

Abstract
Objective
The psychological processes of doubting and skepticism have recently become topics of neuroscientific investigation. In this context, we developed the False Tagging Theory, a neurobiological model of the belief and doubt process, which proposes that the prefrontal cortex is critical for normative doubt regarding properly comprehended cognitive representations. Here, we put our theory to an empirical test, hypothesizing that patients with prefrontal cortex damage would have a doubt deficit that would manifest as higher authoritarianism and religious fundamentalism.
Method
Ten patients with bilateral damage to the ventromedial prefrontal cortex (vmPFC), ten patients with damage to areas outside the vmPFC, and sixteen medical comparison patients, who experienced life-threatening (but non-neurological) medical events, completed a series of scales measuring authoritarianism, religious fundamentalism, and specific religious beliefs.
Results
VMPFC patients reported significantly higher authoritarianism and religious fundamentalism than the other groups. The degrees of authoritarianism and religious fundamentalism in the vmPFC group were significantly higher than normative values, as well; by contrast, the comparison groups did not differ from normative values. Moreover, vmPFC patients reported increased specific religious beliefs after brain injury.
Conclusions
The findings support the False Tagging Theory, and suggest that the vmPFC is critical for psychological doubt and resistance to authoritarian persuasion.
Keywords: lesion, prefrontal cortex, authoritarianism, fundamentalism, belief
INTRODUCTION
How we come to develop the cognitive capacities for belief and doubt has been an enduring focus of psychological and philosophical inquiry. Recently, these processes have begun to be studied from a neuroscience perspective, and there have been efforts to map out the neural bases for belief and doubt. For example, neuroimaging studies have shown that tasks involving evaluation and doubting of beliefs activate the prefrontal cortex, among other brain regions (Elliott, Rees, & Dolan, 1999; Fletcher, Anderson, Shanks, Honey, Carpenter et al., 2001; Harris, Sheth, & Cohen, 2008; Parris, Kuhn, Mizon, Benattayallah, & Hodgson, 2009). However, these studies leave many questions unanswered, and a neuroimaging approach cannot conclusively show that a neural region is critical for the process of accepting or rejecting belief representations. Thus, there remain many gaps in our understanding of how belief and doubt operate in the brain.
We developed the False Tagging Theory (FTT), a neuroanatomically-based theoretical model of the belief and doubt process (Asp & Tranel, 2012). In brief, the FTT asserts that 1) the process of belief occurs in two stages, mental representation and assessment (Gilbert, 1991); 2) all ideas that are represented are initially believed, but a secondary psychological analysis (assessment) can produce disbelief (or doubt) (Gilbert, 1991; Gilbert, Tafarodi, & Malone, 1993); 3) the mental representation of the idea, which is initially believed or regarded as true, must be “tagged” to indicate false value, producing doubt (Gilbert, 1991); 4) the prefrontal cortex is necessary for the “false tag” in the assessment component of belief; and 5) “false tags” are affective in nature, akin to the central tenets of Damasio’s (1994) “somatic marker hypothesis.” The FTT predicts that focal damage to the prefrontal cortex should result in a “doubt deficit,” accompanied by a vulnerability to believe inaccurate information. There is already some evidence in accord with this hypothesis, including the findings that prefrontal patients 1) often have a general personality trait that is overconfident, boastful, grandiose, obstinate, and egocentric (Damasio, Anderson, & Tranel, 2011; Stuss & Benson, 1984), indicating a lack of normative doubt; 2) are more gullible toward disreputable characters (Croft, Duff, Kovach, Anderson, Adolphs et al., 2010; Damasio, 1994); and 3) are more vulnerable to deceptive advertising (Asp, Manzel, Koestner, Cole, Denburg et al., in press). A “doubt deficit” or a disruption in the false tagging mechanism may also explain other cognitive deficits and abnormal behaviors in prefrontal patients, such as perseveration, confabulation, and distractibility (Asp & Tranel, 2012).
Here, we put our false tagging theory to an empirical test, hypothesizing that patients with prefrontal cortex damage would have a doubt deficit that would manifest as higher authoritarianism and religious fundamentalism. Our focus on authoritarianism and religious fundamentalism was motivated by several factors. Individuals high in authoritarianism tend to easily submit to authority, are often aggressive in the name of authority, and tend to hold dogmatic beliefs without a reflexive critique (Adorno, Frenkel-Brunswik, Levinson, & Sanford, 1950; Altemeyer, 1996). High authoritarians rely on authorities to provide their beliefs for them, which ushers in rigid, dogmatic attitudes without skeptical safeguards. Religious fundamentalism refers to an attitude toward religious beliefs, independent from a specific religion or a set of specific religious beliefs. Religious fundamentalists have high religious beliefs and tend to hold them with an immutable, unjustified certainty (Altemeyer, 1996). In regard to specific religious beliefs (e.g., belief in literality of the bible), such beliefs may be particularly valuable for our empirical test in that they are discordant with physical “reality,” professed to all individuals, held to various degrees, and not directly falsifiable. Therefore, on average, an individual who has a “doubt deficit” could be expected to have higher authoritarianism, religious fundamentalism, and more specific religious beliefs.
Not surprisingly, authoritarianism and religious fundamentalism are not entirely different constructs. In fact, authoritarianism has been found to correlate fairly highly with religious fundamentalism, with typical r values of 0.68–0.82; (Altemeyer & Hunsberger, 2004), and religious fundamentalism has even been viewed as simply a religious manifestation of authoritarianism (Altemeyer, 1996). In our foray into the investigation of the neural basis of “doubt deficits,” we explored both constructs, recognizing that they overlap. We also explored changes in religious beliefs, with the idea that in patients with the adult onset of focal damage to the vmPFC, there could be a post-morbid increase in religious beliefs due to damage to the “doubt” mechanism in the vmPFC.
In summary, as an empirical test of our FTT, we studied authoritarianism, religious fundamentalism, and changes in religious beliefs in patients with focal, adult-onset damage to the vmPFC. We included two comparison groups: brain-damaged comparisons, namely, patients with brain damage to regions outside of the vmPFC; and medical comparisons, namely, patients who had undergone a life-threatening medical event that was non-neurological in nature. We hypothesized that vmPFC patients would have higher levels of authoritarianism and religious fundamentalism, and higher post-morbid increases in religious beliefs, than the two comparison groups.
METHOD
Participants
We studied 20 individuals with adult-onset brain lesions: 10 patients with bilateral damage to the ventromedial prefrontal cortex constituted our vmPFC group (Fig. 1), and 10 patients with damage to regions outside the vmPFC constituted our brain damaged comparison group (BDC) (Table 1, 2). VMPFC lesion etiologies consisted of stroke (n = 4) and meningioma (benign tumor) resection (n = 6); BDC lesion etiologies consisted of stroke (n = 5) and surgical resection (n = 5). BDC lesion locations were outside of putative emotion-related neural structures such as the amygdala; and were distributed as follows: occipital (n = 2); temporal (n = 5); posterior frontal (non-prefrontal, n = 2); and parietal (n = 1). The vmPFC patients had impaired autonomic responses to emotionally charged pictures, as well as striking defects in empathy, guilt, and insight; but exhibited mostly intact general intelligence, working memory, and executive functioning (Table 1). All BDC patients had normal social and emotional functioning. Generally, vmPFC patients were also more punitive during the Ultimatum Game and endorsed more immoral actions in personal moral dilemmas (Table 1). The neurological patients were selected from the Patient Registry of the Division of Behavioral Neurology and Cognitive Neuroscience at the University of Iowa (Table 2). We also included a medical comparison group (MC), comprised by 16 patients who had undergone a life-threatening medical event which was non-neurological in nature (Table 2). The MC group’s medical events involved non-neurological cancer (n = 10), myocardial infarction (n =2), dangerous surgery (n = 1), pulmonary embolism (n =1), or a chronic non-neurological disease (n = 2). This group was included to control for authoritarian and religious fundamentalism changes that might be due to having gone through a profound adverse medical event per se (Ingersoll-Dayton, Krause, & Morgan, 2002). All neuroimaging and attitudinal data in the brain damaged participants were obtained in the chronic recovery epoch (defined as 3 months or more post lesion onset). Attitudinal data were collected over a several-month period in 2009 and 2010.
Fig. 1.
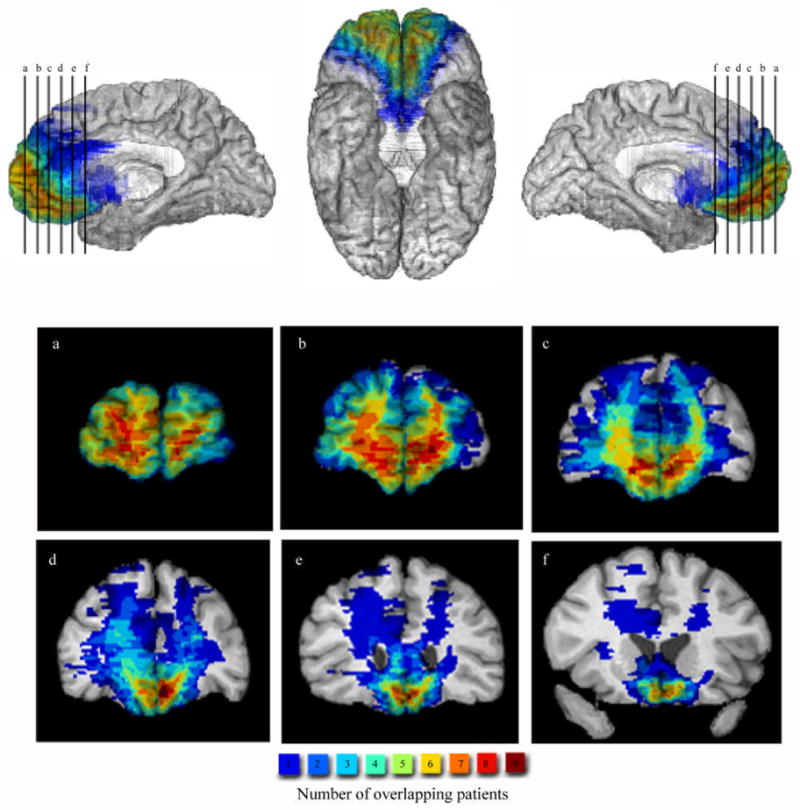
Lesion overlap of vmPFC patients. Lesions of the vmPFC patients displayed in mesial and coronal slices. The color bar indicates the number of overlapping lesions at each voxel.
TABLE 1.
Neuropsychological, social/emotion, and experimental data for vmPFC patients
| Subject # | WAIS-III FSIQ | WMS-III WMI | WCST (PE) | Stroop (Inter) | Autonomic responses | Empathy | Guilt | Insight | Punitive behavior | Moral judgment |
|---|---|---|---|---|---|---|---|---|---|---|
| 318 | 143 | 124 | 4 | 70 | Impaired | 3 | 3 | 3 | 0.83 | 0.52 |
| 1815 | 121 | 105 | 10 | 58 | Impaired | 2 | 2 | 3 | 0.66† | NA |
| 1983 | 108 | 105 | 10 | 67 | Impaired | 3 | 3 | 3 | 0.89 | 0.55 |
| 2352 | 106 | 124 | 9 | 57 | Impaired | 2 | 1 | 2 | 0.44 | 0.29 |
| 2391 | 109 | 102 | 7 | 54 | Impaired | 3 | 3 | 3 | 0.61 | 0.52 |
| 2577 | 84 | 88 | 66 | 73 | Impaired | 3 | 3 | 3 | 0.78 | 0.15 |
| 3032 | 102 | 99 | 25 | 47 | Impaired | 1 | 2 | 1 | 0.00† | 0.38‡ |
| 3336 | 100 | 88 | 5 | 54 | Impaired | 1 | 1 | 1 | NA | 0.43 |
| 3383 | 95 | 95 | 19 | 48 | Impaired | 3 | 3 | 3 | NA** | NA** |
| 3534 | 110* | 127 | 8 | 48 | Impaired | 3 | 3 | 3 | 1.00† | NA |
WAIS-III, Wechsler Adult Intelligence Scale-III scores (FSIQ, full-scale IQ). WMS-III, Wechsler Memory Scale-III scores (WMI, working memory index). WCST (PE), Wisconsin Card Sort Test perseverative errors, a measure of executive function. Stroop (Inter), T-score on the Interference trial of the Stroop Color-Word Test, a measure of response inhibition. Autonomic responses, skin conductance responses to emotionally charged socially significant stimuli (e.g., pictures of social disasters, mutilations, nudes), using methods previously described (Damasio et al., 1990). A clinical neuropsychologist rated each vmPFC patient’s demonstrated capacity for empathy, guilt, and insight in his or her personal life. The rating used a four-point scale denoting severity of impairment, where 0 = normal, 1 = mild, 2 = moderate, and 3 = severe. Ratings were based on data derived from spouse or family member reports in the Iowa Scales of Personality Change (Barrash, Tranel, & Anderson, 2000) and from clinical interview data. Both of these sources provide direct observations about the patient’s emotions and general disposition, and include questions about whether the patient 1) experiences and manifests emotions such as sadness, anxiety, empathy, embarrassment, and guilt; and 2) underestimates or is unaware of shortcomings and personal problems. Punitive behavior and moral judgment were experimental data gathered previously (Koenigs & Tranel, 2007; Koenigs et al., 2007). Punitive behavior values reflect the proportion of punishments given simulated players following unfair offers ($3, $2, and $1) during the Ultimatum Game (a brain damaged comparison group punished unfair offers at M = 0.38, SD = 0.30). Moral judgment values reflect the proportion of moral violations endorsed during personal moral dilemmas (a brain damaged comparison group endorsed moral violations at M = 0.20, SD = 0.15).
Patient 3534 was administered the WAIS-IV rather than the WAIS-III; thus, FSIQ = General Ability Index (GAI).
Data unavailable due to patient discontinuing the project.
Data courtesy of Dr. Timothy Koscik.
Data courtesy of Dr. Michael Koenigs.
TABLE 2.
Demographic data for subject groups
| vmPFC | BDC | MC | Normal 1 | Normal 2 | |
|---|---|---|---|---|---|
|
|
|||||
| Number | 10 | 10 | 16 | 29 | 424 |
| Age (SD) | 58.5 (12.8) | 54.1 (12.4) | 46.7 (14.2) | 57.9 (14.5) | 48.2 (6.1) |
| Education (SD) | 13.6 (2.4) | 15.6 (3.3) | 15.6 (2.3) | 14.0 (1.1) | 14.0 (3.2) |
| Chronicity (SD) | 11.1 (9.0) | 7.7 (3.2) | 9.8 (12.4) | -- | -- |
| Childhood Religiosity (SD) | 3.9 (0.7) | 4.0 (1.0) | 4.0 (0.9) | -- | -- |
| Religious Participation (SD) | 3.0 (1.0) | 2.7 (1.1) | 3.2 (1.0) | -- | -- |
| Sex | 6 M; 4 F | 4 M; 6 F | 4 M; 12 F | 15 M; 14 F | 199 M; 225 F |
Age, education and chronicity are presented in years. Chronicity refers to the length of time between lesion/medical event onset and collection of data for the current experiment. Childhood religiosity was measured by probing whether participants were raised in a religious tradition and how often they attended religious services as a young child. This was measured on a Likert scale (1–5), where a value of 1 represents low childhood religiosity and a value of 5 represents high childhood religiosity. Religious participation was measured by probing how often participants currently attend religious services, using a Likert scale (1–5) where 1 = never, 2 = once or twice a year, 3 = about once a month, 4 = every week, and 5 = several times a week. Normal group 1 data were provided by Wegmann (1992), and Normal group 2 data were provided by Altemeyer (Altemeyer & Hunsberger, 2004).
The patients in this study come from a demographically homogeneous region (mainly rural Iowa), and authoritarian and fundamentalism attitudes in this population tend to be similarly homogeneous. All patients reported affiliation with a moderate/liberal Christian denomination except for one MC patient who reported affiliation with a fundamentalist Christian denomination as a Mennonite (denominational demarcation was done via normative values on the Religious Fundamentalism Scale (Altemeyer & Hunsberger, 1992)): vmPFC patients reported affiliation with Church of Christ (n = 2), Lutheran (n = 2), Methodist (n = 3), Presbyterian (n = 2), and Reformed Church in America (n = 1); BDC patients reported Disciple of Christ Church (n = 1), Lutheran (n = 3), Methodist (n = 2), Roman Catholic (n = 2), and Unitarian (n = 2); and MC patients reported general affiliation (n = 1), Lutheran (n = 5), Mennonite (n = 1), Methodist (n = 2), Presbyterian (n = 2), Roman Catholic (n = 4), and Unitarian (n = 1). No patient reported a change in denomination affiliation after their medical event. There were no significant differences in childhood religiosity or current religious participation between the groups (Table 2). In addition, there were no significant between-group differences in age, education, sex, or chronicity (Table 2). All patients were free from traumatic brain injury, mental retardation, learning disabilities, psychiatric disorders, substance abuse, and dementia. Participants gave informed consent approved by the Institutional Review Board of the University of Iowa.
Scales
Participants were administered the Authoritarianism Scale (AS) and Religious Fundamentalism Scale (RFS) from Altemeyer (Altemeyer & Hunsberger, 1992; Altemeyer & Hunsberger, 2004) and, in addition, four specific religious statements. The AS and RFS have been used extensively and are psychometrically well established (Altemeyer, 1996).
The AS defines authoritarianism as the covariation of three attitudinal clusters: 1) Authoritarian submission, a high degree of submission to authority figures who are perceived to be established and legitimate in society; 2) Authoritarian aggression, a general aggressiveness that is perceived to be sanctioned by established authorities; and 3) Conventionalism, a high degree of adherence to the social conventions that are perceived to be endorsed by society’s authorities. It consists of 30 statements to which patients recorded responses on a 1–5 (Strongly Agree to Strongly Disagree) basis. Fifteen statements were con-trait items where the more authoritarian answer was to disagree.
The RFS defined religious fundamentalism with four dimensions: 1) the belief that there is one set of religious teachings that contains the fundamental, basic, intrinsic, inerrant truth about humanity and deity; 2) this essential truth is opposed to evil which must be actively fought; 3) the truth must be followed today according to the fundamental practices of the past; and 4) that those who follow these fundamental teachings have a special relationship with the deity. It consisted of 12 statements to which patients recorded responses on a 1–5 (Strongly Agree to Strongly Disagree) basis. Six statements were con-trait items where the more fundamentalist answer was to disagree. The balanced items of the scales rule out the possibility that liberal responding, per se, engenders a high authoritarianism or religious fundamentalism score.
To address the question of whether vmPFC damage led to increased specific religious beliefs, we selected four follow-up religious statements and asked the patients to record whether their belief for each specific statement had changed following their brain injury/medical event. Specific belief selection criteria included: 1) Specificity, declarative beliefs which are rooted in the dogmatisms of Christianity; and 2) Generality, beliefs which are common to all Christian denominations.
Procedures
Patients were given a paper version of the scales and asked to record responses in solitude. The scales were administered in a neuropsychological testing room in the Department of Neurology at the University of Iowa Hospitals and Clinics.
Neuroanatomical Analysis
The neuroanatomical analysis of the vmPFC patients (Fig. 1) was based on magnetic resonance data for four patients and on computerized tomography data for six patients. Each patient’s lesion was reconstructed in three dimensions using Brainvox (Frank, Damasio, & Grabowski, 1997). Using the MAP-3 technique, the lesion contour for each vmPFC patient was manually warped into a normal template brain. The overlap of lesions in this volume, calculated by the sum of n lesions overlapping at any single voxel, is color-coded in Figure 1. Neuroanatomical analysis of BDC patients was conducted with magnetic resonance data for seven patients and computerized tomography data for three patients. BDC lesions were analyzed qualitatively on a case-by-case basis.
RESULTS
Across all the patients tested (n = 36), authoritarianism was significantly correlated with religious fundamentalism, r = 0.78, p = 0.001. This finding is consistent with previous research (Altemeyer & Hunsberger, 2004) suggesting a degree of overlap between the constructs of authoritarianism and of religious fundamentalism.
VMPFC patients reported higher authoritarianism (M = 3.45, SE = 0.15) than BDC patients (M = 2.68, SE = 0.20) and MC patients (M = 2.67, SE = 0.22) (Fig. 2). VMPFC patients also reported higher religious fundamentalism (M = 3.73, SE = 0.29) than BDC patients (M = 2.25, SE = 0.24) and MC patients (M = 2.50, SE = 0.24) (Fig. 2). Since authoritarianism and religious fundamentalism were correlated, we analyzed the data with a MANOVA. The MANOVA revealed a significant effect of group on authoritarianism and religious fundamentalism, Wilks’ λ = 0.67, F(4, 64) = 3.63, p = 0.01, partial η2 = 0.19. Simple contrasts showed that vmPFC patients reported significantly higher authoritarianism than BDC patients (p = 0.02) and MC patients (p = 0.01), and significantly higher religious fundamentalism than BDC patients (p = 0.001) and MC patients (p = 0.002). To explore the external validity of the authoritarianism result, we obtained AS data from Wegmann (1992) to compare our values to individuals from the general population. After correcting for scale differences in the normative data (M = 2.78, SE = 0.13) (Fig. 2), t-tests revealed no significant differences between BDC and normal subjects, t(37) = 0.39, p = 0.70, d = 0.14, or between MC patients and normal subjects, t(43) = 0.45, p = 0.66, d = 0.14. However, vmPFC patients reported significantly higher authoritarianism than normal subjects, t(37) = 2.86, p = 0.01, d = 1.05. In parallel, for a broader perspective to the religious fundamentalism result, we obtained RFS normative data from Altemeyer (Altemeyer & Hunsberger, 2004). After correcting for scale differences in the normative data, (M = 2.62, SE = 0.05) (Fig. 2), t-tests revealed no significant differences between BDC patients and normal subjects, t(432) = 1.14, p = 0.25, d = 0.36, or between MC patients and normal subjects, t(438) = 0.47, p = 0.64, d = 0.12. However, vmPFC patients reported significantly higher religious fundamentalism than normal subjects, t(432) = 3.46, p = 0.001, d = 1.11.
Fig. 2.

Authoritarianism and religious fundamentalism mean scores. Authoritarianism is represented by the AS and religious fundamentalism by the RFS, respectively. Error bars indicate SEM. For an external validity indicant, we obtained normative data from two different sources: Wegmann (1992) provided the AS normative group (Normal 1; n = 29) and Altemeyer (Altemeyer & Hunsberger, 2004) provided the RFS normative group (Normal 2; n = 424). For both the AS and RFS, the vmPFC group had significantly higher mean scores than the BDC, MC, and the normative groups.
We conducted a follow-up analysis in which we removed items on the AS scale that explicitly mentioned topics of religion (Items 3, 4, 18, 20, 21). This yielded significant differences between the groups, with the vmPFC group having higher authoritarian scores than the BDC and MC groups, F(2, 33) = 3.42, p = 0.045, η2 = 0.17. This suggests that vmPFC patients did not score high on the AS scale simply because of religion-related item content, but instead, gave more authoritarian answers to all manner of the items.
Although our vmPFC patients had generally intact intelligence and executive functioning (Table 1), we were interested in exploring whether our authoritarianism and fundamentalism results could be explained by a broader disruption of cognition. Across all of the brain-damaged patients, there were no significant relationships between authoritarianism and IQ test (WAIS) scores, τ = −0.26, p = 0.12; WCST perseverative errors, τ = −0.08, p = 0.65; or Stroop interference scores, τ = 0.05, p = 0.77. Similarly, there were no significant relationships between religious fundamentalism and IQ test (WAIS) scores, τ = −0.05, p = 0.75; WCST perseverative errors, τ = 0.04, p = 0.79; or Stroop interference scores, τ = 0.20, p = 0.25. These data support the conclusion that high authoritarianism and religious fundamentalism cannot be explained by a general disruption of intelligence or executive functioning.
The final question was whether vmPFC damage led to increases in specific declarative religious beliefs. On the four specific religious belief items, the vmPFC patients (data available for nine vmPFC patients) reported greater increases in the specific religious beliefs (M = 3.58, SE = 0.24) than BDC patients (M = 2.95, SE = 0.03) and MC patients (M = 3.14, SE = 0.08). A one-way ANOVA revealed a significant effect of group on belief change, F(2, 32) = 5.37, p = 0.01, η2 = 0.25. The changes in the vmPFC group on belief change are illustrated by observations from patient 3534’s husband of 51 years. He reported that his wife’s belief in God was much stronger following her brain injury; she was a “new” person who is now a “strong believer in God and Heaven” and “feels overwhelmed that God did so many miracles.”
DISCUSSION
We found that patients with focal damage to the ventromedial prefrontal cortex (vmPFC) reported higher levels of authoritarianism and religious fundamentalism than neurological comparison patients with damage outside the vmPFC (and other emotion-related structures), and medical comparison patients who had been through a life-threatening (but non-neurological) medical event. Moreover, vmPFC patients reported greater increases in specific religious beliefs following their brain injury. The conclusion that vmPFC damage caused religious beliefs to increase is bolstered by the facts that 1) experiencing a profound, life-threatening medical event, per se, does not account for the results (as evident from the MC data); and 2) brain damage, per se, when outside the vmPFC and other neural structures mediating emotion, does not account for the results (as evident from the BDC data). Our findings support the False Tagging Theory, which posits that the prefrontal cortex is critical in mediating doubt, and thus damage to the prefrontal cortex should result in a “doubt deficit.” There are two potential mechanisms by which specific beliefs could have been increased after prefrontal damage in the FTT model, both plausible and not mutually exclusive: 1) the fictile state account, where following exposure to religious propositions after brain damage, the patient is poor at tagging new religious notions as false, leading to increased beliefs; and 2) the damaged doubt records account, where prefrontal cortex damage selectively destroys existing dispositional doubt records of religious beliefs, thereby increasing beliefs. The FTT suggests that, in effect, prefrontal cortex damage can cause individuals to become more fundamentalist and to hold more extreme religious views, predictions the current data support. However, we would not expect that vmPFC patients’ susceptibility to dogmatic beliefs would be confined to or specific for religious tenets (Harris, Kaplan, Curiel, Bookheimer, Iacoboni et al., 2009). For example, we would predict other dogmatic beliefs frequently espoused by perceived authorities to be higher in vmPFC patients, such as nationalistic, prejudicial, and contemporary social beliefs (Peterson, Doty, & Winter, 1993). Further work examining belief specificity will be crucial for the FTT.
Another convergent line of evidence comes from developmental populations, who tend to have high religious beliefs. The prefrontal cortex in children is disproportionately underdeveloped in comparison to other brain regions (Dempster, 1992; Giedd, Blumenthal, Jeffries, Castellanos, Liu et al., 1999), and frontal lobe functioning improves from infancy to adulthood (Diamond, 2002). Children are also credulous and gullible, with a tendency to accept propositions uncritically (Bruck & Ceci, 1999; Ceci, Ross, & Toglia, 1987). Thus, in accordance with our FTT, religious belief is high in childhood, but tends to decrease in adolescence (Francis, 1989; Gibson, 1989). Moreover, deference to authority is a common rationale for moral judgments in children; such deference decreases in adolescence (Colby & Kohlberg, 1987). At the other end of the developmental spectrum, the structural integrity of the prefrontal cortex in older adults is can be disproportionately diminished relative to other brain regions (Pfefferbaum, Adalsteinsson, & Sullivan, 2005; Raz, Gunning, Head, Dupuis, McQuain et al., 1997), with a decline in frontal lobe functioning (Phillips, MacPherson, & Dalla Sala, 2002; West, 1996). Older adults tend to be more credulous than younger adults (Chen, 2007), and older adults have been shown to be more vulnerable to deceptive advertising than younger adults (Denburg, Cole, Hernandez, Yamada, Tranel et al., 2007). In older adults, there are greater religious beliefs compared to younger adults (Argyle & Beit-Hallahmi, 1975; Hunsberger, 1985), which supports our theorizing. Moreover, authoritarianism tends to increase with age as well (Altemeyer, 1996).
Our findings indicate that vmPFC damage increased authoritarianism, as measured by a psychometric attitudinal scale. Beyond this scale, behavioral and experimental evidence suggests that vmPFC patients exhibit characteristics similar to those often seen in healthy individuals with high authoritarianism and fundamentalism. Healthy individuals high in authoritarianism demonstrate diminished empathy and guilt (Altemeyer, 1996), increased punitive judgments (Altemeyer, 1996), and increased endorsement of immoral, hurtful actions (Altemeyer, 1996; Hing, Bobocel, Zanna, & McBride, 2007). VMPFC patients have acquired deficits in empathy and guilt, tend to manifest punitive behavior (Koenigs & Tranel, 2007), and often endorse moral violations (Koenigs, Young, Adolphs, Tranel, Cushman et al., 2007; Young, Bechara, Tranel, Damasio, Hauser et al., 2010) (see also Table 1). Reflecting their decreased empathy, healthy authoritarians are also profoundly egocentric (Altemeyer, 1996) as most prominently illustrated by their blindness to their own faults and vices (Altemeyer, 1996); likewise, vmPFC patients are notable for being egocentric (Damasio et al., 2011) and having poor insight into their own deficits (Anderson & Tranel, 1989) (Table 1). In sum, the behavioral and personality profile of patients with damage to the vmPFC is strongly reminiscent of authoritarian individuals, consistent with the interpretation that prefrontal damage increases authoritarianism and fundamentalism. This profile arises in the absence of deficits in general intelligence or working memory (Table 1), consistent with the finding that healthy authoritarians have intact general intelligence (Altemeyer, 1996); and even arises in the absence of deficits on putative frontal lobe functioning or executive functioning tests (Table 1). Thus, the increase in authoritarianism and fundamentalism is not due to a general cognitive or executive functioning deficit per se.
The FTT proposes that, in the final analysis, a disruption in the false tagging mechanism can account for the behavioral and personality profile of vmPFC patients (Asp & Tranel, 2012), which is distinctly authoritarian. The vmPFC patients’ abnormal social behaviors (Damasio, 1994) and relative social disinhibition are the direct result of a defective false tagging or doubting mechanism, where the false tagging mechanism filters potential inappropriate response representations in post-rolandic cortices. Thus, the doubting mechanism is an elaborate response selection device that biases the individual away from inappropriate response representations.
This initial empirical foray into the neural basis of authoritarianism suggests that the vmPFC plays a critical role in the resistance of authoritarian persuasion intent on injuring others. Our results extend previous work reporting increased aggression following damage to the frontal lobe (Giancola, 1995; Grafman, Schwab, Warden, Pridgen, Brown et al., 1996), and suggest this hostility may be readily harnessed by perceived authority figures. Behavioral paradigms in vmPFC patients measuring tractability toward authority and aggression against individuals would provide further tests of these findings. Of interest in this context are some recent investigations utilizing a virtual simulation of Milgram’s (1974) obedience paradigm, which have shown activations in the vmPFC (Cheetham, Pedroni, Antley, Slater, & Jäncke, 2009) and increased autonomic responses (Slater, Antley, Davison, Swapp, Guger et al., 2006) when healthy subjects observed the virtual Learner in pain. Indeed, Milgram’s (1974) infamous account of the unemotional Mr. Batta passively forcing the Learner’s hand on the shock plate with indifference raises an intriguing parallel with vmPFC patients characterized by blunted emotions (Damasio et al., 2011) and stagnant autonomic responses to provocative social stimuli (Damasio, Tranel, & Damasio, 1990).
Our study has limitations. Sample size is one issue—although we would hasten to point out that our N’s are reasonably high for studies of this type, which rely on rare neurological patients. Moreover, the main analyses reached a power value (1 − β) of 0.90, indicating we had a high probability to find an effect if one existed. Another issue is that vmPFC patients can be inaccurate reporters of their own behavior. However, self-reports of declarative beliefs are distinct from reports about past events, in that vmPFC patients often believe their errant accounts from the past (Gilboa & Moscovitch, 2002). Belief (and doubt) is an online process that is integral for memory searches about past events (Asp & Tranel, 2012). Thus, poor or inaccurate self-reporting of the past does not imply anything false about the patients’ declarative beliefs at a particular moment. To address this issue more fully, we attempted to obtain collateral information from family members and close friends to corroborate the increased religiosity/authoritarianism of vmPFC patients, but low compliance in returning the questionnaires precluded analysis of these data. Moreover, religious belief knowledge obtained from collateral sources may not be very definitive anyway, since personal declarative beliefs are inherently private and subjective phenomena.
It should be emphasized that the notion that vmPFC damage leads to a bias to accept and believe more religious dogmatisms does not mean that individuals high in authoritarianism or religious fundamentalism have some kind of “dysfunction” in the vmPFC. A wide diversity of experiences and influences act on differing personalities to guide each individual to a particular religious belief landscape. At a group level, some experiences can lead to a decrease in religious beliefs, while others can lead to an increase in religious beliefs. Thus, while we are suggesting that damage to the vmPFC may lead to an increase in religious beliefs, it is certainly true that individuals without vmPFC dysfunction acquire religious beliefs and doubts for a range of reasons, entirely independent of brain integrity.
To conclude, the present findings suggest that the vmPFC is a critical neural substrate for psychological doubt affecting post-rolandic cognitive representations, where damage to the vmPFC acts to increase religious beliefs and submissiveness to authority figures.
Acknowledgments
This study was supported by grants from the National Institutes of Health (NINDS P50 NS19632 and NIDA R01 DA 022549). We thank Emily Johnson, Mallory Small, and Elizabeth Mullens for assistance compiling the scales and inputting the data, Joel Bruss for assistance with the neuroanatomy figure, Dr. Antonio Damasio for discussion of the central theoretical ideas in the paper, Dr. Timothy Koscik and Dr. Michael Koenigs for Table data, and Dr. Diana Cates and Dr. Natalie Denburg for guidance and expertise. We give a special thanks to Dr. Bob Altemeyer and Dr. Mary Wegmann for the normative data.
Footnotes
The authors declare no conflict of interest.
References
- Adorno TW, Frenkel-Brunswik E, Levinson DJ, Sanford RN. The Authoritarian Personality. New York: Harper & Row Publishers; 1950. [Google Scholar]
- Altemeyer B. The Authoritarian Specter. Cambridge, MA: Harvard University Press; 1996. [Google Scholar]
- Altemeyer B, Hunsberger B. Authoritarianism, religious fundamentalism, quest, and prejudice. The International Journal for the Psychology of Religion. 1992;2:113–133. [Google Scholar]
- Altemeyer B, Hunsberger B. A revised religious fundamentalism scale: The short and sweet of it. The International Journal for the Psychology of Religion. 2004;14:47–54. [Google Scholar]
- Anderson SW, Tranel D. Awareness of disease states following cerebral infarction, dementia, and head trauma: Standardized assessment. The Clinical Neuropsychologist. 1989;3:327–339. [Google Scholar]
- Argyle M, Beit-Hallahmi B. The social psychology of religion. Boston: Routledge & Kegan Paul; 1975. [Google Scholar]
- Asp EW, Manzel K, Koestner B, Cole CA, Denburg NL, Tranel D. A neuropsychological test of belief and doubt: Damage to ventromedial prefrontal cortex increases credulity for misleading advertising. Frontiers in Decision Neuroscience. doi: 10.3389/fnins.2012.00100. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Asp EW, Tranel D. False Tagging Theory: Toward a unitary account of prefrontal cortex function. In: Stuss DT, Knight RT, editors. Principles of Frontal Lobe Function. 2. New York: Oxford University Press; 2012. [Google Scholar]
- Barrash J, Tranel D, Anderson SW. Acquired personality disturbances associated with bilateral damage to the ventromedial prefrontal region. Developmental Neuropsychology. 2000;18:355–381. doi: 10.1207/S1532694205Barrash. [DOI] [PubMed] [Google Scholar]
- Bruck M, Ceci SJ. The suggestibility of children’s memory. Annual Review of Psychology. 1999;50:419–439. doi: 10.1146/annurev.psych.50.1.419. [DOI] [PubMed] [Google Scholar]
- Ceci SJ, Ross DF, Toglia MP. Suggestibility of children’s memory: Psycholegal implications. Journal of Experimental Psychology: General. 1987;116:38–49. [Google Scholar]
- Cheetham M, Pedroni AF, Antley A, Slater M, Jäncke L. Virtual milgram: Empathic concern or personal distress? Evidence from functional MRI and dispositional measures. Frontiers in human neuroscience. 2009;3:1–13. doi: 10.3389/neuro.09.029.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen YW. Age differences in social judgments: Why are old adults more susceptible to scams. In: Columbus A, editor. Advances in Psychology Research. Vol. 38. Nova Science Publishers; 2007. pp. 145–161. [Google Scholar]
- Colby A, Kohlberg L. The measurement of moral judgment. I. Cambridge: Cambridge University Press; 1987. [Google Scholar]
- Croft K, Duff M, Kovach C, Anderson SW, Adolphs R, Tranel D. Detestable or marvelous? Neuroanatomical correlates of character judgments. Neuropsychologia. 2010;48:1789–1801. doi: 10.1016/j.neuropsychologia.2010.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Damasio A. Decartes’ Error: Emotion, Reason and the Human Brain. New York: Grosset/Putnam; 1994. [Google Scholar]
- Damasio AR, Anderson SW, Tranel D. The frontal lobes. In: Heilman KM, Valenstein E, editors. Clinical Neuropsychology. 5. New York: Oxford University Press; 2011. [Google Scholar]
- Damasio AR, Tranel D, Damasio H. Individuals with sociopathic behavior caused by frontal damage fail to respond autonomically to social stimuli. Behavioural Brain Research. 1990;41(2):81–94. doi: 10.1016/0166-4328(90)90144-4. [DOI] [PubMed] [Google Scholar]
- Dempster FN. The rise and fall of the inhibitory mechanism: Toward a unified theory of cognitive development and aging. Developmental Review. 1992;12:45–75. [Google Scholar]
- Denburg NL, Cole CA, Hernandez M, Yamada TH, Tranel D, Bechara A, et al. The Orbitofrontal Cortex, Real-World Decision Making, and Normal Aging. Annals of the New York Academy of Sciences. 2007;1121(1):480–498. doi: 10.1196/annals.1401.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diamond A. Normal development of prefrontal cortex from birth to young adulthood: Cognitive functions, anatomy, and biochemistry. In: Stuss DT, Knight RT, editors. Principles of frontal lobe function. New York: Oxford University Press; 2002. pp. 466–503. [Google Scholar]
- Elliott R, Rees G, Dolan RJ. Ventromedial prefrontal cortex mediates guessing. Neuropsychologia. 1999;37:403–411. doi: 10.1016/s0028-3932(98)00107-9. [DOI] [PubMed] [Google Scholar]
- Fletcher PC, Anderson JM, Shanks DR, Honey R, Carpenter TA, Donovan T, et al. Responses of human frontal cortex to surprising events are predicted by formal associative learning theory. Nature Neuroscience. 2001;4:1043–1048. doi: 10.1038/nn733. [DOI] [PubMed] [Google Scholar]
- Francis LJ. Drift from the churches: Secondary school pupils’ attitudes toward Christianity. British Journal of Religious Education. 1989;11:76–86. doi: 10.1111/j.2044-8279.1989.tb03079.x. [DOI] [PubMed] [Google Scholar]
- Frank RJ, Damasio H, Grabowski TJ. Brainvox: An Interactive, Multimodal Visualization and Analysis System for Neuroanatomical Imaging. Neuroimage. 1997;5(1):13–30. doi: 10.1006/nimg.1996.0250. [DOI] [PubMed] [Google Scholar]
- Giancola PR. Evidence for dorsolateral and orbital prefrontal cortical involvement in the expression of aggressive behavior. Aggressive Behavior. 1995;21(6):431–450. [Google Scholar]
- Gibson HM. Attitudes to Religion and Science Among Schoolchildren Aged 11 to 16 Years in a Scottish City. Journal of Empirical Theology. 1989;2:5–26. [Google Scholar]
- Giedd JN, Blumenthal J, Jeffries NO, Castellanos FX, Liu H, Zijdenbos A, et al. Brain development during childhood and adolescence: A longitudinal MRI study. Nature Neuroscience. 1999;2:861–863. doi: 10.1038/13158. [DOI] [PubMed] [Google Scholar]
- Gilbert DT. How mental systems believe. American Psychologist. 1991;46(2):107–119. [Google Scholar]
- Gilbert DT, Tafarodi RW, Malone PS. You Cant Not Believe Everything You Read. Journal of Personality and Social Psychology. 1993;65(2):221–233. doi: 10.1037//0022-3514.65.2.221. [DOI] [PubMed] [Google Scholar]
- Gilboa A, Moscovitch M. The cognitive neuroscience of confabulation: A review and a model. In: Baddeley AD, Kopelman MD, Wilson BA, editors. Handbook of Memory Disorders. 2. Chichester (UK): John Wiley; 2002. pp. 315–342. [Google Scholar]
- Grafman J, Schwab K, Warden D, Pridgen A, Brown HR, Salazar AM. Frontal lobe injuries, violence, and aggression. Neurology. 1996;46(5):1231. doi: 10.1212/wnl.46.5.1231. [DOI] [PubMed] [Google Scholar]
- Harris S, Kaplan JT, Curiel A, Bookheimer SY, Iacoboni M, Cohen MS. The neural correlates of religious and nonreligious belief. PLoS ONE. 2009;4(10):1–9. doi: 10.1371/journal.pone.0007272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris S, Sheth SA, Cohen MS. Functional neuroimaging of belief, disbelief, and uncertainty. Annals of Neurology. 2008;63:141–147. doi: 10.1002/ana.21301. [DOI] [PubMed] [Google Scholar]
- Hing LSS, Bobocel DR, Zanna MP, McBride MV. Authoritarian dynamics and unethical decision making: High social dominance orientation leaders and high right-wing authoritarianism followers. Journal of Personality and Social Psychology. 2007;92:67–81. doi: 10.1037/0022-3514.92.1.67. [DOI] [PubMed] [Google Scholar]
- Hunsberger B. Religion, Age, Life Satisfaction, and Perceived Sources of Religiousness: A Study of Older Persons. Journal of Gerontology. 1985;40(5):615–620. doi: 10.1093/geronj/40.5.615. [DOI] [PubMed] [Google Scholar]
- Ingersoll-Dayton B, Krause N, Morgan D. Religious trajectories and transitions over the life course. The International Journal of Aging and Human Development. 2002;55:51–70. doi: 10.2190/297Q-MRMV-27TE-VLFK. [DOI] [PubMed] [Google Scholar]
- Koenigs M, Tranel D. Irrational economic decision-making after ventromedial prefrontal damage: Evidence from the ultimatum game. The Journal of Neuroscience. 2007;27:951–956. doi: 10.1523/JNEUROSCI.4606-06.2007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koenigs M, Young L, Adolphs R, Tranel D, Cushman F, Hauser M, et al. Damage to the prefrontal cortex increases utilitarian moral judgements. Nature. 2007;446:908–911. doi: 10.1038/nature05631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milgram S. Obedience to authority. New York: Harper & Row Publishers; 1974. [Google Scholar]
- Parris BA, Kuhn G, Mizon GA, Benattayallah A, Hodgson TL. Imaging the impossible: An fMRI study of impossible causal relationships in magic tricks. NeuroImage. 2009;45(3):1033–1039. doi: 10.1016/j.neuroimage.2008.12.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peterson BE, Doty RM, Winter DG. Authoritarianism and attitudes toward contemporary social issues. Personality and Social Psychology Bulletin. 1993;19(2):174–184. [Google Scholar]
- Pfefferbaum A, Adalsteinsson E, Sullivan EV. Frontal circuitry degradation marks healthy adult aging: Evidence from diffusion tensor imaging. NeuroImage. 2005;26(3):891–899. doi: 10.1016/j.neuroimage.2005.02.034. [DOI] [PubMed] [Google Scholar]
- Phillips LH, MacPherson SES, Dalla Sala S. Age, cognition and emotion: The role of anatomical segregation in the frontal lobes. In: Grafman J, editor. Handbook of Neuropsychology. Vol. 7. Amsterdam: Elsevier; 2002. pp. 73–97. [Google Scholar]
- Raz N, Gunning FM, Head D, Dupuis JH, McQuain J, Briggs SD, et al. Selective aging of the human cerebral cortex observed in vivo: Differential vulnerability of the prefrontal gray matter. Cerebral Cortex. 1997;7(3):268–282. doi: 10.1093/cercor/7.3.268. [DOI] [PubMed] [Google Scholar]
- Slater M, Antley A, Davison A, Swapp D, Guger C, Barker C, et al. A virtual reprise of the Stanley Milgram obedience experiments. PLoS ONE. 2006;1(1):e39. doi: 10.1371/journal.pone.0000039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stuss DT, Benson DF. Neuropsychological studies of the frontal lobes. Psychological Bulletin. 1984;95(1):3–28. [PubMed] [Google Scholar]
- Wegmann MF. Information processing deficits of the authoritarian mind. The Fielding Institute; Santa Barbara, CA: 1992. [Google Scholar]
- West RL. An Application of Prefrontal Cortex Function Theory to Cognitive Aging. Psychological Bulletin. 1996;120(2):272–292. doi: 10.1037/0033-2909.120.2.272. [DOI] [PubMed] [Google Scholar]
- Young L, Bechara A, Tranel D, Damasio H, Hauser M, Damasio A. Damage to ventromedial prefrontal cortex impairs judgment of harmful intent. Neuron. 2010;65:845–851. doi: 10.1016/j.neuron.2010.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]