

Abstract
Breast ulceration is an alarming sign for clinicians and places a significant physical and psychological burden on the patient. We report a rare presentation of pyoderma gangrenosum of the breast in a patient known to have ulcerative colitis but no active underlying disease process and no history of breast tissue trauma. This case report with literature review highlights the importance of considering pyoderma gangrenosum as a differential diagnosis in breast ulcers.
Keywords: Breast ulcer, necrotizing skin disease, pyoderma gangrenosum
INTRODUCTION
Although breast cancer would be the most likely differential clinical diagnosis in any patient with breast ulceration, other rare causes should be considered. We present a case report about a postmenopausal woman with breast ulceration caused by pyoderma gangrenosum (PG).
CASE REPORT
A 54-year-old postmenopausal white woman presented with a very painful left breast ulcer of 2 weeks' duration. The ulcer started as a small boil with yellow discharge and then increased gradually in size. She had no history of recent gastrointestinal or other systemic symptoms and had not previously undergone any surgery or biopsy of her left breast.
The patient had been diagnosed with ulcerative colitis (UC) 19 years earlier. Her last colonoscopy was a few months before her presentation; the results did not show features of active colitis. She was on long-term sulphasalazine (3 g/day) for her colitis. She stopped smoking at the age of 35 and had no family history of breast disease.
Clinical examination revealed an approximately 5 × 3 cm superficial ulcer located mainly in the upper central part of the left breast. The ulcer was very tender and surrounded by erythema and induration with yellow discharge (Figure 1). Nothing else was found during examination of both breasts and axillae. Abdominal examination was unremarkable.
Figure 1.

Pretreatment: left breast pyoderma gangrenosum.
Routine blood tests showed normal liver and renal function. The hemoglobin level was 11.3 gm/dL with a normal mean cell volume of 88.9 fL. The white cell and platelet counts were within the normal range. The erythrocyte sedimentation rate (ESR) was slightly elevated at 24 mm/hr, and the autoantibody screening test was unremarkable. The culture and sensitivity test of the ulcer microbiology swab was negative. An ultrasound scan of both breasts was normal. We did not perform mammography because we believed it would be too painful.
A punch biopsy of the ulcer showed occasional superficial subcorneal pustules. The epidermis was acanthotic and spongiotic with inflammatory exocytosis. The dermis contained a dense, diffuse neutrophilic infiltrate. We found no evidence of malignancy. The overall features were those of neutrophilic inflammation with abscess formation. The histologic features were not specific but were compatible with the clinical diagnosis of PG (Figures 2 and 3).
Figure 2.
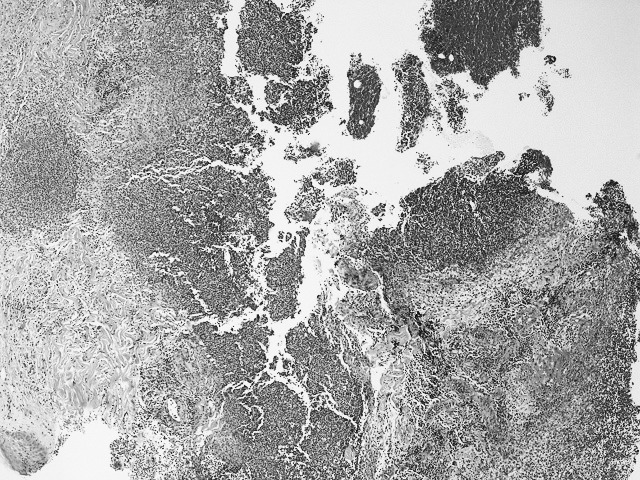
Ulcer edge with evidence of active inflammation and abscess formation in the dermis composed of polymorphs (hematoxylin-eosin stain, magnification ×25).
Figure 3.
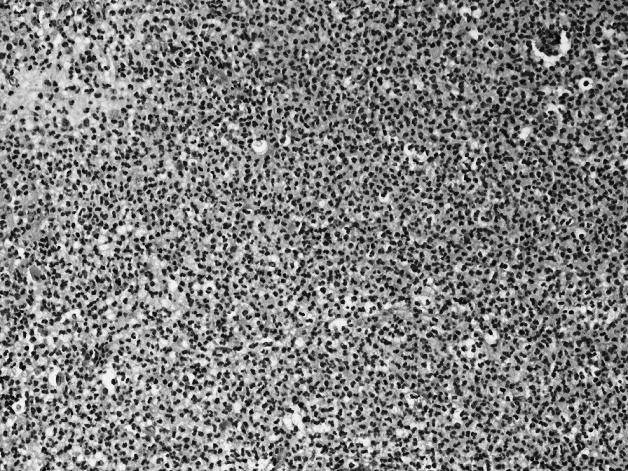
High-power view of the abscess shows large numbers of polymorphs and granulation tissue reaction (hematoxylin-eosin stain, magnification ×40).
The patient was treated with 50 mg prednisolone daily and topical corticosteroids (0.1% betamethasone cream) for the first 3 months; the oral dose has since been reduced. She is currently on 10 mg prednisolone daily. This treatment has resulted in a significant improvement of the ulcer (Figure 4). Her most recent ESR was 18 mm/hr. She is still being seen for regular follow-up, and the oral steroid dose is monitored according to the clinical response.
Figure 4.

Posttreatment: left breast pyoderma gangrenosum.
DISCUSSION
PG is a rare cutaneous necrotising skin disease characterised by a chronic neutrophilic inflammatory reaction and resulting in erythematous papules with blue-purple-red margins, most often presenting as painful ulceration.1,2
Brocq1 first described this idiopathic process in 1916 as occurring in all age groups but most commonly in patients in their 30s through 50s with a similar sex distribution. The overall incidence is unknown because of the rarity of the condition, but the literature estimates it to be 3:1,000,000 annually in the United States.3
The pathogenesis of the process is unknown, but suggested causes include immune-complex mediated neutrophilic vascular reactions. The diagnosis is predominantly clinical; histopathologic findings and laboratory tests serve mostly to rule out mimicking lesions. The presence or absence of vasculitis is a controversial feature but is not thought to be a primary event even if present. The earliest lesions show follicular and perifollicular inflammation with neutrophilic abscesses in the dermis. These lesions can later lead to dermal necrosis with ulceration and undermining inflammation at the ulcer edge.1,2,4-7
The most common anatomical site for PG in patients with inflammatory bowel disease (IBD) is the lower limbs, where it has been reported in 75%-80% of IBD patients.1,8-10 PG was originally thought to be pathognomonic of IBD, affecting UC patients more than those with Crohn disease.2,11-14 Although this connection is commonly true, other conditions have been associated with PG, such as rheumatoid arthritis and hematologic disorders.1,15-20 The prevalence rate of associated systemic disease ranges widely in the literature (50%-78%).1,3,21-24
Reported therapies for PG have often been focused on treatment of the underlying condition; therefore, most information available relates to systemic therapies,2,25,26 probably because many PG lesions mimic the activity of the underlying disease.27 However, our patient had no symptoms of active UC throughout the clinical course of the PG lesion.
First-line therapies include immunosuppressants such as corticosteroids (prednisolone/methylprednisolone) and cyclosporin.2,13,28-30 Other therapies include immunomodulators, biologics, and antileprosy drugs. These treatments have been used predominantly on steroid-refractory PG lesions associated with IBD.1,30 As an adjunct to other treatment, systemic antibiotics may have a role in PG remission.1,31-33 Patients similar to ours, in whom the underlying associated disease is quiescent, can respond variably to standard therapy; PG can even recur after definitive surgery for the underlying disease, for example, colectomy.26,34-36
Angiò et al26 described a case of PG of the sinus mammarum in a patient with UC that emphasized the resistance of the cutaneous ulcer to conventional systemic medical therapy although the treatment was efficacious regarding the colonic process. They used the histopathologic finding of vasculitis at the edge of the lesions to justify the use of antithrombotic topical injections as an adjunct to standard treatment. This isolated case report suggested that perilesional injections of calcic heparin were successful in inducing remission.26
The role of topical therapies is not well evaluated in the literature.1,26 One retrospective analysis of 20 patients showed that topical steroids have little role in healing.1,37 Conversely, other authors have demonstrated improvement of the lesions with intralesional steroids (triamcinolone acetonide).38
Currently, the Study of Treatments for Pyoderma Gangrenosum Patients (STOP GAP) Trial is taking place in approximately 50 hospitals throughout the United Kingdom and Ireland, with the aim to investigate the best way to treat PG lesions. A total of 140 patients will be randomized to have either prednisolone or cyclosporin.39 Patients who initially require topical therapy will enter a parallel observational study. If their PG lesions fail to respond to topical therapy, the participants could be enrolled in the randomized trial of systemic treatments.40
Reported cases of surgical debridement and split skin grafts for PG lesions generally have poor outcomes. Perhaps these poor outcomes result from the pathergy phenomenon, a key feature in the disease process in which any traumatized skin (debridement sites or skin graft donor sites) develops additional necrosis and ulceration.41,42 Therefore, surgical intervention is not recommended in standard practice.
A review of published works disclosed 43 reported cases of PG of the breast, of which 30 cases (approximately 70%) reported that PG lesions were secondary to trauma of the breast tissue such as surgical intervention, reconstruction of the breast, biopsy, and intramuscular injection.1,2,20,26,43-48 Again, the pathergy phenomenon may explain the high percentage of PG lesions after breast trauma.
CONCLUSIONS
Our patient had a rare presentation of PG of the breast, in which she had associated UC but no active underlying disease process and no history of breast tissue trauma. This case highlights the importance of considering PG as one of the differential diagnoses of breast ulcers. Careful specialist clinical assessment could establish an early diagnosis and formulate an effective management plan. Long-term dermatology follow-up and contribution to clinical trials could provide a better understanding of the disease and its response to various treatment options.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
REFERENCES
- 1.Hasselmann DO, Bens G, Tilgen W, Reichrath J. Pyoderma gangrenosum: clinical presentation and outcome in 18 cases and review of the literature. J Dtsch Dermatol Ges. 2007 Jul;5(7):560–564. doi: 10.1111/j.1610-0387.2007.0328.x. [DOI] [PubMed] [Google Scholar]
- 2.Tromm A, May D, Almus E, et al. Cutaneous manifestations in inflammatory bowel disease. Z Gastroenterol. 2001 Feb;39(2):137–144. doi: 10.1055/s-2001-11153. [DOI] [PubMed] [Google Scholar]
- 3.Powell FC, Schroeter AL, Su WP, Perry HO. Pyoderma gangrenosum and sarcoidosis. Arch Dermatol. 1984 Jul;120(7):959–960. [PubMed] [Google Scholar]
- 4.Jorizzo JL, Solomon AR, Zanolli MD, Leshin B. Neutrophilic vascular reactions. J Am Acad Dermatol. 1988 Dec;19(6):983–1005. doi: 10.1016/s0190-9622(88)70264-9. [DOI] [PubMed] [Google Scholar]
- 5.Newell LM, Malkinson FD. Commentary: pyoderma gangrenosum. Arch Dermatol. 1982 Oct;118(10):769–773. doi: 10.1001/archderm.118.10.743. [DOI] [PubMed] [Google Scholar]
- 6.Powell FC, Schroeter AL, Su WP, Perry HO. Pyoderma gangrenosum: a review of 86 patients. Q J Med. 1985 May;55(217):173–186. [PubMed] [Google Scholar]
- 7.Ackerman AB. Questions to the Editorial Board. Am J Dermatopath. 1983;;5(4):409–410. [Google Scholar]
- 8.Levitt MD, Ritchie JK, Lennard-Jones JE, Phillips RK. Pyoderma gangrenosum in inflammatory bowel disease. Br J Surg. 1991 Jun;78(6):676–678. doi: 10.1002/bjs.1800780613. [DOI] [PubMed] [Google Scholar]
- 9.von den Driesch P. Pyoderma gangrenosum: a report of 44 cases with follow-up. Br J Dermatol. 1997 Dec;137(6):1000–1005. [PubMed] [Google Scholar]
- 10.Bennett ML, Jackson JM, Jorizzo JL, Fleischer AB, Jr, White WL, Callen JP. Pyoderma gangrenosum. A comparison of typical and atypical forms with an emphasis on time to remission. Case review of 86 patients from 2 institutions. Medicine (Baltimore) 2000 Jan;79(1):37–46. doi: 10.1097/00005792-200001000-00004. [DOI] [PubMed] [Google Scholar]
- 11.Greenstein AJ, Janowitz HD, Sachar DB. The extra-intestinal complications of Crohn's disease and ulcerative colitis: a study of 700 patients. Medicine (Baltimore) 1976 Sep;55(5):401–412. doi: 10.1097/00005792-197609000-00004. [DOI] [PubMed] [Google Scholar]
- 12.Kirsch B, Gerhardt H, Gladisch R, Heine M, Rohr G, Weiss J. Dermatosen bei chronisch entzündlichen Darmerkrankungen. Ergebnisse einer Untersuchung Von 119 Morbus-Crohn-/colitis Patienten. Akt Dermatol. 1992;;18((1-2)):17–22. [Google Scholar]
- 13.Lamers CB. Treatment of extraintestinal complications of ulcerative colitis. Eur J Gastroenterol Hepatol. 1997 Sep;9(9):850–853. doi: 10.1097/00042737-199709000-00005. [DOI] [PubMed] [Google Scholar]
- 14.McCord ML, Hall RP. Cutaneous manifestations of inflammatory bowel disease. In: Shanahan F, editor. Targan Sr. Inflammatory Bowel Disease: From Bench to Bedside. Baltimore, MD: Williams & Wilkins;; 1994. pp. 682–694. [Google Scholar]
- 15.Bargen JA. Complications and sequelae of chronic ulcerative colitis. Ann Intern Med. 1929 Oct;3(4):335–352. [Google Scholar]
- 16.Crowson AN, Mihm MC, Jr, Magro C. Pyoderma gangrenosum: a review. J Cutan Pathol. 2003 Feb;30(2):97–107. doi: 10.1034/j.1600-0560.2003.00024.x. [DOI] [PubMed] [Google Scholar]
- 17.Tay CH. Letter: pyoderma gangrenosum and leukemia. Arch Dermatol. 1973 Oct;108(4):580–581. [PubMed] [Google Scholar]
- 18.Jacobs P, Palmer S, Gordon-Smith EC. Pyoderma gangrenosum in myelodysplasia and acute leukaemia. Postgrad Med J. 1985 Aug;61(718):689–694. doi: 10.1136/pgmj.61.718.689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Struthers GR. Pyoderma gangrenosum, seronegative polyarthropathy and inflammatory bowel disease. J R Soc Med. 1979 Apr;72(4):284–286. doi: 10.1177/014107687907200414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Labat JP, Simon H, Metges JP, Lucas B, Malhaire JP. [Pyoderma gangrenosum and breast cancer: a new case] Ann Med Interne (Paris) 2000 Jun;151(4):314–315. French. [PubMed] [Google Scholar]
- 21.Perry HO, Brunsting LA. Pyoderma gangrenosum; a clinical study of nineteen cases. AMA Arch Derm. 1957 Mar;75(3):380–386. doi: 10.1001/archderm.1957.01550150066007. [DOI] [PubMed] [Google Scholar]
- 22.Callen JP. Pyoderma gangrenosum. Lancet. 1998 Feb 21;351(9102):581–585. doi: 10.1016/S0140-6736(97)10187-8. [DOI] [PubMed] [Google Scholar]
- 23.Perry HO, Winkelmann RK. Bullous pyoderma gangrenosum and leukemia. Arch Dermatol. 1972 Dec;106(6):901–905. [PubMed] [Google Scholar]
- 24.Prystowsky JH, Kahn SN, Lazarus GS. Present status of pyoderma gangrenosum. Review of 21 cases. Arch Dermatol. 1989 Jan;125(1):57–64. [PubMed] [Google Scholar]
- 25.Thornton JR, Teague RH, Low-Beer TS, Read AE. Pyoderma gangrenosum and ulcerative colitis. Gut. 1980 Mar;21(3):247–248. doi: 10.1136/gut.21.3.247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Angiò LG, Pirrone G, Rivoli G, et al. Pyoderma gangrenosum of the “sinus mammarum” in ulcerative colitis. G Chir. 2003 Jun-Jul;24((6-7)):247–254. [PubMed] [Google Scholar]
- 27.Johnson WT, Norva WM. Cutaneous manifestations of inflammatory bowel disease. In: Lukash WM, Johnson RB, editors. The Systemic Manifestations of Inflammatory Bowel Disease. Springfield, IL: Charles C. Thomas Publisher, Ltd; 1975. p. 212. [Google Scholar]
- 28.Chow RK, Ho VC. Treatment of pyoderma gangrenosum. J Am Acad Dermatol. 1996 Jun;34(6):1047–1060. doi: 10.1016/s0190-9622(96)90285-6. [DOI] [PubMed] [Google Scholar]
- 29.Schwaegerle SM, Bergfeld WF, Senitzer D, Tidrick RT. Pyoderma gangrenosum: a review. J Am Acad Dermatol. 1988 Mar;18(3):559–568. doi: 10.1016/s0190-9622(88)70080-8. [DOI] [PubMed] [Google Scholar]
- 30.Reichrath J, Bens G, Bonowitz A, Tilgen W. Treatment recommendations for pyoderma gangrenosum: an evidence-based review of the literature based on more than 350 patients. J Am Acad Dermatol. 2005 Aug;53(2):273–283. doi: 10.1016/j.jaad.2004.10.006. [DOI] [PubMed] [Google Scholar]
- 31.Wines N, Wines M, Ryman W. Understanding pyoderma gangrenosum: a review. MedGenMed. 2001 Jun 27;3(3):6. [PubMed] [Google Scholar]
- 32.Powell FC, Su WP, Perry HO. Pyoderma gangrenosum: classification and management. J Am Acad Dermatol. 1996 Mar;34(3):395–409. 410–412. doi: 10.1016/s0190-9622(96)90428-4. quiz. [DOI] [PubMed] [Google Scholar]
- 33.Davies MG, Piper S. Pyoderma gangrenosum: successful treatment with minocycline. Clin Exp Dermatol. 1981 Mar;6(2):219–223. doi: 10.1111/j.1365-2230.1981.tb02294.x. [DOI] [PubMed] [Google Scholar]
- 34.Holmlund DE, Wählby L. Pyoderma gangrenosum after colectomy for inflammatory bowel disease. Case report. Acta Chir Scand. 1987 Jan;153(1):73–74. [PubMed] [Google Scholar]
- 35.Mayer L, Janowitz HD. Extraintestinal manifestations of inflammatory bowel disease. In: Kirsner JB, Shorter RG, editors. Inflammatory Bowel Disease. Philadelphia, PA: 1988. p. 299. [Google Scholar]
- 36.Talansky AL, Meyers S, Greenstein AJ, Janowitz HD. Does intestinal resection heal the pyoderma gangrenosum of inflammatory bowel disease? J Clin Gastroenterol. 1983 Jun;5(3):207–210. doi: 10.1097/00004836-198306000-00002. [DOI] [PubMed] [Google Scholar]
- 37.Sheldon DG, Sawchuk LL, Kozarek RA, Thirlby RC. Twenty cases of peristomal pyoderma gangrenosum: diagnostic implications and management. Arch Surg. 2000 May;135(5):564–568. doi: 10.1001/archsurg.135.5.564. discussion 568-569. [DOI] [PubMed] [Google Scholar]
- 38.Goldstein F, Krain R, Thornton JJ. Intralesional steroid therapy of pyoderma gangrenosum. J Clin Gastroenterol. 1985 Dec;7(6):499–501. doi: 10.1097/00004836-198512000-00011. [DOI] [PubMed] [Google Scholar]
- 39.The Stop Gap Trial. UK Dermatology Clinical Trials Network. 2011. July. http://www.stopgaptrial.co.uk/. Accessed 01 October 2011.
- 40.Mitchell E. RCT of treatments for Pyoderma gangrenosum: time to get involved. Wounds UK. 2010;;6(4):27–32. [Google Scholar]
- 41.Kaddoura IL, Amm C. A rationale for adjuvant surgical intervention in pyoderma gangrenosum. Ann Plast Surg. 2001 Jan;46(1):23–28. doi: 10.1097/00000637-200101000-00005. [DOI] [PubMed] [Google Scholar]
- 42.Long CC, Jessop J, Young M, Holt PJ. Minimizing the risk of post-operative pyoderma gangrenosum. Br J Dermatol. 1992 Jul;127(1):45–48. doi: 10.1111/j.1365-2133.1992.tb14826.x. [DOI] [PubMed] [Google Scholar]
- 43.Mansur AT, Balaban D, Göktay F, Takmaz S. Pyoderma gangrenosum on the breast: a case presentation and review of the published work. J Dermatol. 2010 Jan;37(1):107–110. doi: 10.1111/j.1346-8138.2009.00756.x. [DOI] [PubMed] [Google Scholar]
- 44.Duval A, Boissel N, Servant JM, Santini C, Petit A, Vignon-Pennamen MD. Pyoderma gangrenosum of the breast: a diagnosis not to be missed. J Plast Reconstr Aesthet Surg. 2011 Jan;64(1):e17–e20. doi: 10.1016/j.bjps.2010.07.022. Epub 2010 Sep 18. [DOI] [PubMed] [Google Scholar]
- 45.Goshtasby PH, Chami RG, Johnson RM. A novel approach to the management of pyoderma gangrenosum complicating reduction mammaplasty. Aesthet Surg J. 2010 Mar;30(2):186–193. doi: 10.1177/1090820X10366011. [DOI] [PubMed] [Google Scholar]
- 46.Maigre M, Bouachour G, Varache N, Alquier P, Verret JL. [Pseudo-septicemic pyoderma gangrenosum and breast cancer. Apropos of a case caused by an intramuscular injection] Rev Med Interne. 1991 Nov-Dec;12(6):452–454. doi: 10.1016/s0248-8663(05)83195-9. French. [DOI] [PubMed] [Google Scholar]
- 47.Beurey J, Weber M, Delrous JL, Chaulieu Y. [Pyoderma gangrenosum: Clofazimine therapy] Ann Dermatol Venereol. 1977 Oct;104(10):631–634. French. [PubMed] [Google Scholar]
- 48.Caterson SA, Nyame T, Phung T, Lee B, Tobias AM. Pyoderma gangrenosum following bilateral deep inferior epigastric perforator flap breast reconstruction. J Reconstr Microsurg. 2010 Sep;26(7):475–479. doi: 10.1055/s-0030-1261699. Epub 2010 Jun 9. [DOI] [PubMed] [Google Scholar]