

Abstract
Research has documented a negative relationship between religion and risky sexual behavior. Few studies, however, have examined the processes whereby religion exerts this effect. The present study develops and tests a model of various mechanisms whereby parental religiosity reduces the likelihood of adolescents’ participation in risky sexual behavior (early sexual debut, multiple sexual partners, and inconsistent condom use). Structural equation modeling, using longitudinal data from a sample of 612 African American adolescents (55% female), provided support for the model. The results indicated that parental religiosity influenced adolescent risky sexual behavior through its impact on authoritative parenting, adolescent religiosity, and adolescent affiliation with less sexually permissive peers. Some mediating mechanisms differed by the gender of the respondent, suggesting a “double-standard” for daughters but not for sons. Findings also indicated the importance of messages about sexual behavior that are transmitted to adolescents by their peers. Theoretical and policy implications of the findings are discussed.
Keywords: Adolescents, Risky sexual behavior, Parenting, Religion, Peers, African Americans, Structural equation modeling (SEM)
Introduction
Current health and social concerns regarding sexually transmitted infections and unintended pregnancies among adolescents signal that it is essential to know more about the influences on their sexual behavior. Research shows that early initiation of sexual activity and unprotected sexual behavior leads to negative physical and psychological outcomes. Adolescents who engage in sexual behavior at earlier ages have more lifetime sexual partners, a greater likelihood of acquiring HIV/AIDS and other sexually transmitted infections, and a greater likelihood of having an unintended pregnancy (Simons et al. 2009). African American youth and adults are disproportionately at risk for such negative sexual health outcomes. They account for 49% of all new HIV/AIDS cases in the United States but comprise only 13% of the total U.S. population. The rate of AIDS diagnoses for African American adults and adolescents is 10 times the rate for Caucasians and nearly three times the rate for Hispanics (Centers for Disease Control and Prevention 2005). The rates of sexually transmitted infections (STIs) and unintended pregnancies are also significantly higher for African Americans compared with Caucasians (CDC 2000). Disregard for this evidence, especially in the African American community, may lead to growing health disparities associated with HIV/AIDS and other sexually transmitted infections and negative mental health outcomes. Therefore, it has become increasingly important to identify factors that may promote safer sexual behavior such as delayed sexual debut, a reduction in the number of sexual partners, and consistent condom use among African American youth.
Past research has established a negative relationship between religion and adolescent sexual behavior (Rostosky et al. 2004; Sinha et al. 2007). A limited number of studies, however, have gone beyond this bivariate relationship to examine the mechanisms and processes whereby religion exerts this effect. Using a social control framework, the present study attempts to overcome this limitation. This perspective views family and religion as institutions that exercise social control by socializing members to adopt conventional norms and values (Baier and Wright 2001; Sherkat and Ellison 1999). Individuals abide by these norms and values, in part, because they do not want to jeopardize their bonds to these institutions. Over time, these norms and values are internalized and self-sustaining, thereby reducing the probability of deviant behavior (Hirschi 1969). To the extent that religion serves this purpose, one would expect religious adolescents to be less inclined to engage in risky sexual behavior than their less religious peers. This study also extends earlier research by examining the role that parental religiosity may play in influencing adolescents’ risky sexual behavior. For example, parental religiosity has been found to be directly associated with delayed timing of sexual debut (Manlove et al. 2006). However, the authors of that study did not examine the possible avenues whereby parental religiosity indirectly influences adolescent sexual behavior. To this end, the goal of the present study is to identify various mechanisms through which parental religiosity influences adolescent risky sexual behavior.
Although most studies find an association between religiosity and sexual debut, there are variations in the literature as to whether religion is positively associated with another form of risky sexual behavior—inconsistent condom use. Sheeran et al. (1999) reported no association between condom use and the degree of religiosity, whereas Zaleski and Schiaffino (2000) found that sexually active adolescents who identified themselves as religious were less likely to practice safe sex through consistent condom use. Consequently, it may be that religion is an unintended risk factor for unprotected sexual behavior among sexually active adolescents. In other words, adolescents who receive abstinence-only sex education may be less likely to take a proactive stance on obtaining and using condoms in the event of unplanned sexual behavior. The current study examines this relationship and identifies the degree to which religious teachings and proscriptions are protective or unintended risk factors against condom use and other risky sexual behaviors among sexually active adolescents.
Research shows that African Americans tend to have higher rates of religious participation compared with other ethnicities (Sinha et al. 2007). Though a few studies have focused on this population, African American adolescents are significantly more involved in and influenced by religion than their Caucasian and Hispanic counterparts (Smith et al. 2002). Importantly, Elkind (1999) found that involvement in religious activities tends to have different meanings and outcomes for adolescents from different racial and ethnic backgrounds. Thus, findings regarding the role of religiosity in white-only samples may not be generalizable to African American youth. The limited number of studies on African American adolescents has also shown differences in the relationship between religion and sexual behavior. For instance, McCree et al. (2003) found a negative relationship between religion and risky sexual behavior among African American females. The results showed religious adolescents to be more likely to delay sexual debut and increase the likelihood of condom use. In contrast, Bearman and Brucker (2001) reported religiosity to delay sexual initiation in whites, Latinos, and Asian American adolescents, but it has no such effect among African Americans. These studies illustrate the inconsistency that exists in the literature regarding the impact of religion on the risky sexual behavior of African American adolescents.
The present study attempts to bring some clarity to this area of research by addressing some of the limitations inherent in past studies. First, we use a comprehensive measure of religiosity. Most past studies assess only one dimension of religiosity (e.g., frequency of church attendance), often using a single item. We employ a multidimensional religiosity scale that focuses on both religious commitment and involvement. Second, prior research has focused largely on whether or not the adolescent has had sexual intercourse. In addition to sexual debut, the present study includes the number of sexual partners and the consistency of condom use as outcomes. Third, we extend earlier research on the bivariate relationship between religiosity and adolescent sexual behavior by examining the avenues whereby both parental and adolescent religiosity influences adolescent risky sexual behavior. We develop and test hypotheses regarding the extent to which constructs such as authoritative parenting and peer affiliation mediate the impact of religion on risky sexual behavior. Finally, the contention that females are more religious than males is one of the most consistent findings in the research literature. Gender differences have also been shown in the sexual behaviors of adolescents. O’Donnell et al. (2003), for example, found that males engage in more risky sexual behavior than females. Thus the link between religion and risky sexual behavior may vary by gender. Our analyses test this possibility.
Influence of Religion on Adolescents’ Values
Western Christianity-based religion emphasizes self-control and living in accord with moral directives and commitments such as honesty, responsibility, and respect for authority and one’s body (Smith 2005). Adolescents with higher levels of religious commitment may be more apt to align their behaviors with the moral teachings stressed through religion. One common religious teaching is that people should not have sex outside of marriage, which makes engaging in sexual activity before marriage morally unacceptable. As a result, the putative impact of religion on sexual behavior is largely a function of the values that it imparts. These principles are seen as divinely ordained, and behavior that violates them is considered immoral (Simons et al. 2004a, b, c).
Research has consistently linked adolescent religiosity (e.g., attendance, prayer, affiliation, participation) with sexual attitudes and behavior (Rostosky et al. 2004). Thornton and Camburn (1989) noted that adolescents who hold strong religious beliefs and pray have less permissive attitudes about sex and report less sexual activity. Other studies have also found associations between religiosity and the number of adolescent sexual partners (Lammers et al. 2000). This accumulated research provides ample empirical evidence that religion influences adolescents’ sexual behavior. What remains unclear are the specific avenues whereby this influence operates. This includes the role that parental religiosity plays in this association.
Parents’ Transmission of Religious Values to Adolescents
Although adolescents are exposed to many influences such as peers and the media, parents are important agents of socialization, especially during their child’s early development. In large measure, adolescents develop their religious beliefs and associate moral standards within the family context. To this extent, one avenue whereby parental influence may occur is via the transmission of religious values. Parents use religion to, among other things, teach values and exert social control. Myers (1996) found parental religiosity to be the strongest influence on the religiosity of their children. Similarly, Smith et al. (2003) reported parental religiosity to have a significant impact on their adolescent’s religious attachment. Such findings suggest a relationship between parental religiosity and adolescent religiosity. As noted above, research has shown that adolescent religiosity is negatively related to risky sexual behavior. Thus, it may be that religious parents decrease risky sexual behavior by promoting their adolescent’s religious commitment. Religious parents may also influence their child’s sexual behaviors through their parenting practices.
Influence of Authoritative Parenting
Several parenting practices have been found to be important determinants of whether an adolescent engages in risky sexual behavior (Clawson and Reese-Weber 2003; Li et al. 2000). These include parental warmth, involvement, communication, monitoring, inductive reasoning, and consistent discipline. These parenting behaviors, when found at high levels, combine to produce an authoritative parenting style. In other words, exposure to authoritative parenting decreases the likelihood that adolescents will engage in risky sexual behavior. Good parent–child communication is often seen as part of authoritative parenting and sex is one of the most salient topics for adolescents (Huebner and Howell 2003). Therefore, in addition to the warmth and control items often included in a measure of authoritative parenting, this study includes communication specifically about sexual behavior.
Authoritative parents demand age-appropriate behaviors from their children and create consequences for violating those behavior standards. This parenting style has been found to be related to a myriad of positive behavioral outcomes (Gray and Steinberg 1999; Simons and Conger 2007). There is rather strong evidence that religious parents are more likely to display the various components of authoritative parenting (Brody et al. 1996; Gunnoe et al. 1999). Authoritative parenting encourages conventional values and behaviors. Children with supportive, involved parents are more likely to adopt their parents’ values (Brody and Flor 1998). Thus, authoritative parenting of religious parents may increase the chances that their adolescent offspring will adopt their conventional values and eschew risky sexual behavior.
Another aspect of authoritative parenting that might decrease the probability of risky sexual behavior is through the monitoring of children’s friendships. These parents encourage affiliation with less sexually permissive peers while discouraging associations with deviant individuals. Therefore, we expect authoritative parenting of religious parents to decrease adolescents’ engagement in risky sexual behaviors by encouraging conventional peer group affiliation.
Influence of Peers
Peer group influence becomes increasingly important during adolescence. Adolescents’ intentions to engage in sex are strongly influenced by their social context in which peers play a major role in determining normative behavior (Sieving et al. 2008). Research on the effect of peer groups on adolescent behavior has been well established. The results of a recent study on 1,046 African American adolescents found the influence of peer norms to shape both their sexual attitudes and behaviors (Wallace et al. 2008). In addition, adolescents’ religious beliefs have been found to influence their peer group affiliation. For example, Simons et al. (2004a, b, c) found religiosity to decrease the likelihood that youth will associate with unconventional peers and engage in delinquent behavior. In part, this effect is probably a consequence of the fact that individuals tend to establish relationships with people who are similar to themselves. Religious organizations provide opportunities for more conventional adolescents (e.g., less sexually permissive peers) to meet and form bonds.
Parents also play a role in their children’s selection of peers. Simons et al. (2001) found that a child’s friendship choices are influenced by authoritative parenting practices. Religious parents influence their child’s social context by encouraging involvement in church and religious activities where they are exposed to a network of peers with conventional beliefs, values, and behaviors. Further, involved parents monitor their child’s peer affiliations and develop relationships with the parents of their child’s peers (Lynch 2004; Smith 2003). To this end, one of the avenues whereby religious parents discourage risky sexual behavior is by engaging in monitoring and other parenting behaviors that influence their adolescent’s friendship choices.
The Current Study
The current study aims to expand our understanding of the relationship between religion and sexual behavior. Based on the social control theory and previous empirical explanations for investigating this association, we hypothesize that parental religiosity indirectly influences adolescent risky sexual behavior through several paths. First, religious parents will increase the probability that their adolescent children will be religious. Second, religious parents are expected to display an authoritative parenting style. Authoritative parenting, in turn, is predicted to directly lower participation in risky sexual behavior. In addition, authoritative parenting will likely exert an indirect influence on risky sexual behavior by increasing the probability of adolescents’ affiliation with less sexually permissive peers. Adolescents’ religiosity is also expected to decrease involvement in risky sexual behavior both directly and indirectly by increasing affiliation with less sexually permissive peers.
Extant research has found religion to have more of an effect on the sexual behavior of females than males (Rostosky et al. 2003). Therefore, we expect the coefficients for the paths linking religion and sexual behavior to be higher for females. Further, because pregnancy may be more consequential for daughters than sons, we expect parents to display a higher level of monitoring with daughters, with the consequence that parenting is more strongly related to the sexual behavior of females than males. We use structural equation modeling of a sample of 612 African American adolescents to test the model in Fig. 1.
Fig. 1.
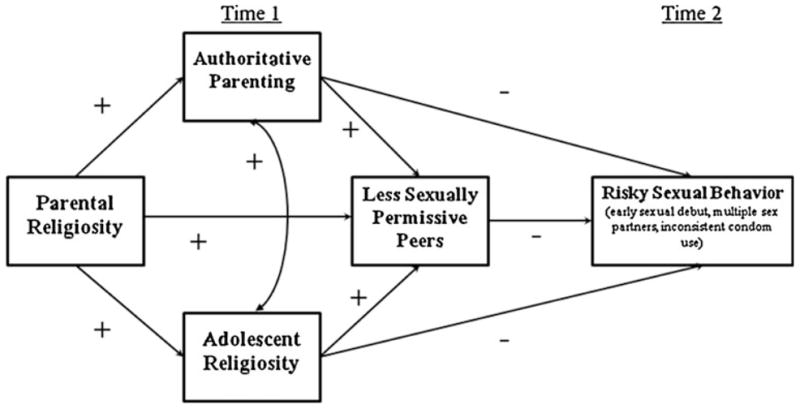
Hypothesized model
Method
Participants
The Family and Community Health Study (FACHS) is a multisite study of neighborhood and family effects on the health and development of African American families. The 867 African American children and their primary caregivers were recruited from small towns and cities in Iowa and Georgia. Block groups, taken from 1990 census data, identified neighborhoods in Iowa and Georgia where the percentage of African American families was high enough for economically practical recruitment and in which at least 10% of families with children live below the poverty line. Two hundred fifty-nine blocks (115 in Georgia and 144 in Iowa) were identified and the families were recruited from them. Families with at least one fifth grade child were randomly selected from rosters. There were no significant gender differences among the adolescents in the socioeconomic status of the primary caregivers, parental religiosity, and per capita income of the families.
The project includes four waves of data. Waves 3 and 4 were selected for the present study because the variables needed to address the research questions were not all included in previous waves. Wave 3, in which the target adolescents were between 15 and 16 years old, was used to predict adolescent risky sexual behavior in Wave 4, in which target adolescents were between 18 and 19 years old. Data were collected 2 years apart, which allows for testing of the lasting effects of various influences on adolescent risky sexual behavior. Wave 3 includes 756 families and Wave 4 includes 778 families.
Procedures
Two home visits were completed with each family. The first home visit focused on the informed consent for both the primary caregiver and the target child. Each home visit contained a self-report questionnaire administered in an interview format using a computer-assisted personal interview (CAPI) for the primary caregiver, child, siblings, and a secondary caregiver if applicable. The CAPI procedure provides an element of privacy that increases the likelihood that respondents will be honest when answering sensitive questions. The CAPI procedure was also used as an attempt to eliminate concerns about underreporting and respondent literacy. The interviews were conducted privately between one participant and one researcher, with no other family members present. Laptop computers were used and the questions appeared in sequence on the screen, which both the interviewer and participant could see. Responses were entered on a keypad operated solely by the respondent and those answers did not appear on the shared screen. Caregivers received $100 and the target child received $70 for participating in the study.
Measures
Parental Religiosity
This measure is based on other commonly used measures of religiosity but has gone beyond the limitations of many measures that only examine church attendance or religious commitment. This study uses both, which allows for a more comprehensive measure of religiosity to represent the various behaviors and beliefs associated with religion. The primary caregiver reported on his/her religious involvement and degree of religious commitment. The scale consisted of 15 items involving questions such as “How important are religious or spiritual beliefs in your day-to-day life?” and “How often in the past month did you attend church services?” The number of response categories varied by item, thus the scores were standardized. All items were coded so that high scores indicated more religiosity. Cronbach’s alpha for this scale was .84.
Adolescent Religiosity
Adolescents were asked questions pertaining to their religious involvement and degree of religious commitment similar to those asked of their parents. This scale consisted of 5 items and the number of response categories varied by item, thus the scores were standardized. All items were coded so that high scores indicated more religiosity. Cronbach’s alpha for the 5-item scale was .81.
Authoritative Parenting
Furman et al. (1989) argue for the use of multiple reporters when assessing parenting practices as a means of reducing error due to shared method variance. As a result, both parent and children reports were combined in order to provide a more valid account of authoritative parenting, as expressed through the combination of several parenting practices (see below). Scale items were adapted from instruments developed for the Iowa Youth and Families Project (IYFP; Conger and Elder 1994). These measures have been shown to have high validity and reliability. For instance, analyses from IYFP have shown that parental reports on these instruments correlate with children’s reports and predict various dimensions of children’s behavior across time (Simons et al. 1998). Other studies have also found predictive validity for the measures in the Family and Community Health Study (FACHS) (Simons et al. 2007; Murry et al. 2008).
Adolescents and parents rated parents’ behaviors on questions involving warmth (e.g., “How often did your parent help you do something that was important to you?”), hostility (e.g., “How often did your parent criticize you or your ideas?”), monitoring (e.g., “How often do you know what your child is doing after school?”), inductive reasoning (e.g., “How often do you give reasons to your child for your decisions?”), consistent discipline (e.g., “How often do you give up when you ask your child to do something and he/she doesn’t do it?), positive reinforcement (e.g., “When your child has done something you like or approve of, how often do you let him/her know you are pleased about it?”), and parent–child discussion of sexual behavior (e.g., “How often has your parent talked to you about sex?”).
These combined parenting practices have been found to predict a variety of child adjustment problems (see Conger et al. 1992). The response format for all items ranged from 1 (never) to 4 (always). Correlations between parent and child reports were all significant and ranged from .40 to .60 across these parenting measures. All items were standardized and summed to form a composite measure. Except for reverse coding of hostility, all items were coded so that high scores indicated a high level of the behavior. The correlations between the various parenting practices ranged from .43 to .70. Cronbach’s alpha for the combined 32-item scale was .84. This composite measure served as an indicator of the extent to which, during early adolescence, the child experienced parenting that combined love, control, and good communication about important matters such as sexual behavior.
Peers Sexual Behavior
Adolescents reported on their affiliation with less sexually permissive peers. A 3-item scale assessed what their friends think and do as it pertains to sexual behavior. The scale included the following: “How many of your close friends have had sex without using a condom?”, “How many of your friends have gotten pregnant or gotten a girl pregnant?”, and “How many of your friends have had sex?” The response format for the items ranged from 1 (none) to 3 (all of them). All items were coded so that high scores indicated less sexually permissive, more conventional peers. Cronbach’s alpha for the scale was .75.
Adolescent Risky Sexual Behavior
An index of risky sexual behavior was constructed using the aggregate scores for sexual debut, number of sexual partners, and inconsistent condom use. Sexual debut was assessed using a question that asked the respondent to report “How old were you when you first had sexual intercourse?” Number of sexual partners was assessed using three questions such as “With how many people have you had sexual intercourse?” and “How many different males/females have you had sexual intercourse with during the last 3 months?” Inconsistent condom use was assessed using two questions: “When you have sexual intercourse, how often do you use a condom?” and “In the last 3 months, how many times have you had sexual intercourse without using a condom (rubber)?” All items were standardized and summed together. The items were coded so that high scores represented more risky sexual behavior. Cronbach’s alpha for the scale was .73.
Analytic Strategy
Structural equation modeling (SEM) was employed (MPlus, Version 5.2, Muthén and Muthén 2004) to test the hypothesized model. One advantage of MPLUS is that it provides tests of significance for indirect or meditational effects. The data were found to be nonnormal (skewness was >2). As a result, bootstrapping was used to correct the standard errors (Nevitt and Hancock 2001). Full Information Maximum Likelihood (FIML) was used to handle missing data. Analyses were performed separately for males and females on the three adolescent risky sexual behaviors (e.g., early sexual debut, number of sexual partners, and inconsistent condom use) to determine whether the various mechanisms of influence affect males and females differently.
The model fit was evaluated using chi-square tests in which a nonsignificant test indicates a model that fits the data well. In addition, the comparative fit index (CFI) was used. CFI compares the hypothesized model over the null model to identify if there was any improvement. CFI varies from 0 to 1; a CFI value close to 1 indicates a very good fit and values above .90 represent an acceptable fit (Bentler 1990). We also used the RMSEA as an index of fit that corrects for model’s complexity. RMSEA values less than .05 indicate a good fit and RMSEA greater than .08 represent errors in approximation (Hu and Bentler 1999).
Results
Descriptive Statistics and Correlational Analyses
The final sample included 612 adolescents (277 males, 335 females) and their primary caregivers. Findings indicate that approximately 89% of the parents in this study reported religious or spiritual beliefs in their day-to-day life to be important. This is consistent with earlier research that contends that African Americans have high levels of religious commitment and involvement (Sinha et al. 2007). Because we were concerned with the influence of religion on the behaviors of sexually active adolescents/emerging adults, respondents who were not sexually active were excluded from the analyses. Further, the outcomes do not make sense for virgins in that we cannot compare age at first sex, number of sexual partners, and inconsistent condom use. Nearly 97% of the adolescents were sexually active by Wave 4. About 80% of adolescents reported having had more than two lifetime sexual partners (89.9% of males, 71.6% of females). Similarly, 39.5% of adolescents reported having had sex before age 15. Of those, 47.8% were males and 32.6% were females. Furthermore, 42% of adolescents (34% males, 25.7% females) never used a condom during sexual intercourse. These statistics are consistent with prior research on the high rates of sexual behavior among African American adolescents (CDC 2007; Kaiser Family Foundation 2008).
Preliminary Analyses
Table 1 presents the means, standard deviations, and correlation matrix for the study constructs. The coefficients above the diagonal are for males and those below are the coefficients for females. The pattern of significant associations was largely consistent with the hypothesized model and suggests differences by gender. For both males and females, parental religiosity was significantly related to authoritative parenting (for males, r = .14, p < .01; for females, r = .17, p < .01) and adolescent religiosity (for males, r = .38, p < .01; for females, r = .44, p < .01). Adolescents’ religiosity was significantly related to less sexually permissive peers (for males, r = .11, p < .05; for females, r = .14, p < .01) and negatively related to risky sexual behavior (for males, r = −.17, p < .01; for females, r = −.27, p < .01). There was also a negative relationship between less sexually permissive peers and risky sexual behavior for both genders (for males, r = −.26, p < .01; for females, r = −.25, p < .01). Authoritative parenting was significantly related to less sexually permissive peers and risky sexual behavior for females (r = .17, p < .01 and r = −.23, p < .01, respectively). However, these relationships were not significant for males.
Table 1.
Correlation matrix for all indicators by gender
| 1 | 2 | 3 | 4 | 5 | Mean | Std. Dev. | |
|---|---|---|---|---|---|---|---|
| 1. Parental religiosity | – | .14** | .38** | .01 | −.03 | 34.26 | 6.1 |
| 2. Authoritative parenting | .17** | – | .26** | .08 | −.06 | 94.08 | 11.02 |
| 3. Adolescent religiosity | .44** | .15** | – | .11* | −.17** | 11.49 | 3.89 |
| 4. Less sexually permissive peers | .05 | .17** | .14** | – | −.26** | 6.96 | 1.54 |
| 5. Risky sexual behavior | −.11 | −.23** | −.27** | −.25** | – | 0.59 | 3.51 |
| Mean | 34.26 | 95.57 | 12.32 | 6.76 | −0.49 | ||
| Std. Dev. | 6.26 | 11.28 | 4.23 | 1.59 | 3.49 |
Note: Correlations above the diagonal are for males (N = 277); those below the diagonal are for females (N = 335)
p ≤ .05
p ≤ .01
Initially, the analyses were performed separately for each risky sexual behavior. While research has shown religion to reduce the likelihood of earlier sexual debut and number of sexual partners, we are less certain about the influence of religion on consistent condom use. The results indicated, however, that the pattern of associations between the variables was the same for all three outcomes. As a result, an aggregate measure of risky sexual behavior was examined and illustrated in the SEM models.
Structural Equation Modeling
The SEM models yield interesting gender differences in the various mechanisms through which the religious commitment of parents impacts adolescent risky sexual behavior. All the factor loadings for constructs with multiple indicators were in an acceptable range, and the chi-square, comparative fit index (CFI), and RMSEA indicated a reasonable fit of the data for each model.
We began by analyzing the fully recursive models. Some of the associations in these models did not approach statistical significance. To obtain more parsimonious models, we reran them only including paths with a t > 1.5. The difference in chi square between the fully recursive and reduced models was not significant (Δχ2 = 2.094, p = .55; Δχ2 = .0312, p = .58 for males and females, respectively) indicating that the reduced models provided a more parsimonious fit of the data (Table 2). The reduced models are presented. All coefficients in the models are standardized.
Table 2.
Model comparison
| χ2 | p | RMSEA | CFI | Model comparison test
|
|||
|---|---|---|---|---|---|---|---|
| Δdf | Δχ2 | p-value | |||||
| Males | |||||||
| Model 1: Fully recursive model | 0.072 | 0.79 | 0.00 | 1.000 | |||
| Model 2: Reduced model | 2.166 | 0.71 | 0.00 | 1.000 | |||
| Model 1 versus Model 2 | 3 | 2.094 | 0.55 | ||||
| Females | |||||||
| Model 1: Fully recursive model | 0.015 | 0.90 | 0.00 | 1.000 | |||
| Model 2: Reduced model | 0.327 | 0.85 | 0.00 | 1.000 | |||
| Model 1 versus model 2 | 1 | 0.312 | 0.58 | ||||
Figure 2 shows the reduced model for males. The effect of parental religiosity on the risky sexual behavior for males was indirect through adolescent religiosity and affiliation with less sexually permissive peers. Parental religiosity was found to predict adolescent religiosity (.39), which in turn, increased the likelihood of adolescent affiliation with less sexually permissive peers (.12) and thus decreasing male risky sexual behavior (−.23). Further, parental religiosity predicted adolescent religiosity which, in turn, decreased male risky sexual behavior (−.14). Peer group affiliation and adolescent religiosity were the only model variables to directly influence male risky sexual behavior. Additionally, the model showed a significant correlation between authoritative parenting and adolescent religiosity (.22).
Fig. 2.
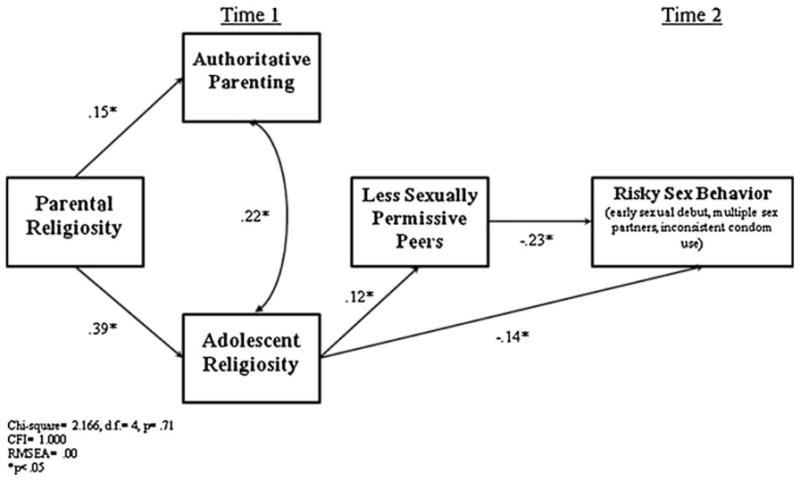
Male risky sexual behavior (N = 277). CFI comparative fit index; RMSEA root mean square error of approximation
The results for females are presented in Fig. 3. Similar to males, parental religiosity had an indirect effect on risky sexual behavior through adolescent religiosity and affiliation with less sexually permissive peers. Parental religiosity increased adolescent religiosity (.44) which, in turn, increased the likelihood of adolescent affiliation with less sexually permissive peers (.12) and thus decreased female risky sexual behavior (−.19). In addition, parental religiosity increased adolescent religiosity which, in turn, decreased female risky sexual behavior (−.23). The most influential variables directly associated with decreasing female risky sexual behavior were authoritative parenting, affiliation with less sexually permissive peers, and adolescent religiosity.
Fig. 3.
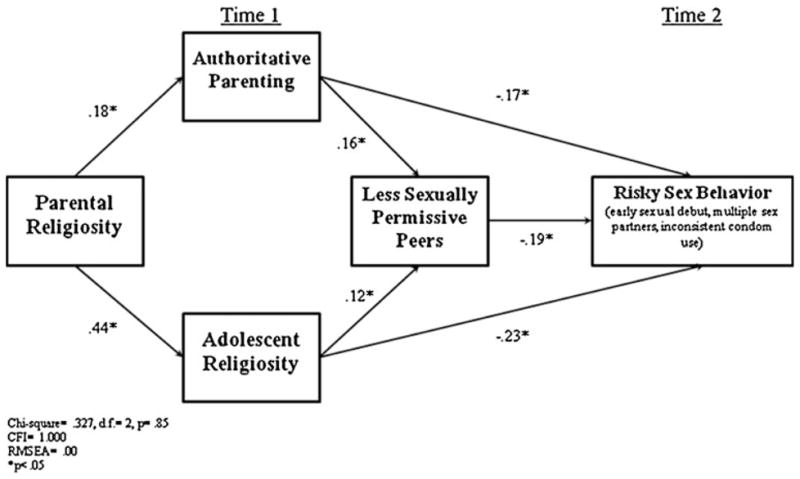
Female risky sexual behavior (N = 335). CFI comparative fit index; RMSEA root mean square error of approximation
Comparisons of the two models suggest support for differences by gender. Parental religiosity was found to have an indirect effect on risky sexual behavior through authoritative parenting only in the female model. For females, authoritative parenting had a direct effect on sexual behavior as well as an indirect effect through peer group affiliation. These effects are not evident in the male model. Further analyses showed, as expected, that parents engage in significantly higher levels of monitoring (p < .01) and communication about sexual issues (p < .001) with their daughters compared with sons. Parents did not differ in the level of warmth, inductive reasoning, positive reinforcement, or consistent discipline that they displayed toward sons versus daughters.
Although the paths of association appear to be different across the male and female models, it was not clear that the differences were statistically significant. Therefore, the model stacking procedure was employed to test for differences in χ2 between the male and female models (Bollen 1989). First, all estimated parameters were constrained to be identical across groups (e.g., restricted model). A non-restrictive model was examined next. This model’s estimated parameters allowed specific relationships to differ across groups. The results are presented in Table 3 and show the coefficients, χ2, change in χ2, and the p-values associated with the differences. The table shows that freeing the paths from authoritative parenting to risky sexual behavior produces a significant improvement in χ2 (p < .05), which suggests that authoritative parenting is associated with risky sexual behavior more strongly for females than for males. Freeing the path between authoritative parenting and affiliation with less sexually permissive peers also improves the fit (p < .05); females have a larger coefficient than males. No improvement in χ2 was found by freeing any of the other paths to differ between groups.
Table 3.
Comparison of the paths for males and females
| Model | β | χ2 | D.F. | Δ χ2(1) | p-value for Δ χ2(1) | |
|---|---|---|---|---|---|---|
| Males | Females | |||||
| Authoritative parenting → Risky sexual behavior | ||||||
| Bs equal in both groups | −.03* | −.03* | 12.14 | 11 | – | – |
| Bs free to differ | .00 | −.05** | 7.73 | 10 | 4.41 | p < .05 |
| Less sexually permissive peers → Risky sexual behavior | ||||||
| Bs equal in both groups | −.48** | −.48** | 12.14 | 11 | – | – |
| Bs free to differ | −.50** | −.46** | 12.09 | 10 | 0.05 | p > .05 |
| Adolescent religiosity → Risky sexual behavior | ||||||
| Bs equal in both groups | −.16** | −.16** | 12.14 | 11 | – | – |
| Bs free to differ | −.11* | −.19** | 10.74 | 10 | 1.4 | p > .05 |
| Authoritative parenting → Less sexually permissive peers | ||||||
| Bs equal in both groups | .02** | .02** | 12.14 | 11 | – | – |
| Bs free to differ | .01 | .02** | 8.00 | 10 | 4.14 | p < .05 |
| Adolescent religiosity → Less sexually permissive peers | ||||||
| Bs equal in both groups | .05** | .05** | 12.14 | 11 | – | – |
| Bs free to differ | .04* | .06** | 11.97 | 10 | 0.17 | p > .05 |
| Parental religiosity → Authoritative parenting | ||||||
| Bs equal in both groups | .30** | .30** | 12.14 | 11 | – | – |
| Bs free to differ | .27** | .32** | 11.99 | 10 | 0.15 | p > .05 |
| Parental religiosity → Adolescent religiosity | ||||||
| Bs equal in both groups | .26** | .26** | 12.14 | 11 | – | – |
| Bs free to differ | .23** | .28** | 11.01 | 10 | 1.13 | p > .05 |
| Parental religiosity → Less sexually permissive peers | ||||||
| Bs equal in both groups | −.01 | −.01 | 12.14 | 11 | – | – |
| Bs free to differ | −.02 | −.01 | 11.72 | 10 | 0.42 | p > .05 |
Significant at .05
Significant at .01
Next, we tested for indirect effects among the male and female models using MPLUS, which provides two significance tests (e.g., delta and bootstrapping). Results were consistent across both methods. Table 4 shows the t-values derived from the delta method for all significant indirect effects. For males, parental religiosity had an indirect effect on both risky sexual behavior and affiliation with less sexually permissive peers through its association with adolescent religiosity. Further, adolescent religiosity was found to have an indirect effect on risky sexual behavior through its association with less sexually permissive peers. For females, parental religiosity had an indirect effect on risky sexual behavior through its impact on authoritative parenting and adolescent religiosity. Parental religiosity also had an indirect effect on affiliation with less sexually permissive peers through its impact on adolescent religiosity and authoritative parenting. Lastly, adolescent religiosity and authoritative parenting had an indirect effect on risky sexual behavior through its impact on affiliation with less sexually permissive peers.
Table 4.
Significance of the indirect effects for males and females (N = 612)
| Predictors | Mediators | Outcomes | ||
|---|---|---|---|---|
| Males | Adolescent religiosity | Less sexually permissive peers | Risky sexual behavior | −0.025 (t = −1.757) |
| Parental religiosity | Adolescent religiosity | Risky sexual behavior | −0.031 (t = −1.923) | |
| Parental religiosity | Adolescent religiosity | Less sexually permissive peers | 0.012 (t = 2.050) | |
| Females | Parental religiosity | Authoritative parenting | Risky sexual behavior | −0.017 (t = −2.530) |
| Parental religiosity | Adolescent religiosity | Risky sexual behavior | −0.055 (t = −3.727) | |
| Adolescent religiosity | Less sexually permissive peers | Risky sexual behavior | −0.018 (t = −1.841) | |
| Authoritative parenting | Less sexually permissive peers | Risky sexual behavior | −0.009 (t = −2.228) | |
| Parental religiosity | Adolescent religiosity | Less sexually permissive peers | 0.013 (t = 2.457) | |
| Parental religiosity | Authoritative parenting | Less sexually permissive peers | 0.007 (t = 2.470) |
Discussion
Risky sexual behavior among adolescents is a social problem that often results in a variety of negative health outcomes. Research on adolescent sexual behavior has shown high rates of sexual activity and engagement in risky sexual behavior, which likely compound the risk for STIs, HIV/AIDS, and unintended pregnancies (CDC 2007; Kaiser Family Foundation 2008). Given the high rates of such outcomes, especially among African Americans, it has become increasingly important to identify factors that may promote safer sexual behavior. Religion is one factor that has been cited to reduce risky sexual behavior; thus, identifying and understanding the mechanisms whereby potential protective factors prevent repeated exposure to sexual risk are needed. The present article extends previous research on the relationship between religion and sexual behavior and attempts to clarify the mechanisms and processes that link parental religiosity to adolescent risky sexual behavior.
Some research has shown that religious adolescents have lower rates of condom use than their less religious counterparts (Zaleski and Schiaffino 2000). To this end, religion may act as an unintended risk factor for unprotected sexual behavior. Our results, however, showed this not to be the case. Rather, all risky sexual behavior (e.g., early sexual debut, multiple sexual partners, and inconsistent condom use) was found to be negatively related to religion. It appears to be the case that, for African American adolescents, religion may be a protective factor against unprotected sexual behavior.
Study findings also showed religious commitment on the part of parents to be positively related to adolescents’ religiosity and authoritative parenting. These findings are consistent with extant research. For example, Smith et al. (2003) reported parents’ religiosity to have a significant impact on their adolescents’ religious commitment. Additionally, Snider et al. (2004) found highly religious parents to be more likely to demonstrate effective parenting practices, such as communication, warmth, and monitoring. Thus, our findings suggest that the religious commitment of parents affect their children’s religious commitment and their parenting practices.
Our results also indicate that adolescents’ affiliation with less sexually permissive peers is partly influenced by religiosity on the part of parents as well as on the part of adolescents. Religious adolescents tended to affiliate with peers who discourage or disapprove of permissive sexual behavior. Having such peers was, in turn, associated with reduced risky sexual behavior. All of these relationships appear in the male and female models.
Study findings reflect some gender differences. Parenting was more strongly related to the sexual behavior of females than males. For females, authoritative parenting was positively associated with an adolescent’s affiliation with less permissive peers and was also directly related to lower levels of risky sexual behavior. This pattern is notable and consistent with extant empirical research because it reveals that parents exert more influence over the actions of their adolescent daughters than their sons (Ramirez-Valles et al. 2002). The results showed that parents provide more monitoring and discussions of sex with their daughters over that of their sons. Therefore, our findings may account for the fact that parenting is more strongly associated with decreased risky sexual behavior for girls compared with boys. In addition, the male model showed a significant correlation between adolescent religiosity and authoritative parenting, while the female model did not. This association is consistent with research showing that religious male adolescents are easier to parent, in part, because they are more likely to take on their parents’ values and are more likely to display obedience and compliance (Kieren and Munro 1987; Ellison and Sherkat 1993), both of which may increase religious participation among male offspring.
Our pattern of findings support the premise of the social control perspective, which posits that people and institutions— such as families, peers, communities, and religion— promote conventional behaviors that use social control to socialize members to adapt to group norms and values (Gottfredson and Hirschi 1990; Simons et al. 2004a, b, c). In the present study, the norms and values of religious parents and adolescents, as well as a less sexually permissive peer group, are associated with delayed sexual debut, fewer sexual partners, and consistent condom use among African American adolescents.
The results of this study have several implications for prevention and intervention programs. First, programs should encourage parents to engage in conscientious, authoritative parenting practices (e.g., warmth, support, good communication, monitoring, consistent discipline). They should also emphasize the salience of exposing their adolescents to other social contexts, such as religion, which gives greater meaning to issues such as sexuality and peer group affiliation. These processes are especially important for laying the ground work at an early age when parents are the primary source of socialization. The Strong African American Families program (SAAF), a preventative intervention program for families, has demonstrated success with this approach. Postponing adolescent early alcohol use and sexual activity was accomplished by encouraging regulated, supportive parenting, providing frequent, harmonious parent–child communication about sex, as well as having prosocial friends. The program is discussed in detail by Brody et al. (2004). Future preventative intervention programs should recognize the continued influence of parents throughout adolescence and teach parents conscientious, authoritative parenting practices.
Secondly, the findings may illustrate a double standard where parents engage in more monitoring and communication about sex with daughters than sons. Presumably, this pattern is a reflection of parents’ concern that their daughters not become pregnant. Certainly, they do not want their sons to impregnate a partner, but the consequences for pregnant girls and their parents may be much higher. As a result, it may be that parents are more vigilant in the parenting of their daughters. Another explanation for this double standard may be partially explained by Mandara et al.’s (2010) suggestion that a possible cause for the high rates of African American male drug use, risky sexual behavior, and conduct problems compared with their sisters may be partly due to their mothers’ strict parenting (e.g., monitoring, etc.) of daughters but not sons. Given these gender differences, preventative intervention programs should help parents navigate their parenting behaviors in a way that is consistent for sons and daughters. Moreover, prevention intervention programs may need to assist parents in the development of gender-appropriate strategies through which they learn to discuss risky sexual behavior with their adolescent sons and daughters.
Our findings indicate that peers have an influence on adolescent sexual behavior and suggest that, in addition to parents, peers are important influences on the risky sexual behavior of African American adolescents. Peers often guide and shape adolescent risk activities (Wallace et al. 2008; Maxwell 2002). That is, peers create a sense of normative behavior in which early sexual debut, having multiple sexual partners, and inconsistent condom use may be supported or rejected by peers, thus becoming a peer group norm. Therefore, programs should encourage parents to be involved in monitoring their children’s peer groups. Our results suggest that parents are doing this with their daughters and it may be that by also doing so with their sons, parents can develop greater influence over their sons’ choice of friends. Because our findings indicate that peers are an important added route through which sex messages are transmitted, preventative intervention programs may benefit from recognizing the impact peers have on adolescent decisions to engage in risky sexual behavior. It might be productive to include peers as a component in the program curriculum. This will allow adolescents and their peers to receive the same messages about risky sexual behavior, thus reinforcing the lessons to each other.
Despite its strengths, our study has certain limitations. First, our sample focuses only on African American families. Although this focus is needed given the high rates of STIs, HIV/AIDS, and unwanted pregnancies in the African American community (CDC 2007), the results may not be generalizable to other ethnicities. Secondly, adolescents reported on their peers’ behaviors, thus the measure was based on adolescents’ reports. It should also be noted that our findings are specific to middle and late adolescent involvement in sexual activities. Thus, the mechanisms through which parental religiosity influences risky sexual behavior may be different during early adolescence. We did not control for adolescent risky sexual behavior at Wave 1 and 2 because data were not available at these waves for the risky sexual behaviors included in our models. In addition, given the sensitive nature of several of the self reported sexual behavior questions, these behaviors may be underreported, which likely attenuates the relationship between study variables. This only underscores the significance of the findings.
In conclusion, there has been discussion in recent years about religion-based solutions for adolescent psychological problems (Smith 2003), delinquency (Regnerus 2003), and risky sexual behavior (Meier 2003). Current interest in faith-based initiatives to tackle the negative outcomes associated with adolescent sexual behavior suggest the need for more empirical studies to examine the ways in which religion affects adolescent risky sexual behavior. The present findings indicate that parental religiosity serves as a protective factor for African American adolescents in that it functions as a social control to reduce the probability of engagement in risky sexual behavior. The findings also show that parental religious commitment is associated with increased adolescent religiosity, authoritative parenting, and affiliation with less sexually permissive peer groups. These three factors, in turn, operate to reduce the chances of an early sexual debut, multiple sexual partners, and inconsistent condom use. The present results provide evidence for the lasting effects of parents, religiosity, and peers on adolescent risky sexual behavior.
Acknowledgments
This research was supported by the National Institute of Mental Health (MH48165, MH62669), the Center for Disease Control (029136-02), the National Institute on Drug Abuse (1P30DA027827), and the National Institute on Alcohol Abuse and Alcoholism (2R01AA012768, 3R01AA012768-09S1).
Biographies
Antoinette Landor is a doctoral student in the Department of Child and Family Development at the University of Georgia. Her research addresses the ways in which various contextual influences such as parents, peers, religion, and community factors influence adolescents’ risk (e.g., aggression and violence, risky sex, delinquency) and resilient behaviors.
Leslie Gordon Simons is an associate professor in the Department of Child and Family Development at the University of Georgia. Her research focuses on quality of parenting and the intergenerational transmission of problem behaviors.
Ronald L. Simons is a Distinguished Research Professor in the Department of Sociology at the University of Georgia. His research focuses on the manner in which family processes, peer associations, community context combine to influence risk for antisocial behavior and emotional problems.
Gene H. Brody is a Regent’s Professor of Child and Family Development and the Director of the Center for Family Research at the University of Georgia. His research examines the risk and protective factors that forecast substance use and other problem behaviors among rural African American youth.
Frederick X. Gibbons is a health-social psychologist and Research Professor in the Department of Psychological and Brain Sciences at Dartmouth College. His primary area of research interest involves the study of psychosocial factors related to health behavior and health status.
Contributor Information
Antoinette Landor, Email: alandor@uga.edu, Department of Child and Family Development, 123 Dawson Hall, University of Georgia, 305 Sanford Dr, Athens, GA 30602, USA.
Leslie Gordon Simons, Email: lgsimons@uga.edu, Department of Child and Family Development, 208 Family Science Center (House A), University of Georgia, 403 Sanford Dr, Athens, GA 30602, USA.
Ronald L. Simons, Email: rsimons@uga.edu, Department of Sociology, Baldwin Hall, University of Georgia, Athens, GA 30602, USA
Gene H. Brody, Email: gbrody@uga.edu, Center for Family Research, University of Georgia, 1095 College Station Rd., Athens, GA 30602, USA
Frederick X. Gibbons, Email: fgibbons@iastate.edu, Department of Psychological and Brain Sciences, Dartmouth College, 6207 Moore Hall, Hanover, NH 03755, USA
References
- Baier CJ, Wright BR. If you love me, keep my commandments: A meta-analysis of the effect of religion on crime. Journal of Research in Crime and Delinquency. 2001;38:3–21. [Google Scholar]
- Bearman PS, Brucker H. Promising the future: Virginity pledges and first intercourse. American Journal of Sociology. 2001;106:859–912. [Google Scholar]
- Bentler PM. Comparative fit indices in structural models. Psychological Bulletin. 1990;107:588–606. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- Bollen KA. Structural equation models with latent variables. New York, NY: Wiley; 1989. [Google Scholar]
- Brody GH, Flor DL. Maternal resources, parenting practices, and child competence in rural, single-parent African American families. Child Development. 1998;69(3):803–816. [PubMed] [Google Scholar]
- Brody GH, Murry VM, Gerrard M, Gibbons FX, Molgaard V, McNair L, et al. The strong African American families program: Translating research into prevention programming. Child Development. 2004;75(3):900–917. doi: 10.1111/j.1467-8624.2004.00713.x. [DOI] [PubMed] [Google Scholar]
- Brody GH, Stoneman Z, Flor D. Parental religiosity, family processes, and youth competence in rural, two-parent African American families. Developmental Psychology. 1996;32(4):696–706. [Google Scholar]
- Centers for Disease Control, Prevention, Division of STD Prevention. Tracking the hidden epidemics: STDs in the United States. Atlanta, GA: Centers for Disease Control and Prevention; 2000. [Google Scholar]
- Centers for Disease Control and Prevention, US Department of Health and Human Services. HIV/AIDS surveillance report. 2005 Retrieved April 23, 2008, www.cdc.gov/hiv/topics/surveillance/resources/reports/
- Centers for Disease Control and Prevention, US Department of Health and Human Services. Youth risk behavior surveillance survey. 2007 Retrieved June 6, 2008, www.cdc.gov/HealthyYouth/yrbs/index.htm.
- Clawson CL, Reese-Weber M. The amount and timing of parent-adolescent sexual communication as predictors of late adolescent sexual risk-taking behaviors. Journal of Sex Research. 2003;40(3):256–265. doi: 10.1080/00224490309552190. [DOI] [PubMed] [Google Scholar]
- Conger RD, Conger KJ, Elder GH, Lorenz FO, Simons RL, Whitbeck LB. A family process model of economic hardship and adjustment of early adolescent boys. Child Development. 1992;63:526–541. doi: 10.1111/j.1467-8624.1992.tb01644.x. [DOI] [PubMed] [Google Scholar]
- Conger RD, Elder GH. Families in troubled times:Adapting to change in rural America. Hawthorne, NY: Aldine de Gruyter; 1994. [Google Scholar]
- Elkind D. Religious development in adolescence. Journal of Adolescence. 1999;22:291–295. [PubMed] [Google Scholar]
- Ellison CG, Sherkat DE. Obedience and autonomy: Religion and parental values reconsidered. Journal for the Scientific Study of Religion. 1993;32(4):313–329. [Google Scholar]
- Furman W, Jones L, Buhrmester D, Adler T. Children’s, parents’, and observers’ perspectives on sibling relationships. In: Zukow PG, editor. Sibling interaction across cultures: Theoretical, methodological issues. New York: Springer; 1989. [Google Scholar]
- Gottfredson M, Hirschi T. A general theory of crime. Stanford, CT: Stanford University Press; 1990. [Google Scholar]
- Gray MR, Steinberg L. Adolescent romance and the parent-child relationship: A contextual perspective. In: Furman W, Brown BB, Feiring C, editors. The development of romantic relationships in adolescence. NewYork: Cambridge University Press; 1999. pp. 235–265. [Google Scholar]
- Gunnoe ML, Hetherington EM, Reiss D. Parent religiosity, parenting style, and adolescent social responsibility. Journal of Early Adolescence. 1999;19:199–225. [Google Scholar]
- Hirschi T. Causes of delinquency. Berkeley, CA: University of California Press; 1969. [Google Scholar]
- Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternative. Structural Equation Modeling: A Multidisciplinary Journal. 1999;6:1–55. [Google Scholar]
- Huebner AJ, Howell LW. Examining the relationship between adolescent sexual risk-taking and perceptions of monitoring, communication, and parenting styles. Journal of Adolescent Health. 2003;33:71–78. doi: 10.1016/s1054-139x(03)00141-1. [DOI] [PubMed] [Google Scholar]
- Kaiser Family Foundation. United States teen sexual activity. 2008 Retrieved January 29, 2008, www.kff.org/youthhivstds.
- Kieren DK, Munro B. Following the leaders: Parents’ influence on adolescent religious activity. Journal of the Scientific Study of Religion. 1987;26(2):249–255. [Google Scholar]
- Lammers C, Ireland M, Resnick M, Blum R. Influences on adolescents’ decision to postpone onset of sexual intercourse: A survival analysis of virginity among youths aged 13 to 18 years. Journal of Adolescent Health. 2000;26:42–48. doi: 10.1016/s1054-139x(99)00041-5. [DOI] [PubMed] [Google Scholar]
- Li X, Stanton B, Feigelman S. Impact of perceived parental monitoring on adolescent risk behavior over 4 years. Journal of Adolescent Health. 2000;27:49–56. doi: 10.1016/s1054-139x(00)00092-6. [DOI] [PubMed] [Google Scholar]
- Lynch CE. Choosing church: What makes a difference for teens. Louisville, KY: Westminster John Knox Press; 2004. [Google Scholar]
- Mandara J, Varner F, Richman S. Do African American mothers really “love” their sons and “raise” their daughters? Journal of Family Psychology. 2010;24:41–50. doi: 10.1037/a0018072. [DOI] [PubMed] [Google Scholar]
- Manlove JS, Terry-Humen E, Ikramullah EN, Moore KA. The role of parent religiosity in teens’ transitions to sex and contraception. Journal of Adolescent Health. 2006;39:578–587. doi: 10.1016/j.jadohealth.2006.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maxwell KA. Friends: The role of peers influence across adolescent risk behaviors. Journal of Youth and Adolescence. 2002;31(4):267–277. [Google Scholar]
- McCree DH, Wingood GM, DiClemente R, Davies S, Harrington KF. Religiosity and risky sexual behavior in African American adolescent females. Journal of Adolescent Health. 2003;33:2–8. doi: 10.1016/s1054-139x(02)00460-3. [DOI] [PubMed] [Google Scholar]
- Meier AM. Adolescents’ transition to first intercourse, religiosity, and attitudes about sex. Social Forces. 2003;81(3):1031–1053. [Google Scholar]
- Murry VM, Brody GH, Simons RL, Cutrona CE, Gibbons F. Disentangling ethnicity and context as predictors of parenting within rural African American families. Applied Developmental Science. 2008;12(4):202–210. doi: 10.1080/10888690802388144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. User’s guide. 3. Los Angeles: Muthén and Muthén; 2004. Mplus: The comprehensive modeling program for applied researchers. [Google Scholar]
- Myers SM. An interactive model of religiosity inheritance: The importance of family context. American Sociological Review. 1996;61:858–866. [Google Scholar]
- Nevitt J, Hancock GR. Performance of bootstrapping approached to model test statistics and parameter standard error estimation in structural equation modeling. Structural Equation Modeling. 2001;8:353–377. [Google Scholar]
- O’Donnell L, Myint UA, O’Donell CR, Stueve A. Long term influences of sexual norms and attitudes on timing of sexual norms and attitudes on timing of sexual initiation among urban minority youth. Journal of School Health. 2003;73:68–76. doi: 10.1111/j.1746-1561.2003.tb03575.x. [DOI] [PubMed] [Google Scholar]
- Ramirez-Valles J, Zimmerman MA, Juarez L. Gender differences of neighborhood and social control processes: A study of the timing of first intercourse among low-achieving, urban, African American youth. Youth and Society. 2002;33(3):418–441. [Google Scholar]
- Regnerus MD. Religion and positive adolescent outcomes: A review of research and theory. Review of Religious Research. 2003;44(4):394–413. [Google Scholar]
- Rostosky SS, Regnerus MD, Wright MC, Laurie M. Coital debut: The role of religiosity and sex attitudes in the add health survey. Journal of Sex Research. 2003;40:358–367. doi: 10.1080/00224490209552202. [DOI] [PubMed] [Google Scholar]
- Rostosky SS, Wilcox B, Wright M, Randall BA. The impact of religiosity on adolescent sexual behavior: A review of the evidence. Journal of Adolescent Research. 2004;19:677–697. [Google Scholar]
- Sheeran P, Abraham C, Ordell S. Psychosocial correlates of heterosexual condom use: A meta-analysis. Psychological Bulletin. 1999;125:90–132. doi: 10.1037/0033-2909.125.1.90. [DOI] [PubMed] [Google Scholar]
- Sherkat DE, Ellison CG. Recent developments and current controversies in the sociology of religion. Annual Review of Sociology. 1999;25:363–394. [Google Scholar]
- Sieving RE, Eisenberg ME, Pettingell S, Skay C. Friends’ influence on adolescents’ first sexual intercourse. Perspectives on Sexual and Reproductive Health. 2008;38:13–19. doi: 10.1363/psrh.38.013.06. [DOI] [PubMed] [Google Scholar]
- Simons LG, Burt C, Peterson FR. The effect of religion on risky sexual behavior among college students. Deviant Behaviors. 2009;30(5):467–485. [Google Scholar]
- Simons RL, Chao W, Conger RD, Elder GH. Quality of parenting as mediator of the effect of childhood defiance on adolescent friendship choices and delinquency: A growth curve analysis. Journal of Marriage and the Family. 2001;63:63–79. [Google Scholar]
- Simons LG, Conger RD. Linking mother-father differences in parenting to a typology of family parenting styles and adolescent outcomes. Journal of Family Issues. 2007;28(2):212–241. [Google Scholar]
- Simons RL, Lin KH, Gordon LC. Socialization in the family of origin and male dating violence: A prospective study. Journal of Marriage and the Family. 1998;60:467–478. [Google Scholar]
- Simons RL, Simons LG, Chen YF, Brody GH, Lin KH. Identifying the psychological factors that mediate the association between parenting practices and delinquency. Criminology. 2007;45(3):481–517. [Google Scholar]
- Simons LG, Simons RL, Conger RD. Identifying the mechanisms whereby family religiosity influences the probability of adolescent antisocial behavior. Journal of Comparative Family Studies. 2004a;34(5):547–563. [Google Scholar]
- Simons LG, Simons RL, Conger RD, Brody GH. Collective socialization and child conduct problems: A multilevel analysis with an African American sample. Youth and Society. 2004b;35(3):267–292. [Google Scholar]
- Simons RL, Simons LG, Wallace LE. Families, delinquency, and crime: Linking society’s most basic institution to antisocial behavior. Los Angeles, CA: Roxbury Publishing Company; 2004c. [Google Scholar]
- Sinha JW, Cnaan RA, Gelles RJ. Adolescent risk behaviors and religion: Findings from a national study. Journal of Adolescence. 2007;30:231–249. doi: 10.1016/j.adolescence.2006.02.005. [DOI] [PubMed] [Google Scholar]
- Smith C. Theorizing religious effects among American Adolescents. Journal for the Scientific Study of Religion. 2003;42:17–30. [Google Scholar]
- Smith C. Soul searching. New York: Oxford; 2005. [Google Scholar]
- Smith C, Denton ML, Faris R, Regnerus M. Mapping American adolescent religious participation. Journal for the Scientific Study of Religion. 2002;41(4):597–612. [Google Scholar]
- Smith C, Faris R, Lundquist M. Mapping American adolescent subjective religiosity and attitudes of alienation toward religion: A research report. Sociology of Religion. 2003;64:111–133. [Google Scholar]
- Snider JB, Clements A, Vazsonyi AT. Late adolescent perceptions of parent religiosity and parenting processes. Family Process. 2004;43(4):489–502. doi: 10.1111/j.1545-5300.2004.00036.x. [DOI] [PubMed] [Google Scholar]
- Thornton A, Camburn D. Religious participation and adolescent sexual behavior and attitudes. Journal of Marriage and the Family. 1989;51(3):641–653. [Google Scholar]
- Wallace SA, Miller KS, Forehand R. Perceived peer norms and sexual intentions among African American preadolescents. AIDS Education and Prevention. 2008;20(3):360–369. doi: 10.1521/aeap.2008.20.4.360. [DOI] [PubMed] [Google Scholar]
- Zaleski EH, Schiaffino KM. Religiosity and sexual risk-taking behavior during the transition to college. Journal of Adolescence. 2000;23:223–227. doi: 10.1006/jado.2000.0309. [DOI] [PubMed] [Google Scholar]