

Abstract
A patient with electrocardiographic abnormalities after scorpion sting, simulating early myocardial infarction, is reported here. Pulmonary edema and congestive heart failure accompanied these electrocardiographic changes. The etiology of the cardiovascular manifestations in severe scorpion sting is related to the venom effects on the sympathetic nervous system and the adrenal secretion of catecholamines as well as to the toxic effects of the venom on the myocardium.
Keywords: Myocardial damage, pulmonary edema, scorpion bite
INTRODUCTION
Scorpion bites are common in our country, particularly in the rural areas. Among 86 species of scorpions present in India, Mesobuthus tumulus (Indian red scorpion) and Heterometrus swammerdami are of medical importance.[1] Though local symptoms including severe pain and burning sensation at the site of sting are the most common manifestations, systemic complications can ensue.[2] Cardiovascular manifestations are particularly prominent following stings by Indian red scorpion.[3] Such bites infrequently have serious clinical sequelae, including myocardial infarction, acute pulmonary edema, cardiogenic shock and even death. We present herein a case report with the clinical manifestations following scorpion bite mimicking acute myocardial infarction (AMI).
CASE PRESENTATION
A 35-year-old lady presented in the Emergency Department with complaints of breathlessness and chest pain associated with cold sweating since half an hour after being stung on her right middle finger by a red scorpion. Her past history was not significant and she had no predisposing cardiac risk factors. On examination, her blood pressure was 154/84 mmHg, heart rate 130/ min, regular and respiratory rate 36/min. There was an audible S3 with bilateral diffuse inspiratory basal crepts. Jugular venous pressure was raised. Serum cardiac enzymes were increased, and the level of creatine phosphokinase (CPK)-MB was 45 U/l and that of troponin-I was 0.06 ng/ml. Chest skiagram revealed pulmonary edema [Figure 1]. Electrocardiogram [Figure 2a] showed sinus tachycardia with secondary “ST-T” changes. However, subsequent ECG on the next day [Figure 2b] revealed normal sinus rhythm with “T”-wave inversions in leads I, aVL, V1 and V2, and ST segment elevation with concavity upward in leads II, III, aVF and V5, and V6. Echocardiogram demonstrated hypokinesia of interventricular septum and inferior posterior wall with moderate mitral and tricuspid regurgitation and left ventricular ejection fraction (LVEF) 28% [Figure 3a and b]. Finally, coronary angiogram was performed which revealed normal coronary vessels [Figures 4 and 5] with positive ergonovine and acetylcholine challenge test for coronary artery vasospasm. She undertook medications including antiplatelet drug and low-dose beta blockers. Her admission course was smooth and she was discharged uneventfully 5 days later. Follow-up ECG taken about 1 month later revealed only symmetric T-wave inversion in leads II, III, aVF and V2-6, and echocardiogram showed no regional wall motion abnormality, with well-preserved LVEF.
Figure 1.
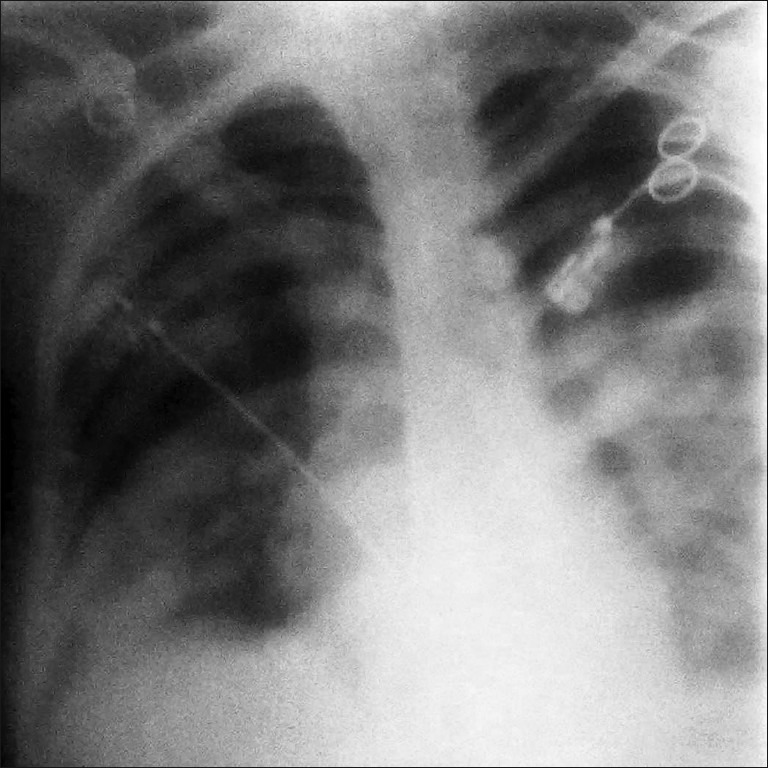
Chest skiagram showing pulmonary edema
Figure 2.
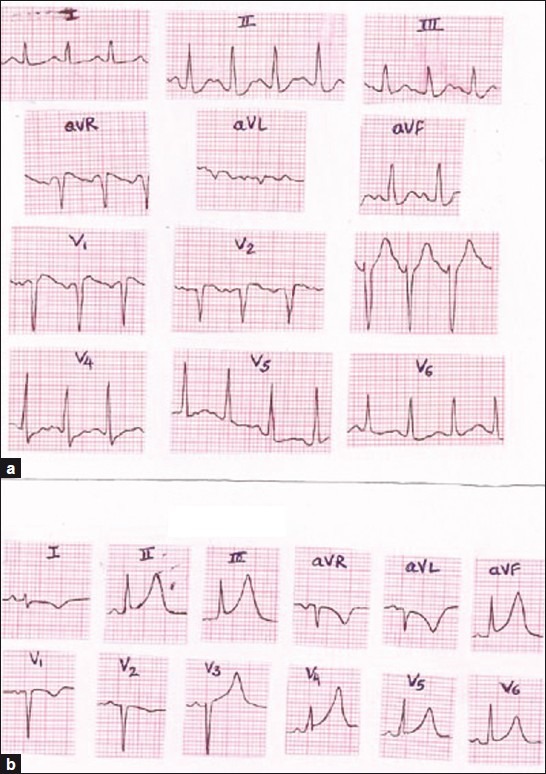
(a) Electrocardiogram showing sinus tachycardia with secondary “ST-T” changes. (b) ECG on the next day showing normal sinus rhythm with “T”-wave inversions in leads I, aVL, V1 and V2, and ST segment elevation with concavity upward in leads II, III, aVF and V5, and V6
Figure 3.
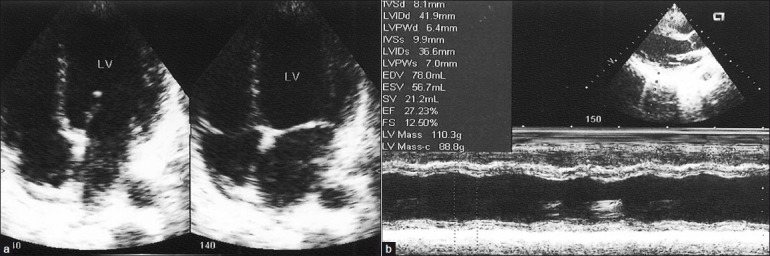
(a) Echocardiogram (apical four-chamber view) demonstrating hypokinesia of interventricular septum, (b) Echocardiogram (parasternal long axis view M mode) demonstrating hypokinesia of interventricular septum and inferior posterior wall with LVEF 28%
Figure 4.
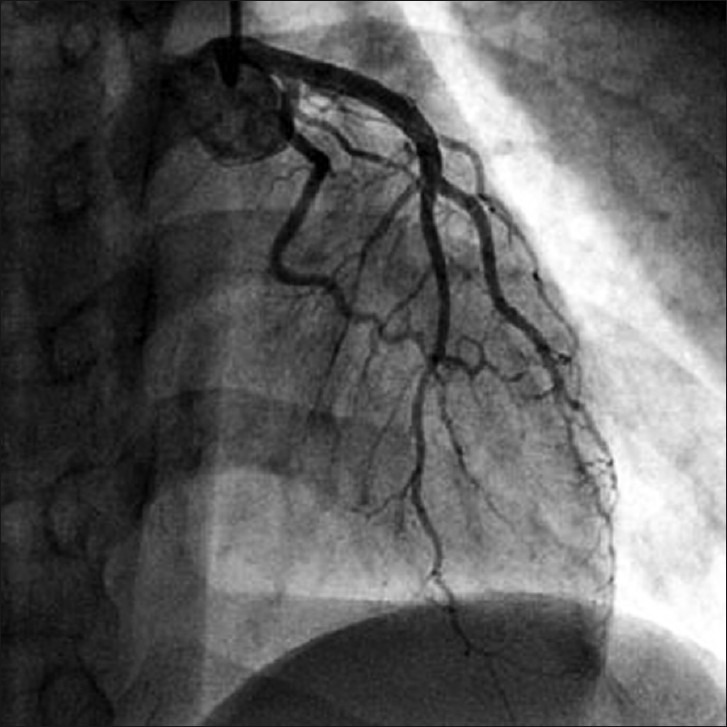
Left coronary angiogram showing normal left anterior descending and left circumflex arteries
Figure 5.
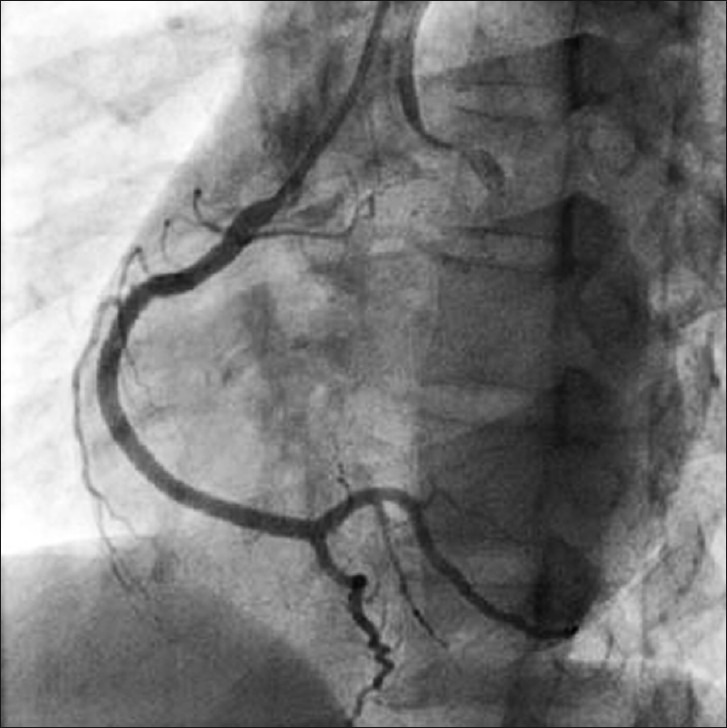
Right coronary angiogram showing normal right coronary artery
DISCUSSION
The scorpion venom is a water soluble antigenic complex mixture of neurotoxin, cardiotoxin, nephrotoxin, hemolysins, phosphodiesterases, phospholipase, hyaluronidases, histamine and other chemicals.[2] The venom can cause myocardial damage by several pathogenetic mechanisms:
Myocardial ischemia by coronary spasm: Release of vasoactive, inflammatory and thrombogenic peptides and amine constituents (histamine, serotonin, bradykinin, leukotrienes, thromboxane), which act on the coronary vasculature and induce coronary artery vasospasm and facilitate platelet aggregation as well as thrombosis.[4]
Direct cardiotoxic effect of the venom causing toxic myocarditis by reduction of Na-K-ATPase and adrenergic myocarditis by releasing adrenaline and noradrenaline from neurons, ganglia and adrenals, thereby increasing myocardial oxygen demand by direct inotropic and chronotropic effect on already compromised myocardial blood supply.[5]
Anaphylactic reaction: Release of allergenic proteins causes anaphylactic shock leading to hypotension with vasodilation and decreased of intravascular volume with reduced myocardial perfusion.
Scorpion venom inhibits angiotensin converting enzyme (ACE), resulting in accumulation of bradykinin, which is implicated in the development of pulmonary edema.[6]
In our patient, the findings mimicked AMI (including clinical symptoms, dynamic changes of ECG, elevated cardiac enzymes and regional wall motion abnormality). Probably, coronary vasospasm compounded with the above-mentioned sequences (myocarditis, pulmonary edema) has precipitated AMI in our case. AMI occurs very rarely after an arthropod envenomization. There are a few cases of AMI due to bee or scorpion bites reported in the literature.[7,8] Hence, it is worth reporting this rare entity.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Erfati P. Epidemiology, symptomatolgy and treatment of buthinae stings. In: Bettini S, editor. Arthropod Venoms: Hand book of experimental Pharmacology. New York: Spring Verlag; 1978. pp. 312–5. [Google Scholar]
- 2.Bawaskar HS, Bawaskar PH. Scorpion sting. J Assoc Physicians India. 1998;46:388–92. [PubMed] [Google Scholar]
- 3.Bawaskar HS, Bawaskar PH. Indian red scorpion envenoming. Indian J Pediatr. 1998;65:383–91. doi: 10.1007/BF02761131. [DOI] [PubMed] [Google Scholar]
- 4.Yang HP, Chen FC, Chen CC, Shen TY, Wu SP, Tseng YZ. Manifestations mimicking acute myocardial infarction after Honeybee Sting. Acta Cardiol Sin. 2009;25:31–5. [Google Scholar]
- 5.Rahav G, Weiss T. Scorpion sting induced pulmonary edema.Scintigraphic evidence of cardiac dysfunction. Chest. 1990;97:1478–80. doi: 10.1378/chest.97.6.1478. [DOI] [PubMed] [Google Scholar]
- 6.Bawaskar HS, Bawaskar PH. Management of scorpion sting. Heart. 1999;82:253–4. doi: 10.1136/hrt.82.2.253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Levine HD. Acute myocardial infarction following wasp sting.Report of two cases and critical survey of the literature. Am Heart J. 1976;91:365–74. doi: 10.1016/s0002-8703(76)80222-0. [DOI] [PubMed] [Google Scholar]
- 8.Wagdi P, Mehan VK, Burgi H, Salzmann C. Acute myocardial infarction after wasp stings in a patient with normal coronary arteries. Am Heart J. 1994;128:820–3. doi: 10.1016/0002-8703(94)90282-8. [DOI] [PubMed] [Google Scholar]