

Abstract
Although spinal metastasis is a common finding in malignancies, however intradural extramedullary metastasis is very rare. This paper presents a 71-year-old woman, known case of papillary carcinoma of thyroid with intradural extramedullary metastasis in thoracic spine.
Background
Spine tumours and mass lesions are traditionally classified by anatomic location into three categories: intramedullary, intradural-extramedullary and extradural.1 Intradural intra and extramedullary metastases of non-neurogenic origin present an extremely rare manifestation of systemic cancer.2 Intradural extramedullary spinal-cord metastasis is seen at autopsy in fewer than 5% of patients who have died from cancer. These tumours are commonly the result of drop lesions from intracranial metastasis from adenocarcinoma of the lung, prostate cancer, breast cancer, melanoma, or lymphoma.3 Intradural extramedullary metastasis from papillary cell carcinoma of thyroid is very rare. This paper presents a 71-year-old woman with this situation.
Case presentation
A 71-year-old woman, a known case of papillary thyroid cancer was referred to our center for palliative radiation therapy for her painful left sacroiliac area. In medical history, the disease had begun 6 years ago. Total thyrodectomy, 100 mCi iodine ablative therapy and hormone replacement therapy were performed in other centers. Two years later however, recurrence in cervical lymph nodes had occurred. Surgery and 200 mCi iodine therapy were performed in the same centres. Whole body bone scan with technetium 99m showed abnormal increased uptake of this radioisotope in L5 and left sacroiliac joint. Reminder of skeleton showed normal radioisotope uptake. Pelvic CT scanning of sacroiliac joint showed a lytic lesion with sclerotic border and confirmed bone metastasis. Local external beam radiation therapy with 4000cGY dose was done. One week later, her pain decreased but 1 month later the patient was referred again to our centre with decreased lower extremity force and mid-thoracic burning pain radiating toward anterior chest wall. Whole body I131 radioisotope scanning did not show any suspicious abnormal uptake especially in the thoracic vertebras. Thoracic MRI with gadolinium showed a well-defined oval shape, 2×1 cm intradural extramedullary mass, isosignal inT1 and hypersignal inT2 at the level of T4-T5 thoracic spine, showing marked homogenous enhancement (figures 1 and 2). Because of progressive muscle weakness the patient was referred to neurosurgeon and was operated. After laminectomy of T3, T4 and T5 a solid grey – red mass intradural appeared compressing the cord.
Figure 1.

MRI show s marked homogenous enhancement.
Figure 2.

MRI show marked homogenous enhancement.
Differential diagnosis
The classic radiologic findings of intradural extramedullary lesions are the expansion of the ipsilateral subarachnoid space and the displacement of the cord to the contralateral side. Meningiomas and nerve sheath tumours account for 80%–90% of these lesions. Metastasic lesions, infection, inflammatory diseases, epidermoid and dermoid tumours, lipomas and arachnoid cysts are the differential diagnosis.
Treatment
Gross total resection was performed and the specimen was sent for pathological examination. H&E staining showed neoplastic tissue composed of sheaths of cells with ovaloid nuclei and without cytoplasmic border some of them revealing ground glass appearance and nuclear grooves. There was also many unevenly distributed psammoma bodies between the cells (figure 3). Pathology revealed metastatic lesion from papillary thyroid carcinoma. Partially pain relief and improving lower extremity force occurred following surgery. MRI with gadolinium was repeated 6 weeks later and although there was not any evidence of gross residual disease however, an enhanced rim in the anterior of dura at the level of T3–T4 was detected. Although it might be due to postsurgical inflammation, however by considering the time of performing MRI, another probable diagnosis was small amounts of residual tumour cells and therefore radiation therapy to the bed of tumour with 2 cm margins with 4000cGY was performed.
Figure 3.
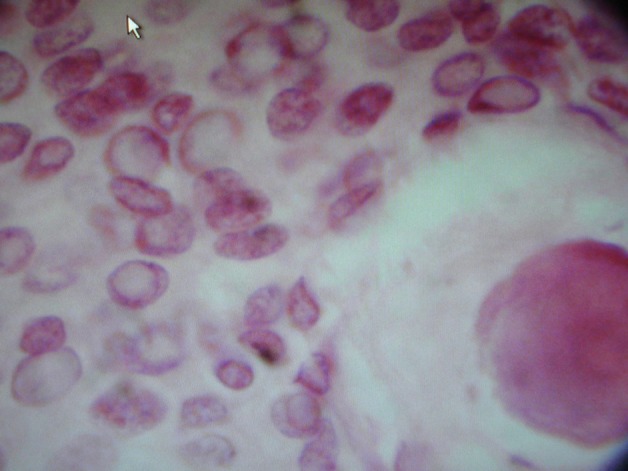
H&E staining showed neoplastic tissue composed of sheaths of cells with ovaloid nuclei and without cytoplasmic border (x10).
Outcome and follow-up
The patient is fairly well now, 6 months after ending of treatment.
Discussion
Papillary carcinoma of the thyroid is the commonest type of thyroid tumour comprising between 30% and 70% of all thyroid carcinoma cases.4 It usually remains intrathyroidal and tends to spread via local extension or metastasis to regional lymph nodes however, distant metastases are very uncommon and mainly occur in lungs and bones.5 CNS metastasis is very rare and usually occurs as brain metastasis. To our knowledge, there are few reports of intradural intramedullry metastasis from thyroid cancer, however we could not find any case of intradural extramedullary metastasis. We believe it is the first case of papillary thyroid cancer with intradural extramedullary metastasis. Extramedullary tumours account for more than 70% of intradural spinal cord tumours in adults and are only slightly less common in children.3 Schwannomas, neurofibromas and meningiomas are the most common intradural extramedullary spinal cord tumours. Less common entities include paragangliomas, metastases, lipomas, spinal nerve sheath myxomas, sarcomas and vascular tumours.6 In most cases, the solitary intradural extramedullary metastasis is located on a nerve root, making difficult its differentiation from a nerve sheath tumour.7 Pain is the initial symptom in occurring in 90% to 95% of patients. This pain is usually local and associated with tenderness elicited by palpation over the spinal process at the level of involvement. On occasion a component of radicular pain, radiating in the distribution of the nerve root at the involved level, may accompany neck or back pain. Pain of a severe, burning, dysesthetic nature is often associated with intradurl extramedullary metastatic lesions, whereas pain aggravated by movement and alleviated by immobility should raise suspicion of spinal instability and pathological fracture–dislocation.8 Motor and sensory deficits, especially the Brown-Sequard syndrome, are common. Sphincter dysfunction is present in about a third of patients.3 This patient had thoracic burning pain that radiated to anterior chest wall and progressive lower extremities weakness. Five routes have been hypothesised for dissemination of metastatic intradural tumour from outside of the central nervous system (CNS): 1) haematogenous, via the arterial system, 2) via the perineural lymphatics, 3) through the venous plexus, 4) spreading via subarachnoid space and 5) seeding from the involved osseous structure to the cerebrospinal fluid through the dura mater.9 Nerve root metastases can radiologically mimic a benign nerve sheath tumour. Nerve sheath tumours are the most common intradural extramedullary spinal cord tumours, showing bone findings on plain films, such as enlargement of the neural foramen, osseous change and pedicle erosion.10 Before MRI, the diagnosis of this condition was made by using myelography and CT scanning,11 however these days gadolinium enhanced MRI is the imaging modality of choice for spinal tumours, including spinal metastases7 and it has been shown to facilitate the earlier diagnosis of spinal metastases than other modalities. It is superior in depicting epidural and bone marrow tumour infiltration, and it delineates the extraosseous soft-tissue component of a neoplasm from the normal paraspinal soft tissue and neural structures. In addition to its diagnostic utility, MRI information is essential for the process of thorough surgical planning. Gadolinium enhancement further increases the sensitivity of MRI investigations, because metastases invariably are enhanced. Visualisation of the entire vertebral axis in multiple orthogonal planes is easily accomplished, a goal that is important given the high incidence of multiple vertebral levels of tumor infiltration. Studies show that the results of MRI investigations alter therapeutic decisions in a significant number of patients, especially with regard to the addition or modification of radiotherapy.8 In this patient, MRI showed a gadolinium enhanced mass isosignal in T1 and hypersignal in T2 and contiguous vertebras (T3,T4 and T5) appeared normal. Schowanoma, astrocytoma and metastatic lesions were considered in differential diagnosis. When whole body I131 radioisotope scanning showed normal findings and thyroglubulin also was in normal level, we thought there was a primary intradural extramedullary lesion than a secondary one, but pathology revealed metastatic lesion.
The best predictor of outcome is the site of primary tumour. Several results are reported. Survival varied by tumour type, with the best prognosis noted in patients with breast or kidney cancer.
Life expectancy is often relatively short, with median survival ranging from 4 to 15 months in various series.8
Management of spinal metastasis is undertaken to relieve pain and preserve neurological function. Palliation is the real treatment goal. Therapeutic irradiation and surgical decompression are the principal and complementary treatment options. Irradiation is particularly effective for metastasis of lymphoreticular origin, moderately effective for metastatic lesions from breast, prostate and less effective for lesions of pulmonary origin. Indications of surgery consist of: failure of irradiation therapy, unknown diagnosis, pathological fracture dislocation and rapidly progressing paraplegia.12
Learning points.
Although metastasis to spinal canal without bone involvement is not common in papillary carcinoma of thyroid it may occur.
Radioisotope scan with I131 may not show any abnormality.
In MRI and even in the time of operation it can mimic a nerve sheath tumour.
Total resection of the mass with or without radiation therapy could be helpful.
Footnotes
Competing interests: None.
Patient consent: Obtained.
References
- 1.Sciubba DM, Gokaslan ZL. Diagnosis and management of metastatic spine disease. Surg Oncol 2006;15:141–51. [DOI] [PubMed] [Google Scholar]
- 2.Wostrack M, Pape H, Kreutzer J, et al. Surgical treatment of spinal intradural carcinoma metastases. Acta Neurochir (Wien) 2012;154:349–57. [DOI] [PubMed] [Google Scholar]
- 3.Traul DE, Shaffrey ME, Schiff D. Part I: spinal-cord neoplasms-intradural neoplasms. Lancet Oncol 2007;8:35–45. [DOI] [PubMed] [Google Scholar]
- 4.Goolden AWG, Mclaughlin JE, Valentine AR, et al. Solitary cerebral metastasis from a papillary carcinoma of the thyroid. Postgrad Med J I990;66:127–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ota T, Bando Y, Hirai M, et al. Papillary carcinoma of the thyroid with distant metastases to the cerebrum: a case report. Jpn J Clin Oncol 2001;31:112–5. [DOI] [PubMed] [Google Scholar]
- 6.Chamberlain MC, Tredway TL. Adult primary intradural spinal cord tumors: a review. Curr Neurol Neurosci Rep 2011;11:320–8. [DOI] [PubMed] [Google Scholar]
- 7.Jung YJ, Kim SW, Chang CH, et al. Intradural extramedullary non-infiltrated solitary metastatic tumor. J Korean Neurosurg Soc 2005;37:466–8. [Google Scholar]
- 8.Jacobs WB, Perrin RG. Evaluation and treatment of spinal metastases: an overview. Neurosurg Focus 2001;11:e10. [DOI] [PubMed] [Google Scholar]
- 9.Ito K, Miahara T, Goto T, et al. Solitary metastatic cauda equina tumor from breast cancer. Neurol Medd Chir (Tokyo) 2010;50:417–20. [DOI] [PubMed] [Google Scholar]
- 10.Ng WP, Fehlings M. Intradura metastasis mimicking nerve sheath tumor. Spine 1995;20:2580–3. [DOI] [PubMed] [Google Scholar]
- 11.Frey I, Le Breton C, Lefkopoulos A, et al. Intradural extramedullary spinal canal secondary neoplasms: MR findings in 30 patients. Eur Radiol 1998;8:1187–92. [DOI] [PubMed] [Google Scholar]
- 12.Babu M, Gupta R, Kumar A, et al. Spinal intradural metastasis. Jk Science 2004;6:48–50. [Google Scholar]