

Abstract
Osteochondroma is a cartilage-covered bony excrescence that arises from the surface of a bone. It is the most common benign bone tumor in the scapula and can also present as multiple masses in multiple hereditary exostosis. A solitary scapular lesion might lead to “snapping scapula” syndrome, which is characterized by a sometimes audible but usually palpable grinding sensation experienced with scapular abduction. Snapping scapula is usually painless without specific symptoms; however, discomfort may result from the mechanical effects of a ventral scapular mass projecting onto a normally smooth, gliding scapulothoracic joint. Furthermore, malignant transformation of the cartilaginous cap, by virtue of the increased mass, may precipitate symptoms. The visual deformities and interference with major joint function are the most frequent musculoskeletal complaints related by patients. Indications for operative intervention include painful mechanical dysfunction unresponsive to conservative measures and sarcomatous change. Ventral scapular osteochondromas have been reported to cause scapular asymmetry and should be ruled out as part of a differential diagnosis to a “winged” scapula. A solitary osteochondroma can be excised either by arthroscopic or by open means, with the size of the lesion dictating precise management. Scapular osteochondromas usually are detected early during maturation due to mechanical symptoms or gross deformity. Unfortunately, most require surgical excision. Most surgical excisions have been reported in adolescents and young adults. We report an unusual case of osteochondroma from the ventral surface of the scapula in 56-year-old woman who had experienced delayed onset mechanical symptoms which required surgical excision.
Keywords: Osteochondroma, scapula, shoulder
INTRODUCTION
Osteochondromas have a propensity to juxta-articular positions on long bones; however, many differing locations have been described.[1–3] The osteochondromas increase in size as the skeleton grows, but normally do not grow after skeletal maturity. Few cases of osteochondromas on flat bones have been described previously in the literature, including the ventral surface of the scapula, and the condition should be ruled out when a “winged” scapula presents.[1,4,5] Only a few studies of the surgical treatment of ventral scapular lesions exist, with only two prior reports describing the surgical technique.[4,5] We report the case of a 56-year-old woman who underwent successful surgical excision of a symptomatic ventral osteochondroma of the scapula.
CASE REPORT
A 56-year-old woman presented with pain in her left shoulder, which had developed gradually over last 2 years. She noticed discomfort on her back when moving her shoulder and an asymmetry of her trunk from behind. Recently, pain developed around the scapular area, disturbing her sleep at night. During the last 6 months, progressive limitation of active motion had developed. On physical examination, scapulothoracic crepitus was noted with forward humeral elevation and external rotation. The patient reported that lying on her back caused pain. A full range of passive motion of both her shoulders was found, with significant painful crepitus from her left scapulothoracic articulation. No other bony exostoses around her body were noted.
Plain radiographic evaluation suggested the presence of ventral scapular osteochondroma [Figure 1a, b]. Three-dimensional reconstructions of computed tomography of the thoracic cage and left scapula revealed two ventral surface osteochondromas along the medial border. There was evidence of a 7.1 cm osteochondroma of the left scapula without significant thoracic cage deformity [Figure 2]. Magnetic resonance imaging (MRI) of the chest was undertaken to reveal a bone tumor on the anterior surface of the left scapula and inferior to the spine, compatible with an osteochondroma. However, there was no evidence of malignant transformation or soft tissue invasion to surrounding structures [Figure 3a, b]. This lesion had apparently been clinically silent for several years and had failed to respond to conservative measures. Therefore, surgical excision was undertaken due to concern about malignant transformation.
Figure 1 (a,b).
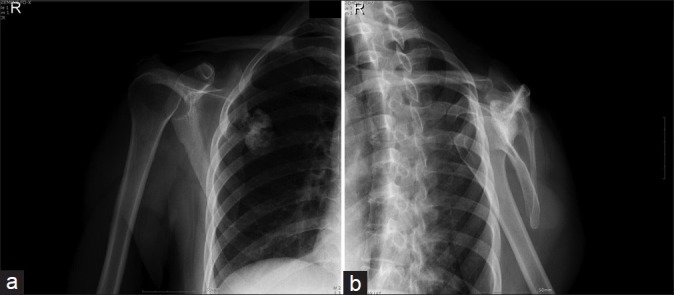
Plain radiographs: Exostoses exposed after lifting the scapula off the chest wall
Figure 2.

Computed tomography shows osteochondroma of the left scapula without significant thoracic cage deformity
Figure 3 (a, b).
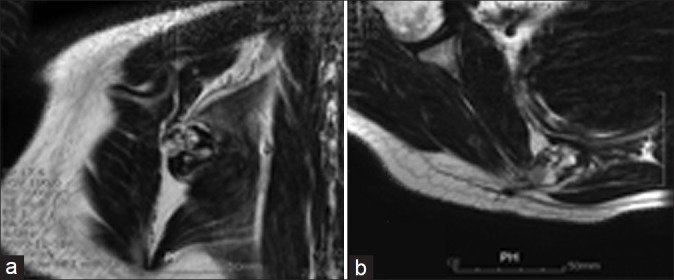
MR images demonstrate osteochondroma on the anterior surface of the left scapula and inferior to the spine
Surgical technique
Under general anesthesia, the patient was positioned in the lateral decubitus position. A parascapular skin incision along the medial border of the left scapula was employed. Five centimeters of the trapezius muscle was divided at the medial scapular border in the line of the skin incision. The rhomboid major muscle was detached from its scapular attachment, leaving a small cuff to allow for repair. It was then retracted medially to expose the medial edge of the scapula. Careful subperiosteal dissection allowed the scapula to be lifted off the chest wall to expose the osteochondromas [Figure 4]. The pedunculated osteochondromas were retracted from the thoracic cage, exposing the full extent of the cartilage caps. They were excised from the base, removing the entire protuberance. Frozen biopsy found no evidence of malignancy in the cartilaginous tissue. The pleura was protected throughout the procedure, and a postoperative chest radiograph confirmed fully inflated lungs on both sides. The specimen measured about 25 mm at the base and 70 mm in length [Figure 5]. The wound was closed in layers, paying particular attention to reattachment of the rhombus major and repair of the trapezius.
Figure 4.
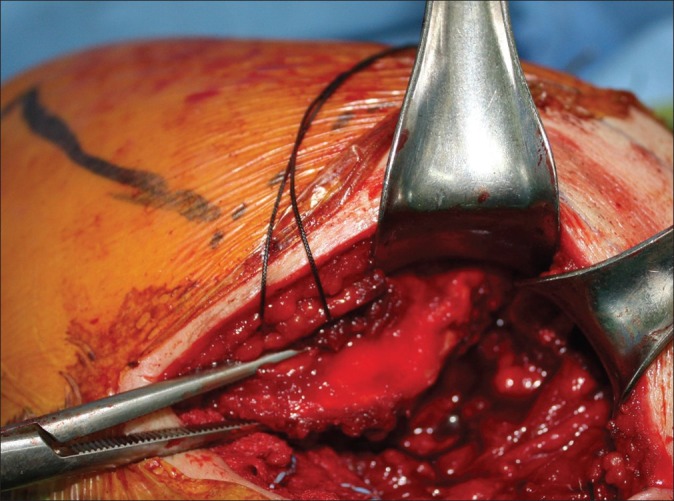
Exposure of the lesion by lifting scapula off the chest wall
Figure 5.

Gross appearance of specimens after removal
Histologic examination revealed characteristic findings of osteochondromas (cartilage capped trabecular bone covered by a fibrous capsule). The intertrabecular spaces contained adipose tissue with occasional islands of hematopoietic marrow. There was no evidence of malignant transformation.
An arm sling was applied for a week and the shoulder gently mobilized as was tolerable. No above shoulder exercises were permitted for 4 weeks postoperatively. Eventually, the patient completely recovered and returned to previous daily activity and sleep. There was no evidence of recurrence of symptoms and mass 24 months after surgery.
DISCUSSION
Osteochondromas have involved the scapula in 3.0–4.6% of all reported cases and comprise 14.4% of all tumors of the scapula.[6] The ventral surface is involved most commonly, and isolated unilateral lesions predominate.[6–8] Osteochondromas are believed to arise from normal, expanding epiphyseal cartilage nestled in sites remote from the growth plate, resulting in the typical asymmetrical mass of enchondral bone with a cartilaginous cap.[9]
Common presenting complaints of patients with an osteochondroma of the scapula include pain, decreased active range of motion, crepitus with movements of the involved shoulder, and “pseudowinging” of the scapula.[7,10] A mass may or may not be palpable. There are a number of reports of ventral scapula lesions being mistaken for “winging” of the scapula.[10]
Diagnosis is usually made by clinical features and imaging and confirmed by histopathologic evaluation, which demonstrates enchondral or lamellar bone connected to normal bone by a thin stalk in continuity with the medullary canal of the native bone.[9] Histologic specimens reveal a cartilage cap of varying thickness. A cartilaginous cap of more than 2 cm in thickness should raise concern for malignant transformation.[11] The growth of osteochondromas typically ceases at the time of closure of the physis, and growth into adulthood should raise concern for possible malignancy. Most of the case reports regarding this condition involve adolescents during the skeletal maturation period.[1,2,5–7,10–14] While our patient did not notice the lesion during maturation or even into middle age, symptoms did develop several months before care was sought. Perhaps, age-related weakness of the scapular rotators may have caused the lesion to become more clinically apparent. Furthermore, chronic bursal irritation may have promoted local soft tissue swelling, and therefore increased local interference with normal scapulothoracic kinematics.
Successful surgical treatment of ventral scapular osteochondroma consists of excision of the mass and any reactive bursa, and can be successfully performed by the surgical technique described.[4,5,6,8,12–16] The result of this surgery was excellent, significantly improving all of the patient's mechanical symptoms. Partial deformity correction was also achieved, owing to the longstanding alteration of the shape of the scapula. Overall prognosis following excision is good, although recurrence may occur if excision is incomplete.[10] Post-resection results show an overall good functional outcome.
CONCLUSIONS
Osteochondroma of the scapula may present well after skeletal maturation and may not necessarily involve malignant transformation. Surgical excision may provide an excellent clinical outcome, as evidenced by this patient.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Aalderink K, Wolf B. Scapular osteochondroma treated with arthroscopic excision using prone positioning. Am J Orthop (Belle Mead NJ) 2010;39:E11–4. [PubMed] [Google Scholar]
- 2.Bloch AM, Nevo Y, Ben-Sira L, Harel S, Shahar E. Winging of the scapula in a child with hereditary multiple exostoses. Pediatr Neurol. 2002;26:74–6. doi: 10.1016/s0887-8994(01)00343-5. [DOI] [PubMed] [Google Scholar]
- 3.Cooley LH, Torg JS. “Pseudowinging” of the scapula secondary to subscapular osteochondroma. Clin Orthop Relat Res. 1982;162:119–24. [PubMed] [Google Scholar]
- 4.Cuomo F, Blank K, Zuckerman JD, Present DA. Scapular osteochondroma presenting with exostosis bursata. Bull Hosp Jt Dis. 1993;52:55–8. [PubMed] [Google Scholar]
- 5.D’Ambrosia R, Ferguson AB., Jr The formation of osteochondroma by epiphyseal cartilage transplantation. Clin Orthop Relat Res. 1968;61:103–15. [PubMed] [Google Scholar]
- 6.Esenkaya I. Pseudowinging of the scapula due to subscapular osteochondroma. Orthopedics. 2005;28:171–2. doi: 10.3928/0147-7447-20050201-22. [DOI] [PubMed] [Google Scholar]
- 7.Fageir MM, Edwards MR, Addison AK. The surgical management of osteochondroma on the ventral surface of the scapula. J Pediatr Orthop B. 2009;18:304–7. doi: 10.1097/BPB.0b013e32832f06f4. [DOI] [PubMed] [Google Scholar]
- 8.Frost NL, Parada SA, Manoso MW, Arrington E, Benfanti P. Scapular osteochondromas treated with surgical excision. Orthopedics. 2010;33:804. doi: 10.3928/01477447-20100924-09. [DOI] [PubMed] [Google Scholar]
- 9.Fukunaga S, Futani H, Yoshiya S. Endoscopically assisted resection of a scapular osteochondroma causing snapping scapula syndrome. World J Surg Oncol. 2007;5:37. doi: 10.1186/1477-7819-5-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Krieg JC, Buckwalter JA, Peterson KK, el-Khoury GY, Robinson RA. Extensive growth of an osteochondroma in a skeletally mature patient.A case report. J Bone Joint Surg Am. 1995;77:269–73. doi: 10.2106/00004623-199502000-00015. [DOI] [PubMed] [Google Scholar]
- 11.Kumar N, Ramakrishnan V, Johnson GV, Southern S. Endoscopically-assisted excision of scapular osteochondroma. Acta Orthop Scand. 1999;70:394–6. doi: 10.3109/17453679908997832. [DOI] [PubMed] [Google Scholar]
- 12.Nercessian O, Denton JR. Cartilaginous exostosis arising from the ventral surface of the scapula. A case report. Clin Orthop Relat Res. 1988;236:145–7. [PubMed] [Google Scholar]
- 13.Schmale GA, Conrad EU, III, Raskind WH. The natural history of hereditary multiple exostoses. J Bone Joint Surg Am. 1994;76:986–92. doi: 10.2106/00004623-199407000-00005. [DOI] [PubMed] [Google Scholar]
- 14.Shackcloth MJ, Page RD. Scapular osteochondroma with reactive bursitis presenting as a chest wall tumour. Eur J Cardiothorac Surg. 2000;18:495–6. doi: 10.1016/s1010-7940(00)00545-5. [DOI] [PubMed] [Google Scholar]
- 15.Tomo H, Ito Y, Aono M, Takaoka K. Chest wall deformity associated with osteochondroma of the scapula: A case report and review of the literature. J Shoulder Elbow Surg. 2005;14:103–6. doi: 10.1016/j.jse.2004.03.007. [DOI] [PubMed] [Google Scholar]
- 16.Yoo WH, Kim JR, Jang KY, Lee SY, Park JH. Rapidly developed huge bursitis associated with scapular osteochondroma of the multiple exostosis: A case report. Rheumatol Int. 2009;29:317–9. doi: 10.1007/s00296-008-0659-8. [DOI] [PubMed] [Google Scholar]