

Abstract
AIM: To evaluate the safety and effectiveness of two-stage vs single-stage management for concomitant gallstones and common bile duct stones.
METHODS: Four databases, including PubMed, Embase, the Cochrane Central Register of Controlled Trials and the Science Citation Index up to September 2011, were searched to identify all randomized controlled trials (RCTs). Data were extracted from the studies by two independent reviewers. The primary outcomes were stone clearance from the common bile duct, postoperative morbidity and mortality. The secondary outcomes were conversion to other procedures, number of procedures per patient, length of hospital stay, total operative time, hospitalization charges, patient acceptance and quality of life scores.
RESULTS: Seven eligible RCTs [five trials (n = 621) comparing preoperative endoscopic retrograde cholangiopancreatography (ERCP)/endoscopic sphincterotomy (EST) + laparoscopic cholecystectomy (LC) with LC + laparoscopic common bile duct exploration (LCBDE); two trials (n = 166) comparing postoperative ERCP/EST + LC with LC + LCBDE], composed of 787 patients in total, were included in the final analysis. The meta-analysis detected no statistically significant difference between the two groups in stone clearance from the common bile duct [risk ratios (RR) = -0.10, 95% confidence intervals (CI): -0.24 to 0.04, P = 0.17], postoperative morbidity (RR = 0.79, 95% CI: 0.58 to 1.10, P = 0.16), mortality (RR = 2.19, 95% CI: 0.33 to 14.67, P = 0.42), conversion to other procedures (RR = 1.21, 95% CI: 0.54 to 2.70, P = 0.39), length of hospital stay (MD = 0.99, 95% CI: -1.59 to 3.57, P = 0.45), total operative time (MD = 12.14, 95% CI: -1.83 to 26.10, P = 0.09). Two-stage (LC + ERCP/EST) management clearly required more procedures per patient than single-stage (LC + LCBDE) management.
CONCLUSION: Single-stage management is equivalent to two-stage management but requires fewer procedures. However, patient’s condition, operator’s expertise and local resources should be taken into account in making treatment decisions.
Keywords: Laparoscopic cholecystectomy, Laparoscopic common bile duct exploration, Endoscopic retrograde cholangiopancreatography, Endoscopic sphincterotomy, Gallstones, Common bile duct stones, Meta-analysis
INTRODUCTION
Choledocholithiasis is concomitant with gallstones in approximately 3%-10% of the patients[1-4]. In the pre-endoscopy and pre-laparoscope era, the standard treatment for patients suffering from gallstones accompanied with common bile duct stones (CBDS) was open cholecystectomy and common bile duct exploration[5]. With the advent of laparoscopic and endoscopic techniques, several alternative treatments, such as laparoscopic cholecystectomy (LC), preoperative or postoperative endoscopic retrograde cholangiopancreatography and endoscopic sphincterotomy (ERCP + EST) and laparoscopic common bile duct exploration (LCBDE), have been developed to treat cholelithiasis. In the past two decades, LC has become gradually accepted as the first choice for the treatment of cholecystolithiasis. Consequently, confirmed or suspected cases of CBDS have been routinely removed via a two-stage management using preoperative ERCP/EST followed by LC. However, even with the strictest selection criteria, over 10% of the preoperative ERCP are normal[6,7], and only 10%-60% of patients will have stones at the time of ERCP[8-11]. As a result, a number of unnecessary ERCP procedures have been performed. To avoid these unnecessary procedures, laparoscopic intraoperative cholangiography combined with selective postoperative ERCP has been proposed[12]. Nevertheless, preoperative ERCP/EST and postoperative ERCP/EST can both result in unpredictable severe complications, even death[13]. Although ERCP/EST has been proven to be a safe and effective option for extracting CBDS in most cases, it also has some adverse effects. This procedure can not only induce several postoperative complications, including bleeding, perforation and pancreatitis[14-17], but also lead to the disruption of the intact sphincter of Oddi[18,19]. Currently, as the laparoscopic technique matures, more and more centers prefer conducting LCBDE through either the transcystic duct or via the choledochotomy to remove CBDS, thus preventing unnecessary preoperative ERCP[20-22]. Above all, LCBDE has the advantage of reducing the two-stage approach to a single-stage approach by minimally invasive surgery. Previously published trials are unclear as to whether two-stage (LC + ERCP/EST) management is better or worse than single-stage (LC + LCBDE) management for choledocholithiasis complicated with cholecystolithiasis. Therefore, we conducted a systematic review and meta-analysis of all randomized controlled trials (RCTs) to evaluate the clinical safety and effectiveness of the two-stage (LC + ERCP/EST) management vs single-stage (LC + LCBDE) management in patients with concomitant gallstones and CBDS.
MATERIALS AND METHODS
Searching strategy
We searched databases, including PubMed, Embase, the Cochrane Central Register of Controlled Trials and the Science Citation Index updated to September 2011, to identify all related published RCTs. The keywords used in the search were as follows: LC, LCBDE, ERCP, EST, gallstones and CBDS. The language of all publications was restricted to English only. The citations within the reference lists of the articles were searched manually to identify additional eligible studies.
Inclusion and exclusion criteria
All studies, published up to and including September 2011, that compared two-stage (LC + ERCP/EST) with single-stage (LC + LCBDE) management in patients with concomitant gallstones and CBDS were eligible for inclusion. The inclusion criteria were: (1) study design, RCT; (2) types of participants, those with proven or suspected CBDS before LC or those with gallstones that were found to have CBDS at LC by intraoperative cholangiography; (3) intervention, preoperative ERCP/EST + LC vs LC + LCBDE or (4) postoperative ERCP/EST + LC vs LC + LCBDE. Non-randomized trials, retrospective analyses and reviews were not included, and studies were excluded if there were no postoperative major outcomes. In addition, those studies comparing intraoperative ERCP/EST + LC with LC + LCBDE were also excluded because both managements were single-stage.
Data extraction and validity assessment
Two authors (Lu J and Cheng Y) independently extracted the data, evaluated the study quality by applying a predesigned standardized form, and then cross-checked. Any disagreement in the two reviewers’ data collection and quality assessment was discussed until a consensus was reached; otherwise, a third reviewer (Xiong XZ) would take part in the discussion as the referee. The general information extracted from the studies included the authors, publication year, study period, country, characteristics of patients, sample size, interventions and outcomes. The risk of bias in the included studies was assessed using the Cochrane collaboration’ tool. The assessment contained six dimensions: (1) random sequence generation; (2) allocation concealment; (3) blinding; (4) incomplete outcome data addressed; (5) selective reporting; and (6) other bias.
Outcomes of interest and definitions
The primary outcomes were stone clearance from the common bile duct (CBD), postoperative morbidity and mortality, while secondary outcomes were conversion to other procedures, length of hospital stay, number of procedures used per patient, total operative time, hospitalization charges, patient acceptance and quality of life scores. Stone clearance from the CBD was determined by ERCP or intraoperative cholangiography, and it was defined as successful stones extracted from the CBD via the planned procedure only once. The overall postoperative morbidity consisted of surgical and nonsurgical complications. The surgical complications included hemorrhage, bile leak, acute pancreatitis, cholangitis, perforation, wound infection, abdominal and wall hematoma that were directly related with the operation, and the nonsurgical complications included myocardial infarction and pulmonary embolism, which had nothing to do with the operation. Mortality was defined as postoperative death before discharge or within 30 postoperative days. Conversion to other procedures was defined as any case in which stones from the CBD were not successfully extracted or other scenarios, such as dense gallbladder adhesions and fibrosis, which resulted in converting the planned procedure into another procedure.
Statistical analysis
All statistical analyses of the extracted data was performed with Review Manager (Review Manager version 5.1, Copenhagen, the Nordic Cochrane Centre, the Cochrane Collaboration, 2008). The results of the meta-analysis were expressed as the risk ratios (RRs) and mean difference (MD) for dichotomous data and continuous data, respectively, with 95% confidence intervals (CIs) for both. The Mantel-Haenzsel method was used for dichotomous variables, while the inverse variance method was used for continuous variables. P values were computed with the Z test, and P < 0.05 was regarded as statistically significant. The heterogeneity among the studies was evaluated using the χ2 test, with its significance set at P < 0.1, and the extent of inconsistency was assessed by the I2 statistic[23]. If significant heterogeneity existed, a random-effect model was used to attempt to explain it. In the absence of significant heterogeneity, a fixed-effect model was adopted. Generally, the estimates of the mean and SD were required to calculate the CIs for continuous data. However, a few published clinical trials reported a median and a range instead of a mean and SD. To adjust for this difference, we assumed that the median was equal to the mean, and we estimated the SD as a quarter of the reported range. Potential publication bias was appraised visually by funnel plots.
RESULTS
Literature search and selection
The literature search identified 792 potentially relevant studies according to our predefined search strategy (Figure 1). Ninety-three studies were removed by the Endnote X4 software, and 667 studies were excluded through scanning titles and abstracts. Full-text papers were retrieved for the remaining 32 eligible studies. Of the remaining 32 studies, 20 studies were excluded because they were non-randomized trials. Three studies were excluded because they were duplicated trials, and two were not included because they compared intraoperative ERCP/EST + LC with LC + LCBDE. Eventually, seven RCTs[5,24-29] were considered to be suitable for the final meta-analysis. There were five trials[4,24,26,28,29] (n = 621) comparing preoperative ERCP/EST + LC with LC + LCBDE and two trials[25,27] (n = 166) comparing postoperative ERCP/EST + LC with LC + LCBDE. The characteristics, outcomes and risk of bias for the included studies are summarized in Tables 123. A manual search and examination of the bibliographies in these reference lists were also performed, and no additional eligible studies were found.
Figure 1.
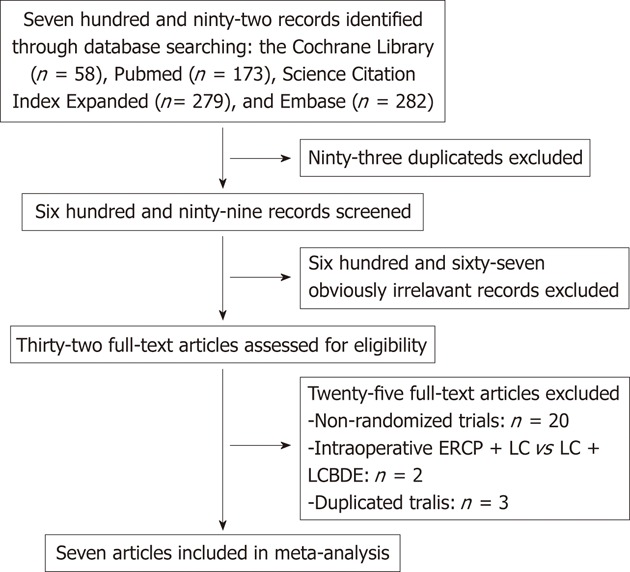
Flow diagram of literature screening. ERCP: Endoscopic retrograde cholangiopancreatography; LC: Laparoscopic cholecystectomy; LCBDE: Laparoscopic common bile duct exploration.
Table 1.
Characteristics of 7 included randomized controlled trials
| Included studies | Country | Study period | Sample size | Comparison | Measured outcomes |
| Bansal et al[5], 2010 | India | 2007-2008 | 30 | Preoperative ERCP/EST + LC (n = 15) vs LC + LCBDE (n = 15) | Successful removal of gallbladder and CBD clearance, complications |
| Rogers et al[24], 2010 | United States | 1997-2003 | 122 | Preoperative ERCP/EST + LC (n = 61) vs LC + LCBDE (n = 61) | Stone clearance from CBD, length of hospital stay, cost of index hospitalization, hospital charges, professional fees, patient acceptance, morbidity, mortality, quality of life scores |
| Rhodes et al[25], 1998 | United Kingdom | 1995-1997 | 80 | Postoperative ERCP/EST + LC (n = 40) vs LC + LCBDE (n = 40) | Duct-clearance rates, morbidity, operating time and hospital stay |
| Cuschieri et al[26], 1999 | Scotland | 1994-1997 | 300 | Preoperative ERCP/EST + LC (n = 150) vs LC + LCBDE (n = 150) | Hospital stay, success rates, conversion rates, morbidity and mortality |
| Nathanson et al[27], 2005 | Australia | 1998-2003 | 86 | Postoperative ERCP/EST + LC (n = 45) vs LC + LCBDE (n = 41) | Operative time, morbidity, retained stone rate, reoperation rate and hospital stay |
| Sgourakis et al[28], 2002 | Greece | 1997-2000 | 78 | Preoperative ERCP/EST + LC (n = 42) vs LC + LCBDE (n = 36) | Stone clearance, morbidity, mortality, conversion, hospital stay, complications |
| Noble et al[29], 2009 | United Kingdom | 2000-2006 | 91 | Preoperative ERCP/EST + LC (n = 47) vs LC + LCBDE (n = 44) | Duct clearance, complications, number of procedures per patient, conversion and hospital stay |
RCTs: Randomized controlled trial; CBD: Common bile duct; LC: Laparoscopic cholecystectomy; ERCP: Endoscopic retrograde cholangiopancreatography; EST: Endoscopic sphincterotomy; LCBDE: Laparoscopic common bile duct exploration.
Table 2.
Outcomes of 7 included randomized controlled trials (endoscopic retrograde cholangiopancreatography/endoscopic sphincterotomy + laparoscopic cholecystectomy) vs (laparoscopic cholecystectomy+ laparoscopic common bile duct exploration)
| Included studies | Stone clearance from the CBD (%) | Postoperative morbidity (%) | Mortality (%) | Conversion to other procedures (%) | Number of procedures per patient | Length of hospital stay (d) | Total operating time (min) (SD or range) | Hospitalization charges ($) (SD or range) |
| Bansal et al[5], 2010 | 86.7 vs 93.3 | Not mentioned | 0 vs 0 | 15.4 vs 6.7 | Not mentioned | 4 (2-11) vs 4.2 (3-9) | 153 (120-240) vs ? | Not mentioned |
| Rogers et al[24], 2010 | 96.8 vs 88.2 | 9.1 vs 10.5 | 0 vs 0 | 1.8 vs 3.5 | 2.0 vs 1.0 | 4.1 (3.5) vs 2.3 (1.9) | 183 (39) vs 174 (67) | 30 617 (16 384) vs 27 675 (11 256) |
| Rhodes et al[25], 1998 | 75 vs 75 | 15 vs 17.5 | Not mentioned | 0 vs 25 | 2.4 vs 1.3 | 3.5 (1-11) vs 1 (1-26) | 105 (60-255) vs 90 (25-310) | Not mentioned |
| Cuschieri et al[26], 1999 | 83.7 vs 82.6 | 12.5 vs 15.8 | 1.5 vs 0.8 | 14.7 vs 15 | 2.0 vs 1.2 | 9 (5.5-14) vs 6 (4.2-12) | Not mentioned | Not mentioned |
| Nathanson et al[27], 2005 | 71.1 vs 97.6 | 13.3 vs 17.1 | 0 vs 0 | 6.7 vs 4.9 | 2.3 vs 1.2 | 7.7 vs 6.4 | 147.9 vs 158.8 | Not mentioned |
| Sgourakis et al[28], 2002 | 84.3 vs 85.7 | 18.8 vs 17.9 | 3.1 vs 0 | 15.6 vs 14.3 | 2.1 vs 1.1 | 9 vs 7.4 | 105 (60-255) vs 90 (70-310) | Not mentioned |
| Noble et al[29], 2009 | 55.6 vs 100 | 29.8 vs 43.2 | Not mentioned | 42.6 vs 9.1 | 2.3 vs 1.0 | 3 (2-7) vs 5 (2-7) | Not mentioned | Not mentioned |
CBD: Common bile duct.
Table 3.
Cochrane risk of bias summary
| Included studies | Random sequence generation | Allocation concealment | Blinding of participants and personnel | Blinding of outcome assessment | Incomplete outcome data | Selective reporting | Other bias |
| Bansal et al[5], 2010 | Low risk | Low risk | High risk | Unclear risk | High risk | High risk | Unclear risk |
| Rogers et al[24], 2010 | Low risk | Low risk | High risk | Unclear risk | High risk | Low risk | Low risk |
| Rhodes et al[25], 1998 | Unclear risk | Unclear risk | High risk | Unclear risk | Low risk | High risk | Unclear risk |
| Cuschieri et al[26], 1999 | Low risk | Unclear risk | High risk | Unclear risk | Low risk | High risk | Unclear risk |
| Nathanson et al[27], 2005 | Low risk | Low risk | High risk | Unclear risk | Low risk | High risk | Unclear risk |
| Sgourakis et al[28], 2002 | High risk | Unclear risk | High risk | Unclear risk | High risk | High risk | Low risk |
| Noble et al[29], 2009 | Low risk | Unclear risk | High risk | Unclear risk | Low risk | High risk | Low risk |
Description of various RCTs including inclusion and exclusion criteria
All of the patients were proven or suspected of having gallstones and CBDS on the basis of clinical presentation (jaundice, biliary pancreatitis and cholangitis) or liver function tests or imaging (ultrasound, magnetic resonance cholangiopancreatography (MRCP) and intraoperative cholangiography) before being enrolled in the trial. Three trials[24,26,28] restricted the participants to the ASA risk grade at the level of I and II. In addition, one trial[29] was specially designed to compare the two-stage (ERCP/EST + LC) approach with the single-stage (LC + LCBDE) approach in higher risk patients, who were defined as those over 60 years of age with comorbidity, those over 70 years of age, or those over 50 years of age with a body mass index exceeding 40. Three trials[5,26,28] did not mention their exclusion criteria. Additionally, three studies[25,27,29] excluded patients who had accepted previous ERCP/EST prior to recruitment into the trials. Patients with severe pancreatitis and cholangitis, which required emergency ERCP/EST, were also excluded from two trials[27,29].
Publication bias
A funnel plot analysis was performed by adopting the occurrence of stone clearance from the CBD as the index, and it appeared to be asymmetrical, which suggested the presence of publication bias (Figure 2).
Figure 2.
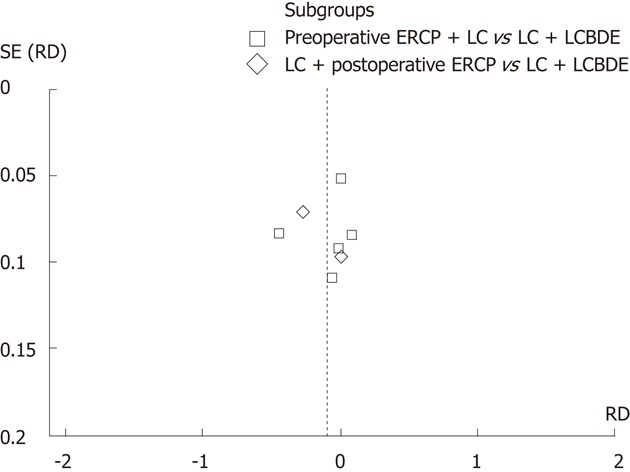
Funnel plot of trials of stone clearance from the common bile duct. ERCP: Endoscopic retrograde cholangiopancreatography; LC: Laparoscopic cholecystectomy; LCBDE: Laparoscopic common bile duct exploration. SE: Standard error; RD: Risk difference.
Meta-analysis results
Stone clearance from the CBD: Stone clearance from the CBD was achieved in 78.8% (234 of 297) of patients in the two-stage (ERCP/EST + LC) group and in 87.2% (251 of 288) of patients in the single-stage (LC + LCBDE) group. The meta-analysis revealed that the difference between the two groups was not statistically significant (RR = -0.10, 95% CI: -0.24 to 0.04, P = 0.17), and there was statistically significant heterogeneity among the studies (χ2 = 33.55, P < 0.00 001, I2 = 82%) (Figure 3A).
Figure 3.
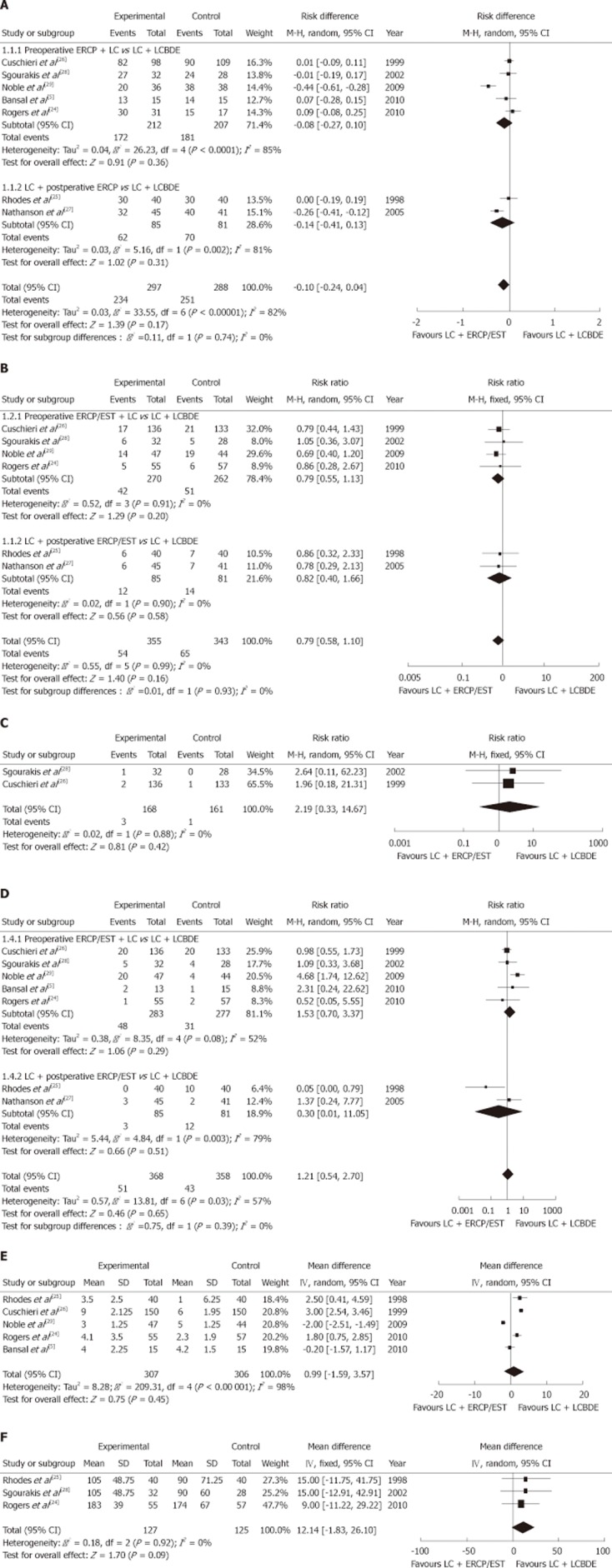
Forest plot of meta-analysis. A: Two-stage [endoscopic retrograde cholangiopancreatography (ERCP)/endoscopic sphincterotomy (EST) + laparoscopic cholecystectomy (LC)] vs single-stage [LC + laparoscopic common bile duct exploration (LCBDE)] in stone clearance from the common bile duct; B: Two-stage (ERCP/EST + LC) vs single-stage (LC + LCBDE) in postoperative morbidity; C: Two-stage (ERCP/EST + LC) vs single-stage (LC + LCBDE) in mortality; D: Two-stage (ERCP/EST + LC) vs single-stage (LC + LCBDE) in conversion to other procedures; E: Two-stage (ERCP/EST + LC) vs single-stage (LC + LCBDE) in length of hospital stay; F: Two-stage (ERCP/EST + LC) vs single-stage (LC + LCBDE) in total operating time. CI: Confidence interval.
Postoperative morbidity: Postoperative morbidity was reported in six trials[24-29]. Overall, postoperative morbidity occurred in 15.2% (54 of 355) of patients in the two-stage (ERCP/EST + LC) group vs 19.0% (65 of 343) of patients in the single-stage (LC + LCBDE) group. The meta-analysis demonstrated that there was no statistically significant difference between the two groups (RR = 0.79, 95% CI: 0.58 to 1.10, P = 0.16). As evidenced by the values of the χ2 and I2 indices (χ2 = 0.55, P = 0.99, I2 = 0%), no significant heterogeneity was found from the trials (Figure 3B).
Mortality: Five trials[5,24,26-28] reported mortality; however, only two of these trials[26,28] reported postoperative deaths. The results of the pooled analysis revealed no statistically significant difference between the two groups (RR = 2.19, 95% CI: 0.33 to 14.67, P = 0.42); and there was no significant heterogeneity between the trials (χ2 = 0.02, P = 0.88, I2 = 0%) (Figure 3C).
Conversion to other procedures: We identified all the trials existing in the data, and the occurrence of conversion was 13.9% (51 of 368) and 12.0% (43 of 358) in the two-stage (ERCP/EST + LC) group and the single-stage (LC + LCBDE) group, respectively. Significant heterogeneity was present in the trials (χ2 = 13.83, P = 0.03, I2 = 57%), and there was no statistically significant difference between the two groups (RR = 1.21, 95% CI: 0.54 to 2.70, P = 0.39) (Figure 3D).
Length of hospital stay: The length of hospital stay was evaluated in all the studies, but only one study[24] reported this data in the form of the mean and the SD. There were two studies[27,28] that provided the mean without the SD, and the rest of studies[5,25,26,29] provided the median and the range. Consequently, according to our predefined plan, we presumed that the median was equal to the mean, and we equated the SD with a quarter of the reported range. Significant heterogeneity was found among the trials (χ2 = 209.70, P < 0.001, I2 = 98%), and the meta-analysis indicated no statistically significant difference between the two groups (MD = 0.99, 95% CI: -1.59 to 3.57, P = 0.45) (Figure 3E).
Total operative time: There were five trials[5,24,25,27,28] that included information about the total operative time; however, only one trial[24] reported the mean and the SD. Two trials[25,28] offered the median and the range instead of the mean and the SD, while one trial[27] offered the mean without the SD. Furthermore, there was one trial[5] that reported the total operative time of the two-stage (ERCP/EST + LC) group, but not the single-stage (LC + LCBDE) group. There was no statistically significant difference between the two groups (MD = 12.14, 95% CI: -1.83 to 26.10, P = 0.09), and no significant heterogeneity was found among the trials (χ2 = 0.18, P = 0.92, I2 = 0%) (Figure 3F).
Hospitalization charges: The hospitalization charges were recorded in only one trial. Rogers et al[24] stated that there was no statistically significant difference in total hospitalization charges between the two groups.
Patient acceptance and quality of life scores: Only one trial[24] reported the patient acceptance and quality of life scores. This article mentioned that the patient acceptance and quality of life scores were the same in both groups using standardized scoring system. However, the study did not provide specific data.
Number of procedures used per patient: It was obvious that the two-stage (LC + ERCP/EST) approach required more procedures per patient than the single-stage (LC + LCBDE) approach (Table 2).
Subgroup analysis: Because there were two options (preoperative ERCP/EST + LC and postoperative ERCP/EST + LC) for the two-stage (ERCP/EST + LC) management technique, which may have influenced the eventual conclusion, we performed a subgroup analysis for three outcomes (stone clearance from the CBD, postoperative morbidity and conversion to other procedures). In the subgroup analysis, the outcomes were also equivalent, and no statistically significant difference was found among the subgroups.
DISCUSSION
In summary, our meta-analysis revealed that both single-stage (LC + LCBDE) and two-stage (LC + ERCP/EST) management achieved equivalent stone clearance from the CBD, but the former procedure was associated with fewer procedures per patient. In addition, there was no statistically difference between the two approaches in terms of postoperative morbidity, mortality, conversion to other procedures, length of hospital stay, total operative time and hospitalization charges.
Currently, the optimal treatment for concomitant gallstones and CBDS is still in dispute[24,30,31]. In the laparoscopic era, the vast majority of patients who suffered from concomitant gallstones and CBDS were routinely managed by ERCP/EST, either preoperatively or postoperatively, prior to LC[25,26]. Although this approach is effective and safe for removing the CBDS, it also has several drawbacks. First, it requires two periods of anesthesia and occasionally two hospital admissions, which may increase the length of hospital stay and hospitalization expenses. Furthermore, if patients still have CBDS detected by intraoperative cholangiography in LC after successful ERCP/EST, surgeons will face the dilemma of depending on LCBDE, postoperative ERCP/EST or traditional open choledochotomy. Most importantly, even in those patients with clinical, biochemical and imaging risk factors for CBDS, preoperative ERCP/EST can produce false-negative results, leading to the possibility of morbidity and mortality[26,32]. Despite postoperative ERCP/EST can indeed avoid the risk inherent in preoperative ERCP/EST to patients without CBDS, it necessitates another surgical procedure when it fails to remove the CBDS[27]. Both preoperative and postoperative ERCP/EST are likely to lead to some short-term and long-term complications. For instance, they may result in postoperative complications, including bleeding, perforation, pancreatitis and even death[14-17]. Moreover, it is notable that the intact sphincter of Oddi is destroyed after EST so that biliary sphincter function is permanently lost, which damages the barrier of the sphincter that prevents duodenobiliary reflux[33]. Reflux from the duodenum into the bile duct is responsible for the high rate of bacterobilia occurring after EST[34], and chronic bacterobilia may even cause neoplastic changes in the biliary epithelium[35]. Therefore, ERCP/EST should be adopted on a selective basis, i.e., in patients with acute obstructive suppurative cholangitis, severe biliary pancreatitis, ampullary stone impaction or severe comorbidity. If possible, MRCP should be used for preoperative diagnosis. According to a meta-analysis, MRCP achieved a high overall sensitivity of 95% and a specificity of 97% for detecting CBDS[36].
With the improvement in laparoscopic equipment and skills, LCBDE has been increasingly used to remove the CBDS. It is considered to be a safe, efficient and cost-effective treatment for choledocholithiasis; it is associated with a high stone clearance rate ranging from 84%-97%, a postoperative morbidity rate of 4%-16%, and a mortality rate of approximately 0%-0.8%[26,37-39]. However, to decompress the bile duct and decrease biliary complications, T-tube drainage has been routinely employed after choledochotomy[40,41], which is inevitable with complications including bile leakage, bile infection and wound infection[41]. Furthermore, the patients have to keep the bile drainage tube in place for several weeks before removal, causing great discomfort and delaying their return to work[42].
Nevertheless, according to a recent meta-analysis[43], primary closure might be as effective as T-tube drainage in the prevention of postoperative complications after choledochotomy. Consequently, it seems that LCBDE is a commendable alternative to the use of ERCP/EST.
Previously published trials have demonstrated that single-stage (LC + LCBDE) and two-stage (LC + ERCP/EST) management are equivalent with respect to stone clearance from the CBD, morbidity and mortality[5,24-26]. However, most of the trials were limited by their small sample size. In 2006, Clayton et al[44] reported a meta-analysis concerning endoscopy and surgery vs surgery alone for CBDS with the gallbladder in situ. In the subgroup analysis, they concluded that the endoscopic and laparoscopic surgery groups had similar outcomes; however, treatment should depend on local resources and expertise. Furthermore, the number of patients included was insufficient, and up-to-date trials were not included. Unlike previous studies, this meta-analysis took patients’ characteristics into consideration and gave suggestions for the optimum management of different patients.
Concerning stone clearance from the CBD, this meta-analysis demonstrated that single-stage (LC + LCBDE) management was as effective as two-stage (LC + ERCP/EST) management (P = 0.17), but one trial[29] was more strongly in favor of the single-stage (LC + LCBDE) management than any other included studies. One possible reason was that they abandoned ERCP/EST at an earlier stage when they detected multiple and large stones in the CBD, and they favored a transductal approach if the bile duct diameter was large or if the stones were large and multiple. Another reason might be the use of intention-to-treat analysis. Our meta-analysis showed that the difference in the length of hospital stay between the two groups was not statistically significant (P = 0.45). Two of the included trials reported that the length of hospital stay was shorter for the single-stage (LC + LCBDE) approach with a statistically significant difference compared with the two-stage (LC + ERCP/EST) management[24,25]. Other studies showed that there was no significant difference between the two groups, but a recent review suggested that single-stage management had the potential merit of a shorter hospital stay[45]. One probable reason was that the definitions of hospital stay varied, which had an impact on the validity of the data. Some trials defined it as the duration from the last finished procedure to discharge, while other trials defined it as the entire duration from hospital admission to discharge. Another explanation for the discrepancy in the studies might be the use of data conversions to produce estimates. In our meta-analysis, only one trial reported hospitalization charges, and there was no significant difference in total hospitalization charges and hospital service charges between the two groups. However, the charges for single-stage (LC + LCBDE) management were lower than those for two-stage (LC + ERCP/EST) management[24]. Other studies[46,47] showed that single-stage management is a cost-effective method compared to two-stage management.
The postoperative morbidity, mortality and total operating time were similar between the two-stage (LC + ERCP/EST) and single-stage (LC + LCBDE) management with no statistically significant difference in this meta-analysis (P = 0.16, P = 0.42 and P = 0.09, respectively). When considering preoperative ERCP/EST + LC vs LC + LCBDE and postoperative ERCP/EST + LC vs LC + LCBDE separately in the subgroup analysis, the outcomes, as stated, remained consistent.
This meta-analysis was subject to some limitations. First, the funnel plot analysis detected publication bias, which results in over-representation of significant or positive studies. However, the random effects model was utilized for this analysis, and this model is known to enlarge the presence of publication bias by attributing heavier weighting to smaller trials compared to the fixed effects models. Second, the different methodological quality and the heterogeneity of the effect after intervention could also account for the asymmetry in the funnel plot. A second potential limitation was the presence of significant heterogeneity for three outcomes, including stone clearance from the CBD, conversion to other procedures and length of hospital stay, which might influence the reliability and validity of the conclusions to some extent. Finally, the restriction of only including studies published in English was another possible limitation.
For future research studies on this topic, the following suggestions may be helpful (1) hospitalization expenses data were available in only one included trial, which was far from sufficient, and future studies should evaluate this significant endpoint; (2) follow-up was poorly reported in most of the included trials, and long-term outcomes, which largely rely on the follow-up, are as yet unknown. Future trials should strengthen the work of follow-up; (3) future studies need to assess outcomes such as pain scores, health economics, patients satisfaction and quality of life scores because it is more practical for patients to choose their optimal treatment; (4) blinded outcome assessment should be employed in future trials to better reduce bias; and (5) as a result of the different data types provided by the included trials, the outcomes, including the length of hospital stay and total operative time were weakened. Thus, future researchers should use unified data types.
In conclusion, single-stage (LC + LCBDE) management is not only as effective as two-stage (LC + ERCP/EST) management and equivalent in terms of postoperative morbidity, mortality and conversion, but it also reduces the number of procedures used per patient and potentially shortens the length of hospital stay. In addition, single-stage (LC + LCBDE) management also eliminates the underlying risk of ERCP/EST and keeps the sphincter of Oddi intact. It is likely that as laparoscopic expertise and operators’ experience improve, the need for two-stage (LC + ERCP/EST) management will decrease, and single-stage (LC + LCBDE) management should be ultimately available for most patients. However, the optimal management of patients with CBDS should depend on the condition of patients, the expertise of operators and local resources.
ACKNOWLEDGMENTS
We would like to acknowledge the support of the Department of Bile Duct Surgery, West China Hospital, Sichuan University, China.
COMMENTS
Background
Patients with concomitant gallstones and common bile duct stones (CBDS) are very common, but surgeons and patients are often faced with difficulties in making treatment decisions when choosing the optimal treatment. Previously published trials were inconclusive as to whether two-stage [laparoscopic cholecystectomy (LC) + preoperative endoscopic retrograde cholangiopancreatography (ERCP)/endoscopic sphincterotomy (EST)] management is better or worse than single-stage [LC + laparoscopic common bile duct exploration (LCBDE)] management. The authors in this study conducted a systematic review and meta-analysis to provide the current best evidence for the management of patients with concomitant gallstones and CBDS.
Research frontiers
Both two-stage (LC + ERCP/EST) and single-stage (LC + LCBDE) management are used for the patients with concomitant gallstones and CBDS. Two-stage (LC + ERCP/EST) management has become very popular in recent years, because it is considered to be safe and effective that can reduce the number of procedures used per patient.
Innovations and breakthroughs
This systematic review and meta-analysis summarized all available randomized controlled trials (RCTs) comparing the two techniques. The authors found that single-stage (LC + LCBDE) management was as effective as two-stage (LC + ERCP/EST) management and required fewer procedures used per patient.
Applications
Single-stage (LC + LCBDE) management is proven to be a safe and effective treatment compared with two-stage (LC + ERCP/EST) management, and it should be recommended for patients with concomitant gallstones and CBDS.
Terminology
ERCP: a technique that combines the use of endoscopy and fluoroscopy to diagnose and treat certain problems of the biliary or pancreatic ductal systems; EST: a minimally invasive surgery that was developed on the basis of ERCP to treat biliary or pancreatic ductal disease; LC: a technique that removes the gallbladder through small punctures in the abdomen to permit the insertion of a laparoscope and surgical instruments; LCBDE: a technique that combines the use of laparoscopy and choledochoscopy to treat biliary tract disease, especially CBDS.
Peer review
This is a good descriptive study in which authors evaluate the safety and effectiveness of two-stage vs single-stage management for concomitant gallstones and CBDS. The results are interesting and suggest that two-stage (LC + ERCP/EST) management clearly required more procedures per patient than single-stage (LC + LCBDE) management.
Footnotes
Peer reviewer: Thilo Hackert, MD, Department of Surgery, University of Heidelberg, Im Neuenheimer Feld 110, 69120 Heidelberg, Germany
S- Editor Gou SX L- Editor Ma JY E- Editor Xiong L
References
- 1.Collins C, Maguire D, Ireland A, Fitzgerald E, O’Sullivan GC. A prospective study of common bile duct calculi in patients undergoing laparoscopic cholecystectomy: natural history of choledocholithiasis revisited. Ann Surg. 2004;239:28–33. doi: 10.1097/01.sla.0000103069.00170.9c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hemli JM, Arnot RS, Ashworth JJ, Curtin AM, Simon RA, Townend DM. Feasibility of laparoscopic common bile duct exploration in a rural centre. ANZ J Surg. 2004;74:979–982. doi: 10.1111/j.1445-1433.2004.03216.x. [DOI] [PubMed] [Google Scholar]
- 3.Petelin JB. Laparoscopic common bile duct exploration. Surg Endosc. 2003;17:1705–1715. doi: 10.1007/s00464-002-8917-4. [DOI] [PubMed] [Google Scholar]
- 4.Fiore NF, Ledniczky G, Wiebke EA, Broadie TA, Pruitt AL, Goulet RJ, Grosfeld JL, Canal DF. An analysis of perioperative cholangiography in one thousand laparoscopic cholecystectomies. Surgery. 1997;122:817–821; discussion 821-823. doi: 10.1016/s0039-6060(97)90092-1. [DOI] [PubMed] [Google Scholar]
- 5.Bansal VK, Misra MC, Garg P, Prabhu M. A prospective randomized trial comparing two-stage versus single-stage management of patients with gallstone disease and common bile duct stones. Surg Endosc. 2010;24:1986–1989. doi: 10.1007/s00464-010-0891-7. [DOI] [PubMed] [Google Scholar]
- 6.Erickson RA, Carlson B. The role of endoscopic retrograde cholangiopancreatography in patients with laparoscopic cholecystectomies. Gastroenterology. 1995;109:252–263. doi: 10.1016/0016-5085(95)90292-9. [DOI] [PubMed] [Google Scholar]
- 7.Enochsson L, Lindberg B, Swahn F, Arnelo U. Intraoperative endoscopic retrograde cholangiopancreatography (ERCP) to remove common bile duct stones during routine laparoscopic cholecystectomy does not prolong hospitalization: a 2-year experience. Surg Endosc. 2004;18:367–371. doi: 10.1007/s00464-003-9021-0. [DOI] [PubMed] [Google Scholar]
- 8.Coppola R, Riccioni ME, Ciletti S, Cosentino L, Ripetti V, Magistrelli P, Picciocchi A. Selective use of endoscopic retrograde cholangiopancreatography to facilitate laparoscopic cholecystectomy without cholangiography. A review of 1139 consecutive cases. Surg Endosc. 2001;15:1213–1216. doi: 10.1007/s004640080019. [DOI] [PubMed] [Google Scholar]
- 9.Williams GL, Vellacott KD. Selective operative cholangiography and Perioperative endoscopic retrograde cholangiopancreatography (ERCP) during laparoscopic cholecystectomy: a viable option for choledocholithiasis. Surg Endosc. 2002;16:465–467. doi: 10.1007/s00464-001-9051-4. [DOI] [PubMed] [Google Scholar]
- 10.Barr LL, Frame BC, Coulanjon A. Proposed criteria for preoperative endoscopic retrograde cholangiography in candidates for laparoscopic cholecystectomy. Surg Endosc. 1999;13:778–781. doi: 10.1007/s004649901097. [DOI] [PubMed] [Google Scholar]
- 11.Bergamaschi R, Tuech JJ, Braconier L, Walsøe HK, Mårvik R, Boyet J, Arnaud JP. Selective endoscopic retrograde cholangiography prior to laparoscopic cholecystectomy for gallstones. Am J Surg. 1999;178:46–49. doi: 10.1016/s0002-9610(99)00110-5. [DOI] [PubMed] [Google Scholar]
- 12.Chang L, Lo S, Stabile BE, Lewis RJ, Toosie K, de Virgilio C. Preoperative versus postoperative endoscopic retrograde cholangiopancreatography in mild to moderate gallstone pancreatitis: a prospective randomized trial. Ann Surg. 2000;231:82–87. doi: 10.1097/00000658-200001000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Vandervoort J, Soetikno RM, Tham TC, Wong RC, Ferrari AP, Montes H, Roston AD, Slivka A, Lichtenstein DR, Ruymann FW, et al. Risk factors for complications after performance of ERCP. Gastrointest Endosc. 2002;56:652–656. doi: 10.1067/mge.2002.129086. [DOI] [PubMed] [Google Scholar]
- 14.Wang P, Li ZS, Liu F, Ren X, Lu NH, Fan ZN, Huang Q, Zhang X, He LP, Sun WS, et al. Risk factors for ERCP-related complications: a prospective multicenter study. Am J Gastroenterol. 2009;104:31–40. doi: 10.1038/ajg.2008.5. [DOI] [PubMed] [Google Scholar]
- 15.Andriulli A, Loperfido S, Napolitano G, Niro G, Valvano MR, Spirito F, Pilotto A, Forlano R. Incidence rates of post-ERCP complications: a systematic survey of prospective studies. Am J Gastroenterol. 2007;102:1781–1788. doi: 10.1111/j.1572-0241.2007.01279.x. [DOI] [PubMed] [Google Scholar]
- 16.Suissa A, Yassin K, Lavy A, Lachter J, Chermech I, Karban A, Tamir A, Eliakim R. Outcome and early complications of ERCP: a prospective single center study. Hepatogastroenterology. 2005;52:352–355. [PubMed] [Google Scholar]
- 17.Masci E, Toti G, Mariani A, Curioni S, Lomazzi A, Dinelli M, Minoli G, Crosta C, Comin U, Fertitta A, et al. Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol. 2001;96:417–423. doi: 10.1111/j.1572-0241.2001.03594.x. [DOI] [PubMed] [Google Scholar]
- 18.Freeman ML. Complications of endoscopic sphincterotomy. Endoscopy. 1998;30:A216–A220. doi: 10.1055/s-2007-1001443. [DOI] [PubMed] [Google Scholar]
- 19.Frimberger E. Long-term sequelae of endoscopic papillotomy. Endoscopy. 1998;30:A221–A227. doi: 10.1055/s-2007-1001444. [DOI] [PubMed] [Google Scholar]
- 20.Berthou JC, Drouard F, Charbonneau P, Moussalier K. Evaluation of laparoscopic management of common bile duct stones in 220 patients. Surg Endosc. 1998;12:16–22. doi: 10.1007/s004649900585. [DOI] [PubMed] [Google Scholar]
- 21.Carroll BJ, Phillips EH, Chandra M, Fallas M. Laparoscopic transcystic duct balloon dilatation of the sphincter of Oddi. Surg Endosc. 1993;7:514–517. doi: 10.1007/BF00316692. [DOI] [PubMed] [Google Scholar]
- 22.Gigot JF, Navez B, Etienne J, Cambier E, Jadoul P, Guiot P, Kestens PJ. A stratified intraoperative surgical strategy is mandatory during laparoscopic common bile duct exploration for common bile duct stones. Lessons and limits from an initial experience of 92 patients. Surg Endosc. 1997;11:722–728. doi: 10.1007/s004649900436. [DOI] [PubMed] [Google Scholar]
- 23.Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1. The Cochrane Collaboration. 2008. Available from: http://www. cochrane-handbook. org. [Google Scholar]
- 24.Rogers SJ, Cello JP, Horn JK, Siperstein AE, Schecter WP, Campbell AR, Mackersie RC, Rodas A, Kreuwel HT, Harris HW. Prospective randomized trial of LC+LCBDE vs ERCP/S+LC for common bile duct stone disease. Arch Surg. 2010;145:28–33. doi: 10.1001/archsurg.2009.226. [DOI] [PubMed] [Google Scholar]
- 25.Rhodes M, Sussman L, Cohen L, Lewis MP. Randomised trial of laparoscopic exploration of common bile duct versus postoperative endoscopic retrograde cholangiography for common bile duct stones. Lancet. 1998;351:159–161. doi: 10.1016/s0140-6736(97)09175-7. [DOI] [PubMed] [Google Scholar]
- 26.Cuschieri A, Lezoche E, Morino M, Croce E, Lacy A, Toouli J, Faggioni A, Ribeiro VM, Jakimowicz J, Visa J, et al. E.A.E.S. multicenter prospective randomized trial comparing two-stage vs single-stage management of patients with gallstone disease and ductal calculi. Surg Endosc. 1999;13:952–957. doi: 10.1007/s004649901145. [DOI] [PubMed] [Google Scholar]
- 27.Nathanson LK, O’Rourke NA, Martin IJ, Fielding GA, Cowen AE, Roberts RK, Kendall BJ, Kerlin P, Devereux BM. Postoperative ERCP versus laparoscopic choledochotomy for clearance of selected bile duct calculi: a randomized trial. Ann Surg. 2005;242:188–192. doi: 10.1097/01.sla.0000171035.57236.d7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sgourakis G, Karaliotas K. Laparoscopic common bile duct exploration and cholecystectomy versus endoscopic stone extraction and laparoscopic cholecystectomy for choledocholithiasis. A prospective randomized study. Minerva Chir. 2002;57:467–474. [PubMed] [Google Scholar]
- 29.Noble H, Tranter S, Chesworth T, Norton S, Thompson M. A randomized, clinical trial to compare endoscopic sphincterotomy and subsequent laparoscopic cholecystectomy with primary laparoscopic bile duct exploration during cholecystectomy in higher risk patients with choledocholithiasis. J Laparoendosc Adv Surg Tech A. 2009;19:713–720. doi: 10.1089/lap.2008.0428. [DOI] [PubMed] [Google Scholar]
- 30.Wright BE, Freeman ML, Cumming JK, Quickel RR, Mandal AK. Current management of common bile duct stones: is there a role for laparoscopic cholecystectomy and intraoperative endoscopic retrograde cholangiopancreatography as a single-stage procedure? Surgery. 2002;132:729–35; discussion 735-737. doi: 10.1067/msy.2002.127671. [DOI] [PubMed] [Google Scholar]
- 31.Poulose BK, Speroff T, Holzman MD. Optimizing choledocholithiasis management: a cost-effectiveness analysis. Arch Surg. 2007;142:43–48; discussion 49. doi: 10.1001/archsurg.142.1.43. [DOI] [PubMed] [Google Scholar]
- 32.Ghazal AH, Sorour MA, El-Riwini M, El-Bahrawy H. Single-step treatment of gall bladder and bile duct stones: a combined endoscopic-laparoscopic technique. Int J Surg. 2009;7:338–346. doi: 10.1016/j.ijsu.2009.05.005. [DOI] [PubMed] [Google Scholar]
- 33.Bergman JJ, van Berkel AM, Groen AK, Schoeman MN, Offerhaus J, Tytgat GN, Huibregtse K. Biliary manometry, bacterial characteristics, bile composition, and histologic changes fifteen to seventeen years after endoscopic sphincterotomy. Gastrointest Endosc. 1997;45:400–405. doi: 10.1016/s0016-5107(97)70151-2. [DOI] [PubMed] [Google Scholar]
- 34.Sand J, Airo I, Hiltunen KM, Mattila J, Nordback I. Changes in biliary bacteria after endoscopic cholangiography and sphincterotomy. Am Surg. 1992;58:324–328. [PubMed] [Google Scholar]
- 35.Tranter SE, Thompson MH. Comparison of endoscopic sphincterotomy and laparoscopic exploration of the common bile duct. Br J Surg. 2002;89:1495–1504. doi: 10.1046/j.1365-2168.2002.02291.x. [DOI] [PubMed] [Google Scholar]
- 36.Romagnuolo J, Bardou M, Rahme E, Joseph L, Reinhold C, Barkun AN. Magnetic resonance cholangiopancreatography: a meta-analysis of test performance in suspected biliary disease. Ann Intern Med. 2003;139:547–557. doi: 10.7326/0003-4819-139-7-200310070-00006. [DOI] [PubMed] [Google Scholar]
- 37.Rojas-Ortega S, Arizpe-Bravo D, Marín López ER, Cesin-Sánchez R, Roman GR, Gómez C. Transcystic common bile duct exploration in the management of patients with choledocholithiasis. J Gastrointest Surg. 2003:492–496. doi: 10.1016/s1091-255x(03)00026-x. [DOI] [PubMed] [Google Scholar]
- 38.Thompson MH, Tranter SE. All-comers policy for laparoscopic exploration of the common bile duct. Br J Surg. 2002;89:1608–1612. doi: 10.1046/j.1365-2168.2002.02298.x. [DOI] [PubMed] [Google Scholar]
- 39.Tinoco R, Tinoco A, El-Kadre L, Peres L, Sueth D. Laparoscopic common bile duct exploration. Ann Surg. 2008;247:674–679. doi: 10.1097/SLA.0b013e3181612c85. [DOI] [PubMed] [Google Scholar]
- 40.Williams JA, Treacy PJ, Sidey P, Worthley CS, Townsend NC, Russell EA. Primary duct closure versus T-tube drainage following exploration of the common bile duct. Aust N Z J Surg. 1994;64:823–826. doi: 10.1111/j.1445-2197.1994.tb04556.x. [DOI] [PubMed] [Google Scholar]
- 41.Paganini AM, Feliciotti F, Guerrieri M, Tamburini A, De Sanctis A, Campagnacci R, Lezoche E. Laparoscopic common bile duct exploration. J Laparoendosc Adv Surg Tech A. 2001;11:391–400. doi: 10.1089/10926420152761923. [DOI] [PubMed] [Google Scholar]
- 42.Pérez G, Escalona A, Jarufe N, Ibáñez L, Viviani P, García C, Benavides C, Salvadó J. Prospective randomized study of T-tube versus biliary stent for common bile duct decompression after open choledocotomy. World J Surg. 2005;29:869–872. doi: 10.1007/s00268-005-7698-z. [DOI] [PubMed] [Google Scholar]
- 43.Zhu QD, Tao CL, Zhou MT, Yu ZP, Shi HQ, Zhang QY. Primary closure versus T-tube drainage after common bile duct exploration for choledocholithiasis. Langenbecks Arch Surg. 2011;396:53–62. doi: 10.1007/s00423-010-0660-z. [DOI] [PubMed] [Google Scholar]
- 44.Clayton ES, Connor S, Alexakis N, Leandros E. Meta-analysis of endoscopy and surgery versus surgery alone for common bile duct stones with the gallbladder in situ. Br J Surg. 2006;93:1185–1191. doi: 10.1002/bjs.5568. [DOI] [PubMed] [Google Scholar]
- 45.Li MKW, Tang CN, Lai ECH. Managing concomitant gallbladder stones and common bile duct stones in the laparoscopic era: A systematic review. Asian J Endosc Surg. 2011;4:53–58. doi: 10.1111/j.1758-5910.2011.00073.x. [DOI] [PubMed] [Google Scholar]
- 46.Liberman MA, Phillips EH, Carroll BJ, Fallas MJ, Rosenthal R, Hiatt J. Cost-effective management of complicated choledocholithiasis: laparoscopic transcystic duct exploration or endoscopic sphincterotomy. J Am Coll Surg. 1996;182:488–494. [PubMed] [Google Scholar]
- 47.Urbach DR, Khajanchee YS, Jobe BA, Standage BA, Hansen PD, Swanstrom LL. Cost-effective management of common bile duct stones: a decision analysis of the use of endoscopic retrograde cholangiopancreatography (ERCP), intraoperative cholangiography, and laparoscopic bile duct exploration. Surg Endosc. 2001;15:4–13. doi: 10.1007/s004640000322. [DOI] [PubMed] [Google Scholar]