

Abstract
AIM: To investigate diffusion-weighted imaging (DWI) and positron emission tomography and computed tomography (PET/CT) with IV contrast for the preoperative evaluation of pelvic lymph node (LN) metastasis in uterine cancer.
METHODS: Twenty-five patients with endometrial or cervical cancer who underwent both DWI and PET/CT before pelvic lymphadenectomy were included in this study. For area specific analysis, LNs were divided into eight regions: both common iliac, external iliac, internal iliac areas, and obturator areas. The classification for malignancy on DWI was a focally abnormal signal intensity in a location that corresponded to the LN chains on the T1WI and T2WI. The criterion for malignancy on PET/CT images was increased tracer uptake by the LN.
RESULTS: A total of 36 pathologically positive LN areas were found in 9 patients. With DWI, the sensitivity, specificity, positive predictive value, negative predictive value and accuracy for detecting metastatic LNs on an LN area-by-area analysis were 83.3%, 51.2%, 27.3%, 93.3% and 57.0%, respectively, while the corresponding values for PET/CT were 38.9%, 96.3%, 70.0%, 87.8% and 86.0%. Differences in sensitivity, specificity and accuracy were significant (P < 0.0005).
CONCLUSION: DWI showed higher sensitivity and lower specificity than PET/CT. Neither DWI nor PET/CT were sufficiently accurate to replace lymphadenectomy.
Keywords: Uterine cancer, Lymph node metastasis, Magnetic resonance imaging, Diffusion-weighed imaging, Positron emission tomography and computed tomography
INTRODUCTION
The International Federation of Gynecology and Obstetrics has described the most widely accepted staging system for uterine cervical and endometrial cancer, and staging is defined in terms of the results of exploratory laparotomy, total abdominal hysterectomy, bilateral salpingo-oophorectomy, pelvic and paraaortic lymphadenectomy, and peritoneal cytology[1]. Prognosis depends on pathological stage, tumor grade and histology, and the extent of lymph node (LN) metastasis[2-7]. The latter is an important prognostic factor, and the survival rates of patients with nodal metastases are significantly lower than those of patients without such metastases[2-7]. Surgical LN assessment is the gold standard for the diagnosis of LN metastasis[8], but is highly specialized and increases the time and cost of diagnosis, with an increased risk of immediate and delayed complications to the patient. If the presence of metastases to LNs could be determined pre-operatively, this would prevent unnecessary lymphadenectomy and allow the extent of surgery to be tailored to each individual. Therefore, a noninvasive technique that accurately identifies LN metastasis would be valuable.
Computed tomography (CT) and magnetic resonance imaging (MRI) are widely used to assess LNs of patients with malignant tumors, including uterine cancer. The identification of metastatic LNs by both CT and MRI is based on measurements of node size, with a short-axis diameter greater than 8-10 mm being the most widely accepted criterion for diagnosis of nodal involvement. However, these morphological imaging techniques have very low sensitivity: the sensitivity rate for the detection of LN metastasis in endometrial cancer is between 27% and 66%, while the specificity rate is between 73% and 99%[9-14]. The corresponding rates for LN metastasis in uterine cervical cancer are between 30% and 73% and between 44% and 93%[13,15-20].
More recently, various functional imaging modalities have been used to assess LNs in patients with malignant tumors. These modalities include diffusion-weighted imaging (DWI) of MRI, MRI with ultrasmall superparamagnetic iron oxide (USPIO)[13,21,22], and positron emission tomography and CT (PET/CT) using 18F-fluorodeoxyglucose (FDG). To date, there have been three reports on apparent diffusion coefficient (ADC) obtained with DWI for the detection of LN metastasis[23-25] and several on PET/CT[20,26-31] for uterine cancer. To the best of our knowledge, there have been no studies comparing the diagnostic accuracy of DWI and PET/CT for preoperative evaluation of LNs in patients with uterine cancer. Our purpose was thus to evaluate the validity of DWI for such evaluation and compare the validity parameters for DWI with those for PET/CT.
MATERIALS AND METHODS
Subjects
A total of 25 consecutive patients, 15 with endometrial cancer and 10 with cervical cancer (age range: 45-67 years, mean age: 56 years) underwent DWI and PET/CT examinations at Dokkyo Medical University Hospital between October 2007 and August 2008 before undergoing total abdominal hysterectomy, bilateral salpingo-oophorectomy, and pelvic lymphadenectomy with or without paraaortic lymphadenectomy for histopathologically proven uterine cancer. Cancer staging of the 15 endometrial cancer patients showed there were 7 patients with stage I, 5 with stage II and 3 with stage III. Cancer staging of the 10 cervical cancer patients resulted in 6 with stage I and 4 with stage II. The time interval between MRI scan and surgical treatment was 2 to 14 d (mean: 9 d). The time interval between PET/CT scan and surgical treatment was 3 to 20 d (mean: 10 d). The time interval between MRI scan and PET/CT scan was 2 to 15 d (mean: 8 d).
Diffusion-weighted MR study
MRI was performed using a 1.5-Tesla MR scanner (Magnetom Symphony Syngo Vision; Siemens AG, Erlangen, Germany) using a phased array pelvic coil for signal reception. Routine pelvic MR images were acquired as follows: axial T1-weighed spin-echo images [repetition time (TR)/echo time (TE): 700/8.5 ms; slice thickness/intersection gap: 5/1 mm; matrix: 320 × 256; field of view (FOV): 250 mm × 250 mm]; and axial and sagittal T2-weighted turbo-spin-echo images (TR/TE: 4500/95 ms, slice thickness/intersection gap: 5/1 mm, echo train length: 11, matrix: 320 × 256, FOV: 250 mm). Axial DWI of the pelvis was performed during free breathing and by using a Stejskal-Tanner spin-echo echo-planar imaging sequence with the following parameters: TR/TE: 3500/88 ms; flip angle: 90°; NEX: 6; b-value: 0, 1000 s/mm2; readout band bandwidth: 1184 Hz/pixel; matrix: 144 × 128; FOV: 350 mm × 350 mm; and slice thickness/gap: 5/1 mm, acceleration factor: two. Motion probing gradient pulses were placed in the three orthogonal planes. 0.1 mmol/kg of gadopentetate dimeglumine (Magnevist, Bayer Health Care Pharmaceuticals, Osaka, Japan) was administered intravenously after DWI and followed by axial and sagittal T1-weighed spin-echo imaging [TR/TE: 700/8.5 ms; slice thickness/intersection gap: 5/1 mm; matrix: 320 × 256; FOV: 250 mm].
PET/CT study
Whole-body PET/CT imaging was performed using a PET/CT scanner (Biograph, Sensation 16 PET/CT system, Siemens AG). CT covered a region ranging from the meatus of the ear to the mid thigh. The technical parameters of the 16-detector row helical CT scanner were a gantry rotation speed of 0.5 s and a table speed of 24 mm per gantry rotation. The PET component of the combined imaging system had an axial view of 16.2 cm (per bed position) with an interslice spacing of 3.75 mm at one bed position and provided an image from the meatus of the ear to the mid thigh at 6-7 bed positions. The transaxial FOV and pixel size of the PET images reconstructed for fusion were 58.5 cm and 4.57 mm, respectively, with a matrix size of 128 × 128 and spatial resolution of 4.5 mm. To avoid artifacts caused by the urinary tract, patients were asked to drink 1000 mL of water 1-2 h prior to image acquisition, and to void just before the start of acquisition. No urinary bladder catheterization was used. After at least 4 h of fasting, patients received an intravenous injection of 4.0 MBq/kg body weight of FDG. The blood glucose levels of all patients were checked before FDG injection and none showed a blood glucose level of more than 8.9 mmol/L.
About 50 min later, initially unenhanced low-dose CT was performed at 140 kV and 40 mA for attenuation correction of PET images. A half-body emission PET scan was performed immediately after the low-dose CT, with a 3 min acquisition per bed position and a three-dimensional acquisition mode. Attenuation-corrected PET images were reconstructed with an ordered-subset expectation maximization iterative reconstruction algorithm (8 subsets, 3 iterations). Finally, diagnostic contrast-enhanced full-dose CT was performed with the same axial coverage at 140 kV and 230 mA and with a 2 mm slice thickness. Intravenous administration of a total volume of 150 mL (maximum) or 2 mL/kg of iodinated contrast material (Iomeprole 300; Eisai, Tokyo, Japan) by means of power injection at a rate of 2.5 mL/s was performed, and scans of the neck/thorax, upper/middle abdomen, and lower abdomen/pelvis regions were started at 45, 75 and 90 s, respectively, after injection. No oral contrast agent was administered. PET, CT, and fused PET/CT images were generated for review on a computer workstation (AZE Virtual Place Version 3.0035; Azemoto, Tokyo, Japan).
Image analysis
MRI was prospectively interpreted through consensus by two experienced radiologists (readers A with 10 and B with 21 years of experience with pelvic MRI) who had no knowledge of either the clinical data or any other imaging results. All DWI was performed with black-and-white reserved-contrast display. The classification of LNs on DWI as cancer-positive was based on the presence of focally abnormal signal intensity on the DWI in a location that corresponded to the LN chains on the enhanced T1WI and T2WI. Because the quantitative ADC value for differentiation of malignant from benign LNs in uterine cancer is reportedly controversial[23-25], LNs in our series were classified as malignant or benign on the basis of visual criteria on DWI, independently of either ADC value or size.
PET/CT images were prospectively interpreted through consensus by two experienced radiologists (readers C with 5 and D with 7 years of experience with PET/CT) who had no knowledge of either the clinical data or any other imaging results. The classification of LNs on PET/CT as cancer-positive was based on the presence of a focal increase in FDG uptake on the PET images in a location that corresponded to the LN chains on the CT images and relative to the uptake in comparable normal structures or surrounding tissue with the exclusion of physiological bowel, vessels, and urinary activity. LNs were graded as malignant or benign on the basis of functional criteria, independent of node size. LNs with focally increased tracer uptake were deemed positive for metastatic spread, even if their short-axis diameter was smaller than 1 cm. Conversely, LNs with no detectable tracer uptake were deemed negative for metastatic spread, even if their short-axis diameter was larger than 1 cm. Semiquantitative analysis to determine a standardized value for FDG uptake in the nodal lesions was not performed in our series, in line with the PET/CT image analysis method of several other studies[26-31].
Surgical procedures and histopathological evaluation
Surgery, including total abdominal hysterectomy, bilateral salpingo-oophorectomy, and pelvic lymphadenectomy with or without paraaortic lymphadenectomy, as well as peritoneal cytology, was performed by two experienced gynecologic oncologists with knowledge of the MRI and PET/CT results. Paraaortic lymphadenectomy was also performed for 14 patients in a systematic manner and in association with sampling of all LN groups. All harvested LNs were grouped according to the name of the adjacent vessel (both common iliac arteries, both external iliac arteries, both internal iliac arteries and both obturator arteries).
The surgical specimens were histopathologically evaluated as whole-mount specimens and with standard histomorphometric techniques. All LNs were sliced, routinely processed, stained with hematoxylin eosin, and examined microscopically by an experienced pathologist, who was blinded to the imaging results. The presence or absence of metastases in all removed LNs was recorded.
Statistical analysis
Patient-based and area-by-area analyses were generally performed with reference to the consensus verdicts. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated by means of standard statistical formulas. McNemar’s test was used to determine statistical significance of differences between DWI and PET/CT interpretations. A P value < 0.05 was regarded as statistically significant.
RESULTS
Metastatic LNs were identified in 9 of 25 patients (36%) in 36 of the 200 LNs regions (18%) that were examined histopathologically.
Node-based analysis
The 36 metastatic LN regions consisted of the common iliac (n = 7), external iliac (n = 7), internal iliac (n = 10), and the obturator fossa (n = 12). DWI was true-positive for 30 of the 36 metastatic node groups and true-negative for 84 of the 164 non-metastatic node groups. PET/CT was true-positive for 14 of the 36 metastatic node groups and true-negative for 158 of the 164 non-metastatic node groups. For all LN groups, the sensitivity, specificity, PPV, NPV, and accuracy of DWI vs PET/CT for the detection of pelvic metastatic LNs were 83.3% vs 38.9%, 51.2% vs 96.3%, 27.3% vs 70.0%, 93.3% vs 87.8% and 57.0% vs 86.0%, respectively (Table 1). The differences between DWI and PET/CT were significant for sensitivity (P = 0.00 018), specificity (P < 0.0001) and accuracy (P < 0.0001) (McNemar’s test). Table 2 shows a region-based comparative analysis of DWI and PET/CT. For metastatic LNs with a short axis diameter of 9 mm or less, DWI and PET/CT showed a detection sensitivity of 75% (18/24) and 16.7% (4/24), and with a diameter of 10 mm or greater the corresponding values were 100% (12/12) and 83.3% (10/12) (Table 3).
Table 1.
Overall patient- and region-based diagnostic accuracy of diffusion-weighted imaging and positron emission tomography and computed tomography n (%)
| Sensitivity | Specificity | PPV | NPV | Accuracy | |
| Patient-based DWI (n = 25) | 8/9 (88.9) | 7/16 (43.8) | 8/17 (47.1) | 7/8 (87.5) | 15/25 (60.0) |
| PET/CT (n = 25) | 4/9 (44.4) | 15/16 (93.8) | 4/5 (80.0) | 15/20 (75.0) | 16/25 (64.0) |
| Region-based DWI (n = 200) | 30/36 (83.3) | 84/164 (51.2) | 30/110 (27.3) | 84/90 (93.3) | 114/200 (57.0) |
| PET/CT (n = 200) | 14/36 (38.9) | 158/164 (96.3) | 14/20 (70.0) | 158/180 (87.8) | 172/200 (86.0) |
DWI: Diffusion-weighted imaging; PET/CT: Positron emission tomography and computed tomography; PPV: Positive predictive value; NPV: Negative predictive value.
Table 2.
Region-based diagnostic accuracy of diffusion-weighted imaging and positron emission tomography and computed tomography n (%)
| Sensitivity | Specificity | Accuracy | |
| Common iliac LNs | |||
| DWI (n = 50) | 6/7 (85.7) | 22/43 (51.2) | 28/50 (56.0) |
| PET/CT (n = 50) | 3/7 (42.9) | 41/43 (95.3) | 44/50 (88.0) |
| External iliac LNs | |||
| DWI (n = 50) | 6/7 (85.7) | 22/43 (51.2) | 28/50 (56.0) |
| PET/CT (n = 50) | 3/7 (42.9) | 41/43 (95.3) | 44/50 (88.0) |
| Internal iliac LNs | |||
| DWI (n = 50) | 8/10 (80.0) | 20/40 (50.0) | 28/50 (56.0) |
| PET/CT (n = 50) | 4/10 (40.0) | 39/40 (97.5) | 43/50 (86.0) |
| Obturator LNs | |||
| DWI (n = 50) | 10/12 (83.3) | 20/38 (52.6) | 30/50 (60.0) |
| PET/CT (n = 50) | 4/12 (33.3) | 37/38 (97.4) | 41/50 (82.0) |
DWI: Diffusion-weighted imaging; PET/CT: Positron emission tomography and computed tomography; LNs: Lymph nodes.
Table 3.
Node-based sensitivity of diffusion-weighted imaging and positron emission tomography and computed tomography according to the node size n (%)
| Node size (mm) | DWI | PET/CT |
| 1-9 | 18/24 (75.0) | 4/24 (16.7) |
| 10-18 | 12/12 (100.0) | 10/12 (83.3) |
| Total | 30/36 (83.3) | 14/36 (38.9) |
DWI: Diffusion-weighted imaging; PET/CT: Positron emission tomography and computed tomography.
Patient-based analysis
DWI was true-positive for nodal metastases for 8 of 9 patients with LN metastasis and true-negative for 7 of 16 patients without node metastasis. PET/CT was true-positive for nodal metastases in 4 of 9 patients with node metastasis and true-negative in 15 of 16 patients without node metastasis. A patient-by-patient comparison demonstrated that the sensitivity, specificity, PPV, NPV, and accuracy of DWI vs PET/CT for the detection of pelvic metastatic LNs were 88.9% vs 44.4%, 43.8% vs 93.8%, 47.1% vs 80.0%, 87.5% vs 75.0% and 60.0% vs 64.0%, respectively (Table 1). Although the differences in sensitivity and accuracy between DWI and PET/CT were not statistically significant (P = 0.134 and P = 0.434, respectively, McNemar’s test), the difference in specificity reached statistical significance (P = 0.0133, McNemar’s test). Table 4 shows patient-stage based analysis. Representative cases are shown in Figures 1 and 2.
Table 4.
Patient-stage based diagnostic accuracy of diffusion-weighted imaging and positron emission tomography and computed tomography n (%)
| Sensitivity | Specificity | Accuracy | |
| Stage I | |||
| DWI (n = 13) | 1/2 (50.0) | 5/11 (45.5) | 6/13 (46.2) |
| PET/CT (n = 13) | 0/2 (42.9) | 11/11 (100.0) | 11/13 (84.6) |
| Stage II | |||
| DWI (n = 9) | 4/4 (100.0) | 2/5 (40.0) | 6/9 (66.7) |
| PET/CT (n = 9) | 2/4 (50.0) | 4/5 (80.0) | 6/9 (66.7) |
| Stage III | |||
| DWI (n = 3) | 3/3 (100.0) | 0/0 (0) | 3/3 (100.0) |
| PET/CT (n = 3) | 2/3 (66.7) | 0/0 (0) | 2/3 (66.7) |
DWI: Diffusion-weighted imaging; PET/CT: Positron emission tomography and computed tomography.
Figure 1.
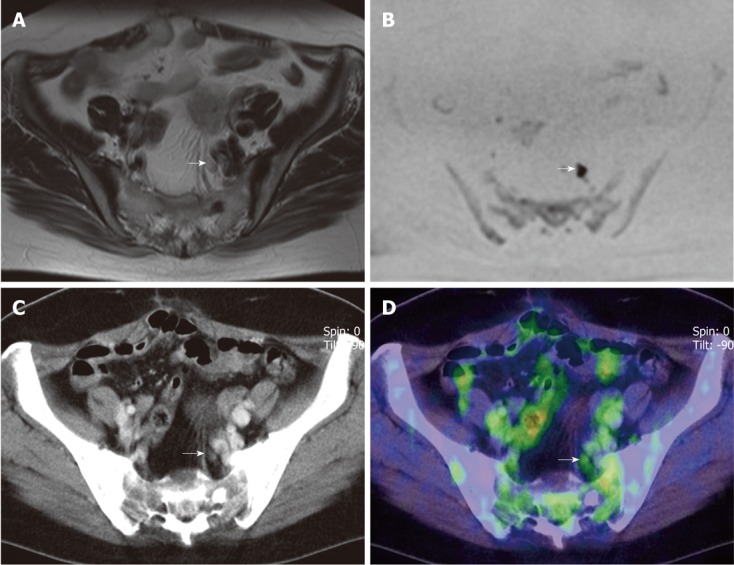
A 61-year-old woman with endometrial cancer with lymph node metastases in left internal iliac area. A: T2-weighted magnetic resonance imaging shows a small lymph node (LN) in left internal iliac area (arrow); B: The LN seen in (A) shows moderately abnormal signal intensity on diffusion-weighted imaging (DWI) (arrow) suggesting presence of nodal cancer spread; C: Enhanced CT component of positron emission tomography and computed tomography (PET/CT) shows a small LN in left internal iliac area (arrow); D: PET/CT shows that abnormal 18F-fluorodeoxyglucose uptake corresponds to the LN seen in (C) (arrow), suggesting the presence of nodal cancer spread. Histopathological specimen findings confirmed extensive LN involvement by cancer in the node. Both DWI and PET/CT were true-positive for the node.
Figure 2.
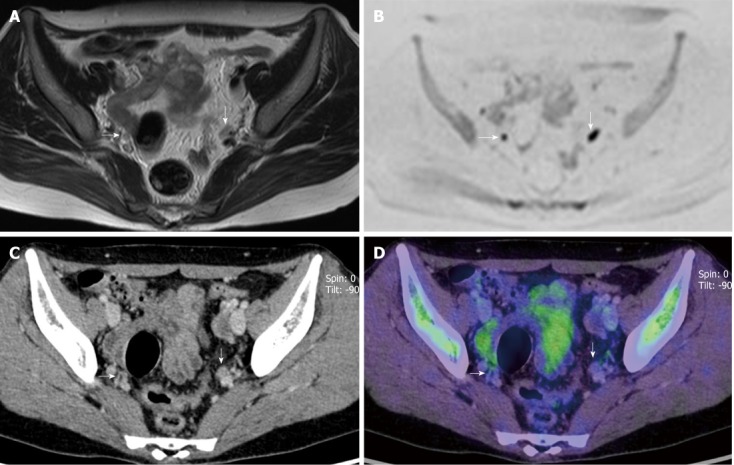
A 51-year-old woman with cervical cancer with lymph node metastases in left internal iliac area. A: T2-weighted magnetic resonance imaging shows two small lymph nodes (LNs) in right and left internal iliac areas (arrows); B: These two LNs seen in (A) show moderately abnormal signal intensity on diffusion-weighted imaging (DWI) (arrows), suggesting the presence of nodal cancer spread; C: Enhanced computed tomography (CT) component of positron emission tomography and CT (PET/CT) shows two small LNs in right and left internal iliac areas (arrows); D: PET/CT shows no 18F-fluorodeoxyglucose uptake corresponding to the two LNs seen in (C) (arrows) suggesting the absence of nodal cancer spread. Histopathological specimen findings confirmed extensive LN involvement by cancer in left internal iliac LN and no involvement in right internal iliac LN. DWI was false-positive for the right and true-positive for the left node. PET/CT was true-negative for the right and false-negative for the left node.
DISCUSSION
A noninvasive technique that can accurately identify LN metastasis in malignant tumors would be beneficial for improving treatment management. To differentiate malignant from benign LNs, cross-sectional imaging techniques based on node size measurements, with a short-axis diameter of 8-10 mm the widely accepted size criterion for LN metastasis, are used for both CT and MRI, but these morphological imaging modalities are not satisfactory[9-20].
To the best of our knowledge, ours is the first study to compare the diagnostic accuracy of DWI and PET/CT for preoperative evaluation of LNs in patients with uterine cancer. For our series, DWI showed high sensitivity and low specificity, whereas PET/CT showed low sensitivity and high specificity.
DWI is a technique for evaluating the rate of microscopic water diffusion in tissues and has recently been used in oncologic imaging for the depiction and characterization of tumors as well as for differentiating benign from malignant lesions in various kinds of tumors including uterine cancer[32-34]. In general, water molecule diffusion is more restricted in malignant than normal tissue, probably because malignant tissue has greater cellular density and less extracellular space. DWI can thus show high sensitivity for detection of small lesions such as peritoneal dissemination[35], and liver metastasis[36]. However, DWI not only visualizes pathological areas in malignant lesions but also benign pathologies with restricted diffusion such as abscesses, neurogenic tumors, epidermoid cysts, and several normal structures, that is brain, salivary glands, tonsils, spleen, gallbladder, small intestine/small intestinal contents, colon, adrenal glands, prostate, testes, penis, endometrium, ovaries, spinal cord, peripheral nerves, bone marrow and LNs[32]. Because normal LNs often exhibit high signal intensity due to high cellular density, the specificity for detection of LN metastasis by visual DWI analysis is low as was confirmed in our series.
The quantitative ADC value is reportedly controversial for differentiating malignant from benign LNs in uterine cancer[23-25]. Kim et al[23] demonstrated that the ADC values for metastatic LNs (0.756 ± 0.114 × 10-3 mm2/s) are significantly lower than those for nonmetastatic LNs (1.002 ± 0.186 × 10-3 mm2/s) of patients with cervical cancer. Lin et al[24] showed that the ADC values for metastatic LNs (0.83 ± 0.15 × 10-3 mm2/s) are higher than those for nonmetastatic LNs (0.75 ± 0.19 × 10-3 mm2/s) of patients with cervical and endometrial cancer. In addition, Nakai et al[25] provided evidence that the ADC values for metastatic LNs (1.4 ± 0.4 × 10-3 mm2/s) and nonmetastatic LNs (1.3 ± 0.24 × 10-3 mm2/s) were almost the same for patients with uterine cancer and sarcoma. We therefore assume that ADC analysis for the preoperative evaluation of LN metastasis in patients with uterine cancer is not acceptable so that ADC analyses were not performed in our study.
There have been several reports demonstrating the accuracy of FDG-PET/CT for detecting LN metastasis in uterine cancer[20,26-31]. They revealed the sensitivity, specificity, and accuracy of PET/CT on region-specific analyses were 36%-72%, 88%-99% and 84%-99%, respectively, and that corresponding values for patient-based analyses were 41%-77%, 56%-100% and 76%-89%. PET/CT thus tends to show low sensitivity and high specificity as was also seen in our series. Because tiny LNs tend to show smaller standardized uptake value than real values due to the partial volume effect, it is difficult to use the usual cut-off point (2.5-3.0) for differentiating malignant from benign LN. Semiquantitative analysis to determine a standardized value for FDG uptake in nodal lesions has not been performed in many studies[26-28]. FDG-PET/CT is primarily limited by its inability to detect microscopic metastasis. This impaired PET/CT performance is not surprising, because 0.5 cm corresponds to the mean value for spatial resolution of the PET components, which is in the range of 0.4 to 0.6 cm. This still limited spatial resolution of the PET component makes the presence of metastasis in small LNs almost indetectable[20,26-28]. Improving the spatial resolution and sensitivity of PET scanners and developing new, more specific radioactive tracers may help to overcome this limitation in the future.
During the past decade, enhanced MRI using a special lymphographic contrast agent - USPIO - has been proposed as useful for evaluating LN metastasis in several human malignant tumors, such as uterine cancer[13], prostate cancer[21], and breast cancer[22]. These researchers have found that USPIO allows the detection of microscopic metastatic LNs and has a high overall level of accuracy for detecting nodal metastasis. Rockall et al[13] reported excellent results with USPIO for detecting LN metastasis in uterine cancer with 82%-93% sensitivity and 97% specificity for node-specific analysis and 91%-100% sensitivity and 87-94% specificity for a patient-based analysis.
Our study has certain limitations. First, the number of patients was relatively small. A larger-scale investigation to evaluate DWI and PET/CT for the detection of LN metastasis is thus warranted. Our findings show the accuracy of PET/CT for a selected cohort of women with uterine cervical and endometrial cancer, but not for a population of women at all stages of the disease. Second, we performed a region-based analysis and thus could not determine the relationship between individual LNs visualized by imaging and LNs analyzed by a pathologist. Third, oral contrast agents were not used for the CT component. Oral contrast material could be helpful for better delineation of LNs and normal bowel. Finally, the surgeons were guided by the preoperative MRI and PET/CT findings, and this may have resulted in verification bias.
In conclusion, DWI showed higher sensitivity and lower specificity than FDG-PET/CT, but neither DWI nor PET/CT are sufficiently accurate to replace lymphadenectomy.
COMMENTS
Background
A noninvasive technique that can accurately identify lymph node (LN) metastasis in malignant tumors would be beneficial for improving treatment management. Because the identification of metastatic LNs by both computed tomography (CT) and magnetic resonance imaging is based on measurements of node size, with a short-axis diameter greater than 8-10 mm being the most widely accepted criterion for diagnosis of nodal involvement, these morphological imaging techniques have very low sensitivity. More recently, various functional imaging modalities such as diffusion-weighted imaging (DWI), ultrasmall superparamagnetic iron oxide, positron emission tomography and CT (PET/CT) have been used to assess LNs in patients with malignant tumors.
Research frontiers
To date, there have been several reports on apparent diffusion coefficient (ADC) obtained with DWI and 18F-fluorodeoxyglucose (FDG)-PET/CT for the detection of LN metastasis in patients with uterine cancer. However, to the best of our knowledge, there have been no studies comparing the diagnostic accuracy of DWI and PET/CT for preoperative evaluation of pelvic LNs in patients with uterine cancer.
Innovations and breakthroughs
This is the first study to compare the diagnostic accuracy of DWI and FDG-PET/CT with IV contrast medium for preoperative evaluation of LN metastasis in patients with uterine cancer, with surgical and histopathological findings used as the reference standard. For our series, DWI showed high sensitivity and low specificity, whereas FDG-PET/CT showed low sensitivity and high specificity.
Applications
Because the spatial resolution of the present PET components is in the range of 0.4 to 0.6 cm, the sensitivity by PET/CT for detecting tiny tumors and LN metastasis is low. Improving the spatial resolution and sensitivity of PET scanners and developing new, more specific radioactive tracers may help to overcome this limitation in the future. The quantitative ADC value is reportedly controversial for differentiating malignant from benign LNs in uterine cancer, so further analysis is needed to clarify the usefulness of ADC values.
Terminology
DWI is a technique for evaluating the rate of microscopic water diffusion in tissues and has recently been used in oncologic imaging for the depiction and characterization of tumors as well as for differentiating benign from malignant lesions in various kinds of tumors including uterine cancer. In general, water molecule diffusion is more restricted in malignant than normal tissue, probably because malignant tissue has greater cellular density and less extracellular space. Metabolic imaging using PET/CT with FDG has had a major impact in oncology over the past decade, allowing combined metabolic and morphological assessment of tumors with a significantly improved impact on patient management-diagnosis, staging, treatment optimization, re-staging, therapy monitoring and prognostication of various malignant tumors.
Peer review
This article addressed a comparison between DWI and PET/CT in evaluating the pelvic lymph node metastasis in uterine cancer. The authors’ work provides some useful clinical information in the field.
Footnotes
Peer reviewers: Feng Chen, MD, PhD, Professor, Department of Radiology, Zhong Da Hospital, Southeast University, 87 Ding Jiaqiao, Nanjing 210009, Jiangsu Province, China; Mohamed Abou El-Ghar, MD, Department of Radiology, Urology and Nephrology center-Mansoura University, 72 El-gomhoria st, Mansoura 35516, Egypt
S- Editor Cheng JX L- Editor O’Neill M E- Editor Zheng XM
References
- 1.Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet. 2009;105:103–104. doi: 10.1016/j.ijgo.2009.02.012. [DOI] [PubMed] [Google Scholar]
- 2.Manetta A, Delgado G, Petrilli E, Hummel S, Barnes W. The significance of paraaortic node status in carcinoma of the cervix and endometrium. Gynecol Oncol. 1986;23:284–290. doi: 10.1016/0090-8258(86)90128-9. [DOI] [PubMed] [Google Scholar]
- 3.Creasman WT, Morrow CP, Bundy BN, Homesley HD, Graham JE, Heller PB. Surgical pathologic spread patterns of endometrial cancer. A Gynecologic Oncology Group Study. Cancer. 1987;60:2035–2041. doi: 10.1002/1097-0142(19901015)60:8+<2035::aid-cncr2820601515>3.0.co;2-8. [DOI] [PubMed] [Google Scholar]
- 4.Inoue T, Morita K. The prognostic significance of number of positive nodes in cervical carcinoma stages IB, IIA, and IIB. Cancer. 1990;65:1923–1927. doi: 10.1002/1097-0142(19900501)65:9<1923::aid-cncr2820650909>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- 5.Gal D, Recio FO, Zamurovic D, Tancer ML. Lymphvascular space involvement--a prognostic indicator in endometrial adenocarcinoma. Gynecol Oncol. 1991;42:142–145. doi: 10.1016/0090-8258(91)90334-2. [DOI] [PubMed] [Google Scholar]
- 6.Stehman FB, Bundy BN, DiSaia PJ, Keys HM, Larson JE, Fowler WC. Carcinoma of the cervix treated with radiation therapy. I. A multi-variate analysis of prognostic variables in the Gynecologic Oncology Group. Cancer. 1991;67:2776–2785. doi: 10.1002/1097-0142(19910601)67:11<2776::aid-cncr2820671111>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 7.Lai CH, Hong JH, Hsueh S, Ng KK, Chang TC, Tseng CJ, Chou HH, Huang KG. Preoperative prognostic variables and the impact of postoperative adjuvant therapy on the outcomes of Stage IB or II cervical carcinoma patients with or without pelvic lymph node metastases: an analysis of 891 cases. Cancer. 1999;85:1537–1546. doi: 10.1002/(sici)1097-0142(19990401)85:7<1537::aid-cncr15>3.0.co;2-6. [DOI] [PubMed] [Google Scholar]
- 8.Chan JK, Cheung MK, Huh WK, Osann K, Husain A, Teng NN, Kapp DS. Therapeutic role of lymph node resection in endometrioid corpus cancer: a study of 12,333 patients. Cancer. 2006;107:1823–1830. doi: 10.1002/cncr.22185. [DOI] [PubMed] [Google Scholar]
- 9.Hricak H, Rubinstein LV, Gherman GM, Karstaedt N. MR imaging evaluation of endometrial carcinoma: results of an NCI cooperative study. Radiology. 1991;179:829–832. doi: 10.1148/radiology.179.3.2028000. [DOI] [PubMed] [Google Scholar]
- 10.Sugiyama T, Nishida T, Ushijima K, Sato N, Kataoka A, Imaishi K, Fujiyoshi K, Yakushiji M. Detection of lymph node metastasis in ovarian carcinoma and uterine corpus carcinoma by preoperative computerized tomography or magnetic resonance imaging. J Obstet Gynaecol (Tokyo 1995) 1995;21:551–556. doi: 10.1111/j.1447-0756.1995.tb00911.x. [DOI] [PubMed] [Google Scholar]
- 11.Connor JP, Andrews JI, Anderson B, Buller RE. Computed tomography in endometrial carcinoma. Obstet Gynecol. 2000;95:692–696. doi: 10.1016/s0029-7844(99)00626-2. [DOI] [PubMed] [Google Scholar]
- 12.Manfredi R, Mirk P, Maresca G, Margariti PA, Testa A, Zannoni GF, Giordano D, Scambia G, Marano P. Local-regional staging of endometrial carcinoma: role of MR imaging in surgical planning. Radiology. 2004;231:372–378. doi: 10.1148/radiol.2312021184. [DOI] [PubMed] [Google Scholar]
- 13.Rockall AG, Sohaib SA, Harisinghani MG, Babar SA, Singh N, Jeyarajah AR, Oram DH, Jacobs IJ, Shepherd JH, Reznek RH. Diagnostic performance of nanoparticle-enhanced magnetic resonance imaging in the diagnosis of lymph node metastases in patients with endometrial and cervical cancer. J Clin Oncol. 2005;23:2813–2821. doi: 10.1200/JCO.2005.07.166. [DOI] [PubMed] [Google Scholar]
- 14.Rockall AG, Meroni R, Sohaib SA, Reynolds K, Alexander-Sefre F, Shepherd JH, Jacobs I, Reznek RH. Evaluation of endometrial carcinoma on magnetic resonance imaging. Int J Gynecol Cancer. 2007;17:188–196. doi: 10.1111/j.1525-1438.2007.00805.x. [DOI] [PubMed] [Google Scholar]
- 15.Kim SH, Kim SC, Choi BI, Han MC. Uterine cervical carcinoma: evaluation of pelvic lymph node metastasis with MR imaging. Radiology. 1994;190:807–811. doi: 10.1148/radiology.190.3.8115631. [DOI] [PubMed] [Google Scholar]
- 16.Scheidler J, Hricak H, Yu KK, Subak L, Segal MR. Radiological evaluation of lymph node metastases in patients with cervical cancer. A meta-analysis. JAMA. 1997;278:1096–1101. [PubMed] [Google Scholar]
- 17.Hawighorst H, Schoenberg SO, Knapstein PG, Knopp MV, Schaeffer U, Essig M, van Kaick G. Staging of invasive cervical carcinoma and of pelvic lymph nodes by high resolution MRI with a phased-array coil in comparison with pathological findings. J Comput Assist Tomogr. 1998;22:75–81. doi: 10.1097/00004728-199801000-00013. [DOI] [PubMed] [Google Scholar]
- 18.Yang WT, Lam WW, Yu MY, Cheung TH, Metreweli C. Comparison of dynamic helical CT and dynamic MR imaging in the evaluation of pelvic lymph nodes in cervical carcinoma. AJR Am J Roentgenol. 2000;175:759–766. doi: 10.2214/ajr.175.3.1750759. [DOI] [PubMed] [Google Scholar]
- 19.Reinhardt MJ, Ehritt-Braun C, Vogelgesang D, Ihling C, Högerle S, Mix M, Moser E, Krause TM. Metastatic lymph nodes in patients with cervical cancer: detection with MR imaging and FDG PET. Radiology. 2001;218:776–782. doi: 10.1148/radiology.218.3.r01mr19776. [DOI] [PubMed] [Google Scholar]
- 20.Choi HJ, Roh JW, Seo SS, Lee S, Kim JY, Kim SK, Kang KW, Lee JS, Jeong JY, Park SY. Comparison of the accuracy of magnetic resonance imaging and positron emission tomography/computed tomography in the presurgical detection of lymph node metastases in patients with uterine cervical carcinoma: a prospective study. Cancer. 2006;106:914–922. doi: 10.1002/cncr.21641. [DOI] [PubMed] [Google Scholar]
- 21.Harisinghani MG, Barentsz J, Hahn PF, Deserno WM, Tabatabaei S, van de Kaa CH, de la Rosette J, Weissleder R. Noninvasive detection of clinically occult lymph-node metastases in prostate cancer. N Engl J Med. 2003;348:2491–2499. doi: 10.1056/NEJMoa022749. [DOI] [PubMed] [Google Scholar]
- 22.Harada T, Tanigawa N, Matsuki M, Nohara T, Narabayashi I. Evaluation of lymph node metastases of breast cancer using ultrasmall superparamagnetic iron oxide-enhanced magnetic resonance imaging. Eur J Radiol. 2007;63:401–407. doi: 10.1016/j.ejrad.2007.02.010. [DOI] [PubMed] [Google Scholar]
- 23.Kim JK, Kim KA, Park BW, Kim N, Cho KS. Feasibility of diffusion-weighted imaging in the differentiation of metastatic from nonmetastatic lymph nodes: early experience. J Magn Reson Imaging. 2008;28:714–719. doi: 10.1002/jmri.21480. [DOI] [PubMed] [Google Scholar]
- 24.Lin G, Ho KC, Wang JJ, Ng KK, Wai YY, Chen YT, Chang CJ, Ng SH, Lai CH, Yen TC. Detection of lymph node metastasis in cervical and uterine cancers by diffusion-weighted magnetic resonance imaging at 3T. J Magn Reson Imaging. 2008;28:128–135. doi: 10.1002/jmri.21412. [DOI] [PubMed] [Google Scholar]
- 25.Nakai G, Matsuki M, Inada Y, Tatsugami F, Tanikake M, Narabayashi I, Yamada T. Detection and evaluation of pelvic lymph nodes in patients with gynecologic malignancies using body diffusion-weighted magnetic resonance imaging. J Comput Assist Tomogr. 2008;32:764–768. doi: 10.1097/RCT.0b013e318153fd43. [DOI] [PubMed] [Google Scholar]
- 26.Sironi S, Buda A, Picchio M, Perego P, Moreni R, Pellegrino A, Colombo M, Mangioni C, Messa C, Fazio F. Lymph node metastasis in patients with clinical early-stage cervical cancer: detection with integrated FDG PET/CT. Radiology. 2006;238:272–279. doi: 10.1148/radiol.2381041799. [DOI] [PubMed] [Google Scholar]
- 27.Park JY, Kim EN, Kim DY, Suh DS, Kim JH, Kim YM, Kim YT, Nam JH. Comparison of the validity of magnetic resonance imaging and positron emission tomography/computed tomography in the preoperative evaluation of patients with uterine corpus cancer. Gynecol Oncol. 2008;108:486–492. doi: 10.1016/j.ygyno.2007.11.044. [DOI] [PubMed] [Google Scholar]
- 28.Kitajima K, Murakami K, Yamasaki E, Fukasawa I, Inaba N, Kaji Y, Sugimura K. Accuracy of 18F-FDG PET/CT in detecting pelvic and paraaortic lymph node metastasis in patients with endometrial cancer. AJR Am J Roentgenol. 2008;190:1652–1658. doi: 10.2214/AJR.07.3372. [DOI] [PubMed] [Google Scholar]
- 29.Kitajima K, Murakami K, Yamasaki E, Kaji Y, Sugimura K. Accuracy of integrated FDG-PET/contrast-enhanced CT in detecting pelvic and paraaortic lymph node metastasis in patients with uterine cancer. Eur Radiol. 2009;19:1529–1536. doi: 10.1007/s00330-008-1271-8. [DOI] [PubMed] [Google Scholar]
- 30.Chung HH, Park NH, Kim JW, Song YS, Chung JK, Kang SB. Role of integrated PET-CT in pelvic lymph node staging of cervical cancer before radical hysterectomy. Gynecol Obstet Invest. 2009;67:61–66. doi: 10.1159/000162101. [DOI] [PubMed] [Google Scholar]
- 31.Signorelli M, Guerra L, Buda A, Picchio M, Mangili G, Dell’Anna T, Sironi S, Messa C. Role of the integrated FDG PET/CT in the surgical management of patients with high risk clinical early stage endometrial cancer: detection of pelvic nodal metastases. Gynecol Oncol. 2009;115:231–235. doi: 10.1016/j.ygyno.2009.07.020. [DOI] [PubMed] [Google Scholar]
- 32.Kwee TC, Takahara T, Ochiai R, Nievelstein RA, Luijten PR. Diffusion-weighted whole-body imaging with background body signal suppression (DWIBS): features and potential applications in oncology. Eur Radiol. 2008;18:1937–1952. doi: 10.1007/s00330-008-0968-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Naganawa S, Sato C, Kumada H, Ishigaki T, Miura S, Takizawa O. Apparent diffusion coefficient in cervical cancer of the uterus: comparison with the normal uterine cervix. Eur Radiol. 2005;15:71–78. doi: 10.1007/s00330-004-2529-4. [DOI] [PubMed] [Google Scholar]
- 34.Fujii S, Matsusue E, Kigawa J, Sato S, Kanasaki Y, Nakanishi J, Sugihara S, Kaminou T, Terakawa N, Ogawa T. Diagnostic accuracy of the apparent diffusion coefficient in differentiating benign from malignant uterine endometrial cavity lesions: initial results. Eur Radiol. 2008;18:384–389. doi: 10.1007/s00330-007-0769-9. [DOI] [PubMed] [Google Scholar]
- 35.Fujii S, Matsusue E, Kanasaki Y, Kanamori Y, Nakanishi J, Sugihara S, Kigawa J, Terakawa N, Ogawa T. Detection of peritoneal dissemination in gynecological malignancy: evaluation by diffusion-weighted MR imaging. Eur Radiol. 2008;18:18–23. doi: 10.1007/s00330-007-0732-9. [DOI] [PubMed] [Google Scholar]
- 36.Nasu K, Kuroki Y, Nawano S, Kuroki S, Tsukamoto T, Yamamoto S, Motoori K, Ueda T. Hepatic metastases: diffusion-weighted sensitivity-encoding versus SPIO-enhanced MR imaging. Radiology. 2006;239:122–130. doi: 10.1148/radiol.2383041384. [DOI] [PubMed] [Google Scholar]