

Abstract
Information on current practices in India for management of renal replacement therapy (RRT) in acute kidney injury (AKI) is lacking. We mailed a questionnaire to 26 pediatric nephrology centers across India to obtain information on the current choice of dialysis modality for management of AKI in children. Acute intermittent peritoneal dialysis was available at all centers surveyed, whereas intermittent hemodialysis and continuous RRT were available in 86% and 17% centers, respectively. Peritoneal dialysis was the predominant modality (accounting for more than 80% of all dialysis) in 14 of the 22 centers, while 4 centers used hemodialysis more commonly. The most important factors influencing the modality choice were patient size, hemodynamic stability, and duration of AKI. These results provide insight into the choice of modality and factors influencing their selection in the management of pediatric AKI in our country.
Keywords: Acute kidney injury, India, renal replacement therapy, survey
Introduction
Acute kidney injury (AKI; formerly known as acute renal failure) is defined as an abrupt (<48 h) increase in serum creatinine resulting from injury or insult that causes a functional or structural change in the kidney.[1] AKI is associated with significant mortality and morbidity, especially in critically ill children.[2,3] Specific indications for the initiation of renal replacement therapy (RRT) include azotemia, fluid overload, hyperkalemia, severe metabolic acidosis, and to make space for nutrition, medications, and blood products. Parallel to changes in the epidemiology of AKI, there have been dramatic changes in the availability of various types of modalities for RRT in pediatric AKI. The options have expanded from acute intermittent peritoneal dialysis (PD) and intermittent hemodialysis (HD) to continuous PD (manual or automated), continuous RRT (CRRT; continuous venovenous hemodialysis/hemofiltration/hemodiafiltration), slow low efficiency dialysis (SLED), and slow continuous ultrafiltration (SCUF). Each of these modalities have their own advantages and limitations and comparisons of these modalities have not shown any differences in survival outcomes.[4,5]
The choice of dialytic modality in our country is largely directed by the availability of resources, skills, and the cost of therapy. In general, PD has long been preferred in our country because of its efficacy, ease of implementation, and low cost. Little is known in our country regarding current RRT practices for pediatric AKI. We conducted a survey of practising pediatric nephrologists in India to obtain information on the choice of modality as well as factors that influence their choice.
Materials and Methods
A one-page questionnaire was mailed to 26 pediatric nephrology centres (11 in metropolitan cities) across India, all of whom provided RRT for management of AKI [Appendix]. Demographic questions included the incidence of AKI, proportion with AKI requiring RRT, and three most common etiologies for AKI over a 12-month period. Six questions related to the availability of infrastructure and equipment for various forms of dialysis and common type of RRT performed. Respondents were also requested to rate a list of 12 factors for relative importance in influencing their choice of modality. Each factor was rated on a scale of 1 to 5 (1- definitely important, 2- important, 3- neutral, 4- not important, and 5- definitely not important). The factors were patient size, personal preference, socioeconomic background of care receiver, etiology of AKI, urine output, blood urea, serum creatinine, potassium level, fluid balance, hemodynamic status, duration of AKI, and timing of admission to hospital. The data collected were summarized using descriptive statistics. Data are presented as median with range or as percentages where appropriate.
Appendix.
Results
Completed surveys were returned from 23 centers (response rate of 88%). Of the centers that responded, 13 were in medical colleges, four in private hospitals, and six in corporate hospitals. Approximately 1,475 children with AKI were managed at the 23 centers over a 12-month period (range, 10-250 per year). AKI accounted for less than 20%, 30-40%, and more than 40% of children with renal disease at 14, 6, and 3 centers, respectively. The proportion of children with AKI requiring RRT varied from less than 10% at five centers to more than 50% at four centers. The most common etiologies of AKI were hemolytic uremic syndrome, diarrhea with dehydration, and acute glomerulonephritis.
Peritoneal dialysis was available at all 23 (100%) centers, HD at 21 (86%) centers, SLED at 6 (23%) centers, and CRRT at 4 (17%) centers [Figure 1]. Only two centers had the infrastructure for all modalities. PD and HD were the primary modalities of choice of RRT at 19 and 4 of the responding centers, respectively. CRRT/SLED constituted 5-10% of all dialysis at the available centers. At all centers, PD is the primary choice of dialytic modality for children below 2 years of age, whereas it is the primary modality at 7 (30%) centers for children aged more than 12 years [Figure 1]. Hemodialysis is the preferred modality for dialysis at 5 centers in children aged 7-12 years and at 16 centers for children aged more than 12 years. Of the centers that had the facility for HD, only 3 (13%) had a standalone HD unit, while the remaining centers shared the facility with the adult nephrology unit. Two centers also had HD facility within the premises of pediatric intensive care unit (PICU). Most of the centers (16/23) performed manual acute intermittent dialysis using the rigid peritoneal catheter, while automated PD was the preferred mode in seven centers. Continuous PD (manual or automated) using Technkoff catheter constituted 10-30% of all PDs done at the centers where the facility was available (7/23 centers).
Figure 1.
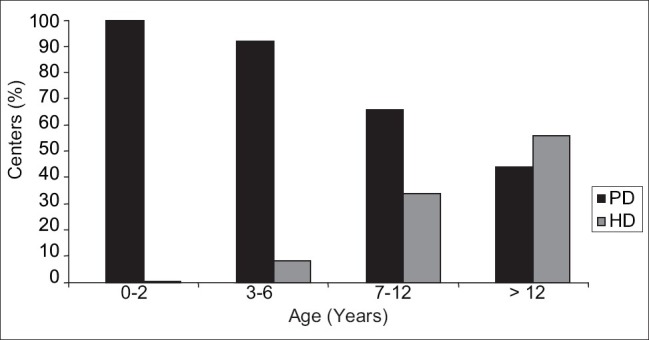
Patient age and preferential use of acute peritoneal dialysis and hemodialysis by participating centers. (PD - Peritoneal dialysis; HD - Hemodialysis)
Respondents were asked to rate a list of 12 factors with regard to the relative importance of each factor in the decisions to initiate dialysis and the choice of modality. Factors rated by the majority of centers (15/23) as definitely important or important were patient size, hemodynamic status, duration of AKI, and severity of hyperkalemia [Figure 2]. Ten centers also considered socioeconomic status of care receiver and personal preference as important factors in deciding the choice of modality.
Figure 2.
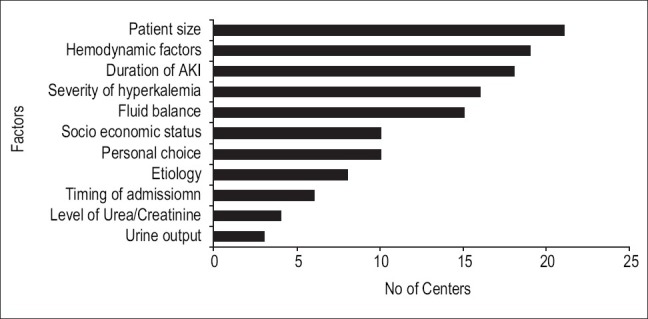
Numbers of centers rating each of the clinical factors as very important or important
Discussion
This survey highlights the present trend in dialytic management of pediatric AKI in India. AKI constituted 10-40% of pediatric renal diseases and 10-30% with AKI required some form of RRT, which suggests that AKI is common in our country, and a significant number of children with AKI require RRT. Our data provide evidence that PD is the most common modality used even if other modalities were available at most centers. This is because PD is technically simple and inexpensive and can be performed in regions with limited infrastructure. This is in contrast to the results of a survey conducted in North America and Europe, where PD usage has decreased dramatically over the past decade and the preferential use of CRRT appears to be increasing.[6,7] In the survey, CRRT was considered the treatment of choice at approximately 30% of the centers and the number of centers using PD as the preferred modality decreased from 45% in 1995 to 20% in 2003. Not unexpectedly, patient age was a significant factor influencing the use of PD, HD, or CRRT as a treatment modality. Our data reflect the fact that PD is preferentially used by all centers in younger children (<2 years) probably because of the difficulty associated with obtaining vascular access in smaller children. Proportionately, the use of HD increases with age of patient and is the primary modality of choice in 70% of the centers for children of age more than 12 years. This is similar to that observed by Warady et al.[6] in their survey in America and Europe. While use of a rigid catheter and acute intermittent PD continues to be the most common form of PD in a majority of centers (70% of centers surveyed), there is an increasing trend in the use of Technkoff catheters for providing manual or automated continuous PD in pediatric AKI in India, with seven centers using it as the primary modality. Continuous PD is associated with lesser incidence of peritonitis and is preferable for children who need prolonged dialysis.[4] These catheters can be inserted by a trained nephrologist or surgeon at the bedside.
Among the centers having access to HD, only two had their own units, thus reflecting the logistics and cost of establishing a HD unit. Children with AKI who are critically ill are often unstable may be put on ventilator and inotropic supports. It is desirable to offer RRT in PICU itself. In contrast to delivery of PD in PICU, SLED, or CRRT was available in four and six centers, respectively. Progress with CRRT is limited in view of the high cost for the equipment and specialized training required to provide the therapy. Many factors could influence the use of specific dialytic modality. Although the respondents were not asked about the RRT choice for each of the specific factors – patient size, hemodynamic status, duration of AKI, and severity of hyperkalemia – these were rated as definitely important or important by a majority of centers in influencing their choice of modality. It is likely that younger children, children in shock, and those with prolonged AKI were more likely to receive PD as compared to other modalities. Physician preference was considered important by nearly half of the centers while choosing a modality and explains the choice of PD over other modalities even though many centers had access to other modalities. The cost of therapy between the modalities could not be done as those surveyed cater to a heterogenous group of patient clientele and cost of therapy would vary. Additional data on indication for dialysis, dosing practices, and correlating patient outcome to choice of modality should be collected in order to formulate guidelines on management of AKI in children.
Conclusion
A significant number of children with AKI require RRT in our country. A wide variability exists in the availability of RRT modalities among the participating centers. Acute intermittent PD continues to be the most common form of modality for dialyzing children with AKI, especially in younger children. Availability, individual patient factors, cost of therapy, and personal preference influence the decision to use PD, HD, or other modalities in an individual with AKI.
Acknowledgments
We thank and acknowledge the following centers and doctors for participating in this survey Abhijeet Saha RML Hospital New Delhi, Amarjeet Mehta SMS Medical College Jaipur, Amitav Pahari Gleaneagles Hospital Calcutta, Arvind Bagga All India Institute of Medical Sciences New Delhi, Fagun Shah Surat, Gurdeep Singh CMC Ludhiana, Indira Agarwal CMC Vellore, Janaki Menon Govrment Medical College Thrissur, Madhuri Kanitkar Armed Forces Medical College Pune, Manisha Sahay Osmania Medical College Hyderabad, Manoj Matnani KEM Hospital Pune, Mukta Mantan Chacha Nehru Children's Hospital New Delhi, Mehul Shah Rainbow Hospital Hyderabad, Nagamani Agarwal JJM Medical College Davengere, OP Mishra Banaras Hindu University, Varanasi, Prahlad Nageswran Mehta's Children Hospital, Chennai, Premaltaha N Bangalre Medical College Bengaluru, Rupesh Jain Ekta Children's Hospital, Raipur, Sairam VK Chennai, Sudarshan Shetty KS Hegde Medical College Mangalore, Susmitha Banerjee Calcutta Medical Research Institute, Calcutta Vinay Agarwal, Apollo Hospitals Delhi.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Bagga A, Bakkaloglu, Devarajan P, Mehta RL, Kellum JA, Shah SV, et al. Improving outcomes from acute kidney injury: Report of an initiative. Pediatr Nephrol. 2007;22:1655–8. doi: 10.1007/s00467-007-0565-4. [DOI] [PubMed] [Google Scholar]
- 2.Walters S, Porter C, Brophy PD. Dialysis and pediatric acute kidney injury: Choice of renal support Modality. Pediatr Nephrol. 2009;24:37–48. doi: 10.1007/s00467-008-0826-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cerda J, Bagga A, Kher V, Chakravarthi RM. The contrasting characetristics of acute kidney injury in developed and developing countries. Nat Clin Pract Nephrol. 2008;4:138–53. doi: 10.1038/ncpneph0722. [DOI] [PubMed] [Google Scholar]
- 4.Maxvold NJ, Smoyer WE, Gardner JJ, Bunchman TE. Management of acute renal failure in the pediatric patient: Hemofiltration versus hemodialysis. Am J Kid Dis. 1997;5:S84–8. doi: 10.1016/s0272-6386(97)90547-3. [DOI] [PubMed] [Google Scholar]
- 5.Abi Antoun T, Palevsky PM. Selection of modality of renal replacement therapy. Semin Dial. 2009;22:108–13. doi: 10.1111/j.1525-139X.2008.00540.x. [DOI] [PubMed] [Google Scholar]
- 6.Belsha CW, Kohaut EC, Warady BA. Dialytic management of childhood acute renal failure: A survey of North American pediatric nephrologists. Pediatr Nephrol. 1995;9:361–3. doi: 10.1007/BF02254215. [DOI] [PubMed] [Google Scholar]
- 7.Warady BA, Bunchman T. Dialysis therapy for children with acute renal failure: Survey results. Pediatr Nephrol. 2000;15:11–3. doi: 10.1007/s004670000420. [DOI] [PubMed] [Google Scholar]