

Summary
Background:
Acute limb ischaemia’ is a sudden, rapidly progressing inhibition of blood supply to a limb, characterised by appearance of new symptoms or by aggravation of the already existing ones, which may lead to amputation of the limb. Computed tomography angiography (CTA) performed with a multislice scanner belongs to methods used for arterial imaging in acute limb ischaemia. The main advantages of this method include: short examination time, low invasiveness, and possibility of a multiplanar and multivolume imaging of the vessels and adjacent tissues.
Case Reports:
We presented 3 cases of acute posttraumatic ischaemia of the upper limbs, diagnosed in the emergency setting with the use of a 64-slice CT scanner.
Conclusions:
The CTA examination performed with the 64-slice CT unit revealed high effectiveness when used for localisation of vascular pathologies resulting in acute ischaemia of the upper limbs. Owing to this rapid radiological diagnostic method, it is now possible to perform successful limb-saving surgeries and to introduce postoperative monitoring immediately after the procedure.
Keywords: acute ischaemia of the upper limbs, computed tomography angiography, CTA
Background
Acute limb ischaemia (ALI) is a sudden or a rapidly progressing inhibition of blood supply to a limb, characterised by appearance of new symptoms or by aggravation of the already existing ones, such as: pulse loss, paleness, decrease in the limb temperature, impaired touch sensation and loss of motor function of the limbs. No treatment or a delayed treatment of ALI may result in limb amputation. ALI is much more frequent in the lower limbs, being a result of arteriosclerotic lesions. Other causes of lower limb acute ischaemia include an injury or a complication of a vascular procedure [1–3]. A more developed collateral circulation in the upper limbs results in a lower number of acute ischaemia incidents in this anatomical region. Such incidents are mostly due to a thromboembolic mechanism or an injury. Their symptoms are less intense than in the case of lower limb ischaemia [4,5].
A method of growing diagnostic importance in cases of upper limb ischaemia is the computed tomography angiography (CTA), especially since the introduction of multislice (CT) units that allowed for scanning of long body parts, with acquisition of high-resolution images and a very good contrast enhancement of the vessels.
In this work, we reported 3 cases of acute posttraumatic ischaemia of the upper limbs, diagnosed in the emergency setting with the use of the 64-slice CT scanner.
Case Report
Case 1
Patient J.O., aged 46, was admitted to the emergency surgical department due to an acute ischaemic incident affecting the right upper limb and caused by the crush of the right elbow joint with an agricultural machine. An emergency CTA revealed extensive injuries of the structures within the right cubital fossa, including the brachial artery. On examination, there was a correct contrast medium distribution of the right subclavian artery, axillary artery and brachial artery in its proximal and central part. An occlusion of the brachial artery was present from the level of the humeral epicondyle. It was accompanied by a pseudoaneurysm, measuring 17×10 mm, and causing contrast agent extravasation with a large haematoma, up to 3 cm thick, occupying the anterior part of the distal arm, the cubital fossa and the proximal part of the forearm (Figure 1). Forearm arteries were not opacified. An emergency reconstruction of the brachial artery was performed – a fragment of the saphenous vein was sewed in. The patient was subjected to intraoperative consultation by a hand surgery specialist, who recommended fasciotomy. A clinical improvement in limb perfusion was observed.
Figure 1.

Case 1. CTA of the right upper limb – VR reconstruction. Obstruction of the distal part of the brachial artery – with pseudoaneurysm, measuring 17×10 mm, and extensive extravasation of the contrast medium.
Case 2
Patient M.M., aged 31, was admitted to the emergency surgical department due to a partial cut-off of both upper limbs with a window pane. This resulted in acute ischaemia. An emergency CTA showed a bilateral occlusion of the brachial arteries, from the level of ¼ of the distal humeral shafts. In the left upper limb, below the occlusion site, there were dilated vessels of the collateral circulation, without any evident extravasation of the contrast agent. Forearm arteries remained nonopacified bilaterally (Figure 2A). The patient was subjected to an emergency surgery. The left radial and ulnar artery were anastomosed with a venous graft. On the right, the anastomosis of the brachial artery was performed with the use of a venous graft. Due to an increasing oedema of the right upper limb, a follow-up postoperative CTA examination was carried out (Figure 2B). It showed ulnar artery, in its whole length, and the radial artery narrowed, with a threadlike lumen from the point of its origin, visible till the half of the forearm only. After the examination, the right limb was operated on again. There was a clinical improvement of limb perfusion during patient’s hospitalisation.
Figure 2A.
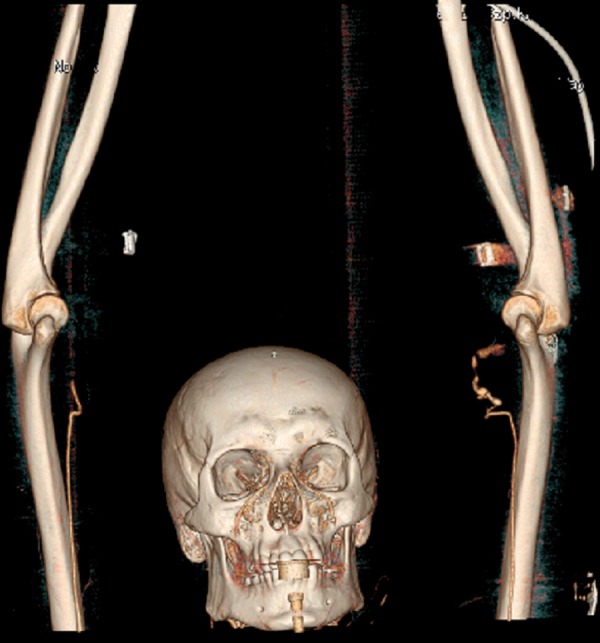
Case 2. CTA of both upper limbs – VR reconstruction. Occlusion of the right and left brachial artery – VR reconstruction.
Figure 2B.

Case 2. Follow-up postoperative CTA – VR reconstruction. Ulnar artery visualised in its whole length, and the radial artery is narrowed from the origin (threadlike lumen), visible till the half of the forearm only.
Case 3
Patient J.J., aged 60, was admitted to the emergency surgical department due to acute ischaemia of the left upper limb, resulting from an injury caused by an agricultural machine. The emergency CTA showed noncontrastet 40 mm segment of the brachial artery, at the level of the distal humerus and the elbow joint (Figure 3). Forearm arteries were normally contrasted via collateral circulation. The patient was operated on in an emergency setting. The part of the left brachial artery was reconstructed with a venous graft, which resulted in a clinical improvement and, finally, in a normal perfusion of the limb.
Figure 3.

Case 3. CTA of the left upper limb – CPR reconstruction. No contrast enhancement in the distal part of the brachial artery, for approx. 40 mm. Contrast enhancement of the forearm arteries.
Discussion
Computed tomography angiography with the use of multislice scanners (especially the 64-slice ones) becomes an excellent tool for arterial imaging [1]. Application of multiple rows of detectors, with a fast scanning rate and a high, sometimes also isotropic, resolution, led to the situation in which all previous limitations connected with the use of CT scanners of an older type were surmounted. Due to the advances in the development of CT scanners, the CTA examination was included in the diagnostic protocol of acute limb ischaemia, as a result of a TransAtlantic Inter-Society Consensus (TASC-II) in 2008 [2,3].
Interruption of transarterial blood flow caused by arterial occlusion or narrowing, leads to a decreased tissue perfusion, which may, in a long run, cause the loss of the limb. In upper limb injuries leading to ischaemia, it is especially important to precisely locate the site of the vessel trauma [4,6]. Owing to rapid diagnostics, it is now possible to immediately introduce an appropriate treatment, which improves the prognosis of limb survival.
Until recently, the basic method of arterial diagnostics was a standard arteriography. Despite its substantial precision, it is also highly invasive and expensive, and requires a group of specialised operators to perform it, which considerably increases the time of the procedure. A completely non-invasive Doppler ultrasonography technique is, on the other hand, much less sensitive than the CTA or the arteriography, and depends on the class of the applied unit, as well as on the experience of the operator. Another minimally invasive method, i.e. MRI angiography, is not frequently performed in the diagnostics of acute posttraumatic limb ischaemia, due to the long examination time and a relatively low availability [7,8].
Nowadays, the most important alternative for the traditional angiography in ALI diagnostics is the multislice spiral computed tomography angiography (CTA). The 64-slice scanners, thanks to a shorter acquisition time, allow for a one-time administration of the contrast medium and investigation of extensive anatomical regions (such as blood vessels in the limbs) with a submillimetre (isotropic) resolution [8]. The main advantages of CTA include: short examination time (approx. 10 minutes including the preparation and positioning time) and minimal invasiveness. The replacement of the standard intraarterial arteriography with CTA, considerably decreases the risk of severe vascular complications such as: bleeding, formation of pseudoaneurysms or acute limb ischaemia caused by a strong compression of the vessel after the procedure [9].
Despite those many advantages, CTA has its limitations as well. It may become diagnostically useless if the contrast agent flows into the examined vessel too early or too late in relation to the beginning of the examination. Such a situation may take place in patients with circulatory abnormalities, e.g. after a multiorgan trauma (when the contrast medium flows more slowly), or after injecting contrast agent to a unproper (too peripheral) vessel, due to which the concentration of the contrast medium in the vessels is too low. The next problem is presence of artefacts resulting from movements of the examined patients or from a poor contact or cooperation of the patient. Another limitation of CTA in the diagnostics of posttraumatic arterial injuries is the presence of artefacts caused by metal fragments in the vicinity of the analysed vessels, e.g. in case of gunshot wounds. They cause streaks that make the precise and correct evaluation of an image impossible. High incidence of metal fragments in the vicinity of blood vessels is one of the main limitations of CTA [7,9].
The above presented patients with posttraumatic acute ischaemia of the upper limbs were diagnosed with a 64-slice LightSpeed scanner (GE Healthcare). A correct performance of the examination required a proper positioning of the patient (as far as the anatomy allowed), which consisted in elevating the upper limbs and placing them over the head, in one line with the body. Contrast medium was injected into the cubital vein of the limb revealing better perfusion, with the a 18G or 20G cannula and an automatic syringe. The volume of the contrast medium was 80–120 ml, depending on the patient’s body mass. The injection rate ranged from 3.5–4.5 ml/sec. Immediately after contrast administration, an additional ‘pushing’ bolus of the physiological saline was administered, which aimed to increase the concentration of the contrast bolus in the vessels. The concentration of the contrast medium was monitored in the aortic arch with the use of a ‘smart-prep’ method; scanning was started a few seconds after obtaining by the contrast medium the plateau phase in the aortic arch. Scanning time of the upper limbs ranged from 5 to 15 seconds (10 sec on average). Radiation doses depended on the examination time mainly, and ranged from 700 to 2000 DLP (Dose Length Product) units (mean: 1200 u DLP). The examined area extended from the aortic arch to the wrist. The slice width was 0.67 mm, the pitch – 1.3, the tube rotation time – 0.5 sec. Every time, the intensity of the tube current was adjusted automatically (mA modulation).
The analysis of the obtained images was carried out with a diagnostic Advantage Workstation 4.4 (GE Healthcare) and Vessel Analysis software. Three types of reconstructions were performed: three-dimensional MIP (Maximum Intensity Projection), Curved Planar Reconstruction (CPR) (Figure 3) and Volume Rendering (VR) (Figures 1, 2A,B).
In all three cases, owing to the application of the above presented protocol, a high-quality image of the upper limb arteries were obtained and the occlusion sites were precisely located. This allowed for successful operations, restoring normal perfusion of the upper limbs.
Conclusions
The presented cases show that CTA allows for rapid and precise diagnostics of arteries in patients with acute post-traumatic ischaemia of the upper limbs. Due to the low invasiveness of the examination, as well as its high effectiveness in the detection of stenoses and occlusions of the vessels in patients with ALI symptoms, the importance of CTA in the diagnostics and treatment monitoring in ALI is increasing. This examination mode may become a golden diagnostic standard in cases of suspected acute ischaemia of the upper limbs, especially when caused by vascular pathology within the elbow and arm.
References:
- 1.Chin AS, Rubin GD. MDCT Angiography of Peripheral Arterial Occlusive Disease. Tech Vasc Interventional Rad. 2006;9:143–49. doi: 10.1053/j.tvir.2007.02.007. [DOI] [PubMed] [Google Scholar]
- 2.Norgren L, Hiatt WR, Dormandy JA, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II) Eur J Vasc Endovasc Surg. 2007;33:1–75. doi: 10.1016/j.jvs.2006.12.037. [DOI] [PubMed] [Google Scholar]
- 3.Management of peripheral arterial disease (PAD) TransAtlantic Inter-Society Consensus (TASC). Section C: acute limb ischaemia. Eur J Vasc Endovasc Surg. 2000;19:115–43. [PubMed] [Google Scholar]
- 4.Sontheimer DL. Peripheral vascular disease: diagnosis and treatment. Am Fam Physician. 2006;73(11):1971–76. [PubMed] [Google Scholar]
- 5.Quraishy MS, Cawthorn SJ, Giddings AEB. Critical ischaemia of the upper limb. J R Soc Med. 1992;85(5):269–73. doi: 10.1177/014107689208500509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Masłowski L, Frołow M. Choroby aorty i tętnic obwodowych. In: Szczeklik A, editor. Choroby wewnętrzne. Medycyna Praktyczna; Kraków: 2005. pp. 381–84. [Google Scholar]
- 7.Diagnosing traumatic arterial injury in the extremities with CT angiography: pearls and pitfalls. Radiographics. 2005;25(Suppl.1):S133–42. doi: 10.1148/rg.25si055511. [DOI] [PubMed] [Google Scholar]
- 8.Jakubiak A, Waliszewska M, Guziński M, et al. The value of 64-detector computer tomography angiography as a diagnostics method during emergency service in acute lower limbs ischemia. Pol J Radiol. 2009;74(3):37–41. [Google Scholar]
- 9.Hsu CS, Hellinger JC, Rubin GD, Chang J. CT angiography in pediatric extremity trauma: preoperative evaluation prior to reconstructive surgery. Hand (NY) 2008;3(2):139–45. doi: 10.1007/s11552-007-9081-z. [DOI] [PMC free article] [PubMed] [Google Scholar]