

Abstract
Background & objectives:
An increased number of cases with influenza like illness (ILI) were reported in Greater Kolkata Metropolitan Area (GKMA) during July and August 2010. We investigated these cases to confirm the outbreak, describe the distribution of patients and propose control measures.
Methods:
A suspected case of influenza like illness (ILI) was defined as acute onset of fever (>38°C) with cough or sore throat and a confirmed case as ILI case with throat swab positive for influenza A (H1N1) on RT-PCR. The demographic and clinical details were collected from patients attending the swine flu OPD of Infectious Disease Hospital, Kolkata, during July 5 to August 16, 2010.
Results:
Overall 440 patients with ILI attended the swine flu OPD of Infectious Disease and Bengal General hospital during the study period, of which 129 were positive for influenza A (H1N1). Four patients died (case fatality ratio: 0.90%). Besides fever, common symptoms included cough (73%), running nose (54%), sore throat (43%), respiratory distress (25%) and diarrhoea (4%). Forty seven (11%) patients (including the four who died) had co-morbidities. The outbreak started on July 10, peaked on July 24 and subsided by August 14, 2010. A total of 372 (85%) patients were from GKMA. Majority (n=168, 45%) of the cases from GKMA were from 6 boroughs of Kolkata Municipal Areas.
Interpretation & conclusions:
An outbreak of influenza A (H1N1) occurred in Kolkata predominantly affecting young and middle aged population. State health authorities implemented several interventions to limit the outbreak including training of health care providers in case management and infection control, vaccination of health care workers, creation of isolation wards and administration of oseltamivir to ILI patients, and community health education about social distance and personal hygiene measures.
Keywords: A (H1N1), pandemic influenza, swine flu
A novel influenza A (H1N1) virus resulting from triple re-assortment emerged in Mexico and the USA in 20091. In late April 2009, WHO declared that the emergence of this virus represented a ‘public health emergency of international concern’ and on June 2009, raised the phase of pandemic alert to six, indicating the emergence of the new influenza pandemic. The H1N1 virus had spread with great speed to all the continents and caused considerable human suffering and an adverse impact on the health services and the economy. Worldwide, 214 countries and overseas territories or communities had reported laboratory confirmed cases of pandemic influenza A (H1N1) including at least 18,449 deaths as on August 20102.
In India, the first confirmed case of pandemic influenza A (H1N1) was reported in Hyderabad on May 16, 20093 and by July 2010, a total of 34,669 laboratory confirmed cases including 1,692 deaths were reported4. During June 2009 to July 2010, a total of 2971 nasal/throat swabs from suspected influenza patients were tested from the eight States (West Bengal, Bihar, Orissa, Meghalaya, Mizoram, Tripura and Andaman and Nicobar islands). Among these, 382 (12.9%) were positive for the influenza A and 103 (3.5%) for influenza B. About 75 per cent of the influenza A positives were sub-typed as pandemic H1N1 (pH1N1) while the remaining were due to seasonal H1N1 and H3N25. West Bengal reported 265 cases of pandemic H1N1 during this period. Only one case was reported from the State during January to June 20105. Since July 2010, there were increased number of cases of influenza like illness (ILI) reported in the Kolkata metropolitan area. We conducted an outbreak investigation to confirm the aetiology, describe the distribution of case-patients by time, place and person, and recommend control measures.
Material & Methods
Case definition: A case of influenza like illness (ILI) was defined as an acute onset of fever (>38 °C) with or without cough or sore throat in the absence of any other diagnosis6. A person with ILI with laboratory confirmation for influenza A (H1N1) on a throat swab by real time reverse transcriptase polymerase chain reaction (RT-PCR) was considered as confirmed case of pandemic influenza (H1N1)7. All the patients meeting the above case definitions and attending the swine flu OPD of Infectious Disease and Bengal General (ID&BG) hospital, Kolkata, were included in the study. Following the death of one confirmed case of H1N1 infection, the Government of West Bengal made it mandatory to refer all ILI cases from private hospitals, medical college hospitals to ID&BG Hospital, Kolkata, for laboratory confirmation.
Data collection: At the time of collecting throat swabs for laboratory confirmation, complete address of the suspected patients was collected. Patients with positive laboratory tests for pandemic H1N1 were encouraged to get admission in the swine flu ward of ID&BG Hospital for treatment. Patients (or their relatives) admitted in other nursing homes were also contacted using the addresses provided by them at the time of laboratory testing.
A team of seven health workers collected information from all the cases of ILI about the demographic details, residence, date of onset of illness, clinical details, results of laboratory investigations, history of travel within and outside the country and history of contact with positive case of influenza (H1N1).
Laboratory investigation: Throat swabs were collected from all the ILI patients in sterile viral transport medium and transported under cold chain to the National Institute of Cholera and Enteric Diseases, (ICMR), Kolkata, the State referral laboratory, for RT-PCR using the CDC/WHO testing protocol for influenza A (H1N1)8.
Data analysis: We calculated the proportion of suspected and laboratory confirmed cases by age groups and gender. The epidemic curve was drawn to study the distribution of cases by time and an area map to know the geographical distribution of all the cases. For describing the distribution by geographic areas, only those patients residing in Greater Kolkata Metropolitan Areas (GKMA) were considered and census population was used as denominator to calculate the attack rates. Greater Kolkata Metropolitan Areas (GKMA) comprise of (i) Kolkata Metropolitan Corporation area (KMC), (ii) Howrah Municipal Corporation areas (HMC), and (iii) three adjacent municipalities from district Nadia, 20 adjacent municipalities from North 24 Parganas district, nine adjacent municipalities from Hooghly district and five adjacent municipalities from district South 24 Parganas. There are 15 boroughs (administrative units) in KMC and five in HMC area.
Results & Discussion
Between July 5 and August 16, 2010, a total of 893 patients attended the swine flu OPD of ID&BG Hospital, Kolkata (average 29 patients per day). Of them, 440 (49%) had symptoms of ILI and their throat swabs were sent to laboratory investigations. Of these 440 ILI throat swabs 149 (33.9%) were referred from the private nursing homes or medical college hospitals. Influenza A (H1N1) virus infection was confirmed in 129 (29%) patients (Table I). Of the 129 laboratory confirmed patients, 96 (74%) were admitted in the ID&BG Hospital, 30 (23%) in the private nursing homes/ medical college hospitals, while three patients remained isolated in their houses (Table I).
Table I.
Distribution of influenza like illness (ILI) cases during the H1N1 outbreak, Greater Kolkata Metropolitan Areas, West Bengal, India 2010
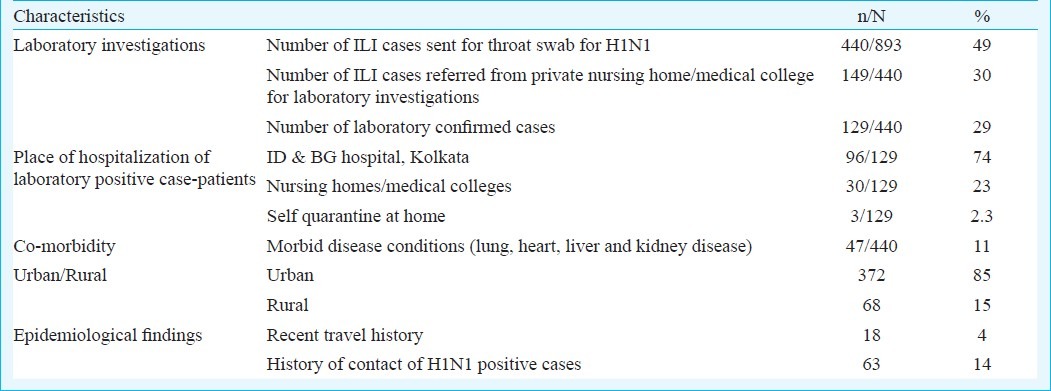
The commonest symptoms included fever (100%), cough (73%), running nose (54%), sore throat (43%), respiratory distress (25%) and diarrhoea (4%). Forty seven patients (11%) had associated co-morbid conditions. The common co-morbidities were chronic obstructive pulmonary disease (COPD) (29.8%), cardiovascular disease (21.3%), liver (10.6%), kidney (10.6%) disease and 2 per cent had diabetes. All except four patients recovered with 5-7 day course of oseltamivir, antibiotics and paracetamol (Case fatality ratio=0.90%). Of the four patients who died, three were aged >50 yr while one was 13 yr old. All had associated co-morbid conditions such as COPD, chronic renal failure, heart failure and hepatitis.
Most of the suspected (n=269, 61.1%) and laboratory confirmed (n=77, 59.7%) cases were in the age group of 15-49 yr [Table II]. ILI cases started occurring from July 10, 2010 with several peaks in the epidemic curve and subsided on August 14, 2010 (Fig. 1). Of the 440 cases, 372 (85%) were from Greater Kolkata Metropolitan areas, while 68 (15%) were from neighbouring districts and States. In GKMA, cases were reported from all the boroughs of the KMC (except borough number 2) and one borough in HMC. Six boroughs in KMC (Number 3, 5, 6, 10, 12 and 14) accounted for 45 per cent (168/372) cases while Bidhannagar and Dum Dum municipality together accounted 20 per cent of the cases (Fig. 2). Sixty three (14%) patients gave history of contact with laboratory confirmed cases of influenza A (H1N1) in the previous week, while 18 (4%) had a recent travel history (either abroad or other States of the country) (Table I).
Table II.
Proportion of suspected and confirmed cases of influenza by age group and gender, West Bengal, India 2010
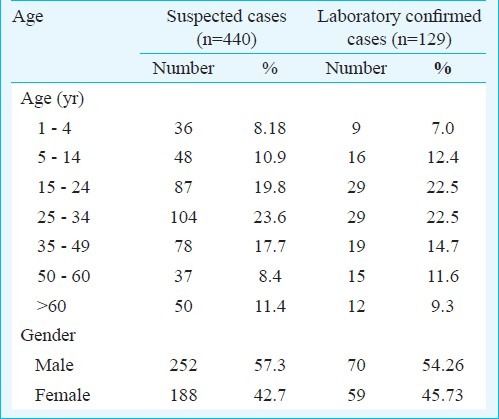
Fig. 1.
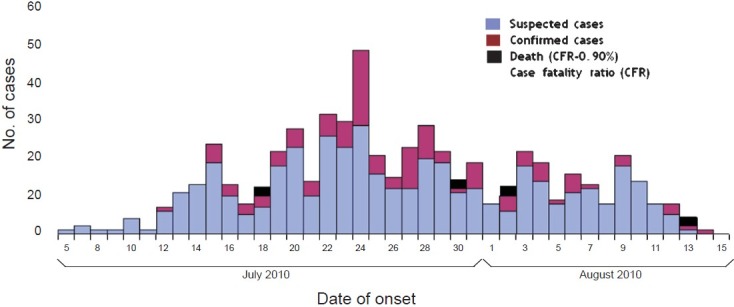
Epidemic curve of swine flu outbreak at Greater Kolkata Metropolitan Area, West Bengal, India, 2010
Fig. 2.
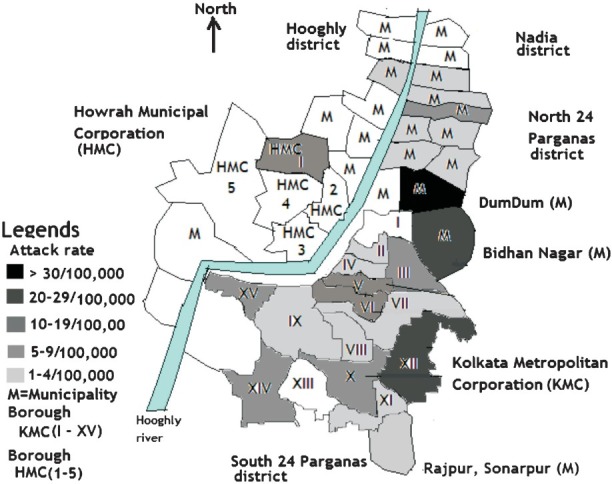
Attack rate per 100,000 population of ILI by borough of Kolkata Metropolitan Corporation, Howrah Municipal Corporation and municipality areas of Greater Kolkata Metropolitan Areas, West Bengal, India, 2010 (Map not to scale)
In India, the earlier H1N1 outbreaks have been reported in institutional settings9,10. The outbreak in Kolkata occurred in the urban population with about half of the cases being reported from six boroughs in KMC, suggesting the possibility of close contact with cases. The outbreak predominantly affected the young and middle aged individuals and the time of occurrence corresponded to the peak season of influenza transmission in India11,12. Majority of the cases were uncomplicated and responded to anti-viral treatment. The case fatality ratio of 0.90 per cent observed in this outbreak was comparable to the CFR estimates of 0.004-1.5 per cent reported from other countries13.
In August 2010, WHO declared the post-pandemic phase of the H1N1. During this phase, cases and outbreaks due to the H1N1 (2009) virus would continue to occur. Early detection of these outbreaks and implementation of control measures are essential to limit the transmission. The West Bengal State Health Department initiated several control measures. The IB & BG Hospital, Kolkata, was designated as the nodal hospital for treatment of cases with a swine flu ward consisting of 35 beds. Facilities for isolation and treatment were also established at the designated nursing homes, medical colleges as well as district hospitals. In Kolkata alone, a total 310 isolation beds in 25 health institutions were made ready for such cases. These health facilities were supplied with adequate quantities of antivirals. All the nursing personnel, doctors, paramedical staffs engaged in the swine flu ward were vaccinated with swine flu vaccine. Government of West Bengal also made it mandatory for all the private nursing homes to refer the cases of ILI to ID&BG Hospital for laboratory test of H1N1 virus. The laboratory confirmed ILI patients were encouraged to get admission in ID & BG Hospital, Kolkata, private nursing home or medical college hospitals. Five days treatment with osteltamivir (Tamiflu) was administered to all the laboratory confirmed patients as well as their close family contacts. Extensive information, education and communication (IEC) activities were done in the communities to educate the people about prevention of influenza.
Acknowledgment
The authors acknowledge Drs Akhil Bandhu Biswas, Asit Kumar Biswas and Sukanta Biswas from Directorate of Health Services, Government of West Bengal, India; the medical officers and para-medical staff of ID&BG Hospital, Kolkata, West Bengal, and Director, NICED, staff of NICED, Kolkata, for their co-operation and help.
References
- 1.Dawood FS, Jain S, Finelli L, Shaw MW, Lindstrom S, Garten RJ, et al. Novel Swine-Origin Influenza A (H1N1) Virus Investigation Team. Emergence of a novel swine-origin influenza A (H1N1) virus in humans. N Engl J Med. 2009;360:2605–15. doi: 10.1056/NEJMoa0903810. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization (WHO) Pandemic (H1N1) 2009-Update 112. 2010. Aug 06, [accessed on October 12, 2011]. Available from: http://www.who.int.csr/don/2010_08_06/en/index.hmt .
- 3.Ministry of Health and Family Welfare, Government of India. Pandemic Influenza A (H1N1) Situational Update. 2009. May 16, [accessed on October 12, 2011]. Available from: http://mohfw-h1n1.nic.in/ documents/PDF/ SituationalUpdatesArchives/may/ Situational%20Updates%20on%2016.05.2009.pdf .
- 4.Ministry of Health and Family Welfare, Government of India. Consolidated status of Influenza A H1N1. 2009. Dec 31, [accessed on October 12, 2011]. Available from: http://mohfw-h1n1.nic.in/documents/PDF/SituationalUpdates Archives/ december/Situational%20Updates%20on%2031.12.2009.pdf .
- 5.Mukherjee A, Roy T, Agrawal AS, Sarkar M, Lal R, Chakrabarti S, et al. Prevalence and epidemiology of pandemic H1N1 strains in hospitals of Eastern India. J Public Health Epidemiol. 2010;2:171–4. [Google Scholar]
- 6.Ministry of Health and Family Welfare, Government of India. 2010. Jun 27, [accessed on October 12, 2011]. Available from: http://mohfwh1n1.nic.in/documents/PDF/SituationalUpdatesArchives/June/ Situational%20Updates%20on%2027.06.2010.pdf,
- 7.World Health Organization (WHO) A practical guide to harmonizing virological and epidemiological influenza surveillance. 2008. [accessed on October 12, 2011]. Available from: http://www.wpro.who.int/entity/emerging_diseases/documents/GuideToHarmonizingInfluenzaSurveillance-revised2302/enlindex.html .
- 8.World Health Organization. CDC protocol of realtime RTPCR for influenza A (H1N1) [accessed on October 12, 2011]. Available from: http://www.who.int/csr/resources/publications/swineflu/CDCRealtimeRTPCR_SwineH1Assay-2009_20090430.pdf .
- 9.Gurav YK, Pawar SD, Chadha MS, Potdar VA, Deshpande AS, Koratkar SS, et al. Pandemic influenza A(H1N1) 2009 outbreak in a residential school at Panchgani, Maharashtra, India. Indian J Med Res. 2010;132:67–71. [PubMed] [Google Scholar]
- 10.Raut DK, Singh S, Roy N, Nair D, Sharma R. Influenza A virus outbreak in Police Training School, Nazafgarh, Delhi 2009. Indian J Med Res. 2010;132:731–2. [PMC free article] [PubMed] [Google Scholar]
- 11.Rao BL, Banerjee K. Influenza surveillance in Pune, India, 1978-90. Bull World Health Organ. 1993;71:177–81. [PMC free article] [PubMed] [Google Scholar]
- 12.Agrawal AS, Sarkar M, Chakrabarti S, Rajendran K, Kaur H, Mishra AC, et al. Comparative evaluation of real-time PCR and conventional RT-PCR during a 2 year surveillance for influenza and respiratory syncytial virus among children with acute respiratory infections in Kolkata, India, reveals a distinct seasonality of infection. J Med Microbiol. 2009;58:1616–22. doi: 10.1099/jmm.0.011304-0. [DOI] [PubMed] [Google Scholar]
- 13.Bautista E, Chotpitayasunondh T, Gao Z, Harper SA, Shaw M, Uyeki TM, et al. Writing Committee of the WHO Consultation on Clinical Aspects of Pandemic (H1N1) 2009 Influenza. Clinical aspects of pandemic 2009 influenza A (H1N1) virus infection. N Engl J Med. 2010;362:1708–19. doi: 10.1056/NEJMra1000449. [DOI] [PubMed] [Google Scholar]