

Summary
Background:
Sarcoidosis is a systemic and multiorgan disease with unknown etiopathogenesis. Granulomas that do not undergo necrosis and caseous degeneration are distinctive for this disease. Mostly it is connected with young adults, more frequently females than males, and changes are mainly situated in the lymph nodes of the pulmonary hilus and pulmonary parenchyma. Somatotropin release inhibiting hormone receptors could be located in epithelioid and giant cells that create sarcoidal tubercles and lymph nodes.
Aim of the study was to determine the usefulness of a single photon emission tomography (SPECT) for an evaluation of the range of sarcoidal changes in the chest after using a receptor tracer. An assumption was made that scintigraphy with the use of Tc-99m-Depreotide could help with location of extrapulmonary sarcoidosis focuses.
Material/Methods:
Authors present five patients with clinically recognized and histopathologically confirmed sarcoidosis. Patients were given Tc-99m-Depreotide and underwent SPECT of chest. The results were compared with X-rays of these patients chests and with the accumulation of radiotracer in 2 other patients with carcinoid syndrome without visible pathological changes in examination.
Patients got an intravenous injection of 500 MBq (14mCi) Tc-99m-Depreotide. SPECT of chest together with a “whole body” examination, was performed after 2 hours and 24 hours.
Results:
Higher radiotracer accumulation was observed in all patients in the area of some chest lymph nodes, in pulmonary tissue in 3 patients and in other groups of lymph nodes in 2 patients.
Conclusions:
Emission Tomography of the chest with the use of receptor radiotracer (Tc-99m-Depreotide) can be a crucial complement of sarcoidosis diagnostics in an evaluation of the extent of lung changes together with an estimation of chest lymph nodes abnormalities.
Keywords: sarcoidosis, depreotide, SPECT
Background
Sarcoidosis is a long-lasting, general disease of unknown etiology with characteristic non-caseous granulomas that could occur in different organs in patients of various age, sex, and race [1–4]. The organ most frequently changed, nearly 90% cases, are the lungs. However, granulomas disappear over 2–5 years in over 60% of patients, though in some cases granulomas get fibrinous and that can seriously impair lungs activity [5]. Frequently, in the course of sarcoidosis, changes are spotted in lymph nodes, particularly mediastinal ones, especially in paratracheal and hiluses of lymph nodes. Also, peripheral nodes particularly cervical, axillar, inguinal are often increased. Changes in the area of eyes, skin, hepar, spleen, heart, central nervous system and other organs can accompany pulmonary symptoms [3,6–8].
Prognosis in sarcoidosis depends on, among others, level and form of progression, therefore early diagnosis with an evaluation of the level of changes influences treatment efficacy and increases patients’ life comfort.
Radiological methods are moreover used in imaging for diagnostic purposes: X-ray images and computed tomography (CT), especially high resolution computed tomography (HRCT). In nuclear medicine, after finding somatotropin release inhibiting hormone receptors in epithelioid and giant cells of sarcoidal nodules, one applies analogues of somatotropin release inhibiting hormone into scintigraphic imaging. Before they were marked by I-123 and In-111, but nowadays depreotide combined with Tc-99m is used.
Aim
The aim of the study was to evaluate a single photon emission tomography (SPECT) according to the extent of sarcoidal changes in the chest after application of the tracer for receptor (Tc-99m-Depreotide scintigraphy). Scintigraphy with use of Tc-99m-Depreotide was applied to locate focuses of extrapulmonary sarcoidosis in “whole body” examination.
Material and Methods
The material was 5 patients (3 females and 2 males) aged 28–52, with sarcoidosis diagnosed clinically and confirmed histopathologically. Increased lymph nodes of pulmonary hiluses, also changes in pulmonal parenchyma in 3 patients, were established by X-ray images of chest and in HRCT examination.
Scintigraphic examinations were performed with a one head gammacamera. Technical parameters of equipment: rectangular crystal. Range of detector: 39×53, diameter of detector: 65, number of photomultipliers: 59. Low energy high resolution collimator was used.
SPECT of chest was performed after 2 and 24 hours after intravenous injection of 500 MBq (14mCi) Tc-99m-Depreotide (64 projections, head rotation of 360 degrees). Acquisition was performed in a matrix of 128×128 pixels. “Whole body” examination was conducted on every patent, also after 2 and 24 hours.
Results and Discussion
In our material, including 5 patients, all of them had established histopathological diagnosis and changes in lungs were visible in X-ray images (Figure 1). Evaluation of the extent of intraparenchymal changes of lungs and the involvement of pulmonary hiluses and mediastinal lymph nodes was possible with use of SPECT of the chest, after application of Tc-99m-Depreotide. Changes in lungs were detected in all patients, and in 3 of them pathological accumulation of radiotracer in different groups of lymph nodes of the chest were diagnosed (Figure 2). “Whole body” examinations performed with patients enabled location of changes in cervical, subclavicular, supraclavicular lymph nodes and in the inguinal area in 2 patients (Figure 3). Pathological accumulation of radioisotope was noticed in the area of elbow, knee and wrist joints in one patent.
Figure 1.

X-ray image of chest in p-a projection. Patient aged 52 with sarcoidosis diagnosed several months previously, no ailments at present, admitted to hospital for further examination to evaluate disease activity. Increased interstitial changes of lungs, in middle-upper pulmonary fields, partially fusing.
Figure 2.
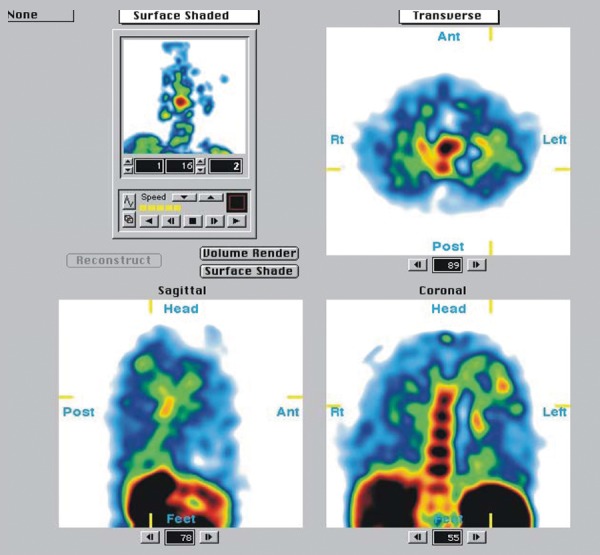
SPECT of chest. Increased uptake of radiotracer in both lungs, especially in left subclavicular field and in area of left hilus.
Figure 3.
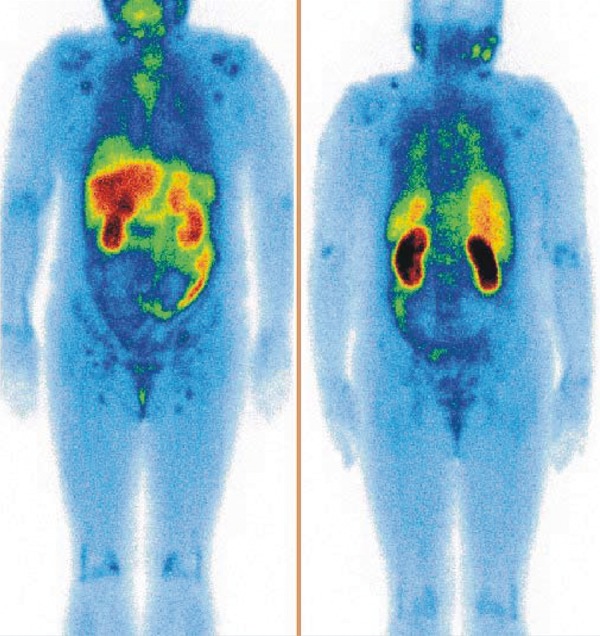
Whole body examination. Patient aged 52 referred to hospital, due to sarcoidal changes in the skin of shoulders and trunk, that had persisted for 2 years, in order to evaluate progression of the disease and to schedule treatment. Increased accumulation of radiotracer in lymph nodes of sub and supraclavicular areas, around neck, both armpits and in areas of the groin is visible. Increased accumulation is also observed in areas of elbow, wrist and knee joints.
Early treatment of sarcoidosis can prevent organs becoming fibrinous [5,9]. Positive diagnosis of this disease can be obtained by biopsy of the suspected organ [10]. X-ray imaging of chest and HRCT are performed according to radiological examinations, and the stage of sarcoidosis can be determined, on this basis, in nearly 92% of patients.
In scintigraphic examination Ga-67 is traditionally used especially to detect extrapulmonary focuses and changes in lymph nodes [3,5]. The main drawback of Ga-67 scintigraphy is high radiation of background caused by physiological accumulation in liver, spleen, bone marrow, lacrimal glands, salivary glands, pectoral glands and lungs that causes some difficulties with location of small uptake changes. In a multicentre examination including over 600 patients, on average, increased uptake of Ga-67 was not observed in 25% of examined patients, despite the fact that the lungs were diseased according to X-ray images. It was concluded that Ga-67 scintigraphy is not more valuable than using more easily available and conducted X-ray examinations and spirometry according to the aforementioned information [3].
Somatotropin release inhibiting hormone analogues constitute an alternative for Ga-67. Somatotropin release inhibiting hormone [SS] consists of two different polypeptides of 14 and 28 aminoacids: SS-14 and SS-28 [1,5]. SS can be found in many places in the human organism: central nervous system, digestive system and endocrine glands are main centres of production [1,5]. In human organism SS primarily inhibits, particularly in connection with processes like the release of hormones [5]. This peptide can function as a neurotransmitter or neurohormone in the central nervous system, though in peripheral tissues it is, among others, a modulator of motor activity of the gastrointestinal passage [1]. SS works through seven membrane receptors of the protein G family, from which five different subtypes hale been cloned so far [1,11]. Both natural ligands, SS-14 and SS-28 show a strong ability to bind to all five subtypes of receptors [11]. Octreotide, an SS analogue, is a peptide of eight aminoacids. Scintigraphic examinations using SS analogues were supposed primarily to be used in evaluation of neuroendocrinal tumors [3]. Receptors of SS turned out to undergo expression also in other malignant neoplasms and inflammations [3,12]. SS receptors were located at epithelicid and giant cells surfaces, that create granulomas [1,5,13]. Receptors were defined as subtypes sst2 and sst5 on the basis of their affinity to the SS analogue – Octreotide. There are two forms of the sst2 receptor: sst2A and sst2B. Sst2A receptor shows bigger affinity to the synthetic, metabolically stable SS analogue [1]. I-123-Tyr-Octreotide, and also In-111-Pentetreotide were used to detect neuroendocrinal tumors and their metastases [5,14]. An advantage of In-111-Pentetreotide is, among others, longer physical half-life that enables imaging tumors after 24 hours and 48 hours from injection when interfering background activity is minimalised by clearance rate [15]. Lebtahi examined 18 patients with sarcoidosis using In-111-Pentetreotide and concluded that changes in X-ray images of chest were strictly connected with areas of bigger radiotracer uptake in scintigrams [16]. This author compared scintigraphy with use of In-111-Pentetreotide with Ga-67 in 18 patients suffering from sarcoidosis. Although Ga-67 scintigraphy detected up to ⅔ of organs clinically occupied by a disease process, In-111-Pentetreotide scintigraphy detected up to 83% of changes though [16]. Scintigraphy with use of In-111 seems to be more precise than Ga-67 scintigraphy [14]. Kwekkeboom examined 46 patients with sarcoidosis by means of In-111 scintigraphy and he detected adenopathy and interstitial changes in the lungs of 97% of patients. Moreover, he located new focuses of sarcoidosis in 50% of patients [14]. Uptake of radiotracer decreased in all examined patients after steroid therapy according to control scintigraphy [14].
In diagnostics of lung tumors Tc-99m-Depreotide is used to evaluate the probability of malignancy. Shorr reports that Tc-99m-Depreotide used to evaluated microcellular lung tumors has a sensitivity of 95% and a specificity of 85% [3]. Hamartoma, an acute inflammation and severe granuloma disease, gives falsely positive results [8,17,18].
After performing Tc-99m-Depreotide procedure in sarcoidosis in 22 patients Shorr found an increased uptake in the area of chest in 81.8% of patients [3]. There was no observed increased uptake in the area of the chest in 4 patients, with no changes in X-ray images suggesting sarcoidosis [3]. A close correlation between X-ray examination results and those of SPECT of the chest exists according to Shorr. There appeared to be strong compatibility of diagnoses if the preliminary diagnosis was based on X-ray examination results. When comparing X-ray images with Tc-99m-Depreotide scintigraphy there was full compatibility of diagnoses in 95.5% of cases [3]. He concluded changes in parenchyma of lungs showed in scintigrams (11 patients), were connected with a worsening of lung function. In patients with scintigrams showing interstitial changes, FEV was 68.6±13.9% as opposed to FEV 84.5±10.7% in patients with normal scintigrams. The level of lung deterioration in sarcoidosis can be evaluated on the basis of Tc-99m-Depreotide scintigraphy. Moreover, Shorr diagnosed extrapulmonary sarcoidosis in 4 cases (heart – 2, nervous system – 1, skin – 1) [3].
Kwekkeboom detected changes in the course of sarcoidosis of lungs in 36 of 37 patients (97%) by means of Tc-99m-Depreotide [19]. Patients underwent treatment and scintigraphy was repeated afterwards. Decreased uptake of marked analogue of somatotropin release inhibiting hormone was detected in patients with radiological improvement which suggests Tc-99m-Depreotide scintigraphy could be used in treatment screening [19].
Conclusions
During routine radiological examinations of the chest, from 30% to 60% of cases of lung sarcoidosis are detected by accident with the patients not showing any symptoms. Preliminary detection can contribute to preventing chronic disease [5]. Emission Tomography of the chest with the use of receptor radiotracer (Tc-99m-Depreotide) can be a crucial complement of sarcoidosis diagnostics in an evaluation of the extent of lung changes together with an estimation of chest lymph nodes abnormalities. Scintigraphic examination with the use of Tc-99m-Depreotide can be used to screen disease. Radiotracer scintigraphy can also be used to detect extrapulmonary changes in patients with sarcoidosis[3].
References:
- 1.TenBokum AM, Hofland LJ, de Jong G, et al. Immunohistochemical localization of somatostatin receptor sst2A in sarcoid granulomas. Eur J Clin Invest. 1999;29:630–36. doi: 10.1046/j.1365-2362.1999.00498.x. [DOI] [PubMed] [Google Scholar]
- 2.Jurowski P, Gos R, Kunert-Radek J. Long acting analogue of somatostatin (Octreotide) for treatment of patients with neurochorioretinitis due to ocular sarcoidosis who failed corticosteroids therapy. Klin Oczna. 2002;104:266–69. [PubMed] [Google Scholar]
- 3.Shorr AF, Helman DL, Lettieri CJ, et al. Depreotide scanning in sarcoidosis: a pilot study. Chest. 2004;126:1337–43. doi: 10.1378/chest.126.4.1337. [DOI] [PubMed] [Google Scholar]
- 4.Thomas KW, Hunninghake GW. Sarcoidosis. JAMA. 2003;24:3300–3. doi: 10.1001/jama.289.24.3300. [DOI] [PubMed] [Google Scholar]
- 5.Dalm VA, Van Hagen PM, Krenning EP. The role of octreotide scintigraphy in rheumatoid arthritis and sarcoidosis. Q J Nucl Med. 2003;47:270–78. [PubMed] [Google Scholar]
- 6.Burns TM. Neurosarcoidosis. Arch Neurol. 2003;60:1166–68. doi: 10.1001/archneur.60.8.1166. [DOI] [PubMed] [Google Scholar]
- 7.Kvale PA. Is it difficult to diagnose sarcoidosis? Chest. 2003;123:330–32. doi: 10.1378/chest.123.2.330. [DOI] [PubMed] [Google Scholar]
- 8.Schuster DM, Alazraki N. Gallium and other agents in diseases of the lung. Semin Nucl Med. 2002;32:193–211. doi: 10.1053/snuc.2002.124178. [DOI] [PubMed] [Google Scholar]
- 9.James DG. Sarcoidosis 2001. Postgrad Med J. 2001;77:177–80. doi: 10.1136/pmj.77.905.177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Avram AM, Mackie GC, Schneider BJ, et al. Differentiation between carcinoid and sarcoid with F-18 FDG PET and In-111 pentetreotide. Clin Nucl Med. 2006;31:197–200. doi: 10.1097/01.rlu.0000204200.66112.a9. [DOI] [PubMed] [Google Scholar]
- 11.Patel YC. Somatostatin and its receptor family. Front Neuroendocrinol. 1999;72:746–61. doi: 10.1006/frne.1999.0183. [DOI] [PubMed] [Google Scholar]
- 12.Kwekkeboom DJ, Krenning EP. Somatostatin receptor imaging. Semin Nucl Med. 2002;32:84–91. doi: 10.1053/snuc.2002.31022. [DOI] [PubMed] [Google Scholar]
- 13.Ferone D, Lombardi G, Colao A. Somatostatin receptors in immune system cells. Minerva Endocrinol. 2001;26:165–73. [PubMed] [Google Scholar]
- 14.Kwekkeboom DJ, Krenning EP, de Jong M. Peptide receptor imaging and therapy. J Nucl Med. 2000;41:1704–13. [PubMed] [Google Scholar]
- 15.Oberg K. State of the art and future prospects in the management of neuroendocrine tumors. Q J Nucl Med. 2000;44:3–12. [PubMed] [Google Scholar]
- 16.Lebtahi R, Crestani B, Belmatoug N, et al. Somatostatin receptor scintigraphy and gallium scintigraphy in patients with sarcoidosis. J Nucl Med. 2001;42:21–26. [PubMed] [Google Scholar]
- 17.Baath M, Kolbeck KG, Danielsson R. Somatostatin receptor scintigraphy with 99mTc-Depreotide (NeoSpect) in discriminating between malignant and benign lesions in the diagnosis of lung cancer: a pilot study. Acta Radiol. 2004;45:833–39. doi: 10.1080/02841850410001394. [DOI] [PubMed] [Google Scholar]
- 18.Blum J, Handmaker H, Lister-James J, et al. A multicenter trial with a somatostatin analog 99mTc-Depreotide in the evaluation of solitary pulmonary nodules. Chest. 2000;117:1232–38. doi: 10.1378/chest.117.5.1232. [DOI] [PubMed] [Google Scholar]
- 19.Kwekkeboom DJ, Krenning EP, Kho GS, et al. Somatostatin receptor imaging in patients with sarcoidosis. Eur J Nucl Med. 1998;25:1284–92. doi: 10.1007/s002590050297. [DOI] [PubMed] [Google Scholar]