

Abstract
The authors report the case of a 49-year-old man with episodes of chest discomfort. Exercise/rest single-photon emission tomography (SPECT) with technetium-99m sestamibi (MIBI) revealed inferior and septal myocardial ischaemia, and MIBI anterior reverse redistribution, representing damaged myocardium. Cardiac tomography documented anomalous origin of the right coronary artery (ARCA) arising from the left sinus of valsalva coursing between the aorta and pulmonary artery. Myocardial ischaemia and myocardial damage revealed by SPECT are related to the transient coronary flow reduction elicited by the compression of the ARCA that is produced by the great arteries during exercise. The ARCA is a rare condition, but may cause myocardial infarction and sudden death. β-blockers and dihydropyridine calcium-channel blockers may provide cardioprotection from inducible myocardial ischaemia. However, in case of failure of medical cardioprotection, relocation of the ARCA to the appropriate aortic sinus and coronary bypass grafting could be considered as the best options.
Background
The prevalence of the anomalous origin of the right coronary artery (ARCA) arising from the left valsalva sinus and coursing between the aorta and pulmonary artery varies from 0.026%1 to 0.25%.2 The knowledge of history and causes of adverse cardiovascular events related to the ARCA may suggest some preventive strategies.
Case presentation
In November 2008, a 49-year-old man presented to us with episodes of chest discomfort. Exercise testing and Holter monitoring were negative for ST depressions or arrhythmias. Exercise/rest single-photon emission tomography (SPECT) with technetium-99m sestamibi (MIBI) revealed inferior and septal reversible defects and anterior MIBI reverse redistribution (figure 1).
Figure 1.

Stress/rest technetium-99m sestamibi (MIBI) cardiac single-photon emission tomography. Reversible perfusion defects, inferior (red arrows), septal (yellow arrow); Anterior reverse redistribution defect (white arrows).
Investigations
In December 2008, this patient underwent cardiac tomography (CT) which documented the presence of extramural course of the ARCA arising from the left sinus of valsalva. Volume-rendered, axial and curved, multi-planar images showed a reduced calibre in the proximal portion of the right coronary artery that coursed between the aorta and the pulmonary artery. The left coronary artery arose normally from the left valvalsa sinus. There was a separate orificium for the right coronary artery and the left coronary artery. The coronary arteries were free of atherosclerotic lesions (figure 2). Echocardiography revealed normal left ventricular contractility.
Figure 2.
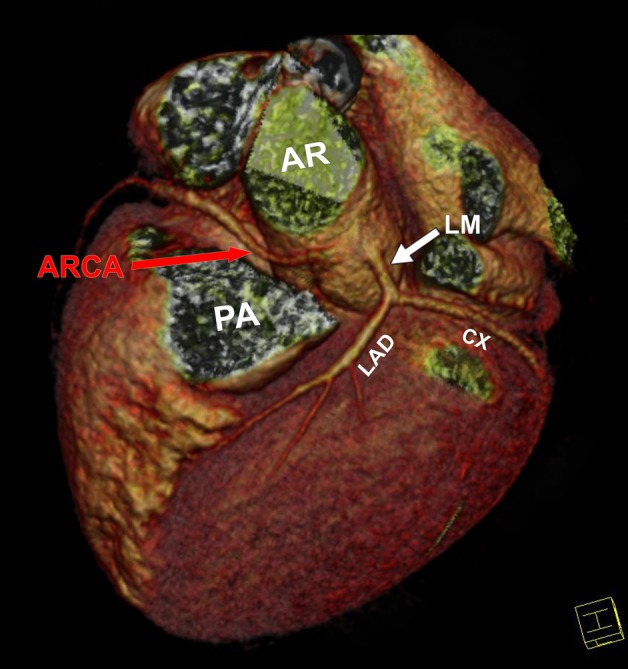
Volume rendered TC mages indicates extramural anomalous origin of the right coronary artery (ARCA) with interarterial course between aortic root (AR) and pulmonary artery (PA); ARCA reduced calibre (red arrow). Left main stem (LM); left anterior descending (LAD); circumflex (CX).
Differential diagnosis
The ARCA from the left coronary sinus is classified into subtypes:
high interarterial course between the aorta and the pulmonary artery.
low interarterial course between the aorta and the right ventricular outflow tract.
hypoplastic ARCA orifice.
The prevalence of ischaemia is higher in patients with the ARCA with a high interarterial course or a hypoplastic orifice. CT is a reliable non-invasive tool that allows accurate delineation of coronary arterial anomalies and provides detailed 3-dimensional anatomic information that may be difficult to obtain with invasive coronary angiography.
Treatment
Guidelines for the ARCA treatment are not available. Therapy remains equivocal. The underlying mechanism of ischaemia and myocardial damage detected with SPECT is reasonably related to the transient coronary flow reduction elicited by the mechanical compression of the ARCA that is produced by the great arteries during exercise or after mild but repeated daily physical activity. Compression of the ARCA by the great arteries during daily life activities may thus induce angina,3 ventricular fibrillation4 or sudden cardiac death.5 Cardioprotection with β-blockers, however,did not improve the patient’s symptomatology.
Outcome and follow-up
The patient returned then 2 years later with persistent episodes of chest discomfort. His clinical situation and therapy were then re-evaluated and was suggested treatment with non-dihydropyridine calcium-channel blockers and a clinical follow-up to evaluate a surgical option.
Discussion
In this patient, the SPECT perfusion defects represented thus exercise-induced myocardial ischaemia of the inferior and septal walls, whereas MIBI reverse redistribution of the anterior wall suggested the presence of damaged but still viable myocardium.6 Thus, the resulting clinical outcome is myocardial instability with vulnerability to life-threatening arrhythmias. The ARCA is a rare but rather benign anomaly. The surgical options in preventing inducible ischaemia include surgical correction by unroofing the ARCA or coronary artery bypass grafting. The unroofing procedure consists of the relocation of the ARCA to the appropriate aortic sinus.7 Translocation is an alternative strategy to unroofing when the ARCA has an intramural course. In that case, the ARCA is transected distally to the intramural segment and anastomosed above the right coronary valsalva sinus.8 Surgical revascularisation with the internal mammary artery by a minimally invasive approach9 has also been found to be safe. All of these procedures have a low risk. In case of failure of medical cardioprotection the CT results support in this patient the evaluation of surgical options for treatment, including the relocation of the ARCA to the appropriate aortic sinus and coronary bypass grafting.
Learning points.
The ARCA with an interarterial course between the great arteries may induce sudden death as the initial presentation.
β-blockers or calcium-channel blockers non-dihydropyridines may reduce left ventricular contractility and great artery dynamics during stress and thus relieve the abnormal mechanical compression of the ARCA.
Stenting is difficult and technically challenging.
Inducible myocardial ischaemia despite pharmacological protection supports considering surgical options. ARCA relocation or minimally invasive coronary bypass grafting are low-risk procedures.
Footnotes
Competing interests: None.
Patient consent: Obtained.
References
- 1.Alexander RW, Griffith GC. Anomalies of the coronary arteries and their clinical significance. Circulation 1956;14:800–5. [DOI] [PubMed] [Google Scholar]
- 2.Kaku B, Shimizu M, Yoshio H, et al. Clinical features of prognosis of Japanese patients with anomalous origin of the coronary artery. Jpn Circ J 1996;60:731–41. [DOI] [PubMed] [Google Scholar]
- 3.Taylor AJ, Rogan KM, Virmani R. Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol 1992;20:640–7. [DOI] [PubMed] [Google Scholar]
- 4.Jo Y, Uranaka Y, Iwaki H, et al. Sudden cardiac arrest: associated with anomalous origin of the right coronary artery from the left main coronary artery. Tex Heart Inst J 2011;38:539–43. [PMC free article] [PubMed] [Google Scholar]
- 5.Meel BL. An anomalous origin of left coronary artery and sudden death in a soccer player: a case report. Med Sci Law 2011;51:182–3. [DOI] [PubMed] [Google Scholar]
- 6.Tanaka R, Nakamura T, Chiba S, et al. Clinical implication of reverse redistribution on 99mTc-sestamibi images for evaluating ischemic heart disease. Ann Nucl Med 2006;20:349–56. [DOI] [PubMed] [Google Scholar]
- 7.Romp RL, Herlong JR, Landolfo CK, et al. Outcome of unroofing procedure for repair of anomalous aortic origin of left or right coronary artery. Ann Thorac Surg 2003;76:589–95; discussion 595–6. [DOI] [PubMed] [Google Scholar]
- 8.Goda M, Meuris B, Meyns B. Right coronary translocation for anomalous origin of right coronary artery from the left coronary sinus. Interact Cardiovasc Thorac Surg 2011;13:201–2. [DOI] [PubMed] [Google Scholar]
- 9.Reddy RC, Takahashi M, Beckles DL, et al. Anomalous right coronary artery from the left sinus: a minimally invasive approach. Eur J Cardiothorac Surg 2012;41:287–90. [DOI] [PubMed] [Google Scholar]