4 | No | 1, 2, 4 | Yes | Yes | Partial | *Accident rate @ 6 months*Accident rate @ 12months†Accident rate @ 18months†Rate of ED visits over 18 months | *HOME score | Yes | 2 |
| 35. | REACH-Futures program, Chicago (Norr et al. 2003) | 3 | 2, 6 | No | 1 | No | Yes | No | †Health problem variables†Formal or informal foster care | †Repeat pregnancy†HOME: parenting attitudes*HOME: appropriate play materials†Other HOME subscales | No | 1 |
| 36. | New Mexico and Arizona HFA (Barlow et al. 2006) | 2–3 (American Indian adolescents) | 2 | No | 1 | No | Yes | No | NA | †Lower drug use but no difference | No | 1 |
| 37a. | Early Head Start, home-based only, 17 sites across USA (Love et al. 2005) | 2–3 | 1, 2 | No | 1, 2, 5, 8, 10 | Yes | Yes | Partial | NA | *HOME score*PCI | Yes | 0 |
| 37b. | Early Head Start, mixed (home- + center-based), 17 sites across USA (Love et al. 2005) | 2–3 | 1, 2 | No | 1, 2, 5, 8, 10 | Yes | Yes | Partial | NA | *HOME score†PCI | Yes | 0 |
| General population + low to medium risk | ||||||||||||
| 30. | Home visiting, Greensboro, NC (Siegel et al. 1980) | 1–3 | 4 | Yes | 1, 2, 5, 9 | No | Partial | No | †Reports of abuse and neglect†Hospitalization and ED visits | †MII: three attachment measures | No | 2 |
| 38. | Healthy Steps for Young Children Program (HS),k Pacific Northwest (USA and Canada) (Johnston et al. 2006) | 1 | 5 | No | 1, 2 | No | No | No | †Exposure to significant physical domestic violence | †Use of illicit drugs†Smoking*Injury control behaviors | No | 2 |
| 39. | Home visiting, Damascus, Syria (Bashour et al. 2008) | 1 | 2 | No | 1, 2, 5, 6 | Yes | Yes | Partial | †Seeking medical treatment | No | 0 | |
| 40. | Cognitive extension of the Healthy Start Program, Santa Barbara, CA (Bugental and Schwartz 2009) | 1, 2 (children born at medical risk) | 4 | Yes | 1, 4, 5, 6 | Yes | Part | Partial | *Injury†Physical abuse | *CTS PC: corporal punishment*Home safety | Yes | 1 |
| 41. | Home visiting,Yamanashi, Japan (Cheng et al. 2007) | 1 | 4 | No | 1, 2, 3, 4, 6 | Yes | No | No | NA | PIRGAS*Relationship group†adapted relationship group | No | 1 |
| 42. | Modified Mother-Infant Transaction Program (MITP), Norway (Kaaresen et al. 2006) | 2, 3 (birth weight below 2000g) | 4 | No | 1, 2, 3 | Yes | Yes | Partial | NA | PSI:*Total stress 6, 12 months, mother; 12 months, father*Child domain, 6 months, mother; 12 months, father*Parent domain, 6 months, mother; 12 months father | Yes | 0 |
| 43. | REST, USA (Keefe et al. 2006) | 1, 2 (infants with. irritability or colic) | 3, 2 | No | 1, 2, 3, 4, 5 | Yes | Yes | Partial | NA | *PSI total score @ 8 weeks*P-CDI subscale†Other two subscales: parental distress and difficult child | Yes | 1 |
| 44. | Home visiting, Ontario, Canada (Steel O’Connor et al. 2003) | 1 | 2 | No | 2, 5 | Yes | Yes | Partial | †Health problems†Number of ED visits†Number of hospital admissions | No | 2 | |
Notes:aDefined in text.
Target population defined in table 2.
Core theory defined in table 3.
Aim as stated in the original manuscripts reporting on each program.
Components defined in table 3.
Match defined in text in Methods.
Primary outcome is a direct or surrogate child abuse outcome. The outcome measure symbols are as follows:
: Intervention group statistically significantly better than control group.
†: No statistically significant difference between intervention and control group.
‡: Intervention group statistically significantly worse than control group.
Other outcomes: Risk factors for child abuse and neglect. Outcome symbols same as in note g.
Success defined in text, in Methods.
Potential for bias (see under Methods Quality Assessment list of potentials for bias).
0 = Study with zero or one potentials for bias (classified as good quality).
1 = Study with two potentials for bias (classified as adequate quality).
2 = Study with three + potentials for bias (classified as poor quality).
Both programs 12 and 32 are Healthy Families Alaska but evaluated through different methods, one through data linkage and matched design, and the other an RCT, covering somewhat different populations. Program 38, Healthy Steps, was the only program whose program components other than home visiting could play a larger role than the home visits (of which there were only three).
NA: No direct child maltreatment outcomes reported.
CAPI: Child Abuse Potential Inventory.
HOME: The Home Observation for Measurement of the Environment inventory.
PSI: Parenting Stress Index.
DV: Domestic Violence.
MCI-CARE: Maternal Child Interaction-CARE Index.
RRB: Rapid Repeat Births.
PIRGAS: Parent-Infant Relationship Global Assessment Scale.
MII: Mother-Infant Interaction.
PCI: Parent Child Interaction Score.
CTS-PC: Parent Child Conflict Tactics Scale.
Program Theoretical Underpinning
The predominant theory (or theories) assigned to each program is reported in table 4. The four most commonly defined theories, covering 80 percent of the programs, were “mothers lack knowledge/skills,” “limited access to health care undermining the physical health of the mother and baby,” “mothers are isolated and lack social/emotional resources,” and “disruption to mother-infant interaction and bonding.” Only 10 percent drew on a theory related to “compromised mental health” (n= 5).
Program Components/Activities
The program components identified in the home-visiting programs were, in order of frequency: education/training/information (n= 46), emotional support (n= 43), referral and linking to services/advocacy (n= 38), modeling/role model (n= 19), problem solving (n= 16), counseling/therapy (n= 16), case management (n= 5), provision of goods and services (n= 5), responsive clinical services (n= 2), and provision of child care (n= 2) (see table 4).
Objective of Child Maltreatment Prevention
Twenty-five out of the fifty-two programs had a stated objective of preventing child maltreatment, and all of these reported direct child abuse outcomes. Of those that did not identify a child abuse and neglect objective, 42 percent still reported a “direct” child abuse outcome.
Program Success
A total of twenty-five (48%) of programs were defined as successful and twenty-seven (52%) as not successful, using the criteria described earlier. Outcomes were more likely to be indirect where reducing child abuse and neglect was not a stated aim.
Match between Theory, Population, and Program Components
Only seven of the fifty-two programs (13.5%) were described as having a complete match for theory, population and program components, and a stated aim to reduce child abuse and neglect. Thirty programs (58%) were classified as a partial match, and fifteen programs (29%) as a clear mismatch.
Likelihood of Program Success and Observed Match between Theory, Population, Program Components, and Child Abuse Prevention Objective
For the seven programs for which a complete match was observed, all—that is, 100 percent—were defined as successful. For the fifteen programs for which a clear mismatch was observed, none was defined as successful; that is, the home-visiting group did no better than the control in any of these programs. Those that had a complete match for part of the target population or a match of the theory, target population, and components but not an objective of reducing child abuse or neglect had an intermediate success rate of 60 percent. For the programs that did not have a child abuse objective, success was typically based on intermediate outcomes, which have a less certain relationship with child maltreatment (see table 5).
TABLE 5.
“Match” and Success of Home Visiting for Fifty-Two Included Programs
| Performance of Home Visiting | |||||
|---|---|---|---|---|---|
| Successfula | Not Successfula | ||||
| Match | Number (%) | Programs | Number (%) | Programs | Totals Number (%) |
| Full match: theory, components, population, child abuse objective | 7 (100) | 1, 2, 25a, 26a, 26b, 31, 45a | 0 (0) | 7 (13.5) | |
| Partial match: theory, components, part population, plus child abuse objective theory, components, population, not child abuse objective | 18 (60) | 12 (40) | 30 (57.7) | ||
| 3, 7, 9, 10, 13, 14, 16a, 19, 40 | 11, 16b, 33, 34 | ||||
| 20, 21, 22, 29b, 37a, 37b, 42, 43, 45b | 23, 24, 25b, 25c, 27, 29a, 39, 44 | ||||
| No match: not a full or partial match | 0 (0) | 15 (100) | 4, 5, 6, 8, 12, 15, 17, 18, 28, 30, 32, 35, 36, 38, 41 | 15 (28.8) | |
| Totals | 25 (48) | 27 (52) | 52 (100) | ||
Notes: Derived from table 4.
See definition in text.
Statistical Analysis
We used Fisher's exact test, owing to our small sample size and the small number of observations (<5) occurring in some cells. The data analysis was consistent with the preceding descriptive analysis, with statistically significant (at p < 0.05) associations found between program success and full, partial, and no match (see table 6).
TABLE 6.
Relationship between Program Success and Full, Partial, or No Match for Theory, Components, Population, and Child Abuse Objective
| Successful (n= 25) | Not Successful (n= 27) | Fisher's Exact p Value (two sided) | |
|---|---|---|---|
| Full match (n= 7) | |||
| Yes | 7 | 0 | |
| No | 18 | 27 | 0.004a |
| Partial match (n= 30) | |||
| Yes | 18 | 12 | |
| No | 7 | 15 | 0.055 |
| No match (n= 15) | |||
| Yes | 0 | 15 | |
| No | 25 | 12 | <0.0001a |
Note:aStatistically significant (p < 0.05).
Discussion
Key Findings
We found that a match between the underpinning theory and program components together with a match between the theory and target population did predict program success. This result is consistent with our hypothesis, that the combination of program theory, program components, and target population is critical. In line with other reviewers, we failed to find any single program component, such as type of professional, timing of intervention, or target population that predicted the success of home visiting (see table 4).
Limitations
Our model did not capture all aspects of program delivery that may be important to program success, such as fidelity in program delivery, program intensity and resourcing, quality of management and staff training, and staff values and approach to their work. However, finding a clear relationship between theory, program components, population, and objective despite this gap might be seen as enhancing the strength of this finding.
Our classification of programs according to a defined theory and, to some extent, program components, lacks precision because of unclear reporting. But two reviewers independently assessed all programs in this regard, with a third reviewer brought in when differences emerged. Defining the target populations tends to be a simpler task, although we often found a difference between the initial description of the target population and the characteristics of persons enrolled in the program.
A dichotomous classification of the performance of individual programs into success or failure necessarily represents a simplification of something that is quite complex. However, we suggest that it is desirable to report on whether or not an individual program worked—or at least to make clear if this cannot be established with certainty. This classification is not a simple matter of looking at statistical significance but of balancing often divergent results across possibly dozens of outcomes, measured at different time points in various subpopulations. Greater attention to this issue in original study reports and by reviewers is warranted.
There is also debate about the outcome measures themselves. For instance, it is argued that home visiting may increase child abuse reports, owing to surveillance bias, whereas self-report also suffers from incompleteness and possible bias. The definition and reporting of child maltreatment are also known to differ across jurisdictions and across countries.
Further exploration of the value of the proposed hierarchy in outcome measures would be useful, to explore more fully how to give the greatest weight to the more robust, objective, and meaningful measures, such as childhood injury or failure to thrive resulting in a hospital visit or admission. We have made a start by describing a clear process for classifying programs as successful, which uses a two-step hierarchy that incorporates in a stepwise fashion both direct and indirect child abuse and neglect outcomes.
As we noted, our measure of success says nothing about value for money, which we have explored elsewhere through a comparative cost-effectiveness analysis in those programs reporting a direct child abuse outcome (Dalziel and Segal forthcoming).
Policy Implications for Home Visiting
This review has a number of key messages for policymakers seeking to implement programs to reduce rates of child maltreatment in vulnerable families. Because it is known that neonate/infant home-visiting programs are not always successful, care must be taken in their design and implementation. Our study suggests that a way to maximize success is through fidelity to a program logic model. Specifically, in designing a home-visiting program, it is important to be clear about the objective (in our review, to reduce child maltreatment) to ensure a sound understanding of the client population and its needs and strengths (the nature of the threats to a safe and nurturing environment), the associated theory or mechanism of change, and the program components that can deliver the change mechanism. Adequate resources and an appropriately skilled team with access to requisite training and quality assurance processes are also crucial. We note that if there is little understanding about how to work with a particular population to achieve a safe and nurturing environment, then it is unlikely that a successful home-visiting program can be developed and delivered.
Even though manualized programs can support fidelity in program delivery, adopting “off-the-shelf program models” is no guarantee of success, particularly if they are not designed for the target population and their specific circumstances.
Conclusion
Our research supports the value of a program logic approach, incorporating a theory (or mechanism) of action, for the review of complex human services interventions to yield new insights. We postulate that the approach will have wide applicability to a range of contexts, particularly for assessing the performance of multifaceted interventions that can target different populations.
A program logic–based systematic review can enhance policy relevance and will be most valuable to policymakers seeking to design and implement effective and efficient programs for improving societal well-being, to ensure that scarce resources are not wasted, and to offer the best prospect of improving outcomes for vulnerable families.
Acknowledgments
Acknowledgments: This study was funded by the Australian Research Council (ARC) as a linkage grant, ID LP0883743, from 2008 to 2012. The funding source played no role in the study's design, conduct, interpretation, writing, or the decision to submit it for publication. The authors declare that they have no conflicts of interest.
We would also like to acknowledge the very generous and detailed comments from Karen Monsen and two anonymous reviewers that have contributed to the clarity of our argument.
APPENDIX A
Search Results and Inclusion/Exclusion
APPENDIX B
Home-Visiting Programs: Key References
| Program Number, Name, and Location | Reference | |
|---|---|---|
| 1. | Special Families Care Project, Minnesota | Velasquez, J., M. Christensen, and B.L. Schommer. 1984. Part II: Intensive Services Help Prevent Child Abuse. American Journal of Maternal Child Nursing 9 (2):13–117. |
| Christensen, M.L., B.L. Schommer, and J. Velasquez. 1984. Part I: An Interdisciplinary Approach to Preventing Child Abuse. American Journal of Maternal Child Nursing 9 (2):108–12. | ||
| 2. | Project 12-Ways, Illinois | Lutzker, J.R., and J.M. Rice. 1984. Project 12-Ways: Measuring Outcome of a Large In-Home Service for Treatment and Prevention of Child Abuse and Neglect. Child Abuse & Neglect 8 (4):519–24. |
| 3. | Healthy Families, New York | DuMont, K., S. Mitchell-Herzfeld, R. Greene, E. Lee, A. Lowenfels, M. Rodriguez, and V. Dorabawila. 2008. Healthy Families New York (HFNY) Randomized Trial: Effects on Early Child Abuse and Neglect. Child Abuse & Neglect 32 (3):295–315. |
| 4. | Home visiting, Perth, Western Australia | Bartu, A., J. Sharp, J. Ludlow, and D.A. Doherty. 2006. Postnatal Home Visiting for Illicit Drug-Using Mothers and Their Infants: A Randomised Controlled Trial. Australian and New Zealand Journal of Obstetrics and Gynaecology 46 (5):419–26. |
| 5. | Home visiting, Baltimore | Schuler, M.E., P. Nair, M.M. Black, and L. Kettinger. 2000. Mother-Infant Interaction: Effects of a Home Intervention and Ongoing Maternal Drug Use. Journal of Clinical Child Psychology 29 (3):424–31. |
| Nair, P., M.E. Schuler, M.M. Black, L. Kettinger, and D. Harrington. 2003. Cumulative Environmental Risk in Substance Abusing Women: Early Intervention, Parenting Stress, Child Abuse Potential and Child Development. Child Abuse & Neglect 27 (9):997–1017. | ||
| 6. | Home visiting, Denver | Gray, J.D., C.A. Cutler, J.G. Dean, and C. Henry Kempe. 1977. Prediction and Prevention of Child Abuse and Neglect. Child Abuse & Neglect 1 (1):45–58. |
| 7. | Home visiting, Queensland, Australia | Armstrong, K.L., J.A. Fraser, M.R. Dadds, and J. Morris. 1999. A Randomized, Controlled Trial of Nurse Home Visiting to Vulnerable Families with Newborns. Journal of Paediatrics & Child Health 35 (3):237–44. |
| Armstrong, K.L., J.A. Fraser, M.R. Dadds, and J. Morris. 2000. Promoting Secure Attachment, Maternal Mood and Child Health in a Vulnerable Population: A Randomized Controlled Trial. Journal of Paediatrics and Child Health 36 (6):555–62. | ||
| Fraser, J.A., K.L. Armstrong, J.P. Morris, and M.R. Dadds. 2000. Home Visiting Intervention for Vulnerable Families with Newborns: Follow-Up Results of a Randomized Controlled Trial. Child Abuse & Neglect 24 (11):1399–1429. | ||
| 8. | Child Parent Enrichment Project, Contra Costa County, California | Barth, R.P. 1991. An Experimental Evaluation of In-Home Child Abuse Prevention Services. Child Abuse & Neglect 15 (4):363–75. |
| 9. | Community Infant Project, Boulder, Colorado | Huxley, P., and R. Warner. 1993. Primary Prevention of Parenting Dysfunction in High-Risk Cases. American Journal of Orthopsychiatry 63 (4):582–88. |
| 10. | Early Intervention Program, San Bernardino, California | Koniak-Griffin, D., I.L. Verzemnieks, N.L.R. Anderson, M.L. Brecht, J. Lesser, S. Kim, and C. Turner-Pluta. 2003. Nurse Visitation for Adolescent Mothers—Two-Year Infant Health and Maternal Outcomes. Nursing Research 52 (2):127–36. |
| Koniak-Griffin, D., N.L.R. Anderson, M.L. Brecht, I. Verzemnieks, J. Lesser, and S. Kim. 2002. Public Health Nursing Care for Adolescent Mothers: Impact on Infant Health and Selected Maternal Outcomes at 1 Year Postbirth. Journal of Adolescent Health 30 (1):44–54. | ||
| 11. | Hawaii Healthy Start Program, Hawaii | Duggan, A., E. McFarlane, L. Fuddy, L. Burrell, S.M. Higman, A. Windham, and C. Sia. 2004. Randomized Trial of a Statewide Home Visiting Program: Impact in Preventing Child Abuse and Neglect. Child Abuse & Neglect 28 (6):597–622. |
| Duggan, A.K., E.C. McFarlane, A.M. Windham, C.A. Rohde, D.S. Salkever, L. Fuddy, L.A. Rosenberg, S.B. Buchbinder, and C.C. Sia. 1999. Evaluation of Hawaii's Healthy Start Program. Future of Children 9 (1):66–90, discussion 177–78. | ||
| El-Kamary, S.S., S.M. Higman, L. Fuddy, E. McFarlane, C. Sia, and A.K. Duggan. 2004. Hawaii's Healthy Start Home Visiting Program: Determinants and Impact of Rapid Repeat Birth. Pediatrics 114 (3):e317–26. | ||
| 12. | Healthy Families Alaska | Gessner, B.D. 2008. The Effect of Alaska's Home Visitation Program for High-Risk Families on Trends in Abuse and Neglect. Child Abuse & Neglect 32 (3):317–33. |
| 13. | Home visiting, Western Australia | Quinlivan, J.A., H. Box, and S.F. Evans. 2003. Postnatal Home Visits in Teenage Mothers: A Randomised Controlled Trial. The Lancet 361 (9361):893–900. |
| 14. | Early Start, New Zealand | Fergusson, D.M., H. Grant, L.J. Horwood, and E.M. Ridder. 2005. Randomized Trial of the Early Start Program of Home Visitation. Pediatrics 116 (6):e803–9. |
| 15. | Family Partnership Model, two counties in the UK | Barlow, J., H. Davis, E. McIntosh, P. Jarrett, C. Mockford, and S. Stewart-Brown. 2007. Role of Home Visiting in Improving Parenting and Health in Families at Risk of Abuse and Neglect: Results of a Multicentre Randomised Controlled Trial and Economic Evaluation. Archives of Disease in Childhood 92 (3):229–33. |
| 16a. | Nurse family partnership home visiting, Denver | Olds, D.L., J. Robinson, L. Pettitt, D.W. Luckey, J. Holmberg, R.K. Ng, K. Isacks, K. Sheff, and C.R. Henderson Jr. 2004. Effects of Home Visits by Paraprofessionals and by Nurses: Age 4 Follow-Up Results of a Randomized Trial. Pediatrics 114 (6):1560–68. |
| 16b. | Paraprofessional home visiting, Denver | Olds, D.L., J. Robinson, R. O’Brien, D.W. Luckey, L.M. Pettitt, C.R. Henderson Jr., R.K. Ng, K.L. Sheff, J. Korfmacher, S. Hiatt, and A. Talmi. 2002. Home Visiting by Paraprofessionals and by Nurses: A Randomized, Controlled Trial. Pediatrics 110 (3):486–96. |
| 17. | Parenting on Edge, Georgia | Mulsow, M.H., and V.M. Murray. 1996. Parenting on Edge: Economically Stressed, Single, African American Adolescent Mothers. Journal of Family Issues 17 (5):704–21. |
| 18. | Linkages for Prevention Project, Durham, North Carolina | Margolis, P.A., R. Stevens, W.C. Bordley, J. Stuart, C. Harlan, L. Keyes-Elstein, and S. Wisseh. 2001. From Concept to Application: The Impact of a Community-Wide Intervention to Improve the Delivery of Preventive Services to Children. Pediatrics 108 (3):e42. |
| 19. | Child and Youth Program Module, Baltimore | Hardy, J.B., and R. Streett. 1989. Family Support and Parenting Education in the Home: An Effective Extension of Clinic-Based Preventive Health Care Services for Poor Children. Journal of Pediatrics 115 (6):927–31. |
| 20. | Home visiting, Memphis | Kitzman, H., D.L. Olds, C.R. Henderson Jr., C. Hanks, R. Cole, R. Tatelbaum, K.M. McConnochie, K. Sidora, D.W. Luckey, D. Shaver, K. Engelhardt, D. James, and K. Barnard. 1997. Effect of Prenatal and Infancy Home Visitation by Nurses on Pregnancy Outcomes, Childhood Injuries, and Repeated Childbearing. A Randomized Controlled Trial. JAMA 278 (8):644–52. |
| Kitzman, H., D.L. Olds, K. Sidora, C.R. Henderson Jr., C. Hanks, R. Cole, D.W. Luckey, J. Bondy, K. Cole, and J. Glazner. 2000. Enduring Effects of Nurse Home Visitation on Maternal Life Course—A 3-Year Follow-Up of a Randomized Trial. JAMA 283 (15):1983–89. | ||
| Olds, D.L., H. Kitzman, R. Cole, J. Robinson, K. Sidora, D.W. Luckey, C.R. Henderson Jr., C. Hanks, J. Bondy, and J. Holmberg. 2004. Effects of Nurse Home-Visiting on Maternal Life Course and Child Development: Age 6 Follow-Up Results of a Randomized Trial. Pediatrics 114 (6):1550–59. | ||
| Olds, D.L., H. Kitzman, C. Hanks, R. Cole, E. Anson, K. Sidora-Arcoleo, D.W. Luckey, C.R. Henderson Jr., J. Holmberg, R.A. Tutt, A.J. Stevenson, and J. Bondy. 2007. Effects of Nurse Home Visiting on Maternal and Child Functioning: Age-9 Follow-Up of a Randomized Trial. Pediatrics 120 (4):e832–45. | ||
| 21. | Three Generation Study, Baltimore | Black, M.M., M.E. Bentley, M.A. Papas, S. Oberlander, L.O. Teti, S. McNary, K. Le, and M. O’Connell. 2006. Delaying Second Births among Adolescent Mothers: A Randomized, Controlled Trial of a Home-Based Mentoring Program. Pediatrics 118 (4):e1087–99. |
| 22. | Parent Training by CETA aide, Miami | Field, T., S. Widmayer, R. Greenberg, and S. Stoller. 1982. Effects of Parent Training on Teenage Mothers and Their Infants. Pediatrics 69 (6):703–7. |
| 23. | Comprehensive Child Development Program, USA | St. Pierre, R.G., and J.I. Layzer. 1999. Using Home Visits for Multiple Purposes: The Comprehensive Child Development Program. Future of Children 9 (1):134–51. |
| 24. | Home visiting, Colorado | Dawson, P., W.J. van Doorninck, and J.L. Robinson. 1989. Effects of Home-Based, Informal Social Support on Child Health. Journal of Developmental & Behavioral Pediatrics 10 (2):63–67. |
| 25a. | The Parents as Teachers (PAT) (a) Teens Combined (including case management), Southern California | Wagner, M.M., and S. Clayton, L. 1999. The Parents as Teachers Program: Results from Two Demonstrations. Future of Children 9 (1):91–115. |
| 25b. | (b) Basic program, Salinas Valley, Northern California | |
| 25c. | (c) Teen PAT, Southern California | |
| 26a. | (a) Nurse Family Partnership, pre- and postnatal, Elmira, New York | Eckenrode, J., B. Ganzel, C.R. Henderson Jr., E. Smith, D.L. Olds, J. Powers, R. Cole, H. Kitzman, and K. Sidora. 2000. Preventing Child Abuse and Neglect with a Program of Nurse Home Visitation: The Limiting Effects of Domestic Violence. JAMA 284 (11):1385–91. |
| 26b. | Nurse Family Partnership, (b) prenatal only, Elmira, New York | Eckenrode, J., D. Zielinski, E. Smith, L.A. Marcynyszyn, C.R. Henderson Jr., H. Kitzman, R. Cole, J. Powers, and D.L. Olds. 2001. Child Maltreatment and the Early Onset of Problem Behaviors: Can a Program of Nurse Home Visitation Break the Link? Development & Psychopathology 13 (4):873–90. |
| Izzo, C.V., J.J. Eckenrode, E.G. Smith, C.R. Henderson Jr., R. Cole, H. Kitzman, and D.L. Olds. 2005. Reducing the Impact of Uncontrollable Stressful Life Events through a Program of Nurse Home Visitation for New Parents. Prevention Science 6 (4):269–74. | ||
| Olds, D.L., C.R. Henderson Jr., R. Tatelbaum, and R. Chamberlin. 1986. Improving the Delivery of Prenatal Care and Outcomes of Pregnancy: A Randomized Trial of Nurse Home Visitation. [erratum appears in Pediatrics, July 1986, 78 (1):138]. Pediatrics 77 (1):16–28. | ||
| Olds, D., C.R. Henderson Jr., H. Kitzman, and R. Cole. 1995. Effects of Prenatal and Infancy Nurse Home Visitation on Surveillance of Child Maltreatment. Pediatrics 95 (3):365–72. | ||
| Olds, D.L., J. Eckenrode, C.R. Henderson Jr., H. Kitzman, J. Powers, R. Cole, K. Sidora, P. Morris, L.M. Pettitt, and D. Luckey. 1997. Long-Term Effects of Home Visitation on Maternal Life Course and Child Abuse and Neglect. Fifteen-Year Follow-Up of a Randomized Trial. JAMA 278 (8):637–43. | ||
| Olds, D.L., C.R. Henderson Jr., and H. Kitzman. 1994. Does Prenatal and Infancy Nurse Home Visitation Have Enduring Effects on Qualities of Parental Caregiving and Child Health at 25 to 50 Months of Life? Pediatrics 93 (1):89–98. | ||
| 27. | Social Support and Family Health Study, London | Wiggins, M., A. Oakley, I. Roberts, H. Turner, L. Rajan, H. Austerberry, R. Mujica, M. Mugford, and M. Barker. 2005. Postnatal Support for Mothers Living in Disadvantaged Inner City Areas: A Randomised Controlled Trial. Journal of Epidemiology and Community Health 59 (4):288–95. |
| Wiggins, M., A. Oakley, I. Roberts, H. Turner, L. Rajan, H. Austerberry, R. Mujica, and M. Mugford. 2004. The Social Support and Family Health Study: A Randomised Controlled Trial and Economic Evaluation of Two Alternative Forms of Postnatal Support for Mothers Living in Disadvantaged Inner-City Areas. Health Technology Assessment 8 (32):iii–107. | ||
| 28. | Home visiting, Quebec, Canada | Infante-Rivard, C., G. Filion, M. Baumgarten, M. Bourassa, J. Labelle, and M. Messier. 1989. A Public Health Home Intervention among Families of Low Socioeconomic Status. Children's Health Care 18 (2):102–7. |
| 29a. | Postnatal home visiting, Montreal | Larson, C.P. 1980. Efficacy of Prenatal and Postpartum Home Visits on Child Health and Development. Pediatrics 66 (2):191–97. |
| 29b. | Pre- and postnatal visiting, Montreal | |
| 30. | Home visiting, Greensboro, North Carolina | Siegel, E., K.E. Bauman, E.S. Schaefer, M.M. Saunders, and D.D. Ingram. 1980. Hospital and Home Support during Infancy: Impact on Maternal Attachment, Child Abuse and Neglect, and Health Care Utilization. Pediatrics 66 (2):183–90. |
| 31. | Home visiting, Baltimore | Black, M.M., P. Nair, C. Kight, R. Wachtel, P. Roby, and M. Schuler. 1994. Parenting and Early Development among Children of Drug-Abusing Women: Effects of Home Intervention. Pediatrics 94 (4):440–48. |
| 32. | Healthy Families Alaska (HFAK) | Duggan, A., D. Caldera, K. Rodriguez, L. Burrell, C. Rohde, and S.S. Crowne. 2007. Impact of a Statewide Home Visiting Program to Prevent Child Abuse. Child Abuse & Neglect 31 (8):801–27. |
| Caldera, D., L. Burrell, K. Rodriguez, S.S. Crowne, C. Rohde, and A. Duggan. 2007. Impact of a Statewide Home Visiting Program on Parenting and on Child Health and Development. Child Abuse & Neglect 31 (8):829–52. | ||
| 33. | Addition of intensive home visitation component to (CAMP), Colorado | Stevens-Simon, C., D. Nelligan, and L. Kelly. 2001. Adolescents at Risk for Mistreating Their Children: Part II: A Home- and Clinic-Based Prevention Program. Child Abuse & Neglect 25 (6):753–69. |
| 34. | Home visiting, Philadelphia | Marcenko, M.O., and M. Spence. 1994. Home Visitation Services for At-Risk Pregnant and Postpartum Women: A Randomized Trial. American Journal of Orthopsychiatry 64 (3):468–78. |
| 35. | REACH-Futures program, Chicago | Norr, K.F., K.S. Crittenden, E.L. Lehrer, O. Reyes, C.B. Boyd, K.W. Nacion, and K. Watanabe. 2003. Maternal and Infant Outcomes at One Year for a Nurse-Health Advocate Home Visiting Program Serving African Americans and Mexican Americans. Public Health Nursing 20 (3):190–203. |
| 36. | New Mexico and Arizona Healthy Families America | Barlow, A., E. Varipatis-Baker, K. Speakman, G. Ginsburg, I. Friberg, N. Goklish, B. Cowboy, P. Fields, R. Hastings, W. Pan, R. Reid, M. Santosham, and J. Walkup. 2006. Home-Visiting Intervention to Improve Child Care among American Indian Adolescent Mothers—A Randomized Trial. Archives of Pediatrics & Adolescent Medicine 160 (11):1101–7. |
| 37a. | Early Head Start, home-based only, 17 sites across USA | Love, J.M., E.E. Kisker, C. Ross, H. Raikes, J. Constantine, K. Boller, J. Brooks-Gunn, R. Chazan-Cohen, L.B. Tarullo, C. Brady-Smith, A.S. Fuligni, P.Z. Schochet, D. Paulsell, and C. Vogel. 2005. The Effectiveness of Early Head Start for 3-Year-Old Children and Their Parents: Lessons for Policy and Programs. Developmental Psychology 41 (6):885–901. |
| 37b. | Early Head Start, mixed (home- and center-based), 17 sites across USA | |
| 38. | Healthy Steps for Young Children Program (HS), Pacific Northwest, USA, and Canada | Johnston, B.D., C.E. Huebner, M.L. Anderson, L.T. Tyll, and R.S. Thompson. 2006. Healthy Steps in an Integrated Delivery System—Child and Parent Outcomes at 30 Months. Archives of Pediatrics & Adolescent Medicine 160 (8):793–800. |
| 39. | Home visiting, Damascus, Syria | Bashour, H.N., M.H. Kharouf, A.A. Abdulsalam, K. El Asmar, M.A. Tabbaa, and S.A. Cheikha. 2008. Effect of Postnatal Home Visits on Maternal/Infant Outcomes in Syria: A Randomized Controlled Trial. Public Health Nursing 25 (2):115–25. |
| 40. | Cognitive extension of the Healthy Start Program, Santa Barbara, California | Bugental, D.B., and A. Schwartz. 2009. A Cognitive Approach to Child Mistreatment Prevention among Medically At-Risk Infants. Developmental Psychology 45 (1):284–88. |
| 41. | Home visiting, Yamanashi, Japan | Cheng, S., N. Kondo, Y. Aoki, Y. Kitamura, Y. Takeda, and Z. Yamagata. 2007. The Effectiveness of Early Intervention and the Factors Related to Child Behavioral Problems at Age 2: A Randomized Controlled Trial. Early Human Development 83 (10):683–91. |
| 42. | Modified Mother-Infant Transaction Program (MITP), Norway | Kaaresen, P.I., J.A. Ronning, S.E. Ulvund, and L.B. Dahl. 2006. A Randomized, Controlled Trial of the Effectiveness of an Early-Intervention Program in Reducing Parenting Stress after Preterm Birth. Pediatrics 118 (1):e9–19. |
| 43. | REST, Utah | Keefe, M.R., K.A. Kajrlsen, M.L. Lobo, A.M. Kotzer, and W.N. Dudley. 2006. Reducing Parenting Stress in Families with Irritable Infants. Nursing Research 55 (3):198–205. |
| 44. | Home visiting, Ontario, Canada | Steel O’Connor, K.O., D.L. Mowat, H.M. Scott, P.A. Carr, J.L. Dorland, and K.F.W. Young Tai. 2003. A Randomized Trial of Two Public Health Nurse Follow-Up Programs after Early Obstetrical Discharge: An Examination of Breastfeeding Rates, Maternal Confidence and Utilization and Costs of Health Services. Canadian Journal of Public Health 94 (2):98–103. |
| 45a. | Parent-Infant intervention model, Ontario, Canada | Barrera, M.E., P.L. Rosenbaum, and C.E. Cunningham. 1986. Early Home Intervention with Low-Birth-Weight Infants and Their Parents. Child Development 57 (1):20–33. |
| 45b. | Developmental intervention (control), Ontario, Canada | |
Note: Program numbers 16a and 16b; 25a, 25b, and 25c; 26a and 26b; 29a and 29b; 37a and 37b; and 45a and 45b share the same reference(s).
References
- ABS (Australian Bureau of Statistics) National Survey of Mental Health and Wellbeing: Summary of Results, 2007. 2008. Available at http://www.abs.gov.au/ausstats/abs@.nsf/mf/4326.0 (accessed July 20, 2011)
- Amos J, Furber G, Segal L. Understanding Maltreating Mothers: A Synthesis of Relational Trauma, Attachment Disorganization, Structural Dissociation of the Personality and Experiential Avoidance. Journal of Trauma and Disassociation. 2011;12(5):1–16. doi: 10.1080/15299732.2011.593259. [DOI] [PubMed] [Google Scholar]
- Armstrong KL, Fraser JA, Dadds MR, Morris J. A Randomised, Controlled Trial of Nurse Home Visiting to Vulnerable Families with Newborns. Journal of Paediatrics & Child Health. 1999;35(3):237–44. doi: 10.1046/j.1440-1754.1999.00348.x. [DOI] [PubMed] [Google Scholar]
- Barlow J, Davis H, McIntosh E, Jarrett P, Mockford C, Stewart-Brown S. Role of Home Visiting in Improving Parenting and Health in Families at Risk of Abuse and Neglect: Results of a Multicentre Randomised Controlled Trial and Economic Evaluation. Archives of Disease in Childhood. 2007;92(3):229–33. doi: 10.1136/adc.2006.095117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barlow A, Varipatis-Baker E, Speakman K, Ginsburg G, Friberg I, Goklish N, Cowboy B, Fields P, Hastings R, Pan W, Reid R, Santosham M, Walkup J. Home-Visiting Intervention to Improve Child Care among American Indian Adolescent Mothers—A Randomized Trial. Archives of Pediatrics & Adolescent Medicine. 2006;160(11):1101–7. doi: 10.1001/archpedi.160.11.1101. [DOI] [PubMed] [Google Scholar]
- Barnard KE, Booth CL, Mitchell SK, Telzrow RW. Newborn Nursing Models: A Test of Early Intervention to High-Risk Infants and Families. In: Hibbs ED, editor. Children and Families: Studies in Prevention and Intervention. Madison, CT: International University Press; 1988. pp. 61–81. [Google Scholar]
- Barrera ME, Rosenbaum PL, Cunningham CE. Early Home Intervention with Low-Birth-Weight Infants and Their Parents. Child Development. 1986;57(1):20–33. doi: 10.1111/j.1467-8624.1986.tb00003.x. [DOI] [PubMed] [Google Scholar]
- Barth RP. An Experimental Evaluation of In-Home Child Abuse Prevention Services. Child Abuse & Neglect. 1991;15(4):363–75. doi: 10.1016/0145-2134(91)90021-5. [DOI] [PubMed] [Google Scholar]
- Bartu A, Sharp J, Ludlow J, Doherty DA. Postnatal Home Visiting for Illicit Drug-Using Mothers and Their Infants: A Randomised Controlled Trial. Australian and New Zealand Journal of Obstetrics and Gynaecology. 2006;46(5):419–26. doi: 10.1111/j.1479-828X.2006.00628.x. [DOI] [PubMed] [Google Scholar]
- Bashour HN, Kharouf MH, Abdulsalam AA, El Asmar K, Tabbaa MA, Cheikha SA. Effect of Postnatal Home Visits on Maternal/Infant Outcomes in Syria: A Randomized Controlled Trial. Public Health Nursing. 2008;25(2):115–25. doi: 10.1111/j.1525-1446.2008.00688.x. [DOI] [PubMed] [Google Scholar]
- Bilukha O, Hahn RA, Crosby A, Fullilove MT, Liberman A, Moscicki E, Snyder S, Tuma F, Corso P, Schofield A, Briss PA, Task Force on Community Preventive Services The Effectiveness of Early Childhood Home Visitation in Preventing Violence—A Systematic Review. American Journal of Preventive Medicine. 2005;28(2):11–39. doi: 10.1016/j.amepre.2004.10.004. [DOI] [PubMed] [Google Scholar]
- Black MM, Bentley ME, Papas MA, Oberlander S, Teti LO, McNary S, Le K, O’Connell M. Delaying Second Births among Adolescent Mothers: A Randomized, Controlled Trial of a Home-Based Mentoring Program. Pediatrics. 2006;118(4):e1087–99. doi: 10.1542/peds.2005-2318. [DOI] [PubMed] [Google Scholar]
- Black MM, Nair P, Kight C, Wachtel R, Roby P, Schuler M. Parenting and Early Development among Children of Drug-Abusing Women: Effects of Home Intervention. Pediatrics. 1994;94(4):440–48. [PubMed] [Google Scholar]
- Bowlby J. Attachment. 2nd ed. New York: Basic Books; 1982. [Google Scholar]
- Bugental DB, Schwartz A. A Cognitive Approach to Child Mistreatment Prevention among Medically At-Risk Infants. Developmental Psychology. 2009;45(1):284–88. doi: 10.1037/a0014031. [DOI] [PubMed] [Google Scholar]
- Centre for Reviews and Dissemination. Systematic Reviews: CRD's Guidance for Undertaking Reviews in Health. York: University of York Press; 2009. [Google Scholar]
- Cheng S, Kondo N, Aoki Y, Kitamura Y, Takeda Y, Yamagata Z. The Effectiveness of Early Intervention and the Factors Related to Child Behavioral Problems at Age 2: A Randomized Controlled Trial. Early Human Development. 2007;83(10):683–91. doi: 10.1016/j.earlhumdev.2007.01.008. [DOI] [PubMed] [Google Scholar]
- Christensen ML, Schommer BL, Velasquez J. Part I: An Interdisciplinary Approach to Preventing Child Abuse. American Journal of Maternal Child Nursing. 1984;9(2):108–12. [PubMed] [Google Scholar]
- Coryn CLS, Noakes LA, Westine CD, Schroter DC. A Systematic Review of Theory-Driven Evaluation Practice from 1990 to 2009. American Journal of Evaluation. 2011;32(2):199–226. [Google Scholar]
- Dalziel K, Segal L. Home Visiting Programs for the Prevention of Child Maltreatment: Cost-Effectiveness of 35 Programs. Archives of Disease in Childhood. doi: 10.1136/archdischild-2011-300795. Forthcoming. [DOI] [PubMed] [Google Scholar]
- Dawson P, van Doorninck WJ, Robinson JL. Effects of Home-Based, Informal Social Support on Child Health. Journal of Developmental & Behavioral Pediatrics. 1989;10(2):63–67. [PubMed] [Google Scholar]
- Doggett C, Burrett S, Osborn DA. Home Visits during Pregnancy and after Birth for Women with an Alcohol or Drug Problem. Cochrane Database of Systematic Reviews. 2005;(4):128. doi: 10.1002/14651858.CD004456.pub2. [DOI] [PubMed] [Google Scholar]
- Drummond JE, Weir AE, Kysela GM. Home Visitation Programs for At-Risk Young Families. A Systematic Literature Review. Canadian Journal of Public Health. 2002;93(2):153–58. doi: 10.1007/BF03404559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dube SR, Felitti VJ, Dong M, Giles WH, Anda RF. The Impact of Adverse Childhood Experiences on Health Problems: Evidence from Four Birth Cohorts Dating Back to 1900. Preventive Medicine. 2003;37(3):268–77. doi: 10.1016/s0091-7435(03)00123-3. [DOI] [PubMed] [Google Scholar]
- Duggan A, Caldera D, Rodriguez K, Burrell L, Rohde C, Crowne SS. Impact of a Statewide Home Visiting Program to Prevent Child Abuse. Child Abuse & Neglect. 2007;31(8):801–27. doi: 10.1016/j.chiabu.2006.06.011. [DOI] [PubMed] [Google Scholar]
- Duggan A, McFarlane E, Fuddy L, Burrell L, Higman SM, Windham A, Sia C. Randomized Trial of a Statewide Home Visiting Program: Impact in Preventing Child Abuse and Neglect. Child Abuse & Neglect. 2004;28(6):597–622. doi: 10.1016/j.chiabu.2003.08.007. [DOI] [PubMed] [Google Scholar]
- Duggan AK, McFarlane EC, Windham AM, Rohde CA, Salkever DS, Fuddy L, Rosenberg LA, Buchbinder SB, Sia CC. Evaluation of Hawaii's Healthy Start Program. Future of Children. 1999;9(1):66–90. discussion 177–78. [PubMed] [Google Scholar]
- DuMont K, Mitchell-Herzfeld S, Greene R, Lee E, Lowenfels A, Rodriguez M, Dorabawila V. Healthy Families New York (HFNY) Randomized Trial: Effects on Early Child Abuse and Neglect. Child Abuse & Neglect. 2008;32(3):295–315. doi: 10.1016/j.chiabu.2007.07.007. [DOI] [PubMed] [Google Scholar]
- Eckersley R. Casualties of Change—The Predicament of Youth in Australia. Melbourne: Australian Commission for the Future; 1988. [Google Scholar]
- Edgeworth J, Carr A. Child Abuse. In: Carr A, editor. What Works with Children and Adolescents? A Critical Review of Psychological Interventions with Children, Adolescents and Their Families. London: Routledge; 2000. pp. 17–48. [Google Scholar]
- Evans E, Hawton K, Rodham K. Suicidal Phenomena and Abuse in Adolescents: A Review of Epidemiological Studies. Child Abuse & Neglect. 2005;29(1):45–58. doi: 10.1016/j.chiabu.2004.06.014. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Grant H, Horwood LJ, Ridder EM. Randomized Trial of the Early Start Program of Home Visitation. Pediatrics. 2005;116(6):e803–9. doi: 10.1542/peds.2005-0948. [DOI] [PubMed] [Google Scholar]
- Field T, Widmayer S, Greenberg R, Stoller S. Effects of Parent Training on Teenage Mothers and Their Infants. Pediatrics. 1982;69(6):703–7. [PubMed] [Google Scholar]
- Gardner JM, Walker SP, Powell CA, Grantham-McGregor S. A Randomized Controlled Trial of a Home-Visiting Intervention on Cognition and Behavior in Term Low Birth Weight Infants. Journal of Pediatrics. 2003;143(5):634–39. doi: 10.1067/S0022-3476(03)00455-4. [DOI] [PubMed] [Google Scholar]
- Gessner BD. The Effect of Alaska's Home Visitation Program for High-Risk Families on Trends in Abuse and Neglect. Child Abuse & Neglect. 2008;32(3):317–33. doi: 10.1016/j.chiabu.2007.08.004. [DOI] [PubMed] [Google Scholar]
- Gilbert R, Kemp A, Thoburn J, Sidebotham P, Radford L, Glaser D, MacMillan HL. Child Maltreatment Series 2: Recognising and Responding to Child Maltreatment. The Lancet. 2009a;373(9658):167–80. doi: 10.1016/S0140-6736(08)61707-9. [DOI] [PubMed] [Google Scholar]
- Gilbert R, Widom CS, Browne K, Fergusson D, Webb E, Janson S. Child Maltreatment Series 1: Burden and Consequences of Child Maltreatment in High-Income Countries. The Lancet. 2009b;373(9657):68–81. doi: 10.1016/S0140-6736(08)61706-7. [DOI] [PubMed] [Google Scholar]
- Gonzalez A, MacMillan HL. Preventing Child Maltreatment: An Evidence-Based Update. Journal of Postgraduate Medicine. 2008;54(4):280–86. doi: 10.4103/0022-3859.43512. [DOI] [PubMed] [Google Scholar]
- Gray JD, Cutler CA, Dean JG, Henry Kempe C. Prediction and Prevention of Child Abuse and Neglect. Child Abuse & Neglect. 1977;1(1):45–58. [Google Scholar]
- Guterman NB. Enrollment Strategies in Early Home Visitation to Prevent Physical Child Abuse and Neglect and the “Universal versus Targeted” Debate: A Meta-analysis of Population-Based and Screening-Based Programs. Child Abuse & Neglect. 1999;23(9):863–90. doi: 10.1016/s0145-2134(99)00062-9. [DOI] [PubMed] [Google Scholar]
- Hahn RA, Bilukha OO, Crosby A, Fullilove MT, Liberman A, Moscicki EK, Snyder S, Tuma F, Schofield A, Corso PS, Briss P. First Reports Evaluating the Effectiveness of Strategies for Preventing Violence: Early Childhood Home Visitation. Findings from the Task Force on Community Preventive Services. Morbidity & Mortality Weekly Report Recommendations & Reports. 2003;52(RR-14):1–9. [PubMed] [Google Scholar]
- Hardy JB, Streett R. Family Support and Parenting Education in the Home: An Effective Extension of Clinic-Based Preventive Health Care Services for Poor Children. Journal of Pediatrics. 1989;115(6):927–31. doi: 10.1016/s0022-3476(89)80744-9. [DOI] [PubMed] [Google Scholar]
- Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. 2009. Version 5.0.2 (updated September 2009). The Cochrane Collaboration. Available at http://www.cochrane-handbook.org (accessed December 12, 2009) [Google Scholar]
- Howard KS, Brooks-Gunn J. The Role of Home-Visiting Programs in Preventing Child Abuse and Neglect. Future of Children. 2009;19(2):119–46. doi: 10.1353/foc.0.0032. [DOI] [PubMed] [Google Scholar]
- Huxley P, Warner R. Primary Prevention of Parenting Dysfunction in High-Risk Cases. American Journal of Orthopsychiatry. 1993;63(4):582–88. doi: 10.1037/h0079478. [DOI] [PubMed] [Google Scholar]
- Infante-Rivard C, Filion G, Baumgarten M, Bourassa M, Labelle J, Messier M. A Public Health Home Intervention among Families of Low Socioeconomic Status. Children's Health Care. 1989;18(2):102–7. [Google Scholar]
- Johnston BD, Huebner CE, Anderson ML, Tyll LT, Thompson RS. Healthy Steps in an Integrated Delivery System—Child and Parent Outcomes at 30 Months. Archives of Pediatrics & Adolescent Medicine. 2006;160(8):793–800. doi: 10.1001/archpedi.160.8.793. [DOI] [PubMed] [Google Scholar]
- Kaaresen PI, Ronning JA, Ulvund SE, Dahl LB. A Randomized, Controlled Trial of the Effectiveness of an Early-Intervention Program in Reducing Parenting Stress after Preterm Birth. Pediatrics. 2006;118(1):e9–19. doi: 10.1542/peds.2005-1491. [DOI] [PubMed] [Google Scholar]
- Kahn J, Moore KA. Child Trends Fact Sheet—What Works for Home Visiting Programs: Lessons from Experimental Evaluations of Programs and Interventions. Washington, DC: Child Trends; 2010. [Google Scholar]
- Kearney MH, York R, Deatrick JA. Effects of Home Visits to Vulnerable Young Families. Journal of Nursing Scholarship. 2000;32(4):369–76. doi: 10.1111/j.1547-5069.2000.00369.x. [DOI] [PubMed] [Google Scholar]
- Keefe MR, Kajrlsen KA, Lobo ML, Kotzer AM, Dudley WN. Reducing Parenting Stress in Families with Irritable Infants. Nursing Research. 2006;55(3):198–205. doi: 10.1097/00006199-200605000-00006. [DOI] [PubMed] [Google Scholar]
- Kemp L, Harris E, McMahon C, Matthey S, Vimpani G, Anderson T, Schmied V. Miller Early Childhood Sustained Home-Visiting (MECSH) Trial: Design, Method and Sample Description. BMC Public Health. 2008;8(424):1–12. doi: 10.1186/1471-2458-8-424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kendrick D, Elkan R, Hewitt M, Dewey M, Blair M, Robinson J, Williams D, Brummell K. Does Home Visiting Improve Parenting and the Quality of the Home Environment? A Systematic Review and Meta Analysis. Archives of Disease in Childhood. 2000;82(6):443–51. doi: 10.1136/adc.82.6.443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kitzman H, Olds DL, Henderson CR, Jr, Hanks C, Cole R, Tatelbaum R, McConnochie KM, Sidora K, Luckey DW, Shaver D, Engelhardt K, James D, Barnard K. Effect of Prenatal and Infancy Home Visitation by Nurses on Pregnancy Outcomes, Childhood Injuries, and Repeated Childbearing. A Randomized Controlled Trial. JAMA. 1997;278(8):644–52. [PubMed] [Google Scholar]
- Koniak-Griffin D, Anderson NLR, Brecht ML, Verzemnieks I, Lesser J, Kim S. Public Health Nursing Care for Adolescent Mothers: Impact on Infant Health and Selected Maternal Outcomes at 1 Year Postbirth. Journal of Adolescent Health. 2002;30(1):44–54. doi: 10.1016/s1054-139x(01)00330-5. [DOI] [PubMed] [Google Scholar]
- Larson CP. Efficacy of Prenatal and Postpartum Home Visits on Child Health and Development. Pediatrics. 1980;66(2):191–97. [PubMed] [Google Scholar]
- Love JM, Kisker EE, Ross C, Raikes H, Constantine J, Boller K, Brooks-Gunn J, Chazan-Cohen R, Tarullo LB, Brady-Smith C, Fuligni AS, Schochet PZ, Paulsell D, Vogel C. The Effectiveness of Early Head Start for 3-Year-Old Children and Their Parents: Lessons for Policy and Programs. Developmental Psychology. 2005;41(6):885–901. doi: 10.1037/0012-1649.41.6.88. [DOI] [PubMed] [Google Scholar]
- Lutzker JR, Rice JM. Project 12-Ways: Measuring Outcome of a Large In-Home Service for Treatment and Prevention of Child Abuse and Neglect. Child Abuse & Neglect. 1984;8(4):519–24. doi: 10.1016/0145-2134(84)90034-6. [DOI] [PubMed] [Google Scholar]
- Lyons-Ruth K. Contributions of the Mother-Infant Relationship to Dissociative, Borderline, and Conduct Symptoms in Young Adulthood. Infant Mental Health Journal. 2008;29(3):203–18. doi: 10.1002/imhj.20173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacMillan HL, Wathen CN, Barlow J, Fergusson DM, Leventhal JM, Taussig HN. Interventions to Prevent Child Maltreatment and Associated Impairment. The Lancet. 2009;373(9659):250–66. doi: 10.1016/S0140-6736(08)61708-0. [DOI] [PubMed] [Google Scholar]
- Marcenko MO, Spence M. Home Visitation Services for At-Risk Pregnant and Postpartum Women: A Randomized Trial. American Journal of Orthopsychiatry. 1994;64(3):468–78. doi: 10.1037/h0079547. [DOI] [PubMed] [Google Scholar]
- Margolis PA, Stevens R, Bordley WC, Stuart J, Harlan C, Keyes-Elstein L, Wisseh S. From Concept to Application: The Impact of a Community-Wide Intervention to Improve the Delivery of Preventive Services to Children. Pediatrics. 2001;108(3):e42. doi: 10.1542/peds.108.3.e42. [DOI] [PubMed] [Google Scholar]
- McNaughton DB. Nurse Home Visits to Maternal-Child Clients: A Review of Intervention Research. Public Health Nursing. 2004;21(3):207–19. doi: 10.1111/j.0737-1209.2004.021303.x. [DOI] [PubMed] [Google Scholar]
- Mikton C, Butchart A. Child Maltreatment Prevention: A Systematic Review of Reviews. Bulletin of the World Health Organization. 2009;87(5):353–61. doi: 10.2471/BLT.08.057075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mulsow MH, Murray VM. Parenting on Edge: Economically Stressed, Single, African American Adolescent Mothers. Journal of Family Issues. 1996;17(5):704–21. [Google Scholar]
- Nair P, Schuler ME, Black MM, Kettinger L, Harrington D. Cumulative Environmental Risk in Substance Abusing Women: Early Intervention, Parenting Stress, Child Abuse Potential and Child Development. Child Abuse & Neglect. 2003;27(9):997–1017. doi: 10.1016/s0145-2134(03)00169-8. [DOI] [PubMed] [Google Scholar]
- Noar SM, Zimmerman RS. Health Behavior Theory and Cumulative Knowledge Regarding Health Behaviors: Are We Moving in the Right Direction? Heath Education Research. 2005;20(3):275–90. doi: 10.1093/her/cyg113. [DOI] [PubMed] [Google Scholar]
- Norr KF, Crittenden KS, Lehrer EL, Reyes O, Boyd CB, Nacion KW, Watanabe K. Maternal and Infant Outcomes at One Year for a Nurse-Health Advocate Home Visiting Program Serving African Americans and Mexican Americans. Public Health Nursing. 2003;20(3):190–203. doi: 10.1046/j.0737-1209.2003.20306.x. [DOI] [PubMed] [Google Scholar]
- Olds DL. Prenatal and Infancy Home Visiting by Nurses: From Randomized Trials to Community Replication. Prevention Science. 2002;3(3):153–72. doi: 10.1023/a:1019990432161. [DOI] [PubMed] [Google Scholar]
- Olds DL, Eckenrode J, Henderson CR, Jr, Kitzman H, Powers J, Cole R, Sidora K, Morris P, Pettitt LM, Luckey D. Long-Term Effects of Home Visitation on Maternal Life Course and Child Abuse and Neglect. Fifteen-Year Follow-Up of a Randomized Trial. JAMA. 1997;278(8):637–43. [PubMed] [Google Scholar]
- Olds DL, Henderson CR, Jr, Tatelbaum R, Chamberlin R. Improving the Delivery of Prenatal Care and Outcomes of Pregnancy: A Randomized Trial of Nurse Home Visitation. [erratum appears in Pediatrics, July 1986, 78(1):138] Pediatrics. 1986;77(1):16–28. [PubMed] [Google Scholar]
- Painter JE, Borba CPC, Hynes M, Mays D, Glanz K. The Use of Theory in Health Behavior Research from 2000 to 2005: A Systematic Review. Annals of Behavioral Medicine. 2008;35(3):358–62. doi: 10.1007/s12160-008-9042-y. [DOI] [PubMed] [Google Scholar]
- Pawson R, Greenhalgh T, Harvey G, Walsh K. Realist Review—A New Method of Systematic Review Designed for Complex Policy Interventions. Journal of Health Services Research & Policy. 2005;10(suppl):121–34. doi: 10.1258/1355819054308530. [DOI] [PubMed] [Google Scholar]
- Peden M, Oyegbite K, Ozanne-Smith J, Hyder AA, Branche C, Fazlur Rahman AKM, Rivara F, Bartolomeos K. World Report on Child Injury Prevention. Geneva: World Health Organization; 2008. [PubMed] [Google Scholar]
- Pinheiro PS. World Report on Violence against Children. Geneva: United Nations, Secretary-General's Study on Violence against Children; 2006. [Google Scholar]
- Productivity Commission. Report on Government Services 2011. Canberra: Australian Government; 2011. [Google Scholar]
- Quinlivan JA, Box H, Evans SF. Postnatal Home Visits in Teenage Mothers: A Randomised Controlled Trial. The Lancet. 2003;361(9361):893–900. doi: 10.1016/S0140-6736(03)12770-5. [DOI] [PubMed] [Google Scholar]
- Reeve R, van Gool K. Sydney: University of Technology, Centre for Health Economics Research and Evaluation (CHERE); 2010. The Long Run Impact of Child Abuse on Health Care Costs and Wellbeing in Australia. Working Paper 2010/10. Available at http://www.chere.uts.edu.au/pdf/wp2010_10.pdf (accessed January 20, 2011) [Google Scholar]
- Roberts I, Kramer MS, Suissa S. Does Home Visiting Prevent Childhood Injury? A Systematic Review of Randomised Controlled Trials. BMJ. 1996;312(7022):29–33. doi: 10.1136/bmj.312.7022.29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogers PJ, Petrosino A, Huebner TA, Hacsi TA. Program Theory Evaluation: Practice, Promise, and Problems. New Directions for Evaluation. 2000;2000(87):5–13. [Google Scholar]
- Runyan D, Wattam C, Ikeda R, Hassan F, Ramiro L. Child Abuse and Neglect by Parents and Caregivers. In: Krug E, Dahlberg L, Mercy J, Zwi A, Lozano R, editors. World Report on Violence and Health. Geneva: World Health Organization; 2002. pp. 59–86. [Google Scholar]
- Schore AN. Back to Basics: Attachment, Affect Regulation, and the Developing Right Brain: Linking Developmental Neuroscience to Pediatrics. Pediatrics in Review. 2005;26(6):204–17. doi: 10.1542/pir.26-6-204. [DOI] [PubMed] [Google Scholar]
- Schuler ME, Nair P, Black MM, Kettinger L. Mother-Infant Interaction: Effects of a Home Intervention and Ongoing Maternal Drug Use. Journal of Clinical Child Psychology. 2000;29(3):424–31. doi: 10.1207/S15374424JCCP2903_13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaw E, Levitt C, Wong S, Kaczorowski J, McMaster University Postpartum Research Group Systematic Review of the Literature on Postpartum Care: Effectiveness of Postpartum Support to Improve Maternal Parenting, Mental Health, Quality of Life, and Physical Health. Birth-Issues in Perinatal Care. 2006;33(3):210–20. doi: 10.1111/j.1523-536X.2006.00106.x. [DOI] [PubMed] [Google Scholar]
- Sidebotham P. An Ecological Approach to Child Abuse: A Creative Use of Scientific Models in Research and Practice. Child Abuse Review. 2001;10(2):97–112. [Google Scholar]
- Siegel E, Bauman KE, Schaefer ES, Saunders MM, Ingram DD. Hospital and Home Support during Infancy: Impact on Maternal Attachment, Child Abuse and Neglect, and Health Care Utilization. Pediatrics. 1980;66(2):183–90. [PubMed] [Google Scholar]
- Steel O’Connor KO, Mowat DL, Scott HM, Carr PA, Dorland JL, Young Tai KFW. A Randomized Trial of Two Public Health Nurse Follow-Up Programs after Early Obstetrical Discharge: An Examination of Breastfeeding Rates, Maternal Confidence and Utilization and Costs of Health Services. Canadian Journal of Public Health. 2003;94(2):98–103. doi: 10.1007/BF03404580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stevens-Simon C, Nelligan D, Kelly L. Adolescents at Risk for Mistreating Their Children: Part II: A Home- and Clinic-Based Prevention Program. Child Abuse & Neglect. 2001;25(6):753–69. doi: 10.1016/s0145-2134(01)00237-x. [DOI] [PubMed] [Google Scholar]
- St. Pierre RG, Layzer JI. Using Home Visits for Multiple Purposes: The Comprehensive Child Development Program. Future of Children. 1999;9(1):134–51. [PubMed] [Google Scholar]
- Sweet MA, Appelbaum MI. Is Home Visiting an Effective Strategy: A Meta-analytic Review of Home Visiting Programs for Families with Young Children. Child Development. 2004;75(5):1435–56. doi: 10.1111/j.1467-8624.2004.00750.x. [DOI] [PubMed] [Google Scholar]
- Thornberry TP, Henry KL, Ireland TO, Smith CA. The Causal Impact of Childhood-Limited Maltreatment and Adolescent Maltreatment on Early Adult Adjustment. Journal of Adolescent Health. 2010;46(4):359–65. doi: 10.1016/j.jadohealth.2009.09.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wagner MM, Clayton S, L The Parents as Teachers Program: Results from Two Demonstrations. Future of Children. 1999;9(1):91–115. [PubMed] [Google Scholar]
- WHO (World Health Organization) Preventing Child Maltreatment: A Guide to Taking Action and Generating Evidence. Geneva: World Health Organization, jointly sponsored by the WHO and the International Society for the Prevention of Child Abuse and Neglect; 2006. [Google Scholar]
- WHO (World Health Organization) World Health Organization Fact Sheet no. 150: Child Maltreatment. 2010. Available at http://www.who.int/mediacentre/factsheets/fs150/en/ (accessed August 9, 2010)
- WHO (World Health Organization) Georgia's Early Childhood Comprehensive System (GECCS) Implementation Project, Children's Trust Fund of Washington. 2011. Available at http://www.familytreemd.org/files/414_ChildAbusePrevTheoryofChangeLogicModel.pdf (accessed March 10, 2011)
- Wiggins M, Oakley A, Roberts I, Turner H, Rajan L, Austerberry H, Mujica R, Mugford M. The Social Support and Family Health Study: A Randomised Controlled Trial and Economic Evaluation of Two Alternative Forms of Postnatal Support for Mothers Living in Disadvantaged Inner-City Areas. Health Technology Assessment. 2004;8(32):iii–107. doi: 10.3310/hta8320. [DOI] [PubMed] [Google Scholar]
- Wiggins M, Oakley A, Roberts I, Turner H, Rajan L, Austerberry H, Mujica R, Mugford M, Barker M. Postnatal Support for Mothers Living in Disadvantaged Inner City Areas: A Randomised Controlled Trial. Journal of Epidemiology and Community Health. 2005;59(4):288–95. doi: 10.1136/jech.2004.021808. [DOI] [PMC free article] [PubMed] [Google Scholar]