

Summary
Background:
The sellar and parasellar region is an area where many heterogenous neoplastic, inflammatory, developmental and vascular pathologies can occur. Differentiation among various diseases may be not easy, because many of these lesions could mimic the clinical, endocrinologic and radiologic features of pituitary adenomas, which can be the cause of possible misdiagnosis.
Case Report:
We report a case of a 52-year-old man who presented with a persistent headache for the last 5–6 years and visual disturbances. Endocrine system examinations disclosed only insignificant hyperprolactinaemia. The MRI revealed an hypointense area – its presentation was similar to that of pituitary adenoma. The correct diagnosis, i.e. a colloid cyst of the pituitary gland, was made intraoperatively.
Conclusions:
Colloid cyst of the pituitary gland is a very rare pathology but it must be considered if there is an hypointense area between the anterior and posterior pituitary lobe in MR imaging without contrast enhancement and if the patient presents with headaches, hypopituitarism and hyperprolactinaemia.
Keywords: colloid cyst, pituitary gland, MRI
Background
Implementation of new diagnostic imaging techniques, such as computed tomography (CT) and magnetic resonance imaging (MRI), as well as state-of-art methods of neurosurgical and pharmacological treatment, revolutionised the diagnostics and therapy of the pituitary gland tumours. Nowadays, the method of choice in pituitary gland and parasellar region imaging is the MRI [1–4].
The sellar and parasellar region is where many various, sometimes very rare, neoplastic, infectious, inflammatory and developmental processes or vascular pathologies occur. The differentiation between those multiple diseases is sometimes difficult, as many rare pathologies within the pituitary gland may mimic the clinical, endocrinological and radiological picture of pituitary adenomas [4], which often leads to misdiagnosis and results in a situation in which many rare pathologies of the pituitary gland are diagnosed correctly as late as during the surgical procedure.
Those rare sellar lesions include colloid cysts of the pituitary gland [5–7]. In this work, we presented a case of a 52-year old man with a colloid cyst, initially diagnosed as a hormonally inactive adenoma of the pituitary gland. Intraoperative verification of the lesion resulted in a correct diagnosis.
Case Report
The 52-year old man was admitted to the Department of Neurosurgery in Wrocław, to undergo surgery of the pituitary tumour. The patient reported persistent headaches for the last 5–6 years, as well as visual disturbances including impaired vision acuity or even periodic episodes of partial loss of vision. The contrast-enhanced MRI of the head, performed under outpatient conditions, revealed in T1-weighted sequences a hypointense area of 1 cm in size, localised between the anterior and the posterior lobe of the enlarged pituitary gland (Figure 1A,B). In T2-weighted images, the area showed an increased signal intensity in its peripheral part, with a hypointense centre of approx. 0.3 cm in size (Figure 2). The FLAIR sequence revealed a significantly increased signal intensity within the lesion (Figure 3). The area was located more to the right site of the sella, while on the left there was a thin, compressed and displaced pituitary gland. The infundibulum of the pituitary gland was dislocated to the left, posteriorly. The optic chiasm seemed to be unaffected – there were no features of its compression – between the upper border of the lesion and the chiasm there was a small amount of cerebrospinal fluid. We revealed no infiltration of the cavernous sinuses. The sphinoidal sinus was normal.
Figure 1.

MR examination performed before surgery. T1-weighted image after contrast administration, coronal plane (A), sagittal plane (B): the intrasellar hypointense mass, located between anterior and posterior lobe of pituitary is visible.
Figure 2.
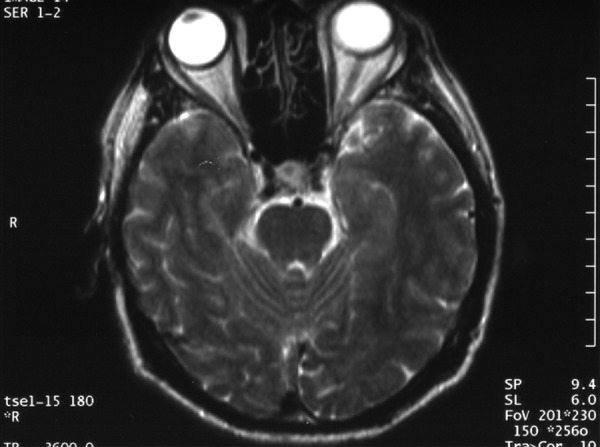
MR examination performed before surgery. T2-weighted image before contrast administration, axial plane: the central portion of the lesion presents with low signal intensity.
Figure 3.

MR examination performed before surgery. FLAIR image before contrast administration, axial plane: the intrasellar mass shows high signal intensity.
Before qualifying the patient for the procedure, a comprehensive endocrinological diagnostic work-up of the diagnosed pituitary tumour was performed. The functional examination of the anterior pituitary lobe was based on the serum level of tropic hormones – somatotropin (GH), follicle-stimulating hormone (FSH), luteotropine (LH), prolactin (PRL), thyrotropin (TSH), adrenocorticotropin (ACTH), and a 24-hour secretion and urinary excretion of cortisol, as well as levels of free thyroxine (fT4), estradiol (E2), testosterone (T) and dehydroepiandrosterone sulphate (DHEA-S).
The functional evaluation of the posterior pituitary gland was carried out by means of tests for diabetes insipidus. Apart from a slight hyperprolactinaemia (PRL=30.6 ng/ml), there were no other abnormalities found.
At the day of admission to the department, neurological examination did not show any deviations from the norm. The sellar tumour was approached surgically through the right nasal aperture and the sphenoid sinus. The tumour was removed. It turned out to be a colloid cyst of the pituitary gland, which was confirmed histopathologically.
During the procedure, a small fragment of adipose tissue was dissected from the thigh and implanted in the postsurgical site, as a filling material.
The procedure was not complicated. We did not reveal any features of diabetes insipidus. The wound on the thigh was healed. The sutures were removed. The wound in the vestibule of the nose was healed as well. After 7 days, the patient was discharged home in a good general condition, without fever or liquorrhea.
After 2 months following the procedure, the patient was admitted to the Department of Endocrinology, in Wrocław, for evaluation of his pituitary gland hormonal function after the surgical procedure. The performed tests revealed no functional abnormalities, including features of diabetes insipidus. The patient required no hormonal substitution. The tested level of prolactin was within the normal range. The patient was advised to undergo a control MRI of the pituitary gland.
The control MRI after 10 months from the procedure revealed no presence of the previously diagnosed lesion (Figure 4A,B). The pituitary gland was small and located at the bottom of the sella. The infundibulum of the pituitary gland was midline in location. Optic chiasm without compression. The sphenoid sinus revealed characteristic postoperative lesions in the form of a thickened sinusal membrane. After contrast administration, the sinus showed peripheral enhancement. The performed examination revealed no presence of the fat implanted during the procedure, meaning it was fully absorbed.
Figure 4.

Follow-up MRI 10 months after surgery. T1-weighted image after contrast administration, coronal plane (A), sagittal plane (B): there is no any endosellar mass, postoperative changes inside the sphenoid sinus are visible.
Discussion
Pituitary gland tumours constitute approximately 10 to 15% of all primary intracranial neoplasms [1,8–10] and are the most frequent cause of functional abnormalities of the pituitary gland and visual field loss [2,3]. Owing to that, their diagnosis and treatment is a difficult clinical problem. The most common tumours of the pituitary gland are adenomas. Among other hormonally inactive tumours of the sellar and parasellar region, cystic lesions are worth noticing. They can be divided into cystic neoplastic lesions (cystic adenomas, cystic craniopharyngiomas etc.) and cystic non-neoplastic lesions. Baskin and Wilson, basing on intraoperative observations and histological analysis of the cystic walls divided the non-neoplastic cysts of that region into four groups:
Non-neoplastic sellar and parasellar cysts are much more seldom than craniopharyngiomas or cystic adenomas of the pituitary gland. Due to the lack of hormonal secretion and small size, they do not tend to be symptomatic and are revealed incidentally (incidetaloma of the pituitary gland). Their incidence amounts to approximately 6–17% and some authors mention 33% in their studies [5]. Teramoto et al. found incidental cystic lesions in 37 pituitary glands after performing 1000 autopsies [7].
Pars intermedia cysts include colloid cysts. They are located between the anterior and the posterior lobe of the pituitary gland and do not communicate with the subarachnoid space. Their pathogenesis is not fully understood. Some authors suggest that colloid cysts may be a consequence of a natural cell degeneration, in the process of which small cysts and pseudocysts including colloid substances are formed around the foci of destroyed and degenerating cells [5,6]. According to some other theory, such cysts are formed from endocrine cells which underwent necrosis due to ischaemia or poorly vascularised intermedial part of the pituitary gland [5,6].
Colloid cysts of the pituitary gland, contrary to Rathke’s cleft cysts, are filled with a colourless or whitish, relatively thick colloid (mucopolysaccharide) substance. Their walls are built of connective tissue devoid of epithelial elements, which indicates to the fact that colloid cysts of the pituitary gland are not of epithelial origin [5].
Colloid cysts are slowly growing, benign tumours which constitute approx. 0.2–2% of all intracranial neoplasms. Their typical location is anterior part of the III ventricle [11–13]. Other locations include pia mater, cerebellum, brainstem, cranial vault and the IV ventricle. There were even cases of reported colloid cysts within the frontal lobe [12].
Colloid cyst of the pituitary gland is a rare phenomenon [5,6]. The available medical literature does not include any numerical data on the incidence of this pathology.
Diagnostic imaging of colloid cysts includes both MRI and CT examinations. As far as the CT is concerned, the cysts are mostly (in two thirds of all examined cases) hyperdense in comparison to the grey matter, while one third of them are hypo- or isodense. These are mainly oval or round structures. After contrast administration, CT reveals a thin layer of enhancement, which may correspond to the capsule of the cyst [12–17]. On MRI, colloid cysts may produce diverse signal intensity. Some lesions are inhomogenous. Sometimes, it is possible to visualise the fluid level or the presence of an additional structure, located centrally or peripherally within the cyst. Approximately 50% of these pathological lesions are hyperintense in T1-weighted images. The rest may be iso- or hypointense as compared to the gray matter. In T2-weighted images, most of the colloid cysts show a decreased signal intensity, while FLAIR sequences reveal an increased signal intensity [13–17]. In DWI sequences, those cysts are shown to form areas of decreased signal intensity [12].
According to some observations, in T2-weighted sequences, many lesions produce a significantly decreased signal intensity in their central part, as compared to the signal intensity of the pehripheral areas of the cyst. It was thus suggested that such a diversity of results concerning MRI signal intensity results from paramagnetic properties of iron, possibly contained in small amounts in macrophages present in colloid cysts. However, on the other hand, microscopic examinations revealed that macrophages accumulate mainly peripherally, and not in the central part of the cyst, which may, as a result, lead to a decreased signal intensity in T2-weighted images of that part [13]. There were some individual cases of minor calcifications inside the colloid cysts [13]. Differentiation between colloid cysts and other types of intracranial cystic lesions in imaging examinations was shown in Table 1 [18–20].
Table 1.
Differential diagnosis of intracranial cysts in CT and MR imaging.
| Intracranial cyst | CT density | Signal intensity on MRI | Remarks | |||
|---|---|---|---|---|---|---|
| T1 | T2 | FLAIR | DWI | |||
| Colloid cyst | Hyperdense in ⅔ of cases/iso- or hypodense | Hyperintense in ½ of the cases/iso- or hypointense | Hypointense | Hyperintense | Hypointense | – |
| Epidermoid cyst | Hypodense/rarely hyperdense | Hypointense | Hyperintense | Hyperintense | Hyperintense | – |
| Dermoid cyst | Hypodense/rarely hyperdense | Hyperintense | Hypointense/hyperintense | Hyperintense | Hyperintense | – |
| Arachnoid cyst | Hypodense | Hypointense | Hyperintense | Hypointense | Hypointense | Isointense in comparison to CSF* in all sequences |
| Choroid plexus cyst | Hypodense | Hypointense | Hyperintense | Hyperintense in ⅔ of cases. | Hyperintense in ⅔ of cases. | – |
| Enlarged perivascular space | Hypodense | Hypointense | Hyperintense | Hypointense | Hypointense | Isointense in comparison to CSF* in all sequences |
| Neurenteric cyst (neuroenteric) | Hypodense | Hyperintense | Hyperintense | Hyperintense | May be insignificantly hyperintense | – |
| Ependymal cyst | Hypodense | Hypointense | Hyperintense | Hypointense | Hypointense | Isointense in comparison to CSF* in all sequences |
| Neuroglial cyst | Hypodense | Hypointense | Hyperintense | Hypointense | Hypointense | Isointense in comparison to CSF* in all sequences |
| Porencephalic cyst | Hypodense | Hypointense | Hyperintense | Hypointense | Hypointense | Isointense in comparison to CSF* in all sequences |
| Abscess | Hypodense | Hypointense/rarely hyperintense | Hyperintense | Hyperintense | Hyperintense | – |
CSF – cerebrospinal fluid.
Colloid cysts of the pituitary gland reveal some typical MRI features which can be helpful in establishing the appropriate diagnosis. However, preoperative diagnosis is often not fully reliable and only the intraoperative findings along with histopathological examination constitute a final confirmation. That is what happened in case of our patient (the MRI showed a lesion suggestive of pituitary adenoma. A rare differential diagnosis of colloid cyst was not considered due to a considerably higher incidence of adenomas).
Due to the location of the colloid cyst in pars intermedia of the pituitary gland, in sagittal sections the lesion is placed between the anterior and the posterior lobe of the pituitary gland. In T1-weighted images, the colloid cyst is hypointense and remains unenhanced after contrast administration [5,6]. Such cysts often have a typical shape, called the ‘baseball-like’ shape in English literature [6].
We reported a case of a lesion which was hypointense in T1-weighted images (Figure 1A,B). It was noteworthy that in T2-weighted sequences, the central part of the cyst produced a significantly decreased signal intensity (Figure 2), while in the FLAIR sequence, there was a significant increase in signal intensity (Figure 3). The MRI image as a whole could be then suggestive of a colloid cyst.
As already mentioned above, colloid cysts are mostly asymptomatic, due to their small size, ranging from 6 to 21 mm [5], and from 5 to 15 mm, according to some other authors [6]. That is why these lesions are often found incidentally. However, growing cysts lead to abnormalities of the endosecretory function, suggestive of sellar pathology. Hypopituitarism affects the gonadotropic cells mostly, leading to menstrual disorder (oligomenorrhea and galactorrhea) and hypogonadotropic hypogonadism in men [5,6]. Moreover, headaches are quite frequent as well – according to Nomikos et al., they are experienced by 27% of patients [6]. There were also reported cases of diabetes insipidus or the pituitary stroke [5]. Panhypopituitarism is very rare in patients with colloid cysts [6]. According to laboratory studies of multiple cases, hyperprolactinaemia is found in as much as 72% of patients [6]. Physiologically, dopamine secreted by the hypothalamus reaches the anterior lobe through the pedicle of the pituitary gland and inhibits prolactin secretion. Hyperprolactinaemia in patients with colloid cysts is most probably the result of a disturbed dopamine transport from the hypothalamus to the pituitary gland [6].
Apart from the disturbed pituitary gland function, the colloid cysts growing suprasellary may compress the optic chiasm and cause visual disturbances [5].
In the presented case, the colloid cyst of the pituitary gland manifested itself by persistent headaches and visual disturbances, although the performed MRI examination did not show any evident features of optic chiasm compression. Preoperatively, the patient was not consulted by an ophthalmologist, but the disturbances disappeared after the surgical procedure. Apart from a slight hyperprolactinaemia, the laboratory tests did not reveal any abnormalities, such as hypopituitarism.
Surgical treatment of colloid cysts are necessary only in case of symptomatic lesions causing endocrinological and neurological disturbances. The method of choice is the approach through the nose and sphenoid sinus. An incidentally revealed asymptomatic colloid cyst of the pituitary gland constitutes an indication for further MRI monitoring for potential growth of the lesion [5,6].
Conclusions
Colloid cyst of the pituitary gland is a very rare pathology. However, it should be considered by the differential diagnosis if the MRI shows a hypointense area between the anterior and the posterior lobe of the pituitary gland, remaining unenhanced after contrast administration and if the patient reports headaches, while the examinations reveal partial hypopituitarism with concurrent hyperprolactinaemia. An additional diagnostic hint should be the presence of a low signal intensity in the central part of the cyst in T2-weighted images and an increased signal intensity in the FLAIR sequence.
References:
- 1.Evanson J. Imaging the pituitary gland. Imaging. 2002;14:93–102. [Google Scholar]
- 2.Zgliczyński S, Brzezińska A. Rozpoznawanie i leczenie guzów przysadki. Med Prakt. 1995;3:69–71. [Google Scholar]
- 3.Bladowska J, Sokolska V, Czapiga E, et al. Postępy w diagnostyce obrazowej przysadki mózgowej i okolicy okołosiodłowej. Adv Clin Exp Med. 2004;13:709–17. [Google Scholar]
- 4.Rennert J, Doerfler A. Imaging of sellar and parasellar lesions. Clin Neurol Neurosurg. 2007;109:111–24. doi: 10.1016/j.clineuro.2006.11.001. [DOI] [PubMed] [Google Scholar]
- 5.Zieliński G, Podgórski JK, Siwik J, et al. Występowanie torbieli koloidowych przysadki mózgowej. Neurol Neurochir Pol. 2002;36:293–306. [PubMed] [Google Scholar]
- 6.Nomikos P, Buchfelder M, Fahlbusch R. Intra- and suprasellar colloid cysts. Pituitary. 1999;2:123–26. doi: 10.1023/a:1009983414014. [DOI] [PubMed] [Google Scholar]
- 7.Teramoto A, Hirakawa K, Sanno N, et al. Incidental pituitary lesions in 1,000 unselected autopsy specimens. Neuroradiology. 1994;193:161–64. doi: 10.1148/radiology.193.1.8090885. [DOI] [PubMed] [Google Scholar]
- 8.Yoon PH, Kim DI, Jeon P, et al. Pituitary adenomas: early postoperative MR imaging after transsphenoidal resection. AJNR. 2001;22:1097–104. [PMC free article] [PubMed] [Google Scholar]
- 9.Bolanowski M. Guzy przysadki – możliwości diagnostyczne i terapeutyczne. Terapia. 2001;102:37–39. [Google Scholar]
- 10.Zhang X, Horwitz GA, Heaney AP, et al. Pituitary tumor transforming gene (PTTG) expression in pituitary adenomas. J Clin Endocrinol Metab. 1999;84:761–67. doi: 10.1210/jcem.84.2.5432. [DOI] [PubMed] [Google Scholar]
- 11.Stachura K, Libionka W, Moskała K, et al. Colloid cysts of the third ventricle. Endoscopic and open microsurgical management. Neurol Neurochir Pol. 2009;43:251–57. [PubMed] [Google Scholar]
- 12.Tanei T, Fukui K, Kato T, et al. Colloid (enterogenous) cyst in the frontal lobe. Neurol Med Chir (Tokyo) 2006;46:401–4. doi: 10.2176/nmc.46.401. [DOI] [PubMed] [Google Scholar]
- 13.Armao D, Castillo M, Chen H, et al. Colloid cyst of the third ventricle: imaging-pathologic correlation. AJNR. 2000;21:1470–77. [PMC free article] [PubMed] [Google Scholar]
- 14.Hadley DM. Colloid cyst of the IIIrd ventricle. J Neurol Neurosurg Psychiatry. 2002;72(Suppl.2):ii15. doi: 10.1136/jnnp.72.suppl_2.ii15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Shaktawat SS, Salman WD, Twaij Z, et al. Unexpected death after headache due to a colloid cyst of the third ventricle. World J Surg Oncol. 2006;4:47–49. doi: 10.1186/1477-7819-4-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Joshi SM, Gnanalingham KK, Mohaghegh P, et al. A case of familial third ventricular colloid cyst. Emerg Med J. 2005;22:909–10. doi: 10.1136/emj.2004.018440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Annamalai G, Lindsay KW, Bhattacharya JJ. Spontaneous resolution of a colloid cyst of the third ventricle. Br J Radiology. 2008;81:e20–e22. doi: 10.1259/bjr/59191880. [DOI] [PubMed] [Google Scholar]
- 18.Osborn AG, Preece MT. Intracranial cysts: radiologicpathologic correlation and imaging approach. Radiology. 2006;239:650–64. doi: 10.1148/radiol.2393050823. [DOI] [PubMed] [Google Scholar]
- 19.Orakcioglu B, Halatsch ME, Fortunati M, et al. Intracranial dermoid cysts: variations of radiological and clinical features. Acta Neurochir (Wien) 2008;150:1227–34. doi: 10.1007/s00701-008-0152-x. [DOI] [PubMed] [Google Scholar]
- 20.Hakyemez B, Yildiz H, Ergin N, et al. Flair and diffusion weighted MR imaging in differentiating epidermoid cysts from arachnoid cysts. Turk J Diagn Intervent Radiol. 2003;9:418–26. [PubMed] [Google Scholar]