

Abstract
Background:
Cheek dimples are usually considered as an attractive feature of facial beauty. Unfortunately, not all beautiful girls have dimples. Literature on dimple creation surgery is sparse.
Aims:
We used a new and simple technique for dimple creation, passing a transcutaneous bolster stitch after scraping off the dermis of all mucomuscular attachments. Our aim was to analyse the positive and negative findings of this technique.
Materials and Methods:
We used this procedure in creation of 100 dimples under local anaesthesia as a daycare procedure and analysed the results.
Results and Conclusion:
This procedure is safe, reliable and easily reproducible. As no tissue is excised, chances of bleeding and haematoma formation are negligible. With this procedure, the patient satisfaction rate is very high, and patients seen long time after surgery continue to be pleased with their surgically created dimples.
KEY WORDS: Anatomical basis of dimple creation, dimple creation, natural dimples
INTRODUCTION
Dimples on cheeks enhance facial beauty and expression. They occur in both sexes with no particular preponderance, may express unilaterally or bilaterally and are genetically inherited as a dominant trait.[1,2] Anatomically, dimples are thought to be caused by a double or bifid zygomaticus major muscle, whose fascial strands insert into the dermis and cause a dermal tethering effect.[3,4] There is an increasing demand for dimple creation surgery in our part of the globe. As a result, we have used this simple technique for creating cheek dimples in our patients.
MATERIALS AND METHODS
Between January 2006 and October 2010, we surgically created 100 dimples in 64 patients by the technique mentioned below. All the dimples were created under local anaesthesia on an outpatient basis. Of the 64 patients, 60 were females and 4 were males. Sixteen patients underwent unilateral dimple creation and 42 underwent bilateral dimple creation. Of the 16 unilateral dimples, 14 dimples were made on the left side and 2 on the right side of the face. All the bilateral dimples were created in females. The average age of the patients was 31 years [Table 1].
Table 1.
Dimple distribution in patients

Anatomy of the dimple
Anatomically, dimples are thought to be caused by a double or bifid zygomaticus major muscle, whose fascial strands insert into the dermis and cause a dermal tethering effect.[3,4]
Operative technique
Positioning of the dimple
Generally, the position of the dimple is marked by the patient in front of the mirror. If the patient is undecided as to the site of the dimple, another landmark described from the cosmetic viewpoint is the intersection of a perpendicular line dropped from the external canthus and a horizontal line drawn from the angle of mouth, as reported by Boo-Chai.[5] However, we feel that the position of the dimple marked by this method is too low. We consider the position of the dimple at the point of intersection of the perpendicular line dropped from the external canthus and horizontal line drawn from the highest point of the cupid's bow laterally. It has also been our observation in patients having natural dimples that if the person sucks his cheeks inside, the area of the maximum depression is the area of the dimple. Similarly, the patient is asked to create a negative suction and suck the cheeks inside. The site of the maximum depression is the marked site of the dimple.
Surgery
The aim of the surgery is to create a scar in the dermis which adheres to the underlying muscle, and becomes a natural dynamic dimple. It is performed under local anaesthesia. Around 2–3 ml of 0.5% lignocaine adrenaline solution is injected from the skin side down to the mucosal side at the marked site. A period of 10min is allowed to lapse. A small stab incision is made with a No. 15 knife, 2cm anterior (towards the lips) to the proposed site of the dimple. Due care is taken to ensure that we are away from the papilla of the stensons duct. The No.15 blade is then inserted through the small stab on the mucosal aspect, with its sharp edge facing the skin. After the blade with its sharp edge comes below the marked site of the dimple, the skin is scraped of all the mucomuscular attachments. A similar procedure is done on the mucosal side, taking care not to breach the mucosa. If a wider dimple is to be created, a wider area is scraped, so that two raw areas are created which will adhere to each other and create the dimple. Similarly, if a smaller dimple is to be created, a proportionately smaller area is scraped. After the scraping is complete, a dent is felt if palpated bimanually. If the desired depression is not created, it means that the scraping is inadequate and needs further scraping. The next step is to create and maintain the adhesion. A No. 3 ethilon on a straight needle is taken. It is inserted through the skin, brought out through the mucosa, reinserted through the mucosa and brought out through the skin and a bolster stitch is taken [Figure 1]. The advantage of the bolster is to have a better longitudinal dimple. Care is taken to keep a small piece of vaseline gauze between the skin, mucosa and the stitch. In the last few cases, we have used a silicon cylinder (block) as a bolster as it is more hygienic and does not keep moisture and food debris in the suture. Due care is also taken to prevent excessive tightening of the stitch to prevent the resulting ischaemia of the mucosa (Video 1).
Figure 1.
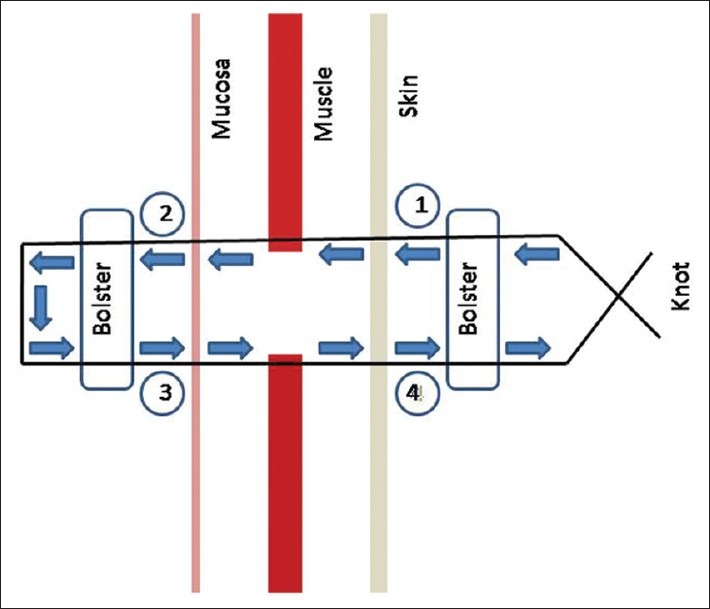
Diagrammatic representation of transcutaneous bolster stitch
Postoperative care
The patient is discharged immediately with antibiotics and analgesics. Meticulous oral hygiene with mouthwash and oral rinse is of utmost importance. The bolster stitch is removed on postoperative day 7. Initially, there is a static dimple which deepens on animation, but gradually with time there is only a hint of dimple when static and accentuates on animation. Clinical pictures are shown [Figures 2–9].
Figure 2.

Pre-op frontal view case 1
Figure 9.

Post-op case 2
Figure 3.

Pre-op lateral view case 1
Figure 4.

Post-op 2 years case 1 – Small dent visualised without animation
Figure 5.

Post-op frontal view case 1
Figure 6.

Post-op lateral view case 1
Figure 7.

Pre-op case 2
Figure 8.

Post-op case 2 at 3 years follow-up with very small dent of dimple without animation
RESULTS
The follow-up of the patients ranged from 3 weeks to 4 years. Of the 100 dimples, only 3 had intraoral infection around the bolster, probably because of too tight bolster leading to ischaemia of the mucosa and poor maintenance of oral hygiene. These were managed by removal of bolster and by antibiotic supplementation. The infection had no adverse effect on the dimple and probably accentuated the dimple because of excessive scarring. Two patients demanded reduction in the dimple size. Partial reduction of the scar was done by releasing the scar intraorally and injecting 0.5 ml of hyaluronic acid in the defect. Three patients demanded accentuation of the dimple for which a redo procedure was done. There was no incidence of haematoma, bleeding or injury to the buccal branch of the facial nerve in any of the patients. By the end of 3 months after the surgery, there was only a small hint of the dimple which was seen without animation and which accentuated on animation. With time, the small dent gradually diminished, but a definite dent was still seen on follow-up to 4 years. The patient satisfaction rate was very high, and patients seen long time after surgery continue to be pleased with their surgically created dimples. None of the patients in the series demanded a complete dimple reversal surgery.
DISCUSSION
The dimple is, from a colourless description given in the Oxford Dictionary, a small hollow especially in the cheek or chin. However, the same word in Chinese calligraphic writing is a picturesque one conveying the dramatic picture of a whirlpool with its ever present ripples.[5] The Orientals view this anatomical endowment with a good will and their women folk cherish and desire it.[5] Unfortunately, not all pretty girls have dimples. But with simple techniques, dimples can be created with much ease.
Published reports of technique of dimple creation are sparse in literature. All the techniques described essentially have the same principle to create adhesion between the underlying muscular structures and the dermis, so that traction may create a dimple due to the dermal tethering effect. All the techniques described have claimed dimple creation surgery to be a very safe procedure with good results and a very low complication rate.
In 1962, Khoo Boo Chai[5] reported his technique. He used a non-absorbable suture as a sling between skin and buccinators muscle; in effect, this simulated integumentary insertion of the muscle.
Shiwei Bao et al.[6] have used a syringe needle to guide a monofilament nylon suture through the dermis and the active facial muscles (usually the buccinators). They formed a sling between the skin and buccinators muscle. The knot is tied and dimple is created.
Thomas et al.[7] have described an open technique that replicates the anatomical basis of a natural dimple.
Saraf et al.[8] used a punch biopsy instrument and an intraoral approach to create a dimple. A circular core composed of mucosa, submucosal fat and cheek muscles is removed, sparing the skin. This creates a shallow cylindrical shaped defect under the skin. A suture is then taken through the cheek muscle on one side of the defect, then through the dermal layer of the skin and finally through the cheek muscle on the other side of the defect. The knot is then tied, resulting in dimpling of the skin.
The open techniques which necessitate excision of tissue have got a risk of bleeding during or after dimple creation surgery. There is also an increased risk of haematoma formation and infection. Though extremely uncommon, there is a potential for injury to the buccal branch of the facial nerve.
We feel that the techniques using syringe needle as a guide to create a sling by Shiwei Bao et al.[6] is cumbersome. They also recommend that patient can return to work or other activities 2 days after the operation, which we feel is a very long time for a minor procedure like dimple creation.
To adjust the dimensions of the dimple, Shiwei Bao et al. have recommended adjusting the tension on the knot and the amount of dermis tissue the injection needle sutures. This may need repeated passes and more tissue trauma to get the desired effect, especially for the beginner.
Natural dimples are longitudinal depressions of 0.5–1.5 cm. This long depression cannot be uniformly achieved by a single stitch, and further excision of mucosa and muscle is a cause of concern. The technique which we have used is very simple and easily reproducible even in the less-experienced hands. More so, it provides the anatomical basis of the dimple creation. No tissue is resected, and so there are no chances of haematoma formation or bleeding and excessive postoperative oedema. The size of the dimple is easy to control. One can easily feel and visualise the indentation before placing the suture to control the size of the dimple. The procedure is done on an outpatient basis, and the patient can immediately go to work after the procedure. One drawback of this procedure is that the bolster suture is visible on the cheek for the first 7 days after the surgery. However, considering the numerous advantages this procedure has, we feel that this is inconsequential.
CONCLUSION
We conclude that dimple creation surgery is a very safe procedure. The patient satisfaction rate is very high, and patients seen long time after surgery continue to be pleased with their surgically created dimples.
Videos available online www.ijps.org
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Argamaso RV. Facial dimple: Its formation by a simple technique. Plast Reconstr Surg. 1971;48:40–3. doi: 10.1097/00006534-197107000-00008. [DOI] [PubMed] [Google Scholar]
- 2.Pentozos Daponte A, Vienna A, Brant L, Hauser G. Cheek dimples in Greek children and adolescents. Int J Anthropol. 2004;19:289–95. [Google Scholar]
- 3.Gassner HG, Rafii A, Young A, Murakami C. Surgical anatomy of the face: Implications for modern face lift techniques. Arch Facial Plast Surg. 2008;10:9–19. doi: 10.1001/archfacial.2007.16. [DOI] [PubMed] [Google Scholar]
- 4.Pessa JE, Zadoo VP, Garza PA, Adrian EK, Jr, Devitt AI. Double or bifid zygomaticus majot muscle: Anatomy, incidence and clinical correlation. Clin Anat. 1998;11:310–3. doi: 10.1002/(SICI)1098-2353(1998)11:5<310::AID-CA3>3.0.CO;2-T. [DOI] [PubMed] [Google Scholar]
- 5.Khoo BC. The facial dimple: Clinical study and operative technique. Plast Reconstr Surg. 1962;30:281–8. doi: 10.1097/00006534-196208000-00008. [DOI] [PubMed] [Google Scholar]
- 6.Bao S, Zhou C, Li S, Zhao M. A new simple technique for making facial dimples. Aesthetic Plast Surg. 2007;31:380–3. doi: 10.1007/s00266-006-0191-8. [DOI] [PubMed] [Google Scholar]
- 7.Thomas M, Menon H, Silva JD. Improved surgical access for facial dimple creation. Aesthet Surg J. 2010;30:798–801. doi: 10.1177/1090820X10383399. [DOI] [PubMed] [Google Scholar]
- 8.Saraf S, Pillutia R. Complication of dimple creation. Indian Dermatol Online J. 2010;1:42–3. doi: 10.4103/2229-5178.73260. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.