

Abstract
Context:
Standards for an aesthetic face are dynamic. The current trend is towards a leaner looking face with preservation of the inverted triangle of youth. Procedures that have been reported to be employed for correction of a chubby face include buccal fat pad excision, facial liposuction and injection lipolysis. In addition to giving the face an aesthetic triangular cut, chin and malar augmentation may be performed. The rounded appearance at the angles may further be reduced by injection of Botulinum toxin into the masseter.
Materials and Methods:
Forty patients who presented to us for correction of chubby (round) faces were analysed and treated by facial sculpting surgery, which included at least two of the procedures in combination. The procedures included facial liposuction, buccal fat pad excision, chin augmentation, malar augmentation and injection lipolysis. All cases were followed-up for a minimum of 6 months after surgery.
Results:
Aesthetic expectations of the patients were met in 39 cases, one patient complained of facial asymmetry following facial liposuction and was subjected to a touch-up injection lipolysis.
Conclusions:
A combination of procedures is necessary to give the face an attractive contour. All the individual procedures have stood the test of time and are safe, proven and are put in mainstream. However, a thorough analysis of the face preoperatively and then subjecting the patient to a combination of these procedures in a single surgical sitting has yielded good results as seen in this study.
KEY WORDS: Chubby face, facial restructuring, facial sculpting, round face
INTRODUCTION
With increasing globalisation, people all across the world tend to form common concepts of beauty, disregarding the ethnic concepts of attractiveness. Chubby cheeks were once considered desirable in an Indian scenario, reflecting the overall health status of not only the individual but the family as a whole. With increasing exposure to international media, both over the television and over the Internet, the concepts of beauty have been globalised to a leaner looking face with maximal fullness in the malar region forming the base of the inverted triangle of youth. With these concerns in mind, there has been an increase in the number of younger patients seeking a leaner looking face.
The techniques used to reduce facial fat are facial liposuction,[1,2] injection lipolysis[3–7] and buccal fat pad excision.[8,9] The areas of face that need augmentation are tackled by malar and chin augmentation by implants.[10] Injection of botulinum toxin type A is an effective alternative for contouring of the lower facial profile by reducing the bulkiness of masseteric muscles.[11] The available literature on these techniques[1–11] has established the usefulness and safety of these individual procedures. The procedures need to be selected carefully in an appropriate combination for a particular patient, and the face needs to be literally sculpted to provide the chiselled look of youth.
We present our technique of facial evaluation and the combination of these procedures: “Facial sculpting”, to achieve a leaner well-defined face.
MATERIALS AND METHODS
We included 40 patients who presented to us with a round or chubby face for correction of facial shape. The patients included in this study are only select patients who required a combination of procedures. The patients were photographed in standard views for face, viz. front, right lateral, left lateral, right three-quarters, left three-quarters and worms eye views. Life size prints were taken and problem areas and options for treatment were discussed in detail with the patients. In addition, if skeletal augmentation was to be considered, a cephalometric analysis was performed for the patients to know the relative projections offered by bony and soft tissue elements to the facial contours. The areas to be augmented and the size of implants were thus selected. Only the patients requiring a combination of procedures were included in the study. Cases that could be managed by any single procedure were excluded. All patients were evaluated keeping the following points in mind:
Aesthetic division of the face in thirds.
Fat deposits along the jaw line and submental region.
Fullness in the buccal area.
Bony prominence of chin and cheeks.
Soft tissue prominence over the malar area.
Bulk of masseter muscle.
The surgical plan was made in a logical and straightforward manner.
Excess fat deposits along the jaw line, submental area and cheeks were to be treated by suction-assisted lipoplasty (SAL).
Bulky masseter was to be reduced in prominence by serial injections of botulinum toxin [Figure 1].
Minimal excess fat over the malar areas reduced with injection lipolysis [Figure 2].
Fullness in the buccal area was to be treated by partial excision of buccal fat pad [Figure 3].
Retruded/small chin leading to a rounded or squarish face was to be offered chin augmentation with extended silicon chin implants [Figure 4].
Malar hypoplasia was addressed by silicone malar implants.
Figure 1.

Marking for injection points of BTX-A chemical debulking of masseter
Figure 2.

Markings for injection lipolysis over the face
Figure 3.

Intraoperative photograph showing buccal fat pad removal trough an upper gingivobuccal approach
Figure 4.
(a) Preoperative photograph case 1. (b) Postoperative photographs of case 1 after chin implant, malar injection lipolysis and buccal fat pad removal
Injection lipolysis has come up as a new technique to target localised areas of fat deposits. We used this technique only in patients who had minimal excess of fat or who had reservations about SAL over their faces, predominantly over the malar areas.
SAL of facial fat deposits was performed after preoperatively topographic marking of the facial fat deposits in the standing position. Standard 2 mm or 1.5 mm cannula was used with wet technique of fluid infiltration to aspirate the fat deposits over the jaw line, submental and, rarely, cheek regions. The access points used were retoauricular and submental. The end point of liposuction was determined by visual symmetry and equal skin fold thickness on palpation. As a rule, all patients after facial liposuction were given sponge dressings for 5 days postoperatively and the liposuction access points were left open.
Bucccal fat pad excision was performed through intraoral upper gingivobuccal sulcus incision opposite the first and second molar teeth, preserving a cuff of mucosa for closure. The buccal extension of Bichet's fat pad was exposed by blunt dissection using curved haemostat, and was gently teased out. The base of the fat pad was cauterised, with the cut taking care of the parotid duct. The mucosa was then loosely approximated with a continuous chromic catgut stitch.
To address the retruded chin, which exaggerates the chubby look, we used extended silicon chin implants. The implant was placed through an incision, placed in the lower third of the lip, about 5-8 mm away from the inferior gingivobuccal sulcus, leaving a cuff of periosteum and mentalis muscle over the mandible in the symphyseal region. The implant was however in direct contact with the bone laterally on both sides. Extended silicone implant gives perfect smoothening effect, and the implant edge is not felt or seen and has thus never been a problem with these implants for us. Malar implant was placed through the upper gingivobuccal sulcus incision. It was secured in place with a screw and a pull-through suture on a bolster through the malar region. The suture was kept in place for a period of 5-7 days.
Injection lipolysis was performed mainly for excess fat deposits over the malar areas, as any liposuction in this area can lead to an appearance of an aged face. Injection lipolysis was performed by 2.5% phophatidyl choline solution diluted in saline. The areas to be treated were premarked with a 1 cm2 grid and 0.3 mL of lipolysis solution was injected in each point using a 27 G needle. The depth of injection was superficial into the subcutaneous fat layer. A maximum of 20 mL of 2.5 % solution is required to treat the entire face.
The squarish appearance to the face, if it was contributed by masseter muscle hypertrophy, was addressed by injection of botulinum toxin into the masseter. We used eight to 12 units of botulinum toxin in each masseter in each session for a total of one to three sessions, 10 days apart.
RESULTS
A total of 40 cases underwent facial sculpting with a combination of two or more procedures, which included face liposuction, injection lipolysis, chin augmentation, malar augmentation and botulinum toxin injection into the masseter. In 39 patients, we were able to achieve the desired results without any major complications. Minor complications like paraesthesiae in the region of the lower lip and abnormal mobility of the lower lip were encountered in five patients. We treated these patients with a course of systemic steroids for a period of 5 days, and the patients recovered uneventfully. Of the 29 cases of buccal fat pad excision, three patients complained of restricted mouth opening in the early postoperative period, probably due to pain and spasm of the masticatory muscles. All of them responded well to jaw stretching exercises. One patient complained of facial asymmetry following facial liposuction and buccal fat pad excision [Figure 5b]. She was subjected to a touch-up with one sitting of injection lipolysis 6 weeks after the initial surgery. The asymmetry reduced to a great level and she was satisfied with her looks at the end of it [Figure 5c].
Figure 5.
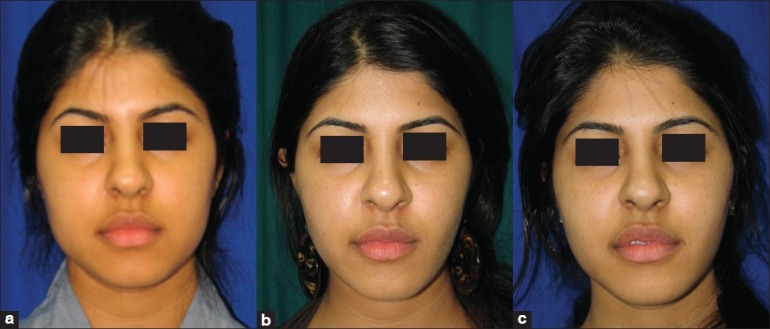
(a) Preoperatice photo case 2. (b) Post operative photograph of case 2 after facial liposuction, chin implant and buccal fat pad excision. Patient was unhappy with the facial asymmetry left less than right. (c) Second Post operative photo of case 2 after injection lipolysis on the right hemiface
Chin implants were required in 35 (87.5%) cases. The number of patients requiring facial liposuction was 31 (77.5%), whereas injection lipolysis was performed in 11 (27.5%) patients.
These and all other procedures performed have been depicted in Table 1, Figures 6 and 7 are examples of results that can be obtained by a judicious combination of these procedures.
Table 1.
Procedures performed
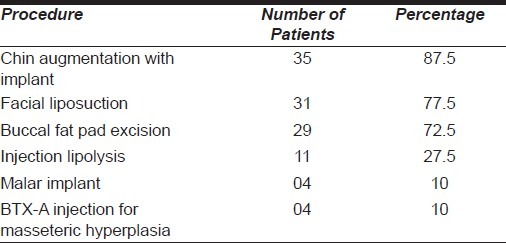
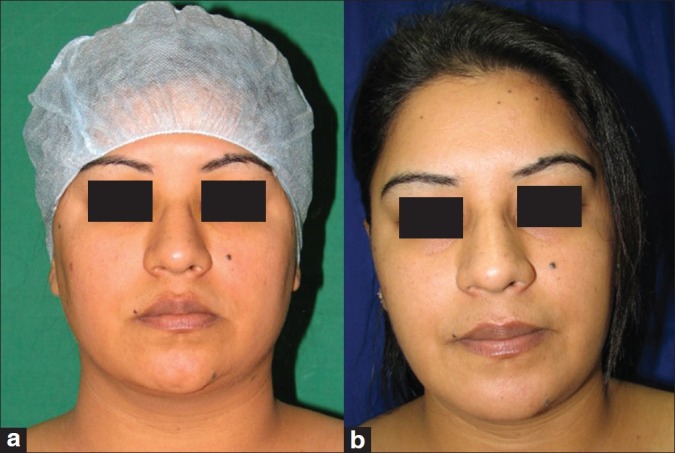
Figure 6.

(a) Preoperative photo graph case 3. (b) Post operative photograph of case 3 after facial liposuction and chin augmentation with extended silicone implant
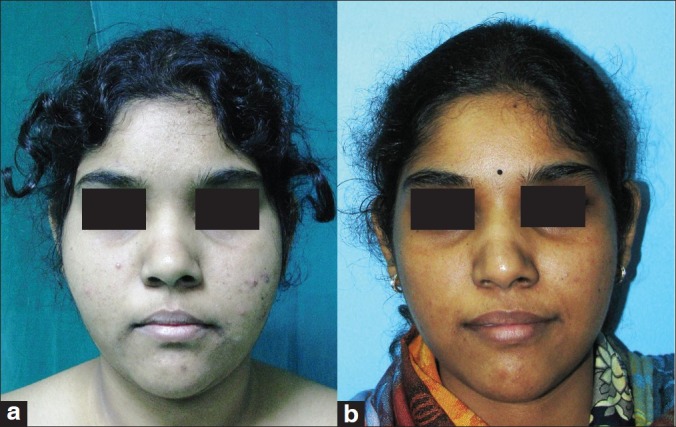
Figure 7.
(a) Preoperative photograph of case 4. (b) Postoperative photograph of case 4 after buccal fat pad excision, malar lipolysis with facial liposuction and two sittings of BTX-A injections for masseteric debulking
DISCUSSION
The face happens to be the most exposed part of one's body, and is an outlet for an individual to the society through his/her varied emotional expressions. Added to this is the constant attention that one pays to the appearance of one's face because it forms a prominent part of their physical persona. With easy access to social media across the world, the quest for a leaner looking face is deeply hidden along with, perhaps, personal and, additionally, social and professional factors. Facial aesthetic surgery has progressed leaps and bounds since its inception at the turn of the century. Surgeons’ armamentarium of procedures to tackle specific problems has increased and one needs to carefully select the appropriate techniques to meet a desired result.[12]
Liposuction of the subcutaneous fat in the face has been attended with caution, as overzealous treatment of this area may result in contour irregularities or neuropraxia of the marginal mandibular nerve.[13] Lipoplasty of the face and neck continues to be popular. There have been improvements in instrumentation, with laser and powered lipoplasty improving the efficiency of fat removal.[14] We, in this study population, performed superficial liposuction of the face for submental and jaw line areas with fine Klien facial cannulae and did not come across any permanent complication except that one of the patients reported asymmetry. We preferred not to do aggressive liposuction over the malar areas as in case the skin over there fails to retract adequately after liposuction it gives an aged and tired look to the face due to exaggeration of the nasolabial fold. In all patients having exogenous fat deposits in this area, we treated them with injection lipolysis and the patients were satisfied with the result.
The buccal pad of fat (Bichet's fat pad)[15] is frequently the cause of fullness of the facial structure in patients with rounded face. Many such patients remain unsatisfied with repeated attempts of facial liposuction and injection. The buccal pad of fat has four limbs and a central portion.[8] It is primarily the central portion and the buccal limb that is excised through the intraoral route. The decrease in bulk of this fat pad gives an appreciable improvement in the face, as this fat is located deep to the muscle layer and is inaccessible to liposuction. Also, the buccal pad of fat is resistant to lipolysis as evidenced by its persistence in even the most emaciated patients.[16] Due consideration is to be given to the amount of fat removed from each side to avoid facial asymmetry. We always compared the amount of fat excised from each side.
Rosen, through his detailed writings about facial aesthetics, has pointed out that when given alternatives to satisfy occlusal inadequacies, it is usually better to expand rather than to reduce the facial skeleton. This skeletal expansion provides support for, and allows better drape of, the soft-tissue mask with, as he demonstrated, a more youthful and attractive appearance.[17,18] A rounded face is in relative terms having a shorter chin and, in some cases, a hypoplastic-looking malar eminence. The patients in whom it was relatively deficient were augmented using silicone implants. It has been our policy to use silicone implants instead of porous polyethylene implants. Augmenting the malar and chin areas worked wonders in combination, with reduction of areas with excess fat deposits. The effect was not only additive but synergistic in reaching a slimmer and longer looking face.
The study of Asian face structure reveals that the lower third is much wider in Asians as compared with Caucasians. The attributes to this have been found to be both the size of the mandible as well as the bulk of the masseter. The surgical procedures to deal with these problems are major undertakings and with a myriad of complications. Hence, a nonsurgical way to chemically decrease the mass of the masseter muscle by injection of botulinum toxin type A was described.[19] The effect of botulinum toxin-induced denervation atrophy is noticed only after 2 weeks, and maximal effect was observed in 9–12 weeks. However, there was return of the muscle bulk between 6 and 8 months following the injection. For this, repeated injections were given and the dose of botulinum toxin was gradually reduced with each sitting, and the effect was found to be longer lasting at the subsequent visits.
CONCLUSION
Thus, it was observed that instead of dealing with the constituents of chubby face problem one at a time, a multipronged approach in one surgical sitting offered a synergistic advantage, without increasing the chances of complications. The patients were very much satisfied with the final outcome of the procedure. Facial sculpting is a good term to denote the combination of procedures to alter the facial soft tissue structure.
Footnotes
Presentation at a meeting: Organisation: 43 rd Annual meeting of Association of Plastic Surgeons of India. Place: Varanasi. Date : Nov 2008
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Goodstein WA. Superficial liposculpture of the face and neck. Plast Reconstr Surg. 1996;98:988–96. doi: 10.1097/00006534-199611000-00009. [DOI] [PubMed] [Google Scholar]
- 2.Illouz YG. Body contouring by lipolysis: A five-year experience with over 3000 cases. Plast Reconstr Surg. 1983;72:591–7. doi: 10.1097/00006534-198311000-00001. [DOI] [PubMed] [Google Scholar]
- 3.Rotunda AM, Kolodney MS. Mesotherapy and phosphatidylcholine injection: Historical clarification and review. Dermatol Surg. 2006;32:465–80. doi: 10.1111/j.1524-4725.2006.32100.x. [DOI] [PubMed] [Google Scholar]
- 4.Madhere S, editor. Aesthetic Mesotherapy and Injection Lipolysis in Clinical Practice. London: Informa Healthcare; 2007. p. 202. [Google Scholar]
- 5.Duncan D, Rubin JP, Golitz L, Badylak S, Kesel L, Freund J, et al. Refinement of technique in injection lipolysis based on scientific studies and clinical evaluation. Clin Plast Surg. 2009;36:195–209. doi: 10.1016/j.cps.2008.11.001. [DOI] [PubMed] [Google Scholar]
- 6.Wong GR, Chen WP. Phosphatidylcholine/deoxycholate lipolysis and hyaluronic acid augmentation to enhance nonsurgical lower facial contouring using botulinum toxin type A. J Cosmet Dermatol. 2011;10:159–62. doi: 10.1111/j.1473-2165.2011.00549.x. [DOI] [PubMed] [Google Scholar]
- 7.Duncan D, Rotunda AM. Injectable therapies for localized fat loss: state of the art. Clin Plast Surg. 2011;38:489–501. doi: 10.1016/j.cps.2011.02.005. [DOI] [PubMed] [Google Scholar]
- 8.Matarasso A. Managing the Buccal Fat Pad. Aesthet Surg J. 2006;26:330–6. doi: 10.1016/j.asj.2006.03.009. [DOI] [PubMed] [Google Scholar]
- 9.Jakson IT. Buccal Fat Pad Removal. Aesthet Surg J. 2003;23:484–5. doi: 10.1016/j.asj.2003.08.005. [DOI] [PubMed] [Google Scholar]
- 10.Yaremchuk MJ, Doumit G, Thomas MA. Alloplastic augmentation of the facial skeleton: An occasional adjunct or alternative to orthognathic surgery. Plast Reconstr Surg. 2011;127:2021–30. doi: 10.1097/PRS.0b013e31820e9263. [DOI] [PubMed] [Google Scholar]
- 11.Yu CC, Chen PK, Chen YR. Botulinum toxin A for lower facial contouring: A prospective study. Aesthetic Plast Surg. 2007;31:445–51. doi: 10.1007/s00266-007-0081-8. [DOI] [PubMed] [Google Scholar]
- 12.Pitanguy I. Facial Cosmetic Surgery: A 30-Year Perspective. Plast Reconstr Surg. 2000;104:1517–26. [PubMed] [Google Scholar]
- 13.Hunstad JP, Aitken ME. Liposuction: techniques and guidelines. Clin Plast Surg. 2006;33:13–25. doi: 10.1016/j.cps.2005.09.003. [DOI] [PubMed] [Google Scholar]
- 14.Doerr TD. Lipoplasty of the face and neck. Curr Opin Otolaryngol Head Neck Surg. 2007;4:228–32. doi: 10.1097/MOO.0b013e32825b0777. [DOI] [PubMed] [Google Scholar]
- 15.Zhang HM, Yan YP, Ai K-M, Wang JQ, Liu ZF. Anatomical structure of the buccal fat pad and its clinical adaptations. Plast Reconstr Surg. 2002;109:2509–18. doi: 10.1097/00006534-200206000-00052. discussion 2519-20. [DOI] [PubMed] [Google Scholar]
- 16.Matarasso A. Buccal fat pad excision: Aesthetic improvement of the midface. Annals Plast Surg. 1991;26:413–8. doi: 10.1097/00000637-199105000-00001. [DOI] [PubMed] [Google Scholar]
- 17.Selber JC, Rosen HM. Aesthetics of facial skeletal surgery. Clin Plast Surg. 2007;34:437–45. doi: 10.1016/j.cps.2007.05.007. [DOI] [PubMed] [Google Scholar]
- 18.Rosen HM. Facial skeletal expansion: Treatment strategies and rationale. Plast Reconstr Surg. 1992;89:798–808. doi: 10.1097/00006534-199205000-00004. [DOI] [PubMed] [Google Scholar]
- 19.Kim NH, Chung JH, Park RH, Park JB. The use of botulinum toxin type A in aesthetic mandibular contouring. Plast Reconstr Surg. 2005;115:919–30. doi: 10.1097/01.prs.0000153236.79775.a0. [DOI] [PubMed] [Google Scholar]